
Revealing Distress and Perceived Stress among Dentists at the Outset of the COVID-19 Pandemic: A Cross-Sectional Factor Analytic Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Exploratory Factor Analysis
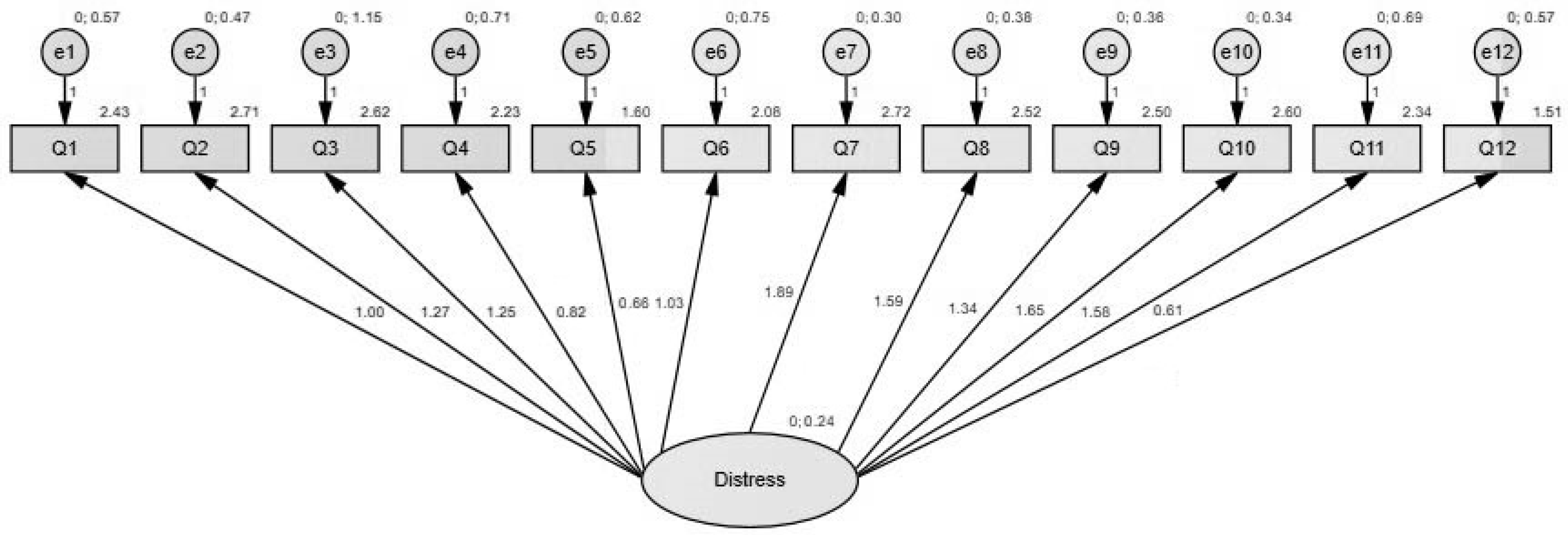
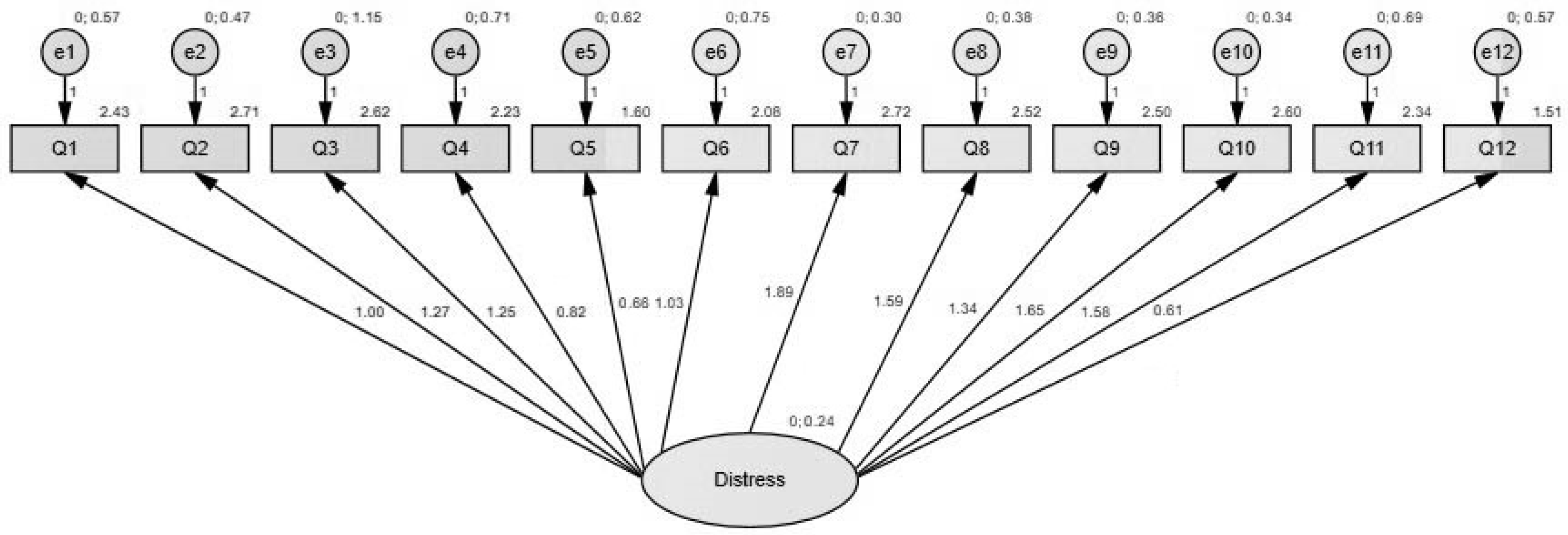
3.2. Confirmatory Factor Analysis
3.3. Effects of COVID-Related Variables on Perceived Stress and Psychological Distress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- She, J.; Jiang, J.; Ye, L.; Hu, L.; Bai, C.; Song, Y. 2019 novel coronavirus of pneumonia in Wuhan, China: Emerging attack and management strategies. Clin. Transl. Med. 2020, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef] [Green Version]
- Ayers, K.M.; Thomson, W.M.; Newton, J.T.; Rich, A.M. Job stressors of New Zealand dentists and their coping strategies. Occup. Med. 2008, 58, 275–281. [Google Scholar] [PubMed] [Green Version]
- Rada, R.E.; Johnson-Leong, C. Stress, burnout, anxiety, and depression among dentists. J. Am. Dent. Assoc. 2004, 135, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Maunder, R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: Lessons learned. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2004, 359, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Maunder, R.G.; Lancee, W.J.; Rourke, S.; Hunter, J.J.; Goldbloom, D.; Balderson, K.; Petryshen, P.; Steinberg, R.; Wasylenski, D.; Koh, D.; et al. Factors associated with the psychological impact of severe acute respiratory syndrome on nurses and other hospital workers in Toronto. Psychosom. Med. 2004, 66, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Mijiritsky, E.; Hamama-Raz, Y.; Liu, F.; Datarkar, A.N.; Mangani, L.; Caplan, J.; Shacham, A.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; et al. Subjective Overload and Psychological Distress among Dentists during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5074. [Google Scholar] [CrossRef]
- Wang, Y.; Di, Y.; Ye, J.; Wei, W. Study on the public psychological states and its related factors during the outbreak of the coronavirus disease 2019 (COVID-19) in some regions of China. Psychol. Health Med. 2021, 26, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Bhumireddy, J.; Mallineni, S.K.; Nuvvula, S. Challenges and possible solutions in dental practice during and post COVID-19. Environ. Sci. Pollut. Res. Int. 2021, 28, 1275–1277. [Google Scholar] [CrossRef] [PubMed]
- Barabari, P.; Moharamzadeh, K. Novel Coronavirus (COVID-19) and Dentistry-A Comprehensive Review of the Literature. Dent. J. 2020, 8, 53. [Google Scholar] [CrossRef]
