
Prevalence of Untreated Early Childhood Caries of 5-Year-Old Children in Hong Kong: A Cross-Sectional Study

 , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participnts
2.2. Sampling Method
2.3. Sample Size Calculation
2.4. Questionnaire Survey
2.5. Clinical Examination
2.6. Statistical Analysis
2.7. Research Ethics and Study Participnts
3. Results
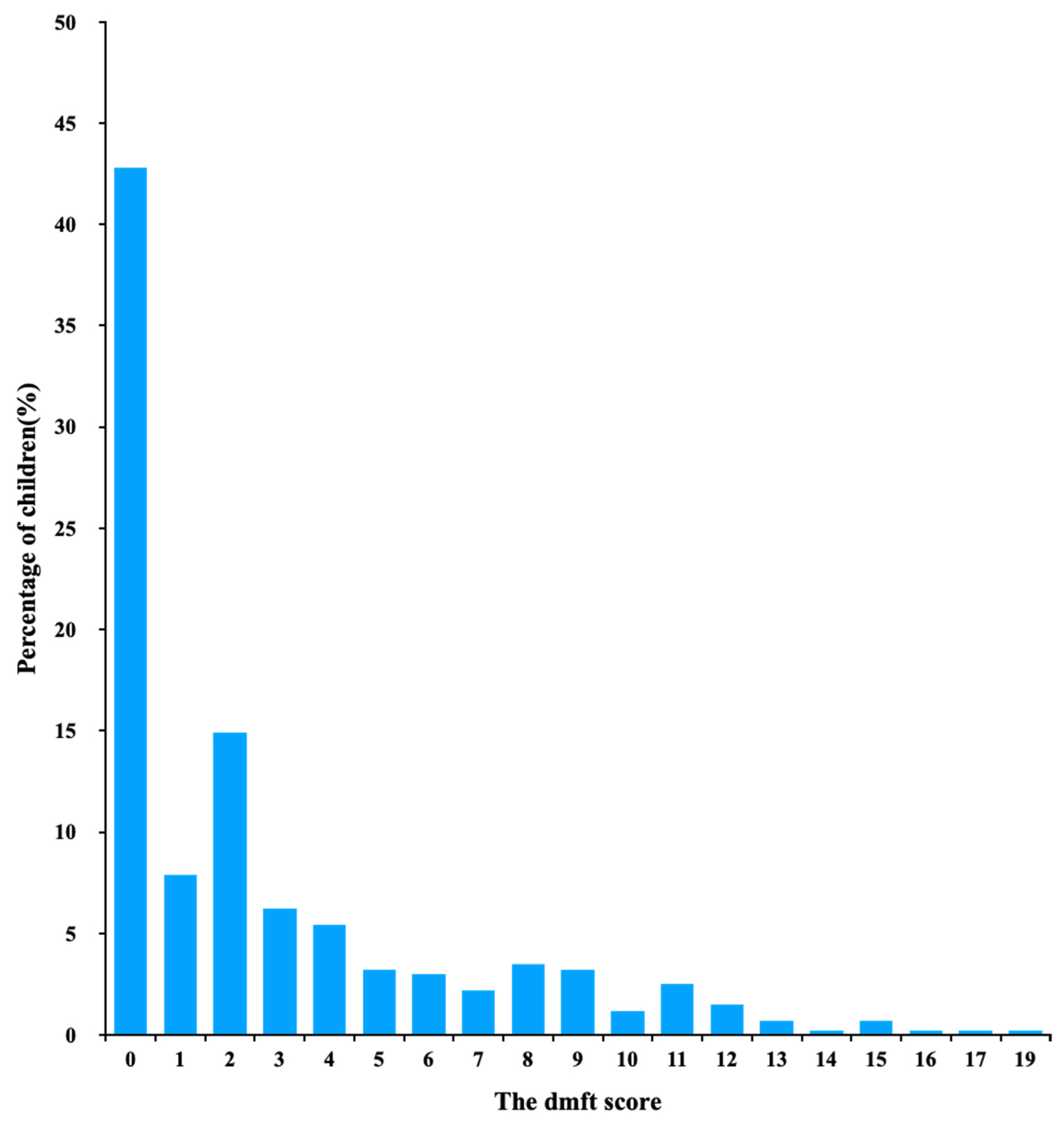
3.1. Overall Situation of Untreated ECC among Hong Kong 5-Year-Old Children
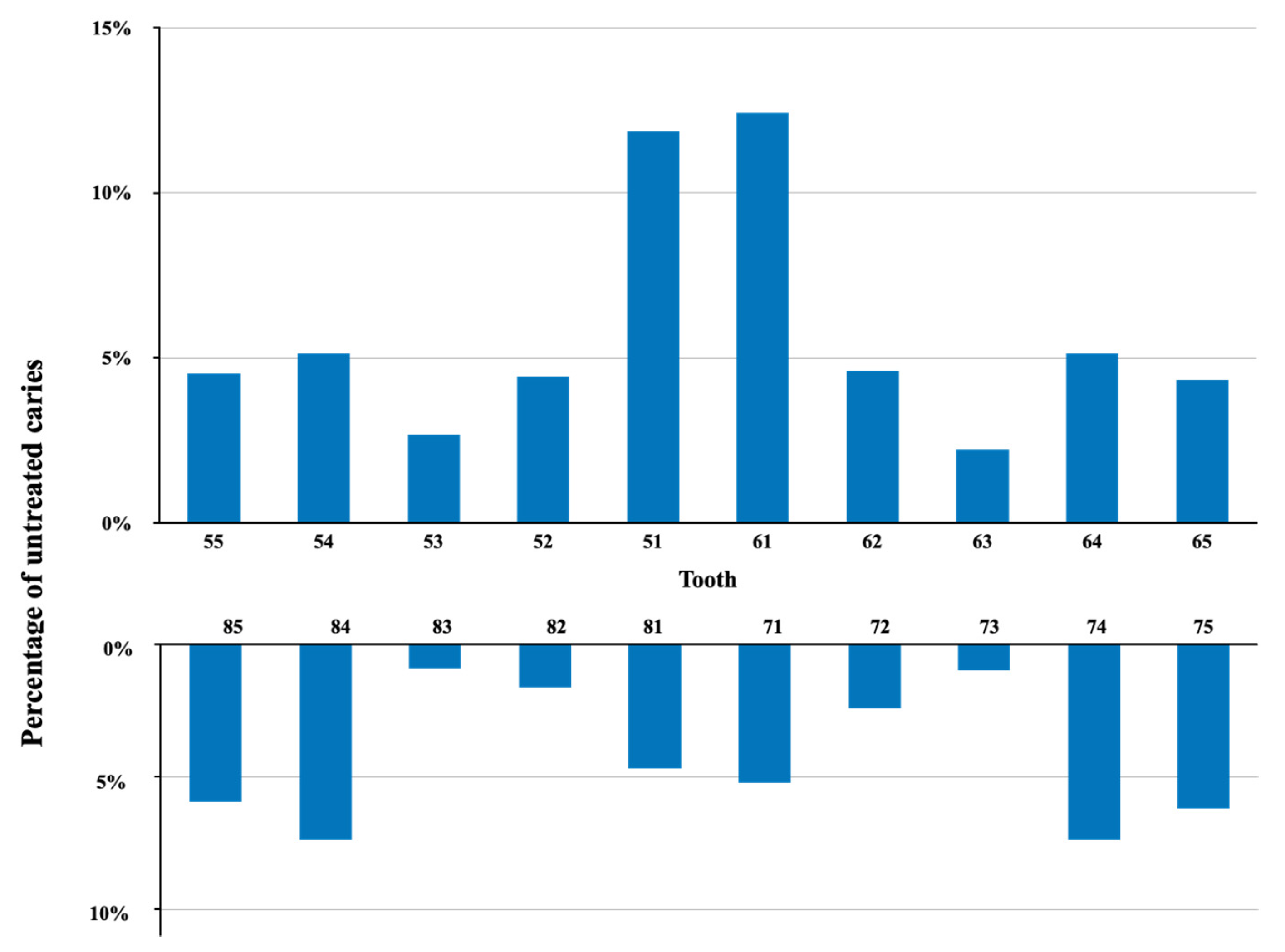
3.2. Distribution of Untreated ECC Teeth
3.3. Untreated ECC Prevalence According to District, Birthplace and Sex
3.4. Untreated ECC and Its Associated Factors among 5-Year-Old Hong Kong Children
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kazeminia, M.; Abdi, A.; Shohaimi, S.; Jalali, R.; Vaisi-Raygani, A.; Salari, N.; Mohammadi, M. Dental caries in primary and permanent teeth in children′s worldwide, 1995 to 2019: A systematic review and meta-analysis. Head Face Med. 2020, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry. Definition of Early Childhood Caries (ECC). Available online: https://www.aapd.org/assets/1/7/d_ecc.pdf (accessed on 21 September 2021).
