
Variation of the Occurrence of Physical Restraint Use in the Long-Term Care: A Scoping Review

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
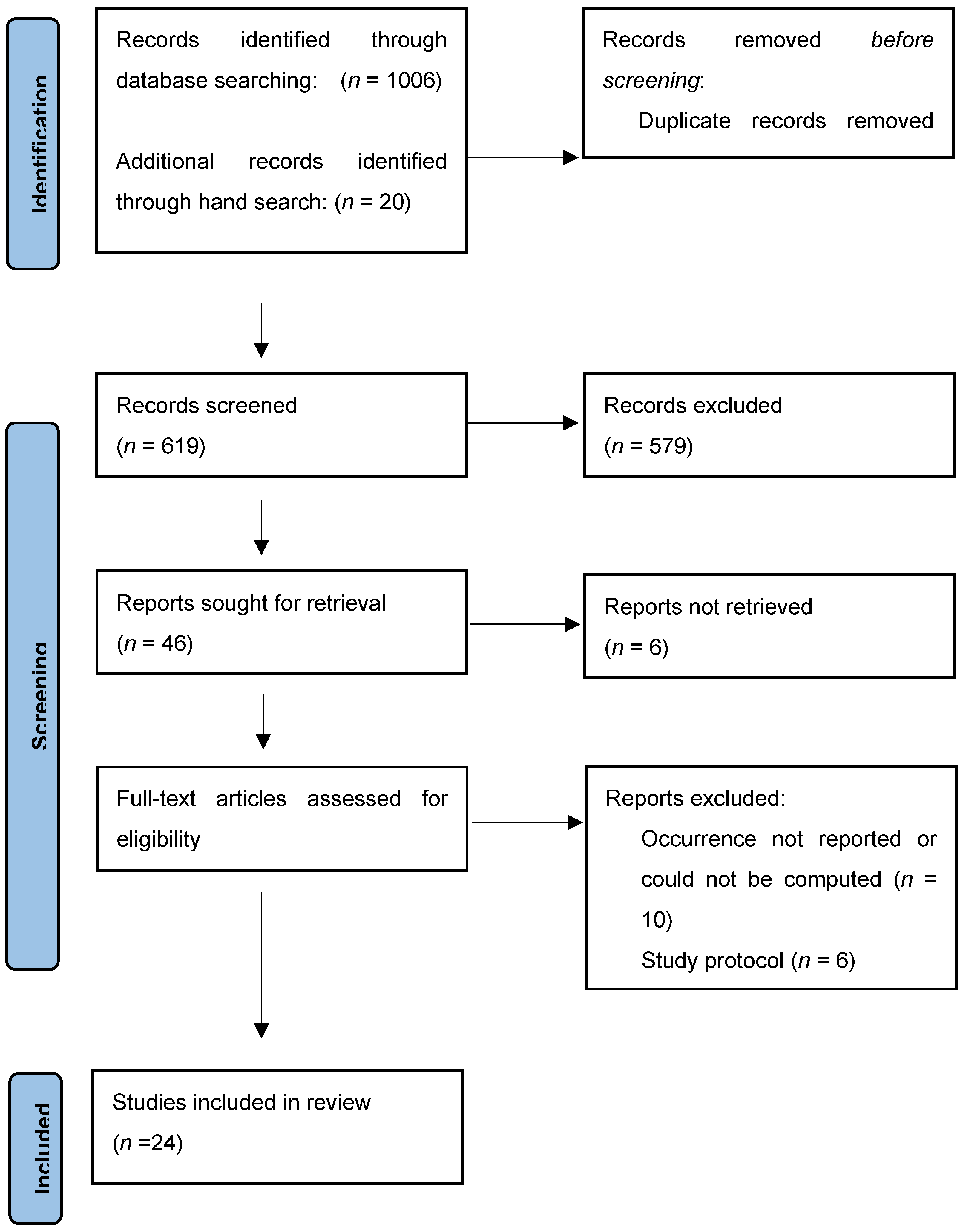
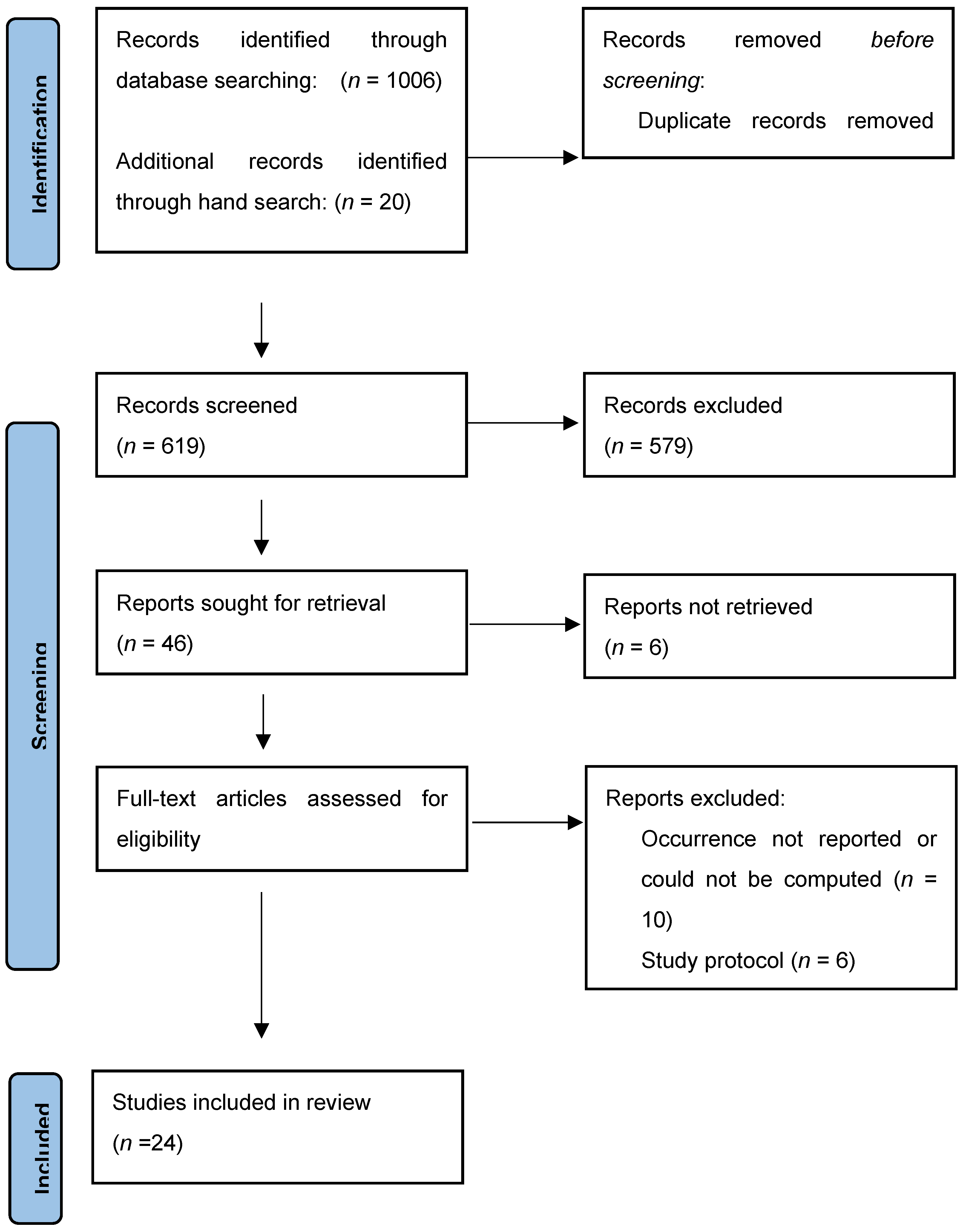
2.2. Identification of Relevant Studies
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Summary of Included Studies
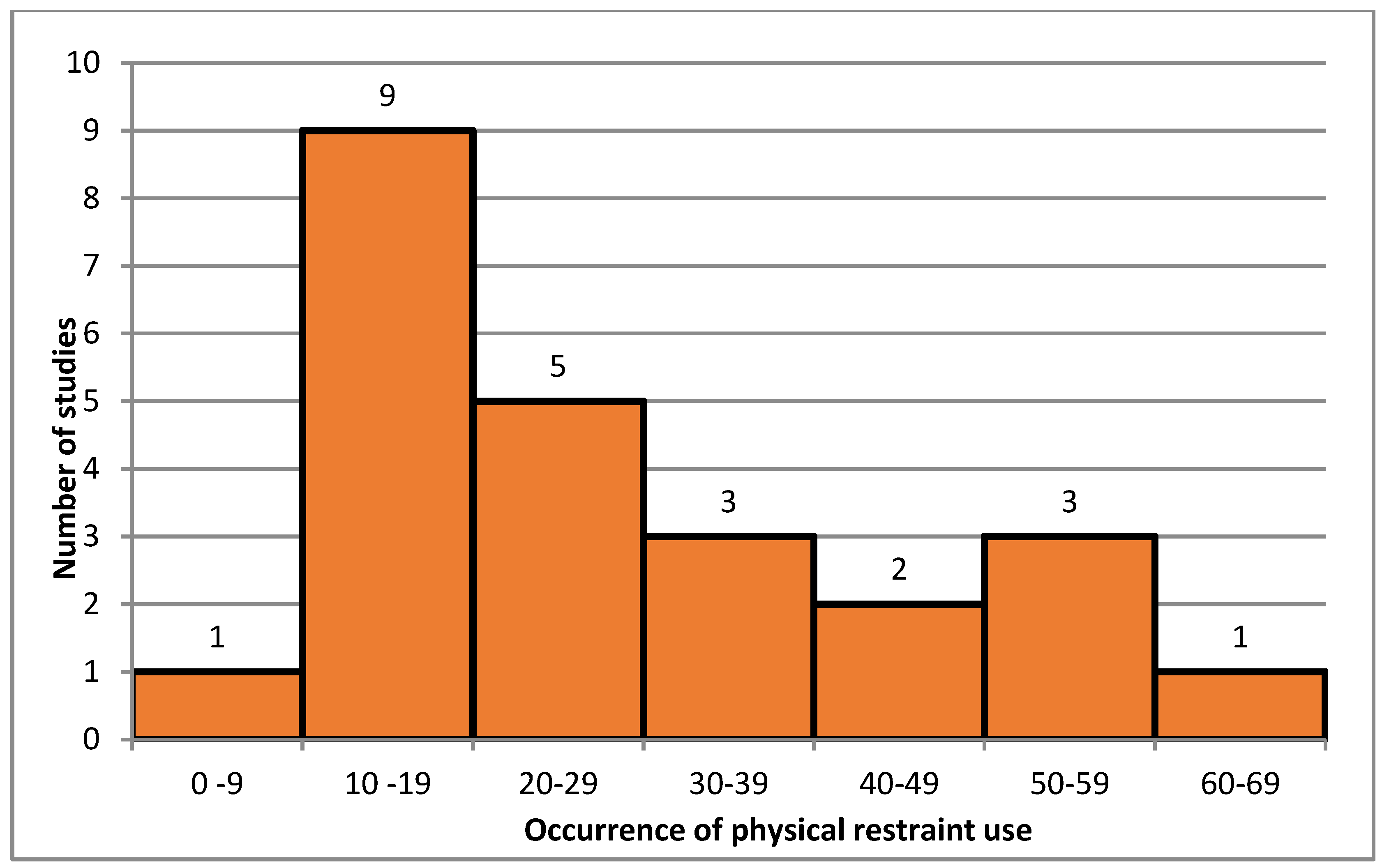
3.2. Occurrence of Physical Restraint Use
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bleijlevens, M.H.; Wagner, L.M.; Capezuti, E.; Hamers, J.P. Physical Restraints: Consensus of a Research Definition Using a Modified Delphi Technique. J. Am. Geriatr. Soc. 2016, 64, 2307–2310. [Google Scholar] [CrossRef]
- Evans, D.; Wood, J.; Lambert, L. A Review of Physical Restraint Minimization in the Acute and Residential Care Settings. J. Adv. Nurs. 2002, 40, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Gallinagh, R.; Nevin, R.; Mc Ilroy, D.; Mitchell, F.; Campbell, L.; Ludwick, R.; McKenna, H. The Use of Physical Restraints as a Safety Measure in the Care of Older People in Four Rehabilitation Wards: Findings from an Exploratory Study. Int. J. Nurs. Stud. 2002, 39, 147–156. [Google Scholar] [CrossRef]
- Luk, E.; Burry, L.; Rezaie, S.; Mehta, S.; Rose, L. Critical Care Nurses’ Decisions Regarding Physical Restraints in Two Canadian Icus: A Prospective Observational Study. Can. J. Crit. Care Nurs. 2015, 26, 16–22. [Google Scholar]
- Via-Clavero, G.; Sanjuán-Naváis, M.; Romero-García, M.; de la Cueva-Ariza, L.; Martínez-Estalella, G.; Plata-Menchaca, E.; Delgado-Hito, P. Eliciting Critical Care Nurses’ Beliefs Regarding Physical Restraint Use. Nurs. Ethics 2019, 26, 1458–1472. [Google Scholar] [CrossRef]
- Benbenbishty, J.; Adam, S.; Endacott, R. Physical Restraint Use in Intensive Care Units across Europe: The Price Study. Intensiv. Crit. Care Nurs. 2010, 26, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Ben Natan, M.; Akrish, O.; Zaltkina, B.; Noy, R.H. Physically Restraining Elder Residents of Long-Term Care Facilities from a Nurses’ Perspective. Int. J. Nurs. Pract. 2010, 16, 499–507. [Google Scholar] [CrossRef]
