
Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Aims of the Study
3. Materials and Methods
3.1. Study Design
3.2. Setting and Sample
3.3. Questionnaires and Data Collection
3.3.1. Socio-Demographic and Work-Related Characteristics
3.3.2. Validation of the Ethical Conflict Scale Covid-19 (ECS-Co19)
3.3.3. Self-Reported Psychological Distress
3.3.4. Psychological Resilience
4. Data Analysis
5. Results
5.1. Socio-Demographic Characteristics
5.2. Validity and Reliability of the Ethical Conflict Scale Covid-19 (ECS-Co19)
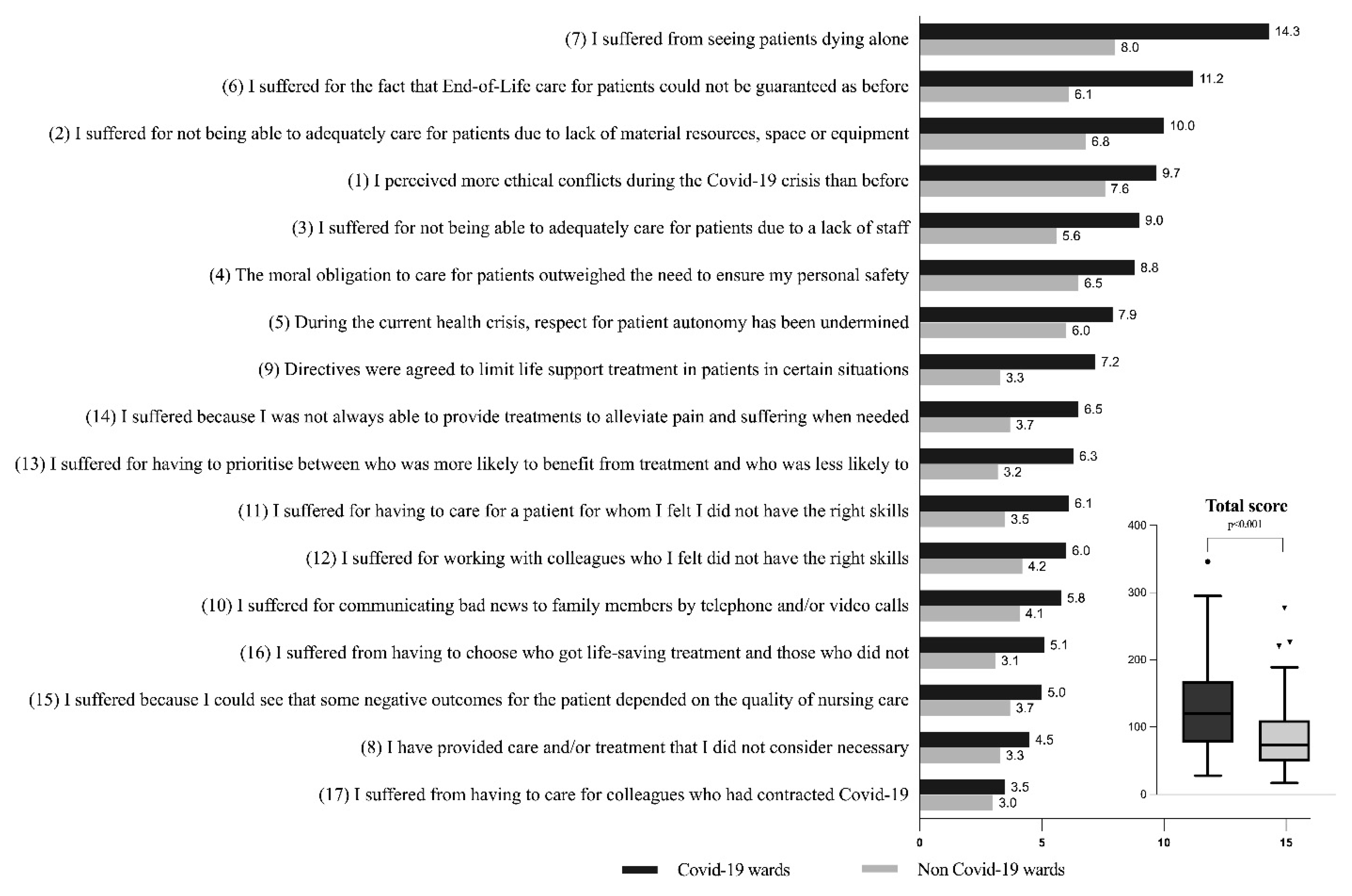
5.3. Ethical Conflict
Psychological Distress
5.4. Resilience
5.5. Risk Factors Associated with High Ethical Conflict and High Psychological Distress
6. Discussion
Limitations of the Study
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Weekly Epidemiological Update. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---15-June-2021 (accessed on 17 June 2021).
