
Effects of Mindfulness-Based Stress Reduction (MBSR) on Stress, Heart Rate Variability, Affect, and Wellbeing among People with Schizophrenia


Abstract
1. Introduction
2. Materials and Methods
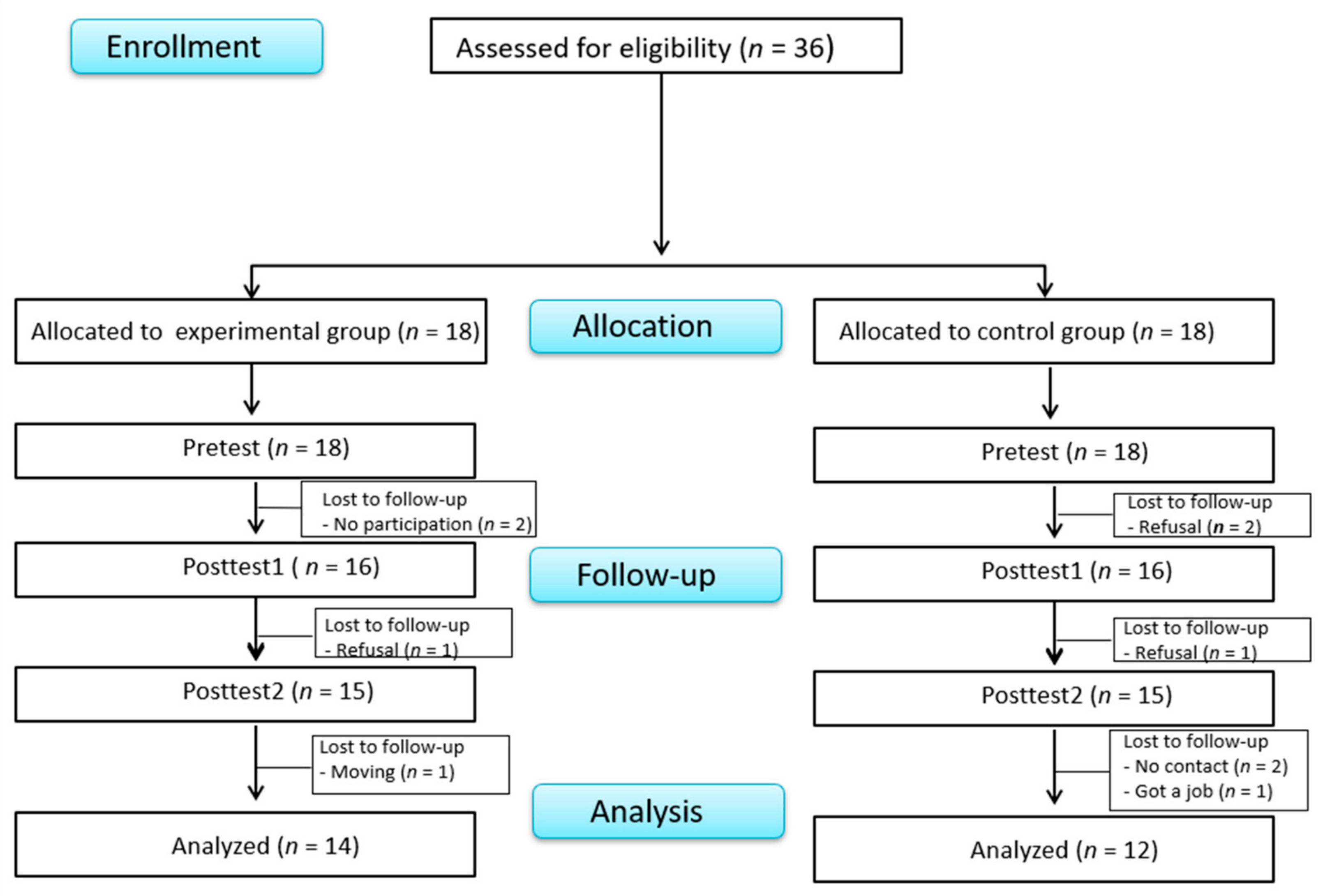
2.1. Study Design and Participants
2.2. MBSR Program
2.3. Measures
2.3.1. Perceived Stress
2.3.2. Heart Rate Variability (HRV)
2.3.3. The Positive and Negative Affect Schedule (PANAS)
2.3.4. Subjective Wellbeing
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Baseline Characteristics and Between-Group Differences
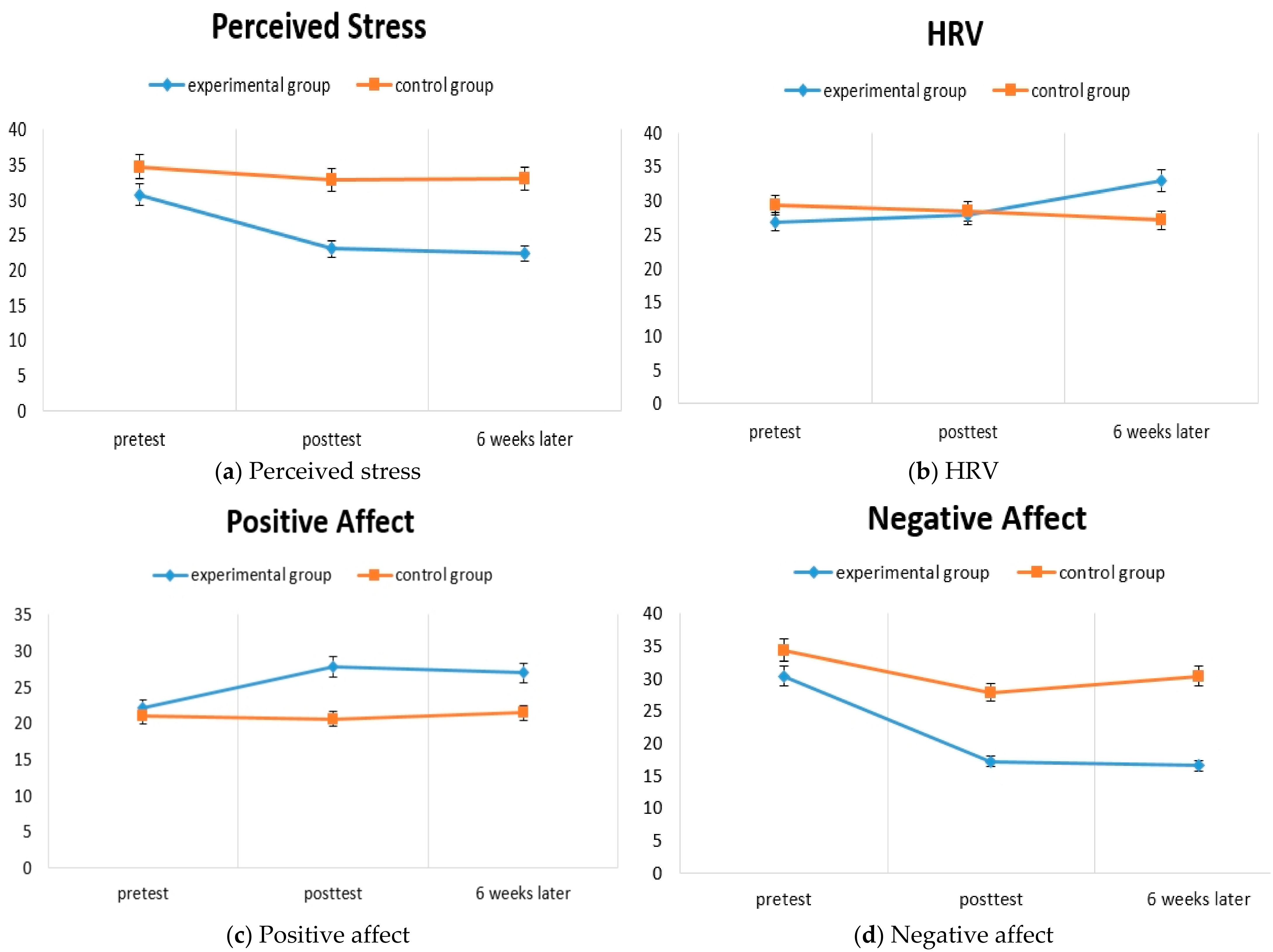
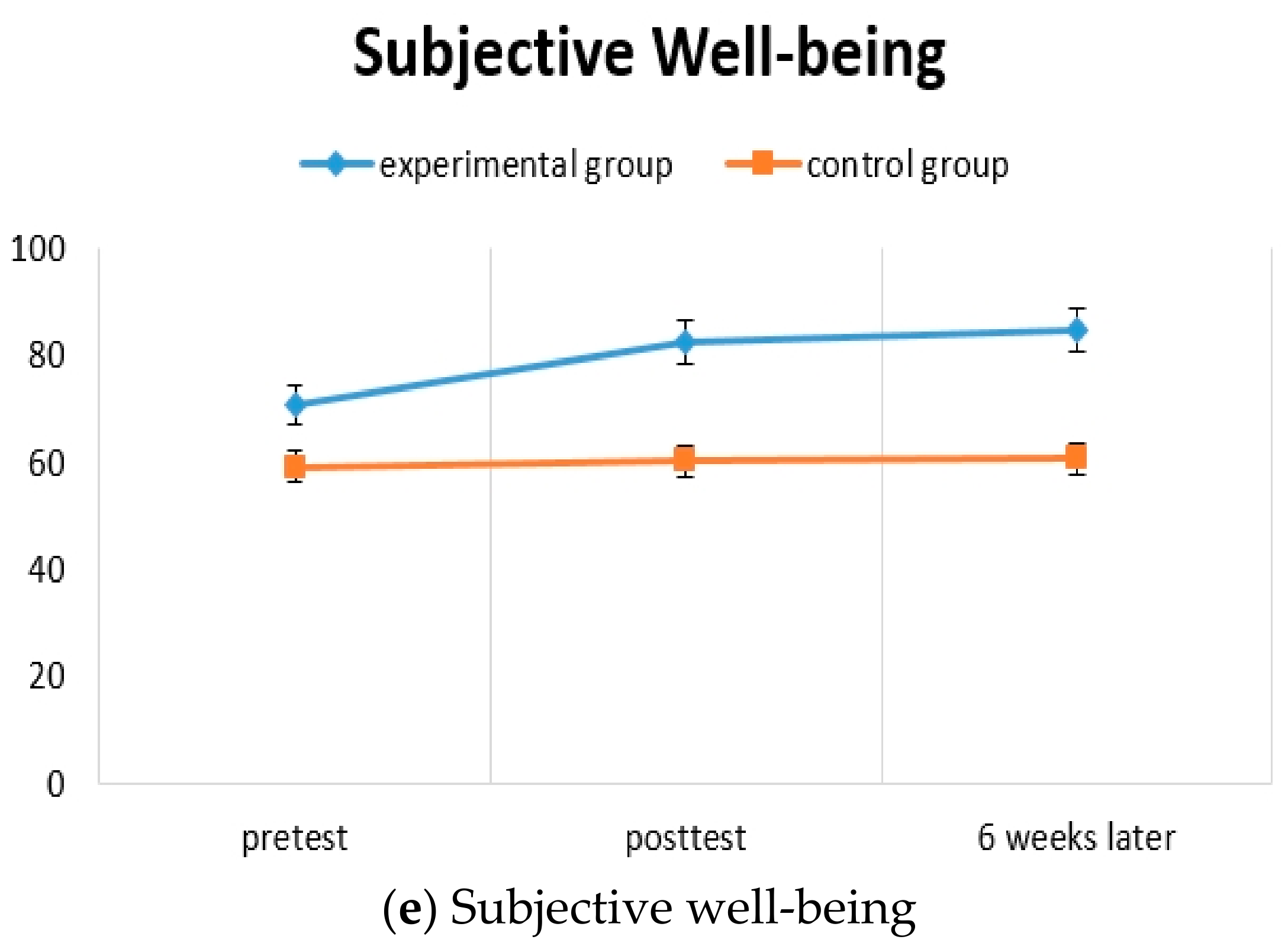
3.2. Hypothesis Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Pre-Test | Posttest 1 (Post 8 Weeks) | Posttest 2 (Post 14 Weeks) | Source | F (df1, df2) | p | Differences (Post 1-Pre) | Differences (Post 2-Pre) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | M ± SD | t (df) | p | M ± SD | t (df) | p | |||||
| Perceived Stress | Exp. | 30.71 ± 6.56 | 23.00 ± 5.17 | 22.36 ± 4.60 | G | 17.69 (1, 24) | <0.001 | −7.71 ± 5.89 | −2.63 (25) | 0.015 | −8.35 ± 5.60 | −2.87 (25) | 0.008 |
| Cont. | 34.67 ± 4.23 | 32.83 ± 5.84 | 33.00 ± 7.23 | T | 9.17 (1.26, 30.26) | 0.001 | −1.84 ± 5.46 | −1.67 ± 6.29 | |||||
| G × T | 3.95 (1.26, 30.26) | 0.034 | |||||||||||
| HRV | Exp. | 26.82 ± 16.70 | 27.90 ± 12.69 | 32.98 ± 14.43 | G | 0.48 (1, 24) | 0.848 | 1.08 ± 16.01 | 0.40 (25) | 0.691 | 6.16 ± 12.39 | 2.00 (25) | 0.057 |
| Cont. | 29.34 ± 15.43 | 28.36 ± 12.05 | 27.13 ± 12.00 | T | 1.08 (1.57, 37.61) | 0.356 | −0.98 ± 8.42 | −2.21 ± 8.04 | |||||
| G × T | 3.66 (1.57, 37.61) | 0.042 | |||||||||||
| Positive Affect | Exp. | 22.14 ± 5.63 | 27.79 ± 9.42 | 27.00 ± 8.81 | G | 4.67 (1, 24) | 0.045 | 5.65 ± 7.50 | 1.76 (25) | 0.090 | 4.86 ± 7.56 | 1.19 (25) | 0.246 |