- Capezuti, E. Minimizing the Use of Restrictive Devices in Dementia Patients at Risk for Falling. Nurs. Clin. N. Am. 2004, 39, 625–647. [Google Scholar] [CrossRef] [PubMed]
- Hamers, J.P.; Huizing, A.R. Why Do We Use Physical Restraints in the Elderly? Z. Gerontol. Geriatr. 2005, 38, 19–25. [Google Scholar] [CrossRef]
- Huizing, A.R.; Hamers, J.P.; de Jonge, J.; Candel, M.; Berger, M.P. Organisational Determinants of the Use of Physical Restraints: A Multilevel Approach. Soc. Sci. Med. 2007, 65, 924–933. [Google Scholar] [CrossRef]
- Hofmann, H.; Schorro, E.; Haastert, B.; Meyer, G. Use of Physical Restraints in Nursing Homes: A Multicentre Cross-Sectional Study. BMC Geriatr. 2015, 15, 129. [Google Scholar] [CrossRef] [Green Version]
- Dunn, K.S. The Effect of Physical Restraints on Fall Rates in Older Adults Who Are Institutionalized. J. Gerontol. Nurs. 2001, 27, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Hirdes, J.P.; Smith, T.F.; Finne-Soveri, H.; Chi, I.; Du Pasquier, J.N.; Gilgen, R.; Ikegami, N.; Mor, V. Use of Physical Restraints and Antipsychotic Medications in Nursing Homes: A Cross-National Study. Int. J. Geriatr. Psychiatry 2009, 24, 1110–1118. [Google Scholar] [CrossRef]
- Marek, K.D.; Rantz, M.J.; Fagin, C.M.; Krejci, J.W. Obra ’87: Has It Resulted in Better Quality of Care? J. Gerontol. Nurs. 1996, 22, 28–36. [Google Scholar] [CrossRef]
- Lee, D.A.; Robins, L.M.; Bell, J.S.; Srikanth, V.; Möhler, R.; Hill, K.D.; Griffiths, D.; Haines, T.P. Prevalence and Variability in Use of Physical and Chemical Restraints in Residential Aged Care Facilities: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2021, 117, 103856. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K.; Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Daudt, H.M.L.; van Mossel, C.; Scott, S.J. Enhancing the Scoping Study Methodology: A Large, Inter-Professional Team’s Experience with Arksey and O’malley’s Framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- Meyer, G.; Köpke, S.; Haastert, B.; Mühlhauser, I. Restraint Use among Nursing Home Residents: Cross-Sectional Study and Prospective Cohort Study. J. Clin. Nurs. 2009, 18, 981–990. [Google Scholar] [CrossRef]