- Barello, S.; Graffigna, G. Caring for Health Professionals in the COVID-19 Pandemic Emergency: Toward an “Epidemic of Empathy” in Healthcare. Front. Psychol. 2020, 11, 1431. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef] [PubMed]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting-A Systematic Review. J. Occup. Health 2020, 62, e12175. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Falcó-Pegueroles, A.; Rosa, D.; Tolotti, A.; Graffigna, G.; Bonetti, L. The psychosocial impact of flu influenza pandemics on healthcare workers and lessons learnt for the COVID-19 emergency: A rapid review. Int. J. Public Health 2020, 65, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, Y.; Hu, K.; Zhang, M.; Du, M.; Huang, H.; Yue, X. Healthcare workers’ stress when caring for COVID-19 patients: An altruistic perspective. Nurs. Ethics 2020, 27, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Lim, M.K.; Chia, S.E.; Ko, S.M.; Qian, F.; Ng, V.; Tan, B.H.; Wong, K.S.; Chew, W.M.; Tang, H.K.; et al. Risk perception and impact of Severe Acute Respiratory Syndrome (SARS) on work and personal lives of healthcare workers in Singapore: What can we learn? Med. Care 2005, 43, 676–682. [Google Scholar] [CrossRef]
- Chen, C.S.; Wu, H.Y.; Yang, P.; Yen, C.F. Psychological distress of nurses in Taiwan who worked during the outbreak of SARS. Psychiatr. Serv. 2005, 56, 76–79. [Google Scholar] [CrossRef]
- Wong, T.W.; Yau, J.K.; Chan, C.L.; Kwong, R.S.; Ho, S.M.; Lau, C.C.; Lau, F.L.; Lit, C.H. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur. J. Emerg. Med. 2005, 12, 13–18. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, E.H.; Park, N.R.; Choi, Y.H. Mental Health of Nurses Working at a Government-designated Hospital During a MERS-CoV Outbreak: A Cross-sectional Study. Arch. Psychiatr. Nurs. 2018, 32, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Carmassi, C.; Foghi, C.; Dell’Oste, V.; Cordone, A.; Bertelloni, C.A.; Bui, E.; Dell’Osso, L. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: What can we expect after the COVID-19 pandemic. Psychiatry Res. 2020, 292, 113312. [Google Scholar] [CrossRef]
- Borasio, G.D.; Gamondi, C.; Obrist, M.; Jox, R. For The Covid-Task Force of Palliative, C. COVID-19: Decision making and palliative care. Swiss Med. Wkly. 2020, 150, w20233. [Google Scholar] [CrossRef] [PubMed]
- Falcó-Pegueroles, A.; Zurigel-Perez, E.; Via-Clavero, G.; Bosch-Alcaraz, A.; Bonetti, L. Ethical conflict during the COVID-19 pandemic: The cases of Spanish and Italian intensive care units. Int. Nurs. Rev. 2021, 68, 181–188. [Google Scholar] [CrossRef] [PubMed]
- McKenna, H. COVID-19: Ethical issues for nurses. Int. J. Nurs. Stud. 2020, 110, 103673. [Google Scholar] [CrossRef]
- Robert, R.; Kentish-Barnes, N.; Boyer, A.; Laurent, A.; Azoulay, E.; Reignier, J. Ethical dilemmas due to the COVID-19 pandemic. Ann. Intensive Care 2020, 10, 84. [Google Scholar] [CrossRef]
- Deschenes, S.; Kunyk, D. Situating moral distress within relational ethics. Nurs. Ethics 2020, 27, 767–777. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Lluch-Canut, T.; Roldan-Merino, J.; Goberna-Tricas, J.; Guàrdia-Olmos, J. Ethical conflict in critical care nursing: Correlation between exposure and types. Nurs. Ethics 2015, 22, 594–607. [Google Scholar] [CrossRef]