- Çolak, H.; Dülgergil, Ç.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinanoff, N.; Baez, R.J.; Guillory, C.D.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Department of Health. Oral Health Survey 2001. Available online: https://www.info.gov.hk/gia/general/200212/12/1212128.htm (accessed on 21 September 2021).
- Wei, S.H.; Holm, A.K.; Tong, L.S.; Yuen, S.W. Dental caries prevalence and related factors in 5-year-old children in Hong Kong. Pediatr. Dent. 1993, 15, 116–119. [Google Scholar] [PubMed]
- Chu, C.H.; Fung, D.S.H.; Lo, E.C.M. Dental caries status of preschool children in Hong Kong. Br. Dent. J. 1999, 187, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Lo, E.C.M.; Loo, E.K.Y.; Lee, C. Dental health status of Hong Kong preschool children. Hong Kong Dent. J. 2009, 6, 6–12. [Google Scholar]
- Chu, C.H.; Ho, P.L.; Lo, E.C.M. Oral health status and behaviours of preschool children in Hong Kong. BMC Public Health 2012, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.J.; Gao, S.S.; Duangthip, D.; Li, S.K.Y.; Lo, E.C.M.; Chu, C.H. Dental caries status and its associated factors among 5-year-old Hong Kong children: A cross-sectional study. BMC Oral Health 2017, 17, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, H.H.; Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. A Kindergarten-Based Oral Health Preventive Approach for Hong Kong Preschool Children. Healthc. Basel 2020, 8, 545. [Google Scholar] [CrossRef] [PubMed]
- Von Elmg, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. Open 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Census and Statistics Department. Land Area, Mid-Year Population and Population Density by District Council District. Available online: https://www.censtatd.gov.hk/en/EindexbySubject.html?scode=150&pcode=D5320189#section3 (accessed on 10 September 2021).
- Nishi, D.M.; Bratthall, P.D.; Stjernswärd, D.J. How to Calculate the Significant Caries Index (SiC Index). Available online: https://capp.mau.se/media/1017/sic-index-manual.pdf (accessed on 1 September 2021).
- Census and Statistics Department. Hong Kong Annual Digest of Statistics. Available online: https://www.censtatd.gov.hk/en/data/stat_report/product/B1010003/att/B10100032020AN20B0100.pdf (accessed on 10 September 2021).
- Preisser, J.S.; Stamm, J.W.; Long, D.L.; Kincade, M.E. Review and recommendations for zero-inflated count regression modeling of dental caries indices in epidemiological studies. Caries. Res. 2012, 46, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Escobar Paucar, G.M.; Ramírez Puerta, B.S.; Álvarez Sánchez, L.G. Caries patterns in primary dentition in 3-to 5-year-old children. Medellín, Colombia. Rev. Fac. Odontol. 2019, 31, 47–56. [Google Scholar] [CrossRef]
- Lukacs, J.R.; Largaespada, L.L. Explaining sex differences in dental caries prevalence: Saliva, hormones, and ″life-history″ etiologies. Am. J. Hum. 2006, 18, 540–555. [Google Scholar] [CrossRef] [PubMed]
- New Immigrants Project. Available online: https://soco.org.hk/en/projecthome/new-immigrants/ (accessed on 8 October 2021).