- Aranda-Gallardo, M.; Morales-Asencio, J.M.; Enriquez de Luna-Rodriguez, M.; Vazquez-Blanco, M.J.; Morilla-Herrera, J.C.; Rivas-Ruiz, F.; Toribio-Montero, J.C.; Canca-Sanchez, J.C. Characteristics, Consequences and Prevention of Falls in Institutionalised Older Adults in the Province of Malaga (Spain): A Prospective, Cohort, Multicentre Study. BMJ Open 2018, 8, e020039. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, A.; Bedin, M.; Stocco, S.; Negrin, V.; Biancon, A.; Cecchetto, G.; Tagliapietra, M. Clinical Outcomes and Complications of Enteral Nutrition among Older Adults. Minerva Med. 2009, 100, 159–166. [Google Scholar] [PubMed]
- Te Boekhorst, S.; Depla, M.F.; Francke, A.L.; Twisk, J.W.; Zwijsen, S.A.; Hertogh, C.M. Quality of Life of Nursing-Home Residents with Dementia Subject to Surveillance Technology Versus Physical Restraints: An Explorative Study. Int. J. Geriatr. Psychiatry 2013, 28, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Foebel, A.D.; Onder, G.; Finne-Soveri, H.; Lukas, A.; Denkinger, M.D.; Carfi, A.; Vetrano, D.L.; Brandi, V.; Bernabei, R.; Liperoti, R. Physical Restraint and Antipsychotic Medication Use among Nursing Home Residents with Dementia. J. Am. Med. Dir. Assoc. 2016, 17, 184.e9–184.e14. [Google Scholar] [CrossRef]
- Gulpers, M.J.; Bleijlevens, M.H.; Ambergen, T.; Capezuti, E.; Van Rossum, E.; Hamers, J.P. Belt Restraint Reduction in Nursing Homes: Effects of a Multicomponent Intervention Program. J. Am. Geriatr. Soc. 2011, 59, 2029–2036. [Google Scholar] [CrossRef]
- Gulpers, M.J.; Bleijlevens, M.H.; Capezuti, E.; Van Rossum, E.; Ambergen, T.; Hamers, J.P. Preventing Belt Restraint Use in Newly Admitted Residents in Nursing Homes: A Quasi-Experimental Study. Int. J. Nurs. Stud. 2012, 49, 1473–1479. [Google Scholar] [CrossRef]
- Gulpers, M.J.; Bleijlevens, M.H.; Ambergen, T.; Capezuti, E.; Van Rossum, E.; Hamers, J.P. Reduction of Belt Restraint Use: Long-Term Effects of the Exbelt Intervention. J. Am. Geriatr. Soc. 2013, 61, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Heeren, P.; Van de Water, G.; De Paepe, L.; Boonen, S.; Vleugels, A.; Milisen, K. Staffing Levels and the Use of Physical Restraints in Nursing Homes: A Multicenter Study. J. Gerontol. Nurs. 2014, 40, 48–54. [Google Scholar] [CrossRef]