- Jameton, A. Nursing Practice: The Ethical Issues; Prentice Hall: Hoboken, NJ, USA, 1984. [Google Scholar]
- Pishgooie, A.H.; Barkhordari-Sharifabad, M.; Atashzadeh-Shoorideh, F.; Falcó-Pegueroles, A. Ethical conflict among nurses working in the intensive care units. Nurs. Ethics 2019, 26, 2225–2238. [Google Scholar] [CrossRef]
- Rittenmeyer, L.; Huffman, D. How professional nurses working in hospital environments experience moral distress: A systematic review. JBI Libr. Syst. Rev. 2009, 7, 1234–1291. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, N.S.; Schiffman, R.; Leske, J. Relationships among Climate of Care, Nursing Family Care and Family Well-being in ICUs. Nurs. Ethics 2019, 26, 2494–2510. [Google Scholar] [CrossRef]
- Abu-El-Noor, N.I.; Abu-El-Noor, M.K. Ethical issues in caring for COVID-patients: A view from Gaza. Nurs. Ethics 2020, 27, 1605–1606. [Google Scholar] [CrossRef]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef] [PubMed]
- Morley, G.; Grady, C.; McCarthy, J.; Ulrich, C.M. COVID-19: Ethical Challenges for Nurses. Hastings Cent. Rep. 2020, 50, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.; Norful, A.A.; Travers, J.; Aliyu, S. Nursing perspectives on care delivery during the early stages of the covid-19 pandemic: A qualitative study. Int. J. Nurs. Stud. Adv. 2020, 2, 100006. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Lluch-Canut, T.; Guàrdia-Olmos, J. Development process and initial validation of the Ethical Conflict in Nursing Questionnaire-Critical Care Version. BMC Med. Ethics 2013, 14, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glorfeld, L.W. An Improvement on Horn’s Parallel Analysis Methodology for Selecting the Correct Number of Factors to Retain. Educ. Psychol. Meas. 1995, 55, 377–393. [Google Scholar] [CrossRef]
- Horn, J.L. A Rationale and Test for the Number of Factors in Factor Analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Howard, M.C. A Review of Exploratory Factor Analysis Decisions and Overview of Current Practices: What We Are Doing and How Can We Improve? Int. J. Hum.-Comput. Interact. 2016, 32, 51–62. [Google Scholar] [CrossRef]
- Craparo, G.; Faraci, P.; Rotondo, G.; Gori, A. The Impact of Event Scale—Revised: Psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatr. Dis. Treat. 2013, 9, 1427–1432. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Faggioni, M.P.; González-Melado, F.J.; Di Pietro, M.L. National health system cuts and triage decisions during the COVID-19 pandemic in Italy and Spain: Ethical implications. J. Med. Ethics 2021, 47, 300–307. [Google Scholar] [CrossRef]
- Haas, L.E.M.; de Lange, D.W.; van Dijk, D.; van Delden, J.J.M. Should we deny ICU admission to the elderly? Ethical considerations in times of COVID-19. Crit. Care 2020, 24, 321. [Google Scholar] [CrossRef] [PubMed]
- Wakam, G.K.; Montgomery, J.R.; Biesterveld, B.E.; Brown, C.S. Not Dying Alone-Modern Compassionate Care in the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e88. [Google Scholar] [CrossRef] [PubMed]
- International Council of Nurses. The ICN Code of Ethics for Nurses. Available online: https://www.icn.ch/sites/default/files/inline-files/2012_ICN_Codeofethicsfornurses_%20eng.pdf (accessed on 28 March 2021).