| Cont. | 21.00 ± 4.80 | 20.58 ± 8.96 | 21.41 ± 10.19 | T | 1.11 (1.17, 28.11) | 0.346 | −0.42 ± 10.00 | 0.41 ± 11.37 | |||||
| G × T | 2.47 (1.17, 28.11) | 0.107 | |||||||||||
| Negative Affect | Exp. | 30.36 ± 6.54 | 17.21 ± 5.26 | 16.50 ± 4.45 | G | 2.91 (1, 24) | 0.101 | −13.15 ± 9.26 | −1.87 (25) | 0.074 | −13.86 ± 7.60 | −3.02 (25) | 0.006 |
| Cont. | 34.33 ± 4.52 | 27.83 ± 9.81 | 30.33 ± 8.64 | T | 24.35 (2, 48) | <0.001 | −6.50 ± 8.77 | −4.00 ± 9.08 | |||||
| G × T | 4.55 (2, 48) | 0.022 | |||||||||||
| Subjective Well-being | Exp. | 70.64 ± 17.43 | 82.35 ± 16.82 | 84.71 ± 15.24 | G | 12.21 (1, 24) | 0.002 | 11.71 ± 17.83 | 1.39 (25) | 0.177 | 14.07 ± 16.56 | 1.81 (25) | 0.083 |
| Cont. | 59.00 ± 9.69 | 60.25 ± 19.97 | 60.66 ± 19.15 | T | 2.78 (1.33, 31.88) | 0.083 | 1.25 ± 20.54 | 1.67 ± 18.37 | |||||
| G × T | 1.69 (1.33, 31.88) | 0.207 | |||||||||||
References
- Moreno-Küstner, B.; Martin, C.; Pastor, L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS ONE 2018, 13, e0195687. [Google Scholar] [CrossRef]
- Kim, S.W. Psychosocial intervention for patients with schizophrenia. J. Korean Neuropsychiatr. Assoc. 2018, 57, 235–243. [Google Scholar] [CrossRef]
- Kumar, S.; Mohanty, S. Factors associated with self-esteem in patients with chronic schizophrenia. SIS J. Proj. Psychol. Ment. Health 2016, 23, 56–60. [Google Scholar]
- Lee, H.Y.; Ham, B.J. Stress and mental illness. J. Korean Med. Assoc. 2013, 56, 471–477. [Google Scholar] [CrossRef][Green Version]
- OECD [Organization for Economic Cooperation and Development]. Health Statistics; OECD: Paris, France, 2015. [Google Scholar]
- Mitchell, A.J.; Vancampfort, D.; Sweers, K.; van Winkel, R.; Yu, W.; De Hert, M. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders—A systematic review and meta-analysis. Schizophr. Bull. 2011, 39, 306–331. [Google Scholar] [CrossRef]