- Heinze, C.; Dassen, T.; Grittner, U. Use of Physical Restraints in Nursing Homes and Hospitals and Related Factors: A Cross-Sectional Study. J. Clin. Nurs. 2012, 21, 1033–1040. [Google Scholar] [CrossRef]
- Huizing, A.R.; Hamers, J.P.; Gulpers, M.J.; Berger, M.P. A Cluster-Randomized Trial of an Educational Intervention to Reduce the Use of Physical Restraints with Psychogeriatric Nursing Home Residents. J. Am. Geriatr. Soc. 2009, 57, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Koczy, P.; Becker, C.; Rapp, K.; Klie, T.; Beische, D.; Büchele, G.; Kleiner, A.; Guerra, V.; Rissmann, U.; Kurrle, S.; et al. Effectiveness of a Multifactorial Intervention to Reduce Physical Restraints in Nursing Home Residents. J. Am. Geriatr. Soc. 2011, 59, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Köpke, S.; Mühlhauser, I.; Gerlach, A.; Haut, A.; Haastert, B.; Möhler, R.; Meyer, G. Effect of a Guideline-Based Multicomponent Intervention on Use of Physical Restraints in Nursing Homes: A Randomized Controlled Trial. JAMA 2012, 307, 2177–2184. [Google Scholar] [CrossRef] [Green Version]
- Morichi, V.; Fedecostante, M.; Morandi, A.; Di Santo, S.G.; Mazzone, A.; Mossello, E.; Bo, M.; Bianchetti, A.; Rozzini, R.; Zanetti, E.; et al. A Point Prevalence Study of Delirium in Italian Nursing Homes. Dement. Geriatr. Cogn. Disord. 2018, 46, 27–41. [Google Scholar] [CrossRef]
- Muñiz, R.; Gómez, S.; Curto, D.; Hernández, R.; Marco, B.; García, P.; Tomás, J.F.; Olazarán, J. Reducing Physical Restraints in Nursing Homes: A Report from Maria Wolff and Sanitas. J. Am. Med. Dir. Assoc. 2016, 17, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Pellfolk, T.J.; Gustafson, Y.; Bucht, G.; Karlsson, S. Effects of a Restraint Minimization Program on Staff Knowledge, Attitudes, and Practice: A Cluster Randomized Trial. J. Am. Geriatr. Soc. 2010, 58, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Testad, I.; Ballard, C.; Brønnick, K.; Aarsland, D. The Effect of Staff Training on Agitation and Use of Restraint in Nursing Home Residents with Dementia: A Single-Blind, Randomized Controlled Trial. J. Clin. Psychiatry 2010, 71, 80–86. [Google Scholar] [CrossRef]
