
Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies



Abstract
:1. Introduction
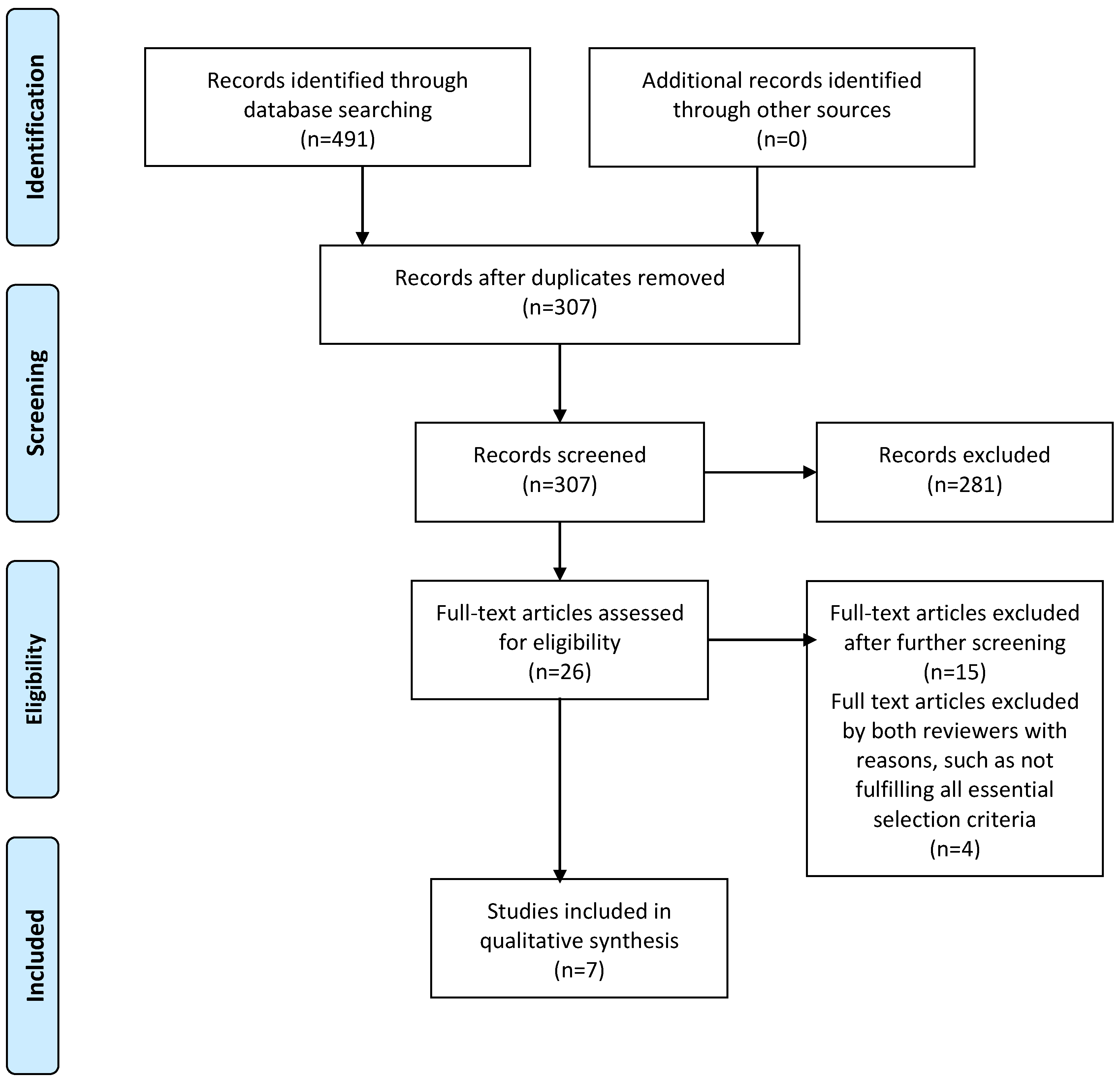
2. Methods
3. Results
4. Discussions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Simonds, J.F.; Parraga, H. Sleep behaviors and disorders in children and adolescents evaluated at psychiatric clinics. J. Dev. Behav. Pediatr. 1984, 5, 6–10. [Google Scholar] [PubMed]
- Edis, T.E.; Rosenberg, L.; Hudnell, G.; Jones, L. Sleep disorders among psychiatric outpatients. South Med. J. 1984, 77, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- Bartle, E.J.; Sun, J.H.; Thompson, L.; Light, A.I.; McCool, C.; Heaton, S. The effects of acute sleep deprivation during residency training. Surgery 1988, 104, 311–316. [Google Scholar] [PubMed]
- Sleep and Mental Health. Once viewed only as symptoms, sleep problems may actually contribute to psychiatric disorders. Harv. Ment. Health Lett. 2009, 26, 1–3. [Google Scholar]
- Tsuang, M.T.; Tohen, M.; Jones, P. Textbook of Psychiatric Epidemiology; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Ferrie, J.E.; Kumari, M.; Salo, P.; Singh-Manoux, A.; Kivimäki, M. Sleep epidemiology—A rapidly growing field. Int. J. Epidemiol. 2011, 40, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Tavernier, R.; Willoughby, T. Bidirectional associations between sleep (quality and duration) and psychosocial functioning across the university years. Dev. Psychol. 