- Lee, J.-S.; Yoon, B.-H.; Song, J.-H.; Hea, Y.-H. The Effect of Weight Reduction on the Obesity-Related Quality of Life, Physical and Emotional Well-Being in Obese Schizophrenic Inpatients. Korean J. Psychopharmacol. 2012, 23, 190–199. [Google Scholar]
- Kim, M.Y.; Jun, S.S. Development and Effects of a Cognitive-behavioral Therapy Based Program in Reducing Internalized Stigma in Patients with Schizophrenia. J. Korean Acad. Nurs. 2016, 46, 349–363. [Google Scholar] [CrossRef]
- Schultz, S.H.; North, S.W.; Shields, C.G. Schizophrenia: A review. Am. Fam. Physician 2007, 75, 1821–1829. [Google Scholar] [PubMed]
- Wang, L.Q.; Chien, W.T.; Yip, L.K.; Karatzias, T. A randomized controlled trial of a mindfulness-based intervention program for people with schizophrenia: 6-month follow-up. Neuropsychiatr. Dis. Treat. 2016, 12, 3097. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, P.; Taylor, K.N.; Abba, N. Mindfulness groups for people with psychosis. Behav. Cogn. Psychother. 2005, 33, 351–359. [Google Scholar] [CrossRef]
- van der Valk, R.; van de Waerdt, S.; Meijer, C.J.; van den Hout, I.; de Haan, L. Feasibility of mindfulness-based therapy in patients recovering from a first psychotic episode: A pilot study. Early Interv. Psychiatry 2013, 7, 64–70. [Google Scholar] [CrossRef]
- Wahbeh, H.; Nelson, M. iRest meditation for older adults with depression symptoms: A pilot study. Int. J. Yoga Ther. 2019, 29, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Henderson, V.P.; Clemow, L.; Massion, A.O.; Hurley, T.G.; Druker, S.; Hébert, J.R. The effects of mindfulness-based stress reduction on psychosocial outcomes and quality of life in early-stage breast cancer patients: A randomized trial. Breast Cancer Res. Treat. 