- Testad, I.; Mekki, T.E.; Førland, O.; Øye, C.; Tveit, E.M.; Jacobsen, F.; Kirkevold, Ø. Modeling and Evaluating Evidence-Based Continuing Education Program in Nursing Home Dementia Care (Medced)—Training of Care Home Staff to Reduce Use of Restraint in Care Home Residents with Dementia. A Cluster Randomized Controlled Trial. Int. J. Geriatr. Psychiatry 2016, 31, 24–32. [Google Scholar] [CrossRef]
- Verbeek, H.; Zwakhalen, S.M.; van Rossum, E.; Ambergen, T.; Kempen, G.I.; Hamers, J.P. Effects of Small-Scale, Home-Like Facilities in Dementia Care on Residents’ Behavior, and Use of Physical Restraints and Psychotropic Drugs: A Quasi-Experimental Study. Int. Psychogeriatr. 2014, 26, 657–668. [Google Scholar] [CrossRef]
- Willemse, B.M.; de Jonge, J.; Smit, D.; Dasselaar, W.; Depla, M.F.; Pot, A.M. Is an Unhealthy Work Environment in Nursing Home Care for People with Dementia Associated with the Prescription of Psychotropic Drugs and Physical Restraints? Int. Psychogeriatr. 2016, 28, 983–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuronen, M.; Kautiainen, H.; Karppi, P.; Hartikainen, S.; Koponen, H. Physical Restraints and Associations with Neuropsychiatric Symptoms and Personal Characteristics in Residential Care: A Cross-Sectional Study. Int. J. Geriatr. Psychiatry 2017, 32, 1418–1424. [Google Scholar] [CrossRef] [PubMed]
- (RNAO), The Registered Nurses’ Association of Ontario. Promoting Safety: Alternative Approaches to the Use of Restraints; RNAO: Toronto, ON, Canada, 2012. [Google Scholar]
- Øye, C.; Jacobsen, F.F.; Mekki, T.E. Do Organisational Constraints Explain the Use of Restraint? A Comparative Ethnographic Study from Three Nursing Homes in Norway. J. Clin. Nurs. 2017, 26, 1906–1916. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, H.; Hahn, S. Characteristics of Nursing Home Residents and Physical Restraint: A Systematic Literature Review. J. Clin. Nurs. 2014, 23, 3012–3024. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | N. Studies | Median Occurrence (%) | IQR | p-Value | |