2014, 50, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Wakeford, R. Association and causation in epidemiology—Half a century since the publication of Bradford Hill’s interpretational guidance. J. R. Soc. Med. 2015, 108, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.H.; Lazo, M.; Carnethon, M.; Bertoni, A.G.; Schreiner, P.J.; Roux, A.V.D.; Lee, H.B.; Lyketsos, C. Examining a bidirectional association between depressive symptoms and diabetes. JAMA 2008, 299, 2751–2759. [Google Scholar] [CrossRef] [PubMed]
- Blakemore, S.J. Adolescence and mental health. Lancet 2019, 393, 2030–2031. [Google Scholar] [CrossRef]
- Oerlemans, A.M.; Wardenaar, K.J.; Raven, D.; Hartman, C.A.; Ormel, J. The association of developmental trajectories of adolescent mental health with early-adult functioning. PLoS ONE 2020, 15, e0233648. [Google Scholar] [CrossRef]
- Keynejad, R.C.; Dua, T.; Barbui, C.; Thornicroft, G. WHO Mental Health Gap Action Programme (mhGAP) Intervention Guide: A systematic review of evidence from low and middle-income countries. Evid. Based Ment. Health 2018, 21, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, K.J. Epidemiology: An Introduction, 2nd ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- United Nations General Assembly. Convention on the Rights of the Child, Treaty Series, 1577:3; United Nations: New York, NY, USA, 1989. [Google Scholar]
- WHO. Adolescence Health. World Health Organization: Geneva, Switzerland. Available online: https://www.who.int/southeastasia/health-topics/adolescent-health (accessed on 2 July 2021).