- WHO Expert Consultation on Public Health Intervention against Early Childhood Caries: Report of a meeting, Bangkok, Thailand, 26–28 January 2016. Geneva: World Health Organization; 2017 (WHO/NMH/PND/17.1). License: CC BY-NC-SA 3.0 IGO. Available online: https://apps.who.int/iris/bitstream/handle/10665/255627/WHO-NMH-PND-17.1-eng.pdf (accessed on 8 October 2021).
- Hobdell, M.; Clarkson, J.; Petersen, P.; Johnson, N. Global goals for oral health 2020. Int. J. Clin. Dent. 2003, 53, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Lo, G.L.; Bagramian, R.A. Declining prevalence of dental caries in school children in Singapore. Oral Dis. 1997, 32, 121–125. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables (n = 404) | Untreated ECC Prevalence | p-Value 1 | Mean dt (SD) | Mean Rank of dt | p-Value 2 | Mean SiUC (SD) | p-Value 3 |
|---|---|---|---|---|---|---|---|
| All children | 57% | 2.8 (3.8) | 7.1 (3.6) | ||||
| Child lived in district | 0.003 | 0.002 | <0.001 | ||||
| Hong Kong Island a (54) | 43% | 1.5 (2.4) | 163 | a < b | 4.2 (2.5) | a < b, c | |
| Kowloon b (121) | 69% | 3.5 (4.1) | 227 | 8.3 (3.8) | |||
| New Territories c (229) | 55% | 2.7 (3.7) | 199 | 7.1 (3.4) | |||
| Born inmainlandChina | 0.174 | 0.077 | <0.001 | ||||
| Yes a (45) | 56% | 2.6 (3.6) | 198 | 6.8 (3.5) | |||
| No b (357) | 67% | 4.1 (4.8) | 229 | 10.1 (3.2) | a > b | ||
| Sex | 0.480 | 0.256 | 0.369 | ||||
| Boys (216) | 56% | 2.6 (3.6) | 197 | 6.6 (3.6) | |||
| Girls (188) | 59% | 3.0 (3.9) | 209 | 7.7 (3.5) |
| Variables (n = 404) | n (%) | Untreated ECC Prevalence | p-Value | Pairwise Comparison |
|---|---|---|---|---|
| Mother’s education level | <0.001 | a > b | ||
| Secondary school or below a | 282 (70%) | 64% | ||
| Post-secondary school b | 122 (30%) | 41% | ||
| Monthly family income (HK$) | <0.001 | a > b | ||
| Below 15,000 a | 99 (24%) | 72% | ||
| 15,001 to 30,000 a | 201 (50%) | 60% | ||
| Over 30,000 b | 104 (26%) | 39% | ||
| Father’s education level (n = 396) | 0.004 | a > b | ||
| Secondary school or below a | 170 (67%) | 62% | ||
| Post-secondary school b | 130 (33%) | 47% | ||
| Using toothpaste for tooth brushing | 0.032 | |||
| Yes | 43 (11%) | 42% | ||
| No | 361 (89%) | 59% | ||
| Tooth brushing at least twice daily | 0.120 | |||
| Yes | 263 (65%) | 55% | ||
| No | 141 (35%) | 62% | ||
| Snacking more than twice daily | 0.090 | |||
| Yes | 53 (13%) | 68% | ||
| No | 351 (87%) | 56% | ||
| Parents as primary caregiver (n = 403) | 0.740 | |||
| Yes | 287 (71%) | 58% | ||
| No | 116 (29%) | 56% |
| Variables (n = 404) | Mean dt Score (SD) | Mean Rank of dt | p-Value | Pairwise Comparison |
|---|---|---|---|---|
| Mother’s education level | <0.001 | a < b | ||
| Secondary school or below a | 3.3 (3.9) | 219 | ||
| Post-secondary school b | 1.7 (3.1) | 164 | ||
| Monthly family income (HK$) | <0.001 | a > b > c | ||
