
Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors

 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Dependent Variables
Psychological Symptoms
2.3. Independent Variables
2.4. Covariate Variable
2.5. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, J.W. Life after ‘Humidifier Disinfectant’: Parents’ Becoming Victims in a Risk Society; Seoul National University: Seoul, Korea, 2019. [Google Scholar]
- Park, J.H.; Kim, H.J.; Kwon, G.Y.; Gwack, J.; Park, Y.J.; Youn, S.K.; Kwon, J.W.; Yang, B.G.; Lee, M.S.; Jung, M.; et al. Humidifier Disinfectants Are a Cause of Lung Injury among Adults in South Korea: A Community-Based Case-Control Study. PLoS ONE 2016, 11, e0151849. [Google Scholar]
- Choi, Y.; Lee, I. A Comparative Study of the Humidifier Disinfectant Disaster and Minamata Disease. J. Environ. Health Sci. 2019, 45, 326–339. [Google Scholar]
- Park, D.U.; Park, S.; Park, J.H.; Park, J.; Hong, S.J.; Paek, D. Abrupt Rise of Humidifier Disinfectant Associated Health Problems Since 2008: Was It Chance or Inevitable? J. Environ. Health Sci. 2020, 46, 128–135. [Google Scholar]
- Park, J.H.; Ko, M.H. A Study on the Damage Relief in Humidifier Sterilizer Case—Focused on Expanding the Role of Epidemiological Causality for Presumption of Causal Relationship. Law J. 2020, 48, 265–306. [Google Scholar]
- Social Disaster Special Investigation Committee. A Survey of Households Affected by Humidifier Disinfectants in 2018. Available online: http://www.socialdisasterscommission.go.kr (accessed on 3 September 2021).