2012, 131, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.C.; Park, E.J. PT746. The Effect of Mindfulness Meditation Programs on Perceived Stress and Quality of Life of Mental Health Professionals: A Pilot Study. Int. J. Neuropsychopharmacol. 2016, 19 (Suppl. S1), 71. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Chapleau, M.-A.; Paquin, K.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Eberth, J.; Sedlmeier, P. The effects of mindfulness meditation: A meta-analysis. Mindfulness 2012, 3, 174–189. [Google Scholar] [CrossRef]
- Shawyer, F.; Farhall, J.; Mackinnon, A.; Trauer, T.; Sims, E.; Ratcliff, K.; Larner, C.; Thomas, N.; Castle, D.; Mullen, P.; et al. A randomised controlled trial of acceptance-based cognitive behavioural therapy for command hallucinations in psychotic disorders. Behav. Res. Ther. 2012, 50, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A. (Ed.) Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Santorelli, S.; Kabat-Zinn, J. (Eds.) Mindfulness-Based Stress Reduction Professional Training: Scientific Papers from the Stress Reduction Clinic and the Center for Mindfulness in Medicine, Health Care, and Society 2001–1982; Center for Mindfulness in Medicine, Health Care, and Society: Worcester, MA, USA, 2014. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Hodann-Caudevilla, R.M.; Díaz-Silveira, C.; Burgos-Julián, F.A.; Santed, M.A. Mindfulness-based interventions for people with schizophrenia: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 4690. [Google Scholar] [CrossRef]
- Liu, Y.-C.; Li, I.-L.; Hsiao, F.-H. Effectiveness of mindfulness-based intervention on psychotic symptoms for patients with schizophrenia: A meta-analysis of randomized controlled trials. J. Adv. Nurs. 2021, 77, 2565–2580. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 59, 52–60. [Google Scholar] [CrossRef]