- Mazur, M.; Duś-Ilnicka, I.; Jedliński, M.; Ndokaj, A.; Janiszewska-Olszowska, J.; Ardan, R.; Radwan-Oczko, M.; Guerra, F.; Luzzi, V.; Vozza, I.; et al. Facial and Oral Manifestations Following COVID-19 Vaccination: A Survey-Based Study and a First Perspective. Int. J. Environ. Res. Public Health 2021, 18, 4965. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, E.; Wachholtz, A. The effect of perceived stress on life satisfaction: The mediating effect of self-efficacy. Chongsonyonhak Yongu 2016, 23, 29–47. [Google Scholar] [PubMed] [Green Version]
- Arvidsdotter, T.; Marklund, B.; Kylén, S.; Taft, C.; Ekman, I. Understanding persons with psychological distress in primary health care. Scand. J. Caring Sci. 2016, 30, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Özarlsan, M.; Caliskan, S. Attitudes and predictive factors of psychological distress and occupational burnout among dentists during the COVID-19 pandemic in Turkey. Curr. Psychol. 2021, 40, 3113–3124. [Google Scholar]
- Hage-El, W.; Hingray, C.; Lemogne, C.; Yrondi, A.; Brunault, P.; Bienvenu, T.; Etain, B.; Paquet, C.; Gohier, B.; Dennabi, D.; et al. Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks? Encéphale 2020, 46, S73–S80. [Google Scholar]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef]
- Patel, M. Infection control in dentistry during COVID–19 pandemic: What has changed? Heliyon 2020, 30, e05402. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Narayana, T.V.; Mohanty, L.; Sreenath, G.; Vidhyadhari, P. Role of preprocedural rinse and high-volume evacuator in reducing bacterial contamination in bioaerosols. J. Oral Maxillofac. Pathol. 2016, 20, 59–65. [Google Scholar]
- Chuaybamrong, P.; Chotigawin, R.; Supothina, S.; Sribenjalux, P.; Larpkiattaworn, S.; Wu, C.Y. Efficacy of photocatalytic HEPA filter on microorganism removal. Indoor Air 2010, 20, 246–254. [Google Scholar] [CrossRef]
- Rexhepi, I.; Mangifesta, R.; Santilli, M.; Guri, S.; Di Carlo, P.; D’Addazio, G.; Caputi, S.; Sinjari, B. Effects of Natural Ventilation and Saliva Standard Ejectors during the COVID-19 Pandemic. A Quantitative Analysis of Aerosol Produced during Dental Procedures. Int. J. Environ. Res. Public Health 2021, 18, 7472. [Google Scholar] [CrossRef]
- Dave, M.; Seoudi, N.; Coulthard, P. Urgent dental care for patients during the COVID-19 pandemic. Lancet 2020, 395, 1257. [Google Scholar] [CrossRef]
- Izzetti, R.; Nisi, M.; Gabriele, M.; Graziani, F. COVID-19 Transmission in Dental Practice: Brief Review of Preventive Measures in Italy. J. Dent. Res. 2020, 99, 1030–1038. [Google Scholar] [CrossRef]