- WHO. Improving Early Childhood Development: WHO Guideline; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicinel: Westchester, IL, USA, 2014. [Google Scholar]
- Carter, K.A.; Hathaway, N.E.; Lettieri, C.F. Common sleep disorders in children. Am. Fam. Physician 2014, 89, 368–377. [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Arlington, VA, USA, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 89, 873–880. [Google Scholar]
- Johnson, E.O.; Chilcoat, H.D.; Breslau, N. Trouble sleeping and anxiety/depression in childhood. Psychiatry Res. 2000, 94, 93–102. [Google Scholar] [CrossRef]
- Gregory, A.M.; O’Connor, T.G. Sleep problems in childhood: A longitudinal study of developmental change and association with behavioral problems. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 964–971. [Google Scholar] [CrossRef]
- Paavonen, E.J.; Solantaus, T.; Almqvist, F.; Aronen, E.T. Four-year follow-up study of sleep and psychiatric symptoms in preadolescents: Relationship of persistent and temporary sleep problems to psychiatric symptoms. J. Dev. Behav. Pediatr. 2003, 24, 307–314. [Google Scholar] [CrossRef]
- Ong, S.H.; Wickramaratne, P.; Tang, M.; Weissman, M.M. Early childhood sleep and eating problems as predictors of adolescent and adult mood and anxiety disorders. J. Affect Disord. 2006, 96, 1–8. [Google Scholar] [CrossRef]
- Silva, G.E.; Goodwin, J.L.; Parthasarathy, S.; Sherrill, D.L.; Vana, K.D.; Drescher, A.A.; Quan, S.F. Longitudinal association between short sleep, body weight, and emotional and learning problems in Hispanic and Caucasian children. Sleep 2011, 34, 1197–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, J.M.; Ruttle, P.L.; Klein, M.H.; Essex, M.J.; Benca, R.M. Associations of child insomnia, sleep movement, and their persistence with mental health symptoms in childhood and adolescence. Sleep 2014, 37, 901–909. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Isensee, C.; Becker, A.; Wong, J.; Eastwood, P.R.; Huang, R.-C.; Runions, K.C.; Stewart, R.M.; Meyer, T.; Brüni, L.G.; et al. Developmental Trajectories of Sleep Problems from Childhood to Adolescence Both Predict and Are Predicted by Emotional and Behavioral Problems. Front. Psychol. 2016, 7, 1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lereya, S.T.; Winsper, C.; Tang, N.K.; Wolke, D. Sleep Problems in Childhood and Borderline Personality Disorder Symptoms in Early Adolescence. J. Abnorm. Child Psychol. 2017, 45, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales-Muñoz, I.; Broome, M.R.; Marwaha, S. Association of Parent-Reported Sleep Problems in Early Childhood with Psychotic and Borderline Personality Disorder Symptoms in Adolescence. JAMA Psychiatry 2020, 77, 1256–1265. [Google Scholar] [CrossRef] [PubMed]
- Slykerman, R.F.; Budd, C.; Thompson, J.M.D.; Bekker, M.; Buckley, J.; Wall, C.; Murphy, R.; Mitchell, E.A.; Waldie, K.E. Physical Activity, Sleep, Body Mass Index, and Associated Risk of Behavioral and Emotional Problems in Childhood. J. Dev. Behav. Pediatr. 2020, 41, 187–194. [Google Scholar] [CrossRef]
- Carpena, M.X.; Munhoz, T.N.; Xavier, M.O.; Rohde, L.A.; Santos, I.S.; Del-Ponte, B.; Barros, F.C.; Matijasevich, A.; Tovo-Rodrigues, L. The Role of Sleep Duration and Sleep Problems during Childhood in the Development of ADHD in Adolescence: Findings From a Population-Based Birth Cohort. J. Atten. Disord. 2020, 24, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Centre of Evidence-Based Medicine (CEBM). Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 1 October 2021).