- Kuijpers, H.J.; Van der Heijden, F.; Tuinier, S.; Verhoeven, W.M.A. Meditation-induced psychosis. Psychopathology 2007, 40, 461–464. [Google Scholar] [CrossRef]
- Jung, C.Y.; Kim, S.H.; Lee, W.K.; Kim, W.Y. The effects of meditation program combining mindfulness and compassion meditation on emotional state of chronic inpatients with schizophrenia: Pilot study. J. Korean Assoc. Soc. Psychiatry 2011, 16, 66–73. [Google Scholar]
- Kim, S.H.; Lee, Y.K. The effects of mindfulness based group intervention on negative symptom, emotional state, and ward behavior with chronic schizophrenia: A preliminary study. Korean J. Schizophr. Res. 2011, 14, 27–33. [Google Scholar]
- Song, J.Y.; Kim, K.T.; Lee, S.K.; Kim, Y.H.; Noh, J.H.; Kim, J.W.; Chang, W.I.; Bahn, G.H.; Kang, W.S. Reliability and validity of the Korean version of the scale to assessment unawareness of mental disorder (SUMD-K). J. Korean Neuropsychiatr. Assoc. 2006, 45, 307–315. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- la Cour, P.; Petersen, M. Effects of mindfulness meditation on chronic pain: A randomized controlled trial. Pain Med. 2015, 16, 641–652. [Google Scholar] [CrossRef]
- Son, M.A.; Lee, Y.M.; Jung, K.A. The effects of a combined exercise program on obesity and metabolic syndrome factors for chronic psychiatric inpatients. J. Korean Biol. Nurs. Sci. 2014, 16, 105–112. [Google Scholar] [CrossRef]
- Stahl, B.; Goldstein, E. A Mindfulness-Based Stress Reduction Workbook; New Harbinger Publications: Oakland, CA, USA, 2010. [Google Scholar]
- Shapiro, S.L.; Schwartz, G.E.R. Intentional systemic mindfulness: An integrative model for self-regulation and health. Adv. Mind-Body Med. 2000, 16, 128–134. [Google Scholar] [PubMed]