- Sinjari, B.; Rexhepi, I.; Santilli, M.; D’Addazio, G.; Chiacchiaretta, P.; Di Carlo, P.; Caputi, S. The Impact of COVID-19 Related Lockdown on Dental Practice in Central Italy-Outcomes of A Survey. Int. J. Environ. Res. Public Health 2020, 17, 5780. [Google Scholar] [CrossRef] [PubMed]
- Spoorthy, M.S.; Pratapa, S.K.; Mahani, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic: A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Ibn-Mohammed, T.; Mustapha, K.B.; Godsell, J.; Adamu, Z.; Babatunde, K.A.; Akintade, D.D.; Acquaye, A.; Ndiaye, M.M.; Yamoah, F.A.; Koh, S.C.L. A critical analysis of the impacts of COVID-19 on the global economy and ecosystems and opportunities for circular economy strategies. Resour. Conserv. Recycl. 2021, 164, 105169. [Google Scholar] [CrossRef]
- Uhlen, M.M.; Ansteinsson, V.E.; Stangvaltaite-Mouhat, L.; Korzeniewska, L.; Skudutyte-Rysstad, R.; Shabestari, M.; Mdala, I.; Hovden, E.A.S. Psychological impact of the COVID-19 pandemic on dental health personnel in Norway. BMC Health Serv. Res. 2021, 21, 420. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Noreen, S.; Farooq, I.; Bugshan, A.; Vohra, F. Risk assessment of healthcare workers at the frontline against COVID-19. Pak. J. Med. Sci. 2020, 36, S99–S103. [Google Scholar] [CrossRef]
- Kulkarni, S.; Dagli, N.; Duraiswamy, P.; Desai, H.; Vyas, H.; Baroudi, K. Stress and professional burnout among newly graduated dentists. J. Int. Soc. Prev. Community Dent. 2016, 6, 535–541. [Google Scholar]
- Al-Sowygh, Z.H. Academic distress, perceived stress, and coping strategies among dental students in Saudi Arabia. Saudi Dent. J. 2013, 25, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Murphy, R.J.; Gray, S.A.; Sterling, G.; Reeves, K.; DuCette, J. A Comparative Study of Professional Student Stress. J. Dent. Educ. 2009, 73, 328–337. [Google Scholar] [CrossRef]
- Cohen, S.; Kamar, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Singh, S.; Tiwari, V.; Vanza, B.; Khare, N.; Bharadwaj, P. Assessment of Level of Perceived Stress and Sources of Stress Among Dental Professionals Before and During the COVID-19 Outbreak. J. Int. Soc. Prev. Community Dent. 2020, 10, 794–802. [Google Scholar] [PubMed]
- Stauder, A.; Konkoly, T.B. Az Észlelt Stressz Kérdőív (PSS) Magyar verziójának jellemzői. Mentálhigiéné és Pszichoszomatika 7 2006, 3, 203–216. [Google Scholar] [CrossRef] [Green Version]
- Flesia, F.; Monaro, M.; Mazza, C.; Fietta, V.; Colicino, E.; Segatto, B.; Roma, P. Predicting Perceived Stress Related to the COVID-19 Outbreak through Stable Psychological Traits and Machine Learning Models. J. Clin. Med. 2020, 9, 3350. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Bryant, F.B.; Yarnold, P.R. Principal-components analysis and exploratory and confirmatory factor analysis. In Reading and Understanding Multivariate Statistics; Grimm, L.G., Yarnold, P.R., Eds.; American Psychological Association: Washington, DC, USA, 1995; pp. 99–136. [Google Scholar]