- Mayer, D. Essential Evidence-Base Medicine, 2nd ed.; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Siegel, J.M. The neurotransmitters of sleep. J. Clin. Psychiatry 2004, 65, 4–7. [Google Scholar] [PubMed]
- Eban-Rothschild, A.; Appelbaum, L.; de Lecea, L. Neuronal Mechanisms for Sleep/Wake Regulation and Modulatory Drive. Neuropsychopharmacology 2018, 43, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Linley, S.B.; Vertes, R.P. Serotonergic Systems in Sleep and Waking. In Handbook of Behavioral Neuroscience; Dringenberg, H.C., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 30, pp. 101–123. [Google Scholar]
- Staner, L. Sleep and anxiety disorders. Dialogues Clin. Neurosci. 2003, 5, 249–258. [Google Scholar] [CrossRef]
- Mann, J. Role of the Serotonergic System in the Pathogenesis of Major Depression and Suicidal Behavior. Neuropsychopharmacology 1999, 21, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Wajszilber, D.; Santiseban, J.A.; Gruber, R. Sleep disorders in patients with ADHD: Impact and management challenges. Nat. Sci. Sleep 2018, 10, 453–480. [Google Scholar] [CrossRef] [Green Version]
- Freeman, D.; Sheaves, B.; Waite, F.; Harvey, A.G.; Harrison, P.J. Sleep disturbance and psychiatric disorders. Lancet Psychiatry 2020, 7, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Rafihi-Ferreira, R.E.; Pires, M.L.N.; Silvares, E.F.D.M. Behavioral intervention for sleep problems in childhood: A Brazilian randomized controlled trial. Psicol. Refl. Crít. 2019, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference (Author, Year, Place) | Participants | Study Methodology | Exposure, Confounding Variables and Measures | Outcome Variable and Measures | Method of Analysis and Variables Adjusted | Results | Comments |
|---|---|---|---|---|---|---|---|
| Gregory and O’Connor, (2002), CO, USA | Participants of the study were part of the Colorado Adoption Project with children and parents recruited from adoptive and non-adoptive families. In total, 490 families were recruited with an equal number of family types. | Parents and children were recruited and followed since birth. Assessment on children was conducted annually since recruitment. Baseline assessment on sleep problems was conducted at the time when the child was 4 years old when sleep problems were first assessed. Mental health assessment was evaluated annually until 15 years old (n = 490). | Exposure: Early Childhood sleep problems with common symptoms of sleep disorders, including nightmares, sleepwalking and talking, trouble in falling asleep. Measures: The Sleep Problem Scale of the Child Behavior Checklist (CBCL) Confounding variables: Child sex, adoption status, anxiety/depression at age 4, attention problems at age 4, and aggression at age 4, assessed by CBCL. | Outcome: Anxiety/depression and attention problems. Measures: The Behavioral/Emotional Scale of the CBCL.A combined assessment across 13, 14, and 15 years because of attrition. | Relations between early childhood sleep problems and anxiety/depression, as well as attentional problems were examined with hierarchical linear regression with adjustment for child’s sex, adoption status, and behavioral/emotional problems at age 4. | Regression analyses results suggested sleep problems at 4 year significantly predicted anxiety/depression in mid-adolescence (β = 0.16, p < 0.01, R2 = 0.12). Similarly sleep problems at age 4 also significantly predicted attentional problems at mid-adolescence (β = 0.11, p < 0.05, R2 = 0.25). | Strengths and Limitations: The study was limited by a high attrition rate (26%), although the original sample was of a reasonable size (n = 490). Furthermore, the assessments on sleep problems and mental health problems were self-parents. Without an additional informant, especially the child at the adolescence period, report basis might be an issue. Some important confounding variables, such as parental mental health, might be missing |