- Park, D.U.; Lee, S.; Lim, H.K.; Kim, S.Y.; Kim, J.; Park, J.; Zoh, K.E. Comprehensive Review on Humidifier Disinfectant (HD) Products, Focusing on the Number of Products and Their Disinfectant Type. J. Environ. Health Sci. 2020, 46, 481–494. [Google Scholar]
- Leem, J.H.; Joh, J.; Hong, Y.; Kim, J.; Park, S.; Lim, S.; Kim, Y. Characteristics of a new respiratory syndrome associated with the use of a humidifier disinfectant: Humidifier disinfectant-related respiratory syndrome (HDRS). Int. J. Occup Med. Environ. Health 2020, 33, 829–839. [Google Scholar] [CrossRef]
- Yoon, J.; Kang, M.; Jung, J.; Ju, M.J.; Jeong, S.H.; Yang, W.; Choi, Y.H. Humidifier Disinfectant Consumption and Humidifier Disinfectant-Associated Lung Injury in South Korea: A Nationwide Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 6136. [Google Scholar] [CrossRef]
- Oh, J.H. Exploratory Study on the Influencing Factors of Embitterment of the Victims of Humidifier Disinfectants; Seoul National University: Seoul, Korea, 2019. [Google Scholar]
- Lê, F.; Tracy, M.; Norris, F.H.; Galea, S. Displacement, County Social Cohesion, and Depression After a Large-Scale Traumatic Event. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1729–1741. [Google Scholar] [CrossRef]
- Huang, Y.; Wong, H. Impacts of Sense of Community and Satisfaction with Governmental Recovery on Psychological Status of the Wenchuan Earthquake Survivors. Soc. Indic. Res. 2014, 117, 421–436. [Google Scholar] [CrossRef]
- Manesi, Z.; Van Lange, P.A.; Van Doesum, N.J.; Pollet, T.V. What Are the Most Powerful Predictors of Charitable Giving to Victims of Typhoon Haiyan: Prosocial Traits, Socio-Demographic Variables, or Eye Cues? Personal. Individ. Differ. 