- Jöreskog, K.G.; Sörbom, D. LISREL VI: Analysis of Linear Structural Relationships by Maximum Likelihood and Least Squares Methods; Scientific Software: Mooresville, IN, USA, 1986. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Arbuckle, J.L. Amos (Version 23.0); Computer Program; IBM SPSS: Chicago, IL, USA, 2014. [Google Scholar]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- DiMatteo, M.R.; Shugars, D.A.; Hays, R.D. Occupational stress, life stress and mental health among dentists. J. Occup. Orang. Psychol. 1993, 66, 153–162. [Google Scholar] [CrossRef]
- Puriene, A.; Janulyte, V.; Musteikyte, M.; Bendinskaite, R. General Health of Dentists. Literature review. Stomatologija 2007, 9, 10–20. [Google Scholar]
- León-Manco, R.A.; Agudelo-Suárez, A.A.; Armas-Vega, A.; Figueiredo, M.C.; Verdugo-Paiva, F.; Santana-Pérez, Y.; Viteri-García, A. Perceived Stress in Dentists and Dental Students of Latin America and the Caribbean during the Mandatory Social Isolation Measures for the COVID-19 Pandemic: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5889. [Google Scholar] [CrossRef]
- Meira, T.M.; Paiva, S.M.; Antelo, O.M.; Guimarães, L.M.; Bastos, S.Q.; Tanaka, O.M. Perceived stress and quality of life among graduate dental faculty. J. Dent. Educ. 2020, 84, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Bardellini, E.; Amadori, F.; Veneri, F.; Conti, G.; Majorana, A. Coronavirus Disease-2019 and dental practice: A project on the use of ozonized water in the water circuit of the dental armchair. Stomatologija 2020, 22, 35–38. [Google Scholar]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Badru, O.A.; Oloko, K.O.; Hassan, A.O.; Yusuf, O.B.; Abdur-Razaq, U.A.; Yakub, S.S. Prevalence and correlates of psychological distress amongst healthcare workers during the COVID-19 pandemic: An online survey. S. Afr. J. Psychiatry 2021, 27, 1617. [Google Scholar] [CrossRef]
- Dziedzic, A.; Wojtyczka, R. The impact of coronavirus infectious disease 19 (COVID-19) on oral health. Oral Dis. 2021, 27, 703–706. [Google Scholar] [CrossRef]
- Sinjari, B.; D’Ardes, D.; Santilli, M.; Rexhepi, I.; D’Addazio, G.; Di Carlo, P.; Chiacchiaretta, P.; Caputi, S.; Cipollone, F. SARS-CoV-2 and Oral Manifestation: An Observational, Human Study. J. Clin. Med. 2020, 9, 3218. [Google Scholar] [CrossRef]
- Cooper, C.L.; Watts, J.; Baglioni, A.J.; Kelly, M. Job satisfaction, mental health, and job stressors among general dental practitioners in the UK. Br. Dent. J. 1987, 162, 77–81. [Google Scholar] [CrossRef]