| Silva et al. (2011), Tucson, USA | Children, aged 6–12 years of Hispanic and Caucasian origin were recruited in the Tucson Children’s Assessment of Sleep Apnea Study. Children were recruited from the Tucson Unified School District, excluding those who had a history of tonsillectomy and mental disorders. The mean age was 8.9 years at baseline assessment. | Children were followed after baseline assessments (n = 503) on sleep apnea and behavioral/emotional problems. They were followed for about 5 years with 304 participants retained in the study for outcome assessments. All assessments were conducted during the in-home visit (n = 304). | Exposure: Sleep apnea and sleep history characteristics. Measures: Sleep apnea was assessed using unattended home polysomnograms (PSGs). Sleep scores were calculated by a somnographic technologist who was blind to the child’s mental status. Sleep history and characteristics were assessed using the Sleep Habits Questionnaires (SHQs) by parental reports. Confounding variables: Baseline BMI, ethnicity, sleep apnea at follow-up, age at follow-up, caffeine use at follow-up, and anxiety/depression at baseline were included in the analyses. | Outcome: Anxiety/depression. Measures: Assessed using Child Behaviour Checklist (CBCL) completed by parents at the follow-up visit. | Multivariate mixed-effect linear regression modeling was applied to examine the effect of childhood sleep problems on anxiety/depression at adolescence, controlling for confounding factors. | Short duration of sleep (<7.5 h/night) at childhood was marginally predictive of the anxiety/depression at adolescence but not significant at 5% Type I error rate (OR = 3.3, 95% CI = 0.83–13.5). | Strengths and Limitations: Sleep apnea was measured objectively using polysomnograms. However, the actual measures on sleep apnea were used in the analyses. Instead, the duration of sleep was used as the outcome variable, although it would be argued that a short duration of sleep was highly correlated to the symptoms of sleep apnea. Some important confounding variables, such as parental mental health, might be missing |
| Armstrong et al. (2013), Wisconsin, USA | The sample was drawn from the Wisconsin Study of Family and Work for this secondary data analysis study. | Families were recruited from pregnancy and followed until the child reached 18 years. Of the original 570 families recruited, 341 had complete data on both childhood sleep problems at the age of 4.5 and 9 years and mental health at age 18 (n = 341). | Exposure: Sleep problems included insomnia, sleep movement, hypersomnia, and a range of parasomnias. Due to low frequencies in other problems, the study focused on persistent insomnia and sleep movement defined as having the individual problem at both 4.5 and 9 years. Measures: Sleep problems were assessed using the Children’s Sleep Habits Questionnaires (SHQs) by maternal reports. Confounding variables: Potential confounding variables were included in the final analyses. These were the child’s sex, medication of psychostimulant. | Outcome: Anxiety, depression, externalizing behaviors, and ADHD Measures: Assessed using the MacArthur Health and Behavior Questionnaire (HBQ) self-reported by the child at the age of 18. | Multivariate analysis of variance (MONOVA) was used to examine the association between persistent sleep problems at age 9 and mental health problems at 18 years controlling for confounding factors. | Persistent insomnia was significantly related to anxiety and externalizing behaviours in adolescence (F(2,334) = 4.82, p = 0.009 and F(2,334) = 4.53, p = 0.011). Persistent sleep movement was also significantly associated with ADHD at adolescence (F(2,334) = 6.68, p = 0.001). | Strengths and Limitations: The study was well-executed and the follow-up process was complete with comparisons on many demographic variables between the participating and on-participating families. Two main limitations were identified: (1) most demographic variables were not included in the analyses to be considered as potentially confounding; (2) assessments on the exposure and outcome variables were conducted by self-reported questionnaires risking certain degree of report bias by mothers and children. (3) Other important confounding variables, such as parental mental health, might be missing. |
| Wang et al. (2016), Perth, Western Australia | This secondary data analysis study drew the sample from the Western Australian Pregnancy Cohort (Raine) Study. | Women between 16 and 20 weeks gestation were recruited from the public antenatal clinic at the participating sites. Mother had consented to be followed annually until the child reached the age of 18. Assessments were conducted via questionnaire and physical examination. This study focused on childhood sleep data collected at 5, 8, 10, 14-year follow-up and mental health assessment at 17 years (n = 1182). | Exposure: Childhood sleep problems with common symptoms of sleep disorders, including nightmares, sleepwalking and talking, trouble in falling asleep. Measures: The Sleep Problem Scale of the Child Behavior Checklist (CBCL). However, the focus of the study was the latent trajectory classes of sleep problems from age 5 to 14. Early childhood sleep problem was classified as normal