- Bonalumi, G.; di Mauro, M.; Garatti, A.; Barili, F.; Gerosa, G.; Parolari, A. The COVID-19 outbreak and its impact on hospitals in Italy: The model of cardiac surgery. Eur. J. Cardiothorac. Surg. 2020, 57, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Vergano, M.; Bertolini, G.; Giannini, A.; Gristina, G.R.; Livigni, S.; Mistraletti, G.; Riccioni, L.; Petrini, F. Clinical ethics recommendations for the allocation of intensive care treatments in exceptional, resource-limited circumstances: The Italian perspective during the COVID-19 epidemic. Crit. Care 2020, 24, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemida Salem, A. Critical Care Nurses’ Perceptions of Ethical Distresses and Workplace Stressors in the Intensive Care Units. Int. J. Nurs. Educ. 2015, 7, 93–99. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public-A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Nelson, S.E. COVID-19 and ethics in the ICU. Crit. Care 2020, 24, 519. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef]
- Ip, V.H.Y.; Sondekoppam, R.V. The Need to Protect Health Care Workers Is Unchanged in the Presence of COVID-19 Pandemic Fatigue: The Probable Might Still Be Possible. Anesth. Analg. 2021, 132, e42–e43. [Google Scholar] [CrossRef]
- Vincent, J.L.; Creteur, J. Ethical aspects of the COVID-19 crisis: How to deal with an overwhelming shortage of acute beds. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 248–252. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Hung, Y.T.; Wang, H.H.; Ma, S.C.; Chang, S.C. Factors of Resilience in Emergency Department Nurses Who Have Experienced Workplace Violence in Taiwan. J. Nurs. Scholarsh. 2016, 48, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Rushton, C.H.; Batcheller, J.; Schroeder, K.; Donohue, P. Burnout and Resilience Among Nurses Practicing in High-Intensity Settings. Am. J. Crit. Care 2015, 24, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Kuek, J.T.Y.; Ngiam, L.X.L.; Kamal, N.H.A.; Chia, J.L.; Chan, N.P.X.; Abdurrahman, A.; Ho, C.Y.; Tan, L.H.E.; Goh, J.L.; Khoo, M.S.Q.; et al. The impact of caring for dying patients in intensive care units on a physician’s personhood: A systematic scoping review. Philos. Ethics Humanit. Med. 2020, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensive Crit. Care Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef]
- Thusini, S. Critical care nursing during the COVID-19 pandemic: A story of resilience. Br. J. Nurs. 2020, 29, 1232–1236. [Google Scholar] [CrossRef]

{kind=link}
| Variables | All Nurses (N = 548) | Non-Covid-19 Wards (N = 273) | Covid-19 Wards (N = 275) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Age, years | 40 | ±10 | 40.8 | ±10.2 | 39.7 | ±10.1 | 0.8 |
| Female | 419 | (76.5) | 230 | (84.2) | 189 | (76.5) | <0.001 |
| Years of experience as nurse | N | % | N | % | N | % | |
| 0 to 5 | 89 | (16.2) | 37 | (13.2) | 52 | (18.9) | 0.245 |
| 6 to 10 | 122 | (22.3) | 64 | (23.4) | 58 | (21.1) | |
| 11 to 20 | 137 | (25) | 65 | (23.8) | 76 | (26.2) | |
| over 20 | 200 | (36.5) | 107 | (39.2) | 93 | (33.8) | |
| Live alone | 144 | (26.3) | 71 | (26) | 73 | (26.5) | 0.886 |
| Live with frail people (i.e., children or older/ill people) | 257 | (46.9) | 136 | (49.9) | 121 | (44) | 0.144 |
| Post-basic education | 317 | (57.8) | 148 | (54.2) | 169 | (61.5) | 0.086 |
| Work-time percentage | N | % | N | % | N | % | |
| lower than 60% | 34 | (6.2) | 25 | (9.9) | 9 | (3.3) | <0.001 |
| 60 to 90% | 213 | (38.9) | 130 | (47.6) | 83 | (30.2) | |
| over 90% | 301 | (54.9) | 118 | (43.2) | 183 | (66.5) | |