|---|---|---|---|---|---|
| Overall | 24 | 100% | 26.39 | (6.7–40.4) | |
| European Countries | - | ||||
| Netherlands | 8 | 33.3% | 41.7 | (26.9–57.3) | |
| Germany | 4 | 16.7% | 27.2 | (21.6–29.3) | |
| Norway | 2 | 8.3% | 26.5 | (21.5–31.6) | |
| Spain | 2 | 8.3% | 14.8 | (13.8–15.8) | |
| Italy | 2 | 8.3% | 19.0 | (13.7–24.4) | |
| Belgium | 1 | 4.2% | 47.5 | (47.5–47.5) | |
| Sweden | 1 | 4.2% | 25.3 | (25.3–25.3) | |
| Swiss | 1 | 4.2% | 26.7 | (26.7–26.7) | |
| Finland | 1 | 4.2% | 52.0 | (52.0–52.0) | |
| Combinations | 2 | 8.3% | 18.3 | (17.7–18.9) | |
| Year of publication | 0.841 $ | ||||
| 2009–2013 | 14 | 58.3% | 27.2 | (17.6- 35.7) | |
| 2014–2019 | 10 | 41.7% | 23.2 | (16.7–43.4) | |
| Study design | 0.125 † | ||||
| Cross-sectional | 8 | 33% | 29.9 | (23.8–40.7) | |
| Randomized Controlled Trial | 6 | 25% | 26,7 | (18.7–34.5) | |
| Quasi-experimental | 5 | 21% | 45.0 | (29.5–59.2) | |
| Cohort | 5 | 21% | 16.8 | (14.5–19.1) | |
| Data sources | 0.149 † | ||||
| Chart review/Electronic records | 7 | 29% | 36.6 | (20.1–43.0) | |
| Observation | 9 | 38% | 29.5 | (26.0–56.6) | |
| Standardized scale and interview | 4 | 17% | 16.8 | (15.2– 17.5) | |
| Combinations | 4 | 17% | 18.2 | (16.2–25.9) | |
| Sample size | 0.473 † | ||||
| 100–299 | 8 | 33% | 33.0 | (16.0–47.9) | |
| 300–999 | 5 | 21% | 25.3 | (19.6–47.5) | |
| 1000+ | 11 | 46% | 26.3 | (15.1–30.5) | |
| Average age of enrolled patients | 0.742 $ | ||||
| <85 years | 16 | 66.7% | 27.0 | (16.2–46.7) | |
| >85 years | 8 | 33.3% | 23.2 | (18.4–33.9) | |
| Sex percentage | - | ||||
| Mostly females > 50% | 24 | 100% | 26.4 | (16.7–40.1) | |
| Mostly males >50% | -- | -- | - | - | |
| Health care setting | 0.04 $ | ||||
| Nursing home and long-term care | 18 | 75% | 22.5 | (16.6–31.8) | |
| Psychogeriatric units | 6 | 25% | 50.8 | (33.4–58.5) | |
| Physical restraint role | 0.009 $ | ||||
| Outcome | 18 | 75% | 31.2 | (25.6–46.9) | |
| Covariate | 6 | 25% | 15.7 | (13.7–18.5) | |
| Definition of physical restraint | 0.002 † | ||||