and troubled sleepers using unconditional growth mixture models. Confounding variables: Not mentioned in the study. | Outcome: Anxiety, depression, externalizing behaviors, and ADHD Measures: Assessed using the Youth Self Report (YSR), which is the youth version of the self-reported by the child at the age of 17. | Simple independent sample Student’s t-tests were applied to examine the differences in the scores on the YSR between normal and troubled sleepers. | There was a significant difference in the mean score of ADHD between groups with troubled sleepers scored higher (Mnormal = 4.93, Mtroubled = 5.73, p < 0.05). The mean score of the troubled sleepers was also significantly higher than that of the controls (Mnormal = 7.79, Mtroubled = 9.04, p < 0.05). No significant differences in anxiety and depression were observed between groups. | Strengths and Limitations: This secondary data analysis study utilized a data set with a large sample size and a long period of follow-up. Similar to the Armstrong et al.’s study, two main limitations were identified: (1) assessments on the exposure and outcome variables were conducted by self-reported questionnaires, thus, the risk of report basis by mothers and children was high; (2) simple comparisons on main outcome variables between groups were conducted without any considerations of potential confounding factors on the results. (3) Should also consider confounding issues. |
| Lereya et al. (2017), Avon, UK | This was another secondary data analysis study using data collected in the Avon Longitudinal Study of the Parents and Children (ALSPAC) in the UK. | Mother and child dyads were recruited in the Avon birth cohort study with an initial 14,541 pregnant women enrolled. Parents responded to postal questionnaires on their child’s health development during follow-up. The Child was assessed annually via face-to-face interviews on psychosocial and physical health. This study utilized data collected on borderline personality disorder when the child was about 12 years (mean age 11.8 years) (n = 6050). | Exposure: Childhood sleep problems included nightmares, sleep maintenance problems, and trouble falling asleep. Measures: Sleep problems were assessed by a set of sleep questions when the child was 2.5, 3.5, 4.8, and 6.8 years of age. In this study, sleep problems were categorized in accordance to the responses at each time point for each type of problem. For example, no nightmare at all, nightmare at 1 time point, 2 time points, 3 or more time points. Confounding variables: A number of potential confounding variables were controlled. These included: sex, emotional temperament at 2 years, family adversity index, physical and sexual abuse at 2.5, 3.5, 4.8, or 6.8 years, preschool maladaptive parenting, Developmental and Wellbeing Assessment at 7 years, and emotional and behavioral problems at 9.5 and 11.7 years. | Outcome: Borderline personality disorder (BPD) symptoms. Measures: Assessed by a trained psychologist at face-to-face interview using the UK Childhood Interview for DSM-IV-Borderline Personality Disorder at about 12 years. | Logistic regression analysis as the primary analytical approach and verified with path analysis | Having persistent nightmares (i.e., nightmares assessed as positive at 3 or more time points) during early childhood was significantly associated with BPD symptoms at adolescence after controlling for potential confounding variables (OR = 1.62, 95% CI = 1.12–2.32). Results were also verified with path analysis. | Strengths and Limitations: Similar to the previous study in this review, this secondary data analysis study utilized a large data set that could provide sufficient power for demonstrating a true effect between the exposure and outcome variables. Another strength of the study was that sufficient control for potential confounding effects was in place to ensure the precision of the effect estimate. |
| Morales-Munoz et al. (2020), Avon, UK | This was another secondary data analysis study using data of the same Avon Longitudinal Study of the Parents and Children (ALSPAC) in UK as Lereya et al. | Mother and child dyads were recruited in the Avon birth cohort study with an initial 14,541 pregnant women enrolled. Parents responded to postal questionnaires on their child’s health development during follow-up. The Child was assessed annually via face-to-face interviews on psychosocial and physical health (n = 7155). This study utilized data collected on Psychotic symptoms and BPD since the child was 12 years. The main focus of the study was on psychotic symptoms (n = 7155). | Exposure: Childhood