| Relocation to another ward during the pandemic | 167 | (30.5) | 37 | (13.6) | 130 | (47.3) | <0.001 |
| ICU during Covid-19 | 103 | (18.8) | 33 | (12.1) | 70 | (25.5) | <0.001 |
| Desire to change profession before the pandemic (yes/no) | 147 | (26.8) | 76 | (27.6) | 71 | (26.0) | 0.67 |
| Desire to change profession during the pandemic (yes/no) | 119 | (21.7) | 66 | (24) | 53 | (19.4) | 0.19 |
| Perception of the risk of being infected during the pandemic, (score 0 = low risk to 10 = high risk) (Median (25th, 75th percentiles)) | 5 | [4–8] | 6 | [4–8] | 4 | [3–7] | <0.001 |
| Perception of one’s own health status (SF12 first question: How do you rate your health status on a scale from 1 = poor to 5 = excellent) (Median [25th, 75th percentiles]) | 4 | [2–4] | 4 | [2–4] | 4 | [2–4] | 0.008 |
| Ethical Conflict Scale Covid-19 (ECS-Co19) Items | All Nurses | Non-Covid-19 Wards | Covid-19 Wards | p-Value # | ||||
|---|---|---|---|---|---|---|---|---|
| N = 548 | N = 273 | N = 275 | ||||||
| 1 | I perceived more ethical conflicts during the Covid-19 crisis than before. | 9 | [4.0–12.0] ç | 8.0 | [4.0–9.0] | 9.0 | [4.0–12.0] | <0.001 |
| 2 | I suffered for not being able to adequately care for patients due to lack of material resources, space or equipment. | 6 | [4.0–12.0] | 4.0 | [2.5–9.0] | 9.0 | [4.0–16.0] | <0.001 |
| 3 | I suffered for not being able to adequately care for patients due to a lack of staff. | 4 | [1.0–9.0] | 4.0 | [1.0–8.5] | 6.0 | [2.0–15.0] | <0.001 |
| 4 | The moral obligation to care for patients outweighed the need to ensure my personal safety. | 6 | [3.0–12.0] | 4.0 | [2.0–9.0] | 8.0 | [4.0–12.0] | <0.001 |
| 5 | During the current health crisis, respect for patient autonomy has been undermined. | 6 | [2.0–9.0] | 4.0 | [1.0–9.0] | 6.0 | [4.0–10.0] | <0.001 |
| 6 | I suffered for the fact that End-of-Life care for patients could not be guaranteed as before. | 6 | [2.0–16.0] | 4.0 | [1.0–9.0] | 10.0 | [4.0–16.0] | <0.001 |
| 7 | I suffered for seeing patients dying alone. | 9 | [4.0–16.0] | 5.0 | [1.0–12.0] | 15.0 | [8.0–20.0] | <0.001 |
| 8 | I provided care and/or treatment that I did not consider necessary. | 2 | [1.0–5.0] | 1.0 | [1.0–4.0] | 3.0 | [1.0–6.0] | 0.012 |
| 9 | Directives were agreed to limit life support treatment in patients in certain situations. | 4 | [1.0–8.0] | 2.0 | [1.0–4.0] | 6.0 | [2.0–12.0] | <0.001 |
| 10 | I suffered for communicating bad news to family members by telephone and/or video calls. | 4 | [1.0–6.0] | 4.0 | [1.0–5.0] | 4.0 | [1.0–9.0] | 0.003 |
| 11 | I suffered for having to care for a patient for whom I felt I did not have the right skills. | 4 | [1.0–6.0] | 1.0 | [1.0–4.0] | 4.0 | [1.0–9.0] | <0.001 |
| 12 | I suffered for working with colleagues who I felt did not have the right skills. | 4 | [1.0–6.0] | 3.0 | [1.0–5.0] | 4.0 | [1.0–9.0] | <0.001 |
| 13 | I suffered for having to prioritise between who was more likely to benefit from treatment and who was less likely to. | 3 | [1.0–6.0] | 1.0 | [1.0–4.0] | 4.0 | [1.0–9.0] | <0.001 |
| 14 | I suffered because I was not always able to provide treatments to alleviate pain and suffering when needed. | 4 | [1.0–8.0] | 3.0 | [1.0–5.0] | 5.0 | [1.0–9.0] | <0.001 |
| 15 | I suffered because I could see that some negative outcomes for the patient depended on the quality of nursing care. | 4 | [1.0–5.0] | 1.0 | [1.0–5.0] | 4.0 | [1.0–6.0] | 0.005 |
| 16 | I suffered for having to choose patients who got life-saving treatment and those who did not. | 1 | [1.0–5.0] | 1.0 | [1.0–5.0] | 2.0 | [1.0–8.0] | 0.002 |