- Coulthard, P. Dentistry and coronavirus (COVID-19)—Moral decision-making. Br. Dent. J. 2020, 228, 503–505. [Google Scholar] [CrossRef]
- Archuleta, K.L.; Scott, D.A. College students and financial distress: Exploring debt, financial satisfaction, and financial anxiety. J. Financ. Couns. Plan. 2013, 24, 50–62. [Google Scholar]
- Ferneini, E.M. The Financial Impact of COVID-19 on Our Practice. J. Oral Maxillofac. Surg. 2020, 78, 1046–1048. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, H.; Atteya, S.; Ihab, M.; Nyan, M.; Maharani, D.A.; Rahardjo, A.; Shaath, M.; Aboalshamat, K.; Butool, S.; Shamala, A.; et al. Dental practice closure during the frst wave of COVID-19 and associated professional, practice and structural determinants: A multi-country survey. BMC Oral Health 2021, 21, 243. [Google Scholar] [CrossRef]
- Farooq, I.; Ali, S. COVID-19 outbreak and its monetary implications for dental practices, hospitals, and healthcare workers. Postgrad. Med. J. 2020, 96, 791–792. [Google Scholar] [CrossRef] [PubMed]
- Humphris, G.M.; Cooper, C.L. New Stressors for GDPs in the past ten years: A qualitative study. BMJ 1998, 185, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.; Chu, C.M.; Pan, P.C.; Yiu, M.G.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Yap, A.U.; Bhole, S.; Teo, C.S. A cross-cultural comparison of perceived sources of stress in the dental school environment. J. Dent. Educ. 1996, 60, 459–464. [Google Scholar] [CrossRef]
- Mahendran, K.; Patel, S.; Sproat, C. Psychosocial effects of the COVID-19 pandemic on staff in a dental teaching hospital. Br. Dent. J. 2020, 229, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Pouradeli, S.; Shahravan, A.; Eskandarizden, A.; Rafie, F.; Hashemipour, M.A. Occupational Stress and Coping Behaviours Among Dentists in Kerman, Iran. Sultan Qaboos Univ. Med. J. 2016, 16, e341–e346. [Google Scholar] [CrossRef]
- Mahdee, A.F.; Gul, S.S.; Abdulkareem, A.A.; Qasim, S.S.B. Anxiety, Practice Modification, and Economic Impact Among Iraqi Dentists During the COVID-19 Outbreak. Front. Med. 2020, 7, 595028. [Google Scholar] [CrossRef] [PubMed]
- Allan, S.M.; Bealey, R.T.; Birch, J.; Cushing, T.; Parke, S.; Sergi, G.; Bloomfield, M.; Meiser-Stedman, R. The prevalence of common and stress-related mental health disorders in healthcare workers based in pandemic-affected hospitals: A rapid systematic review and meta-analysis. Eur. J. Psychotraumatol. 2020, 11, 1810903. [Google Scholar] [CrossRef] [PubMed]
- Lung, F.-W.; Lu, Y.-C.; Chang, Y.-Y.; Shu, B.-C. Mental Symptoms in Different Health Professionals During the SARS Attack: A Follow-up Study. Psychiatry Q. 2009, 80, 107–116. [Google Scholar] [CrossRef]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | N | % |