| Below 15,000 a | 4.1 (4.4) | 240 | ||
| 15,001 to 30,000 b | 2.8 (3.7) | 207 | ||
| Over 30,000 c | 1.4 (2.6) | 157 | ||
| Father’s education level (n = 396) | 0.004 | a > b | ||
| Secondary school or below a | 3.1 (3.9) | 210 | ||
| Post-secondary school | 2.1 (3.4) | 176 | ||
| Snacking more than twice daily | 0.040 | |||
| Yes | 3.9 (4.4) | 232 | ||
| No | 2.6 (3.6) | 198 | ||
| Using toothpaste for tooth brushing | 0.029 | |||
| Yes | 1.7 (2.8) | 167 | ||
| No | 2.9 (3.8) | 207 | ||
| Tooth brushing at least twice daily | 0.072 | |||
| Yes | 2.7 (3.8) | 195 | ||
| No | 3.0 (3.6) | 216 | ||
| Parents as primary caregiver (n = 403) | 0.920 | |||
| Yes | 2.8 (3.8) | 202 | ||
| No | 2.7 (3.6) | 201 |
| Negative Binomial Portion of the Zero-Inflated Negative Binomial Analysis | ||||
|---|---|---|---|---|
| Variables (n = 401) | Incidence Risk Ratio | p-Value # | 95% Confidence Interval | Pairwise Comparison |
| Monthly family income (HK$) | 0.004 | a > c | ||
| * Below 15,000 a | ||||
| 15,001 to 30,000 b | 0.801 | 0.093 | (0.619, 1.037) | |
| Over 30,000 c | 0.589 | 0.005 | (0.408, 0.852) | |
| Zero-Inflated Portion of the Zero-Inflated Negative Binomial Analysis | ||||
| Variables(n = 401) | Odds Ratio | p-Value # | 95%Confidence Interval | Pairwise Comparison |
| Monthly family income (HK$) | 0.011 | c > a | ||
| * Below 15,000 a | ||||
| 15,001 to 30,000 b | 1.770 | 0.123 | (0.857, 3.655) | |
| Over 30,000 c | 3.455 | 0.003 | (1.524, 7.830) | |
| Mother’s education level | 0.007 | |||
| * Secondary school | ||||
| Post-secondary school | 2.211 | (1.238, 3.949) | ||
| Using toothpaste when brushing | 0.044 | |||
| * No | ||||
| Yes | 2.362 | (1.022, 5.463) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, F.M.; Yan, I.G.; Duangthip, D.; Gao, S.S.; Lo, E.C.M.; Chu, C.H. Prevalence of Untreated Early Childhood Caries of 5-Year-Old Children in Hong Kong: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11934. https://doi.org/10.3390/ijerph182211934
Zheng FM, Yan IG, Duangthip D, Gao SS, Lo ECM, Chu CH. Prevalence of Untreated Early Childhood Caries of 5-Year-Old Children in Hong Kong: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(22):11934. https://doi.org/10.3390/ijerph182211934
Chicago/Turabian StyleZheng, Faith Miaomiao, Iliana Gehui Yan, Duangporn Duangthip, Sherry Shiqian Gao, Edward Chin Man Lo, and Chun Hung Chu. 2021. "Prevalence of Untreated Early Childhood Caries of 5-Year-Old Children in Hong Kong: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 22: 11934. https://doi.org/10.3390/ijerph182211934
APA StyleZheng, F. M., Yan, I. G., Duangthip, D., Gao, S. S., Lo, E. C. M., & Chu, C. H. (2021). Prevalence of Untreated Early Childhood Caries of 5-Year-Old Children in Hong Kong: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(22), 11934. https://doi.org/10.3390/ijerph182211934