2019, 146, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Tsujiuchi, T. Post-traumatic stress due to structural violence after the Fukushima Disaster. Jpn. Forum. 2020, 33, 161–188. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Adult Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Family: Burlington, VT, USA, 2003. [Google Scholar]
- Kim, M.Y.; Kim, Y.A.; Lee, J.; Kim, H.J.; Oh, K.J. A Validity Study on the Korean Version of the Adult Self Report. Korean J. Clin. Psychol. 2014, 33, 615–632. [Google Scholar]
- Rescorla, L.A.; Achenbach, T.M.; Ivanova, M.Y.; Turner, L.V.; Althoff, R.R.; Árnadóttir, H.A.; Au, A.; Bellina, M.; Caldas, J.C.; Chen, Y.; et al. Problems and Adaptive Functioning Reported by Adults in 17 Societies. Int. Perspect. Psychol. 2016, 5, 91–109. [Google Scholar] [CrossRef]
- Chen, H.; Cohen, P.; Chen, S. How Big Is a Big Odds Ratio? Interpreting the Magnitudes of Odds Ratios in Epidemiological Studies. Commun. Stat.—Simul. Comput. 2010, 39, 860–864. [Google Scholar] [CrossRef]
- Guilaran, J.; de Terte, I.; Kaniasty, K.; Stephens, C. Psychological Outcomes in Disaster Responders: A Systematic Review and Meta-Analysis on the Effect of Social Support. Int. J. Disaster Risk Sci. 2018, 9, 344–358. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.S. Factors Associated with Quality of Life Among Disaster Victims: An Analysis of the 3rd Nationwide Panel Survey of Disaster Victims. J. Korean Acad. Commun. Health Nurs. 2019, 30, 217–225. [Google Scholar] [CrossRef]
- Miech, R.A.; Caspi, A.; Moffitt, T.E.; Wright, B.R.; Silva, P.A. Low Socioeconomic Status and Mental Disorders: A Longitudinal Study of Selection and Causation During Young Adulthood. Am. J. Sociol. 1999, 104, 1096–1131. [Google Scholar] [CrossRef] [Green Version]