| Bed rails included | 11 | 45.8% | 36.6 | (28.8–54.3) | |
| Bed rails excluded | 10 | 41.7% | 16.9 | (13.7–23.8) | |
| Not specified | 3 | 12.5% | 14.5 | (13.9–17.1) | |
| Presence of dementia in enrolled patients | - | ||||
| Dementia/cognitive impairment (from mild to severe) | 16 | 66.7% | 93.9 | (62.1–100.0) | |
| Not reported | 8 | 33.3% | - | - | |
| Presence of ADLs dependence in enrolled patients | 0.002 † | ||||
| No | 4 | 16.67% | 8.0 | (5.7–13.2) | |
| Mild | 9 | 37.5% | 7.2 | (5.0–30.0) | |
| Severe | 8 | 33.3% | 39.7 | (37.1- 42.5) | |
| Very severe | 11 | 45.8% | 53.8 | (21.9- 64.5) | |
| Not reported | 13 | 54.2% | - | - | |
| Use of drugs in enrolled patients | 0.014 † | ||||
| Antipsychotics/neuroleptics | 7 | 29.1% | 44.7 | (36.-67.5) | |
| Benzodiazepines | 7 | 29.1% | 29.1 | (20.8–33.9) | |
| Psychoactive drugs (not specified) | 9 | 37.5% | 68.2 | (53.5–70.2) | |
| Not reported | 8 | 33.3% | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambrosi, E.; Debiasi, M.; Longhini, J.; Giori, L.; Saiani, L.; Mezzalira, E.; Canzan, F. Variation of the Occurrence of Physical Restraint Use in the Long-Term Care: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11918. https://doi.org/10.3390/ijerph182211918
Ambrosi E, Debiasi M, Longhini J, Giori L, Saiani L, Mezzalira E, Canzan F. Variation of the Occurrence of Physical Restraint Use in the Long-Term Care: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(22):11918. https://doi.org/10.3390/ijerph182211918
Chicago/Turabian StyleAmbrosi, Elisa, Martina Debiasi, Jessica Longhini, Lorenzo Giori, Luisa Saiani, Elisabetta Mezzalira, and Federica Canzan. 2021. "Variation of the Occurrence of Physical Restraint Use in the Long-Term Care: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 22: 11918. https://doi.org/10.3390/ijerph182211918
APA StyleAmbrosi, E., Debiasi, M., Longhini, J., Giori, L., Saiani, L., Mezzalira, E., & Canzan, F. (2021). Variation of the Occurrence of Physical Restraint Use in the Long-Term Care: A Scoping Review. International Journal of Environmental Research and Public Health, 18(22), 11918. https://doi.org/10.3390/ijerph182211918