- Arch, J.J.; Ayers, C.R.; Baker, A.; Almklov, E.; Dean, D.J.; Craske, M.G. Randomized clinical trial of adapted mindfulness-based stress reduction versus group cognitive behavioral therapy for heterogeneous anxiety disorders. Behav. Res. Ther. 2013, 51, 185–196. [Google Scholar] [CrossRef]
- Park, J.O.; Seo, Y.S. Validation of the perceived stress scale (PSS) on samples of Korean university students. Korean J. Psychol. Gen. 2010, 29, 611–629. [Google Scholar]
- Cohen, F. Coping. Behavioral Health: A Handbook of Health Enhancement and Disease Prevention; Wiley: New York, NY, USA, 1984. [Google Scholar]
- Lim, Y.J.; Yu, B.H.; Kim, D.K.; Kim, J.H. The positive and negative affect schedule: Psychometric properties of the Korean version. Psychiatry Investig. 2010, 7, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Kim, S.W.; Shin, I.S.; Kim, J.M.; Yoo, J.A.; Ahn, Y.M.; Kwon, J.S.; Yang, S.J.; Yoon, J.S. A validation study of the Korean version of the subjective well-being under neuroleptic treatment scale-short form. Korean J. Psychopharmacol. 2007, 18, 221–230. [Google Scholar]
- Naber, D.; Moritz, S.; Lambert, M.; Rajonk, F.; Holzbach, R.; Mass, R.; Andresen, B.; Frank, P.; Rüdiger, H.; Reinhard, M.; et al. Improvement of schizophrenic patients’ subjective well-being under atypical antipsychotic drugs. Schizophr. Res. 2001, 50, 79–88. [Google Scholar] [CrossRef]
- Kolahkaj, B.; Zargar, F. Effect of mindfulness-based stress reduction on anxiety, depression and stress in women with multiple sclerosis. Nurs. Midwifery Stud. 2015, 4, e29655. [Google Scholar] [CrossRef] [PubMed]
- Marzabadi, E.A.; Zadeh, S.M.H. The Effectiveness of Mindfulness Training in Improving the Quality of Life of the War Victims with Post Traumatic stress disorder (PTSD). Iran. J. Psychiatry 2014, 9, 228–236. Available online: http://eprints.bmsu.ac.ir/id/eprint/1753 (accessed on 10 July 2021).