- Wadsworth, M.E.; Achenbach, T.M. Explaining the Link Between Low Socioeconomic Status and Psychopathology: Testing Two Mechanisms of the Social Causation Hypothesis. J. Consult. Clin. Psychol. 2005, 73, 1146–1153. [Google Scholar] [CrossRef]
- Belle, D.; Doucet, J. Poverty, Inequality, and Discrimination as Sources of Depression Among US Women. Psychol. Women Q. 2003, 27, 101–113. [Google Scholar] [CrossRef]
- Costello, E.J.; Compton, S.N.; Keeler, G.; Angold, A. Relationships between Poverty and Psychopathology: A Natural Experiment. J. Am. Med. Assoc. 2003, 290, 2023–2029. [Google Scholar] [CrossRef] [Green Version]
- Marsh, H.W.; Parker, J.W. Determinants of Student Self-Concept: Is It Better to Be a Relatively Large Fish in a Small Pond Even If You Don’t Learn to Swim as Well? J. Pers. Soc. Psychol. 1984, 47, 213–231. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Aida, J.; Hase, A.; Sato, Y.; Koyama, S.; Tsuboya, T.; Osaka, K. Do Community- and Individual-Level Social Relationships Contribute to the Mental Health of Disaster Survivors?: A Multilevel Prospective Study after the Great East Japan Earthquake. Soc. Sci. Med. 2016, 151, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Arnberg, F.K.; Hultman, C.M.; Michel, P.O.; Lundin, T. Social Support Moderates Posttraumatic Stress and General Distress After Disaster. J. Trauma. Stress 2012, 25, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Cherry, K.E.; Sampson, L.; Nezat, P.F.; Cacamo, A.; Marks, L.D.; Galea, S. Long-Term Psychological Outcomes in Older Adults After Disaster: Relationships to Religiosity and Social Support. Aging Ment. Health 2015, 19, 430–443. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Dependent Variables | General Group (n = 228) Mean (SD) | Survivor Group (n = 228) Mean (SD) | Cohen’s d |
|---|---|---|---|
| Anxious/Depressed | 0.43 (0.31) | 0.85 (0.43) | 1.12 |
| Withdrawn | 0.32 (0.33) | 0.74 (0.42) | 1.11 |
| Somatic Complaints | 0.25 (0.27) | 0.67 (0.49) | 1.06 |
| Thought Problems | 0.19 (0.18) | 0.39 (0.30) | 0.81 |
| Attention Problems | 0.42 (0.30) | 0.64 (0.38) | 0.64 |
| Aggressive Behavior | 0.34 (0.31) | 0.62 (0.37) | 0.82 |
| Rule-Breaking Behavior | 0.16 (0.19) | 0.22 (0.24) | 0.28 |
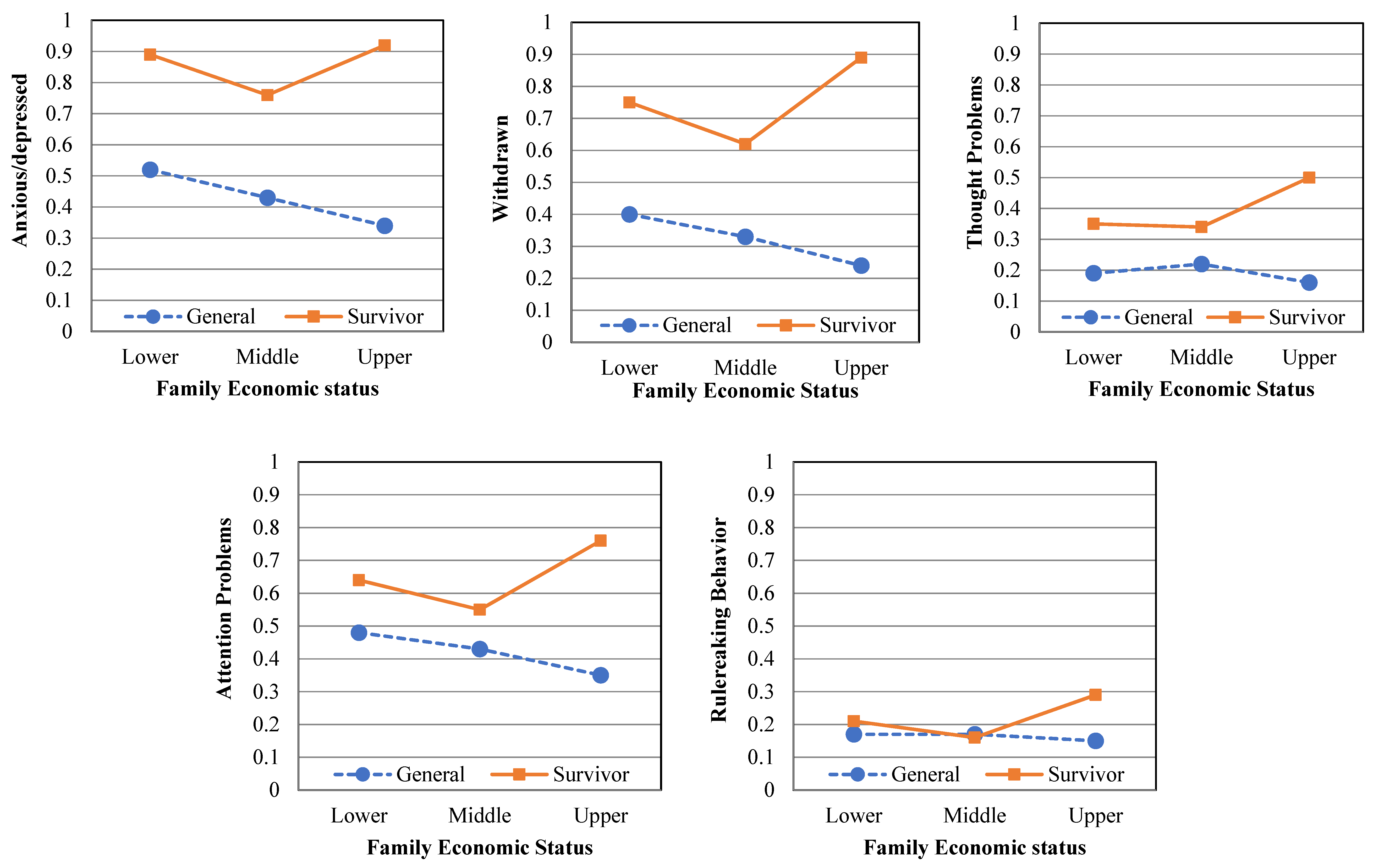
| Dependent Variables | General Group (n = 228) Mean (SD) | Survivor Group (n = 228) Mean (SD) | ||||
|---|---|---|---|---|---|---|
| Lower (61) | Middle (97) | Upper (70) | Lower (61) | Middle (93) | Upper (74) | |
| Anxious/Depressed | 0.52 (0.33) | 0.43 (0.29) | 0.34 (0.32) | 0.89 (0.44) | 0.76 (0.39) | 0.92 (0.46) |
| Withdrawn | 0.40 (0.37) | 0.33 (0.29) | 0.24 (0.32) | 0.75 (0.41) | 0.62 (0.35) | 0.89 (0.46) |
| Thought Problems | 0.19 (0.16) | 0.22 (0.20) | 0.16 (0.18) | 0.35 (0.30) | 0.34 (0.22) | 0.50 (0.36) |
| Attention Problems | 0.48 (0.27) | 0.43 (0.29) | 0.35 (0.33) | 0.64 (0.38) | 0.55 (0.31) | 0.76 (0.42) |
| Rule-Breaking Behavior | 0.17 (0.17) | 0.17 (0.19) | 0.15 (0.22) | 0.21 (0.24) | 0.16 (0.18) | 0.29 (0.29) |
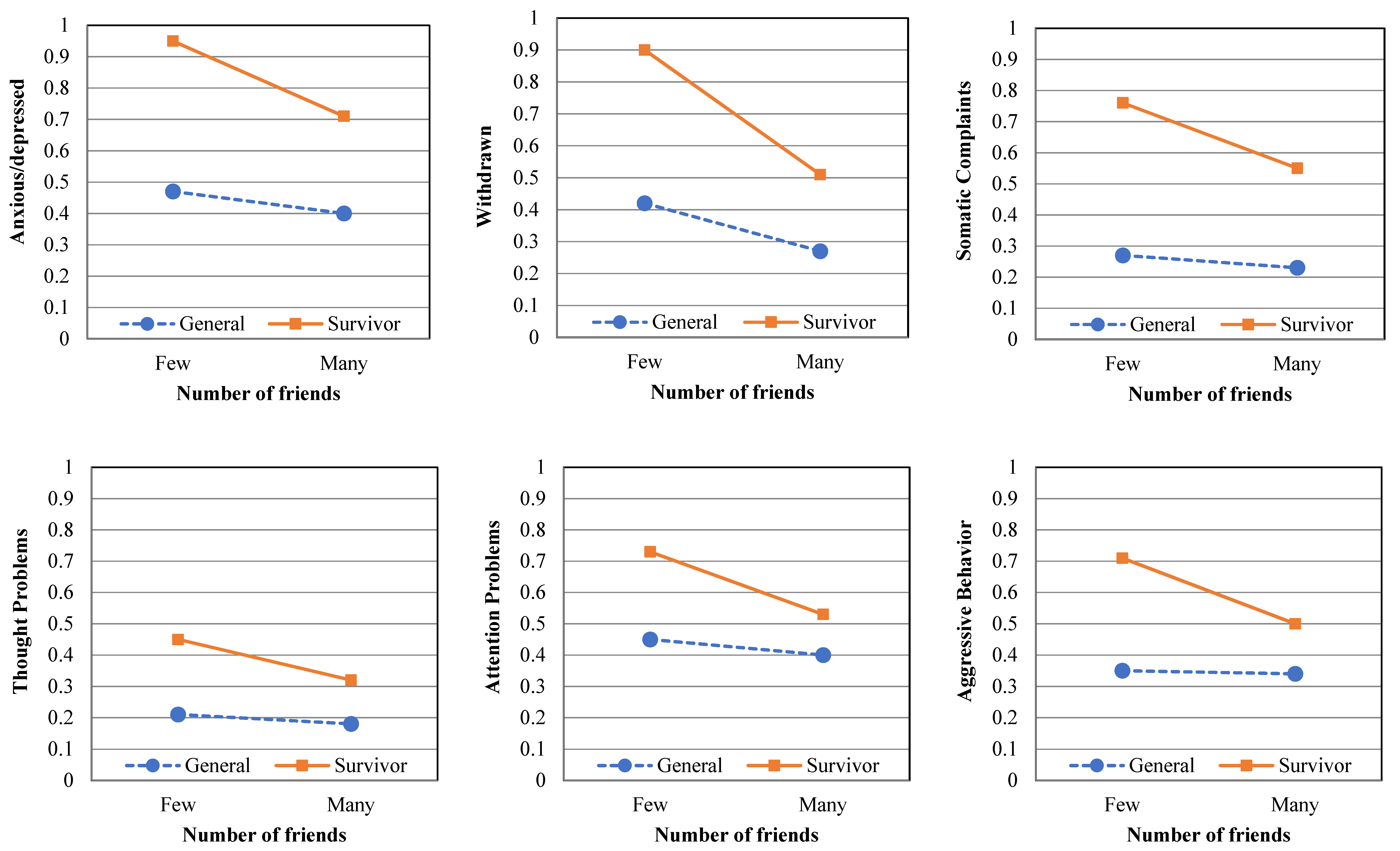
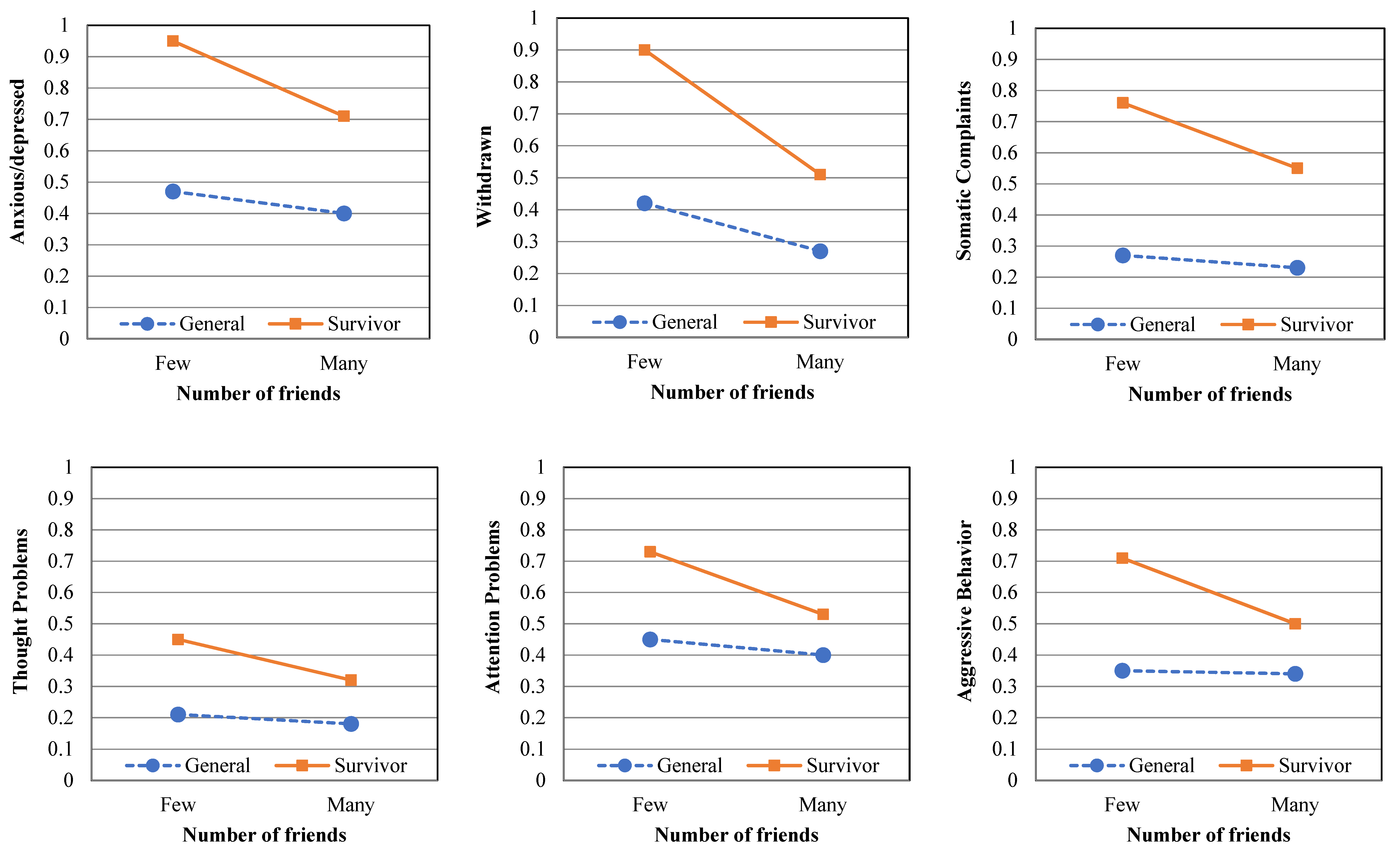
| Dependent Variables | General Group (n = 228) Mean (SD) | Survivor Group (n = 228) Mean (SD) | ||