| 17 | I suffered for having to care for colleagues who had contracted Covid-19. | 1 | [1.0–4.0] | 1.0 | [1.0–4.0] | 1.0 | [1.0–5.0] | 0.988 |
| Total score | 111.5 | [76.0–152.0] | 91.0 | [68.5–125.0] | 133.0 | [91.0–179.0] | <0.001 | |
| Impact of Event Scale (IES)-Revised Scoring Sum of the Item Values | All Nurses (548) | Non-Covid-19 Wards (N = 273) | Covid-19 Wards (N = 275) | p-Value # | |||
|---|---|---|---|---|---|---|---|
| IES Subscale Avoidance | 5 | [2–8.75] ç | 4 | [1–8] | 5 | [2–9] | 0.029 |
| IES Subscale Intrusion | 6 | [3–11] | 5 | [2–10] | 7 | [3–14] | <0.001 |
| IES Subscale hyper-arousal | 4 | [1–7] | 3 | [1–6] | 4 | [1–8] | 0.301 |
| IES Impact of Event Scale (0–88) (Total score) | 15 | [7–26] | 12 | [6–23.5] | 17 | [7–29] | 0.005 |
| IES-R > 30 N (%) | 109 (19.9) | 41 (15.0) | 62 (24.7) | <0.001 | |||
| Variables | All Nurses (N = 548) | Covid-19 Wards (N = 275) | Non-Covid-19 Wards (N = 273) | p-Value # | |||
|---|---|---|---|---|---|---|---|
| Brief Resilience Scale—usual resilience, (score 0 to 5) | 3 | [2.8–3.2] ç | 3 | [2.8–3] | 3 | [2.8–3.2] | 0.23 |
| Brief Resilience Scale—during the pandemic, (score 0 to 5) | 3 | [2.8–3.0] | 3 | [2.8–3] | 3 | [2.8–3] | 0.57 |
| Variables | High Ethical Conflict | IES-R > 30 Points | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | P-Value | |
| Female | 2.62 (1.56–4.39) | <0.001 | 2.54 (1.38–4.66) | 0.003 |
| Years of experience as nurse | 0.69 (0.56–0.86) | 0.001 | 1.08 (0.86–1.36) | 0.468 |
| Post-basic education | 1.25 (0.77–2.02) | 0.352 | 0.95 (0.57–1.59) | 0.865 |
| Full-time job | 0.92 (0.59–1.45) | 0.743 | 1.33 (0.82–2.18) | 0.242 |
| Desire to change profession before the pandemic | 1.21 (0.78–1.89) | 0.378 | 1.15 (0.71–1.86) | 0.555 |
| Brief Resilience Scale (usual resilience) | 0.50 (0.26–0.94) | 0.033 | 0.81 (0.42–1.59) | 0.558 |
| Hospital wards | ||||
| General ward | (reference) | NA | (reference) | NA |
| Covid-19 ward | 5.85 (3.56–9.61) | <0.001 | 2.16 (1.29–3.60) | 0.003 |
| ICU | 3.18 (1.41–7.16) | <0.005 | 1.04 (0.39–2.74) | 0.929 |
| Covid-19 ICU | 7.18 (3.96–13.01) | <0.001 | 1.75 (0.93–3.31) | 0.083 |
| HL-test p = 0.124 AUC = 75 (CI 95% 71–80) | HL-test p = 0.458 AUC = 64 (CI 95% 58–69) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villa, M.; Balice-Bourgois, C.; Tolotti, A.; Falcó-Pegueroles, A.; Barello, S.; Luca, E.C.; Clivio, L.; Biegger, A.; Valcarenghi, D.; Bonetti, L. Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards. Int. J. Environ. Res. Public Health 2021, 18, 12012. https://doi.org/10.3390/ijerph182212012
Villa M, Balice-Bourgois C, Tolotti A, Falcó-Pegueroles A, Barello S, Luca EC, Clivio L, Biegger A, Valcarenghi D, Bonetti L. Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards. International Journal of Environmental Research and Public Health. 2021; 18(22):12012. https://doi.org/10.3390/ijerph182212012
Chicago/Turabian StyleVilla, Michele, Colette Balice-Bourgois, Angela Tolotti, Anna Falcó-Pegueroles, Serena Barello, Elena Corina Luca, Luca Clivio, Annette Biegger, Dario Valcarenghi, and Loris Bonetti. 2021. "Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards" International Journal of Environmental Research and Public Health 18, no. 22: 12012. https://doi.org/10.3390/ijerph182212012
APA StyleVilla, M., Balice-Bourgois, C., Tolotti, A., Falcó-Pegueroles, A., Barello, S., Luca, E. C., Clivio, L., Biegger, A., Valcarenghi, D., & Bonetti, L. (2021). Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards. International Journal of Environmental Research and Public Health, 18(22), 12012. https://doi.org/10.3390/ijerph182212012