|---|---|---|
| Gender | ||
| Male | 62 | 34.1 |
| Female | 120 | 65.9 |
| Age (SD) | 50.95 (13.67) (min–max: 24–81 years) | |
| Residence | ||
| Capital city | 48 | 26.4 |
| City | 117 | 64.3 |
| Town | 5 | 2.7 |
| Village | 11 | 6.0 |
| Years of being a dental practitioner (SD) | 25.90 (13.63) (min–max: 0–57 years) | |
| Place of dental practice | ||
| Capital city | 50 | 27.5 |
| City | 106 | 58.9 |
| Town | 12 | 6.7 |
| Village | 12 | 6.7 |
| Marital status | ||
| Married/In domestic partnership | 145 | 79.7 |
| Single | 33 | 18.1 |
| Number of Children | ||
| 0 | 36 | 19.8 |
| 1 | 39 | 21.4 |
| 2 | 74 | 40.7 |
| 3 | 25 | 13.7 |
| 4 | 4 | 2.2 |
| 5 | 2 | 1.1 |
| Financial status compared to national average | ||
| significantly better | 20 | 11.0 |
| better | 111 | 61.0 |
| similar | 43 | 23.6 |
| worse | 6 | 3.3 |
| significantly worse | 1 | 0.5 |
| Question Regarding Emotions and Attitudes towards COVID-19 | Mean (SD) |
|---|---|
| I am preoccupied by things that are not at all or slightly worrying | 2.44 (0.902) |
| I get annoyed easily | 2.71 (0.903) |
| I have trouble sleeping | 2.62 (1.241) |
| I am indifferent towards various activities | 2.23 (0.936) |
| I have barely any or no appetite | 1.60 (0.853) |
| I feel emotionally distant from others | 2.08 (1.008) |
| I feel restless | 2.73 (1.082) |
| I feel sad | 2.52 (1.001) |
| I feel angry | 2.50 (0.897) |
| I have mood swings | 2.60 (1.002) |
| I am noticing the signs of burnout | 2.34 (1.144) |
| I employ addictive behaviour (smoking, drugs, alcohol) to cope with stress | 1.51 (0.814) |
| Question regarding dental professionals’ concerns and opinions | Mean (SD) |
| I feel that the COVID-19 pandemic will have long-lasting consequences on the financial situation of my practice. | 3.53 (1.016) |
| I feel that phone or online consultations will remain an integral part of my practice even after the COVID-19 pandemic will be under control. | 3.21 (1.128) |
| I feel that not even the strict compliance with professional rules can fully resolve the issues caused by aerosol propagation. | 3.99 (1.049) |
| I feel that my personal professional development is facilitated by online education until the pandemic gets under control. | 3.35 (1.098) |
| Factor | Initial Eigenvalues | Extraction Sums of Squared Loadings | Rotation Sums of Squared Loadings | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Variance% | Cumulative% | Total | Variance% | Cumulative% | Total | Variance% | Cumulative% | |
| 1 | 5.275 | 43.958 | 43.958 | 5.275 | 43.958 | 43.958 | 4.088 | 34.070 | 34.070 |