|---|---|---|---|---|
| Few (83) | Many (145) | Few (133) | Many (95) | |
| Anxious/Depressed | 0.47 (0.34) | 0.40 (0.30) | 0.95 (0.43) | 0.71 (0.39) |
| Withdrawn | 0.42 (0.39) | 0.27 (0.27) | 0.90 (0.40) | 0.51 (0.33) |
| Somatic Complaints | 0.27 (0.31) | 0.23 (0.24) | 0.76 (0.52) | 0.55 (0.41) |
| Thought Problems | 0.21 (0.23) | 0.18 (0.16) | 0.45 (0.34) | 0.32 (0.22) |
| Attention Problems | 0.45 (0.32) | 0.40 (0.28) | 0.73 (0.39) | 0.53 (0.34) |
| Aggressive Behavior | 0.35 (0.30) | 0.34 (0.32) | 0.71 (0.39) | 0.50 (0.32) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, H.-Y.; Ryu, S.-H.; Lee, M.-J.; Lee, H.-J.; Kwon, S.-Y.; Kim, S.-M.; Lee, S.-M. Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors. Int. J. Environ. Res. Public Health 2021, 18, 11811. https://doi.org/10.3390/ijerph182211811
Ko H-Y, Ryu S-H, Lee M-J, Lee H-J, Kwon S-Y, Kim S-M, Lee S-M. Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors. International Journal of Environmental Research and Public Health. 2021; 18(22):11811. https://doi.org/10.3390/ijerph182211811
Chicago/Turabian StyleKo, Hye-Yun, Seung-Hun Ryu, Min-Joo Lee, Hun-Ju Lee, Soo-Young Kwon, Seong-Mi Kim, and Sang-Min Lee. 2021. "Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors" International Journal of Environmental Research and Public Health 18, no. 22: 11811. https://doi.org/10.3390/ijerph182211811
APA StyleKo, H.-Y., Ryu, S.-H., Lee, M.-J., Lee, H.-J., Kwon, S.-Y., Kim, S.-M., & Lee, S.-M. (2021). Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors. International Journal of Environmental Research and Public Health, 18(22), 11811. https://doi.org/10.3390/ijerph182211811