- Mihaljević-Peleš, A.; Bajs Janović, M.; Šagud, M.; Živković, M.; Janović, Š.; Jevtović, S. Cognitive deficit in schizophrenia: An overview. Psychiatr. Danub. 2019, 31, 139–142. [Google Scholar] [PubMed]
- Krygier, J.R.; Heathers, J.A.; Shahrestani, S.; Abbott, M.; Gross, J.J.; Kemp, A.H. Mindfulness meditation, well-being, and heart rate variability: A preliminary investigation into the impact of intensive Vipassana meditation. Int. J. Psychophysiol. 2013, 89, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, F.A.; Lu, L.M.; Sollers, J.J.; Krivoschekov, S.G.; Booth, R.J.; Consedine, N.S. Why it pays to be mindful: Trait mindfulness predicts physiological recovery from emotional stress and greater differentiation among negative emotions. Mindfulness 2015, 6, 175–185. [Google Scholar] [CrossRef]
- Suh, J.W.; Hwang, E.Y.; Chung, S.Y.; Hang, W.W.; Kim, J.W. Effect of Meditation According to Emotional State and Meditation Subgroup Evaluated by HRV (Heart Rate Variability). J. Orient. Neuropsychiatry 2009, 20, 133–147. [Google Scholar]
- Léonard, A.; Clément, S.; Kuo, C.D.; Manto, M.U. Changes in Heart Rate Variability During Heartfulness Meditation: A Power Spectral Analysis Including the Residual Spectrum. Front. Cardiovasc. Med. 2019, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.P.; Penn, D.L.; Fredrickson, B.L.; Kring, A.M.; Meyer, P.S.; Catalino, L.I.; Brantley, M. A pilot study of loving-kindness meditation for the negative symptoms of schizophrenia. Schizophr. Res. 2011, 129, 137–140. [Google Scholar] [CrossRef]
- Beblo, T.; Pelster, S.; Schilling, C.; Kleinke, K.; Iffland, B.; Driessen, M.; Fernando, S. Breath versus emotions: The impact of different foci of attention during mindfulness meditation on the experience of negative and positive emotions. Behav. Ther. 2018, 49, 702–714. [Google Scholar] [CrossRef]
- Snippe, E.; Dziak, J.J.; Lanza, S.T.; Nyklíček, I.; Wichers, M. The shape of change in perceived stress, negative affect, and stress sensitivity during mindfulness-based stress reduction. Mindfulness 2017, 8, 728–736. [Google Scholar] [CrossRef]
- Garland, E.; Gaylord, S.; Park, J. The role of mindfulness in positive reappraisal. Explore 2009, 5, 37–44. [Google Scholar] [CrossRef]
- Szekeres, R.A.; Wertheim, E.H. Evaluation of Vipassana meditation course effects on subjective stress, well-being, self-kindness and mindfulness in a community sample: Post-course and 6-month outcomes. Stress Health 2015, 31, 373–381. [Google Scholar] [CrossRef]
- Jazaieri, H.; Goldin, P.R.; Werner, K.; Ziv, M.; Gross, J.J. A randomized trial of MBSR versus aerobic exercise for social anxiety disorder. J. Clin. Psychol. 2012, 68, 715–731. [Google Scholar] [CrossRef]



| Session | Themes | Content of the Program | Time (min) |
|---|---|---|---|
| 1 | Orientation to the MBSR program and recognition of internal resources | 1. MBSR program introduction | 20 |
| 2. Mindful breathing and body scan meditation | 25 | ||
| 3. Review and discussion | 15 | ||
| 2 | Perception and creative responding: a way to see and respond | 1. Mindful breathing and body scan meditation | 20 |
| 2. Mindful eating meditation | 20 | ||
| 3. Review and discussion | 20 | ||
| 3 | Pleasure and power in being present | 1. Mindful breathing meditation | 20 |
| 2. Mindful hatha yoga meditation | 25 | ||
| 3. Meditation discussion | 15 | ||
| 4 | How does conditioning and perception shape our experience | 1. Mindful breathing and sound meditation | 10 |
| 2. Mindful walking meditation | 30 | ||
| 3. Review and discussion | 20 | ||
| 5 | Awareness of conditioned patterns of escape from difficulty and making selective reactions | 1. Mindful breathing and mindful sound meditation | 20 |
| 2. Mindful thoughts and emotions meditation: review and discussion | 20 | ||