| 2 | 1.148 | 9.964 | 53.522 | 1.148 | 9.564 | 53.522 | 2.334 | 19.452 | 53.522 |
| Items | Factor Loadings | Communalities |
|---|---|---|
| I feel restless | 0.847 | 0.727 |
| I have mood swings | 0.811 | 0.705 |
| I feel sad | 0.798 | 0.638 |
| I feel angry | 0.758 | 0.665 |
| I am noticing the signs of burnout | 0.729 | 0.532 |
| I get annoyed easily | 0.689 | 0.672 |
| I am preoccupied by things that are not at all or slightly worry | 0.613 | 0.378 |
| I feel emotionally distant from others | 0.566 | 0.325 |
| I have trouble sleeping | 0.563 | 0.518 |
| I am indifferent towards various activities | 0.512 | 0.313 |
| I have barely any or no appetite | 0.460 | 0.642 |
| I employ addictive behaviour (smoking, drugs, alcohol) to cope with stress | 0.441 | 0.308 |
| 1st Regression | B | Std. Error | β | t | sig. | Tolerance | VIF |
|---|---|---|---|---|---|---|---|
| aerosol propagation | 0.501 | 0.614 | 0.283 | 4.075 | ≤0.001 | 0.987 | 1.014 |
| financial status | 3.558 | 0.914 | 0.272 | 3.892 | ≤0.001 | 0.977 | 1.024 |
| years in dental practice | −0.216 | 0.048 | −0.314 | −4.449 | ≤0.001 | 0.978 | 1.022 |
| 2nd Regression | |||||||
| aerosol propagation | 0.240 | 0.070 | 0.249 | 3.429 | 0.001 | 0.987 | 0.013 |
| financial status | 0.346 | 0.105 | 0.242 | 3.296 | 0.001 | 0.969 | 1.032 |
| age | −0.015 | 0.005 | −0.201 | −2.738 | 0.007 | 0.972 | 1.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serota, K.S.; Andó, B.; Nagy, K.; Kovács, I. Revealing Distress and Perceived Stress among Dentists at the Outset of the COVID-19 Pandemic: A Cross-Sectional Factor Analytic Study. Int. J. Environ. Res. Public Health 2021, 18, 11813. https://doi.org/10.3390/ijerph182211813
Serota KS, Andó B, Nagy K, Kovács I. Revealing Distress and Perceived Stress among Dentists at the Outset of the COVID-19 Pandemic: A Cross-Sectional Factor Analytic Study. International Journal of Environmental Research and Public Health. 2021; 18(22):11813. https://doi.org/10.3390/ijerph182211813
Chicago/Turabian StyleSerota, Kenneth S., Bálint Andó, Katalin Nagy, and Ildikó Kovács. 2021. "Revealing Distress and Perceived Stress among Dentists at the Outset of the COVID-19 Pandemic: A Cross-Sectional Factor Analytic Study" International Journal of Environmental Research and Public Health 18, no. 22: 11813. https://doi.org/10.3390/ijerph182211813
APA StyleSerota, K. S., Andó, B., Nagy, K., & Kovács, I. (2021). Revealing Distress and Perceived Stress among Dentists at the Outset of the COVID-19 Pandemic: A Cross-Sectional Factor Analytic Study. International Journal of Environmental Research and Public Health, 18(22), 11813. https://doi.org/10.3390/ijerph182211813