| 3. Explanation of stress response and mindfulness autonomic response | 20 | ||
| 6 | Awareness and balancing in stressful situations, especially acute or chronic stress | 1. Mindful breathing meditation and mindful sound meditation | 20 |
| 2. Mindful thoughts and emotions meditation | 20 | ||
| 3. Review and discussion | 20 | ||
| 7 | Integrating mindfulness practice | 1. Mindful breathing and body scan meditation | 20 |
| 2. Review and discussion | 20 | ||
| 3. Generosity in interpersonal relationships | 20 | ||
| 8 | Keeping up mindfulness meditation in daily life and finishing the program | 1. Mindful breathing meditation | 25 |
| 2. Review and stress reduction discussion | 25 | ||
| 3. Explain home practice and finishing meditation | 10 |
| Characteristics | Categories | Exp. (n = 14) | Cont. (n = 12) | χ2/t | p |
|---|---|---|---|---|---|
| n (%)/M ± SD | n (%)/M ± SD | ||||
| Gender | Male | 8 (30.8) | 7 (26.9) | 0.01 | 1.000 † |
| Female | 6 (23.1) | 5 (19.2) | |||
| Age (year) | 28–59 | 46.43 ± 8.25 | 44.42 ± 7.03 | 0.66 | 0.514 |
| Education | ≤Middle school | 2 (7.7) | 4 (15.4) | 2.06 | 0.725 |
| ≥High school | 12 (46.1) | 8 (30.8) | |||
| Marital status | Single | 11 (42.3) | 10 (38.5) | 0.90 | 0.638 |
| Married | 3 (11.5) | 2 (7.7) | |||
| Religion | Yes | 9 (34.6) | 6 (23.1) | 1.37 | 0.713 |
| No | 5 (19.2) | 6 (23.1) | |||
| Cohabitants | Family | 12 (46.1) | 9 (34.7) | 0.70 | 0.952 |
| None | 2 (7.7) | 3 (11.5) | |||
| Working status | Employed | 3 (11.5) | 1 (3.9) | 0.85 | 0.598 † |
| Unemployed | 11 (42.3) | 11 (42.3) | |||
| Monthly income | None | 4 (15.4) | 8 (30.8) | 4.13 | 0.127 |
| Less than 850 USD | 10 (38.4) | 4 (15.4) | |||
| Disease duration (years) | ≤5 | 1 (3.8) | 2 (7.6) | 23.32 | 0.224 |
| 6~9 | 2 (7.6) | 1 (3.8) | |||
| ≥10 | 11 (42.4) | 9 (34.8) | |||
| Number of psychiatric hospitalizations | No | 1 (3.8) | 2 (7.7) | 2.39 | 0.792 |
| 1–2 | 5 (19.2) | 5 (19.2) | |||
| ≤3 | 8 (30.9) | 5 (19.2) | |||
| Age at first onset | ≤20 | 2 (7.6) | 4 (15.2) | 17.28 | 0.504 |
| 21–29 | 7 (26.8) | 2 (7.6) | |||
| 30–39 | 5 (19.0) | 6 (23.8) | |||
| Presence of support groups | Yes | 9 (34.6) | 8 (30.8) | 0.02 | 1.000 † |
| No | 5 (19.2) | 4 (15.4) | |||
| Perceived stress | 30.71 (6.56) | 34.67 (4.23) | −1.79 | 0.086 | |
| HRV | 26.82 (16.70) | 29.34(15.43) | −0.40 | 0.695 | |
| Positive affect | 22.14 (5.63) | 21.00 (4.80) | 0.56 | 0.582 | |
| Negative affect | 30.36 (6.54) | 34.33 (4.52) | −1.77 | 0.089 | |
| Subjective wellbeing | 70.64 (17.43) | 59.00 (9.69) | 2.05 | 0.051 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, A.S.; Jang, M.H.; Sun, M.J. Effects of Mindfulness-Based Stress Reduction (MBSR) on Stress, Heart Rate Variability, Affect, and Wellbeing among People with Schizophrenia. Int. J. Environ. Res. Public Health 2021, 18, 11871. https://doi.org/10.3390/ijerph182211871
Kim AS, Jang MH, Sun MJ. Effects of Mindfulness-Based Stress Reduction (MBSR) on Stress, Heart Rate Variability, Affect, and Wellbeing among People with Schizophrenia. International Journal of Environmental Research and Public Health. 2021; 18(22):11871. https://doi.org/10.3390/ijerph182211871
Chicago/Turabian StyleKim, Ae Sil, Mi Heui Jang, and Min Jung Sun. 2021. "Effects of Mindfulness-Based Stress Reduction (MBSR) on Stress, Heart Rate Variability, Affect, and Wellbeing among People with Schizophrenia" International Journal of Environmental Research and Public Health 18, no. 22: 11871. https://doi.org/10.3390/ijerph182211871
APA StyleKim, A. S., Jang, M. H., & Sun, M. J. (2021). Effects of Mindfulness-Based Stress Reduction (MBSR) on Stress, Heart Rate Variability, Affect, and Wellbeing among People with Schizophrenia. International Journal of Environmental Research and Public Health, 18(22), 11871. https://doi.org/10.3390/ijerph182211871