sleep problems included nightmares, duration of sleep, sleep maintenance problems, and sleep routine regularity. Measures: Sleep problems were assessed by a set of sleep questions when the child was 6 months, 18 months, 30 months, 3.5, 4.8, and 5.8 years of age. This study focused on the duration of sleep, sleep maintenance, and sleep routine. Confounding variables: A number of potential confounding variables were controlled. These included: sex, emotional temperament at 2 years, family adversity index, physical and sexual abuse, prematurity, and maternal age when the child was born. | Outcome: Psychotic symptoms. Measures: Assessed by a trained psychologist at face-to-face interview using the Psychotic-Like Symptom Interview. | Logistic regression analysis as the primary analytical approach. Of interest to the authors was also the possible mediating effect of depression at 10 years on the relationship between early childhood sleep problems and psychotic symptoms with path analysis which was similar to Lereya’s study. | There were significant relationships between a regular sleep routine and psychotic symptoms. Children with a regular sleep routine at 6 months had a reduced odds of psychotic symptoms at 12 to 13 years by about 30% (OR = 0.68, 95% CI = 0.50–0.93). Children with a regular sleep routine at 30 months had a reduced odds of psychotic symptoms of about 35% 4 (OR = 0.68, 95% CI = 0.44–0.95). Children with a regular sleep routine at 5.8 years had an even greater reduction in odds of psychotic symptoms at 12 to 13 years by about 70% (OR = 0.32, 95% CI = 0.19–0.53). Results were obtained after the adjustment of confounding variables. A possible mediating effect of depression on children’s regular sleep routine at 5.8 years and psychotic symptoms at 12 to 13 years was also reported. | Strengths and Limitations: Similar to Lereya’s study utilizing the same data set, this study shared the same strengths that the large sample size could provide sufficient power for demonstrating a true effect between the exposure and outcome variables. Similarly, sufficient control for potential confounding effect was in place to ensure the precision of the effect estimate was another strength of the study. |
| Slykerman et al. (2020), Auckland, New Zealand | This was a secondary data analysis study utilizing data collected from the Auckland Birthweight Collaborative Study (ABC Study). | Mothers, mainly of European ethnicity, and their newborn children were recruited to the Study. All children were born full-term with a gestation of 37 weeks or longer between October 1995 and November 1997. Children were then followed until 11 years. Data on sleep problems were collected at 7 years and mental health problems were assessed at 11 years. In total, 547 children had provided data on both the exposure and outcome variables. (n = 547). | Exposure: Sleep duration at 7 years was the only sleep variable of interest. Measures: Sleep duration was measured by actigraphy for 24 h. Confounding variables: Birthweight, sex, gestation, socioeconomic status, maternal smoking during pregnancy, marital status at the time the child was born, maternal school leaving age, and child intelligence were included in the analyses for adjustment. | Outcome: Emotional/behavioral difficulties and ADHD. Measures: Emotional/ behavioral difficulties were assessed by the Strengths and Difficulties Questionnaire (SDQ) self-reported by both parent and child at age 11. For ADHD, it was assessed using the Conner’s Rating Scale (CRS) filled in by parents and teachers when the child was 11 years old. | Logistic regression analyses were applied to examine the relationship between the exposure and outcome variables. | After adjusting for potential confounding factors, there was no significant relationship between sleep duration at 7 years and emotional/behavioral problems as well as ADHD at 11 years. | Strengths and Limitations: Similar to other studies in this review, this study suffered similar shortcomings as the other. Despite the objective measures of sleep problems using actigraphy, sleep duration was the only variable under investigation. Given the sound approach in exposure assessment, other sleep variables should also be considered. The self-reporting on the outcome variables might incur some report bases by parents, children, and teachers. Another shortcoming of this study was the lack of information on sleep problems of children at their earlier stage of development. |
| Studies | |||||||
|---|---|---|---|---|---|---|---|
| Gregory and O’Connor | Silva et al. | Armstrong et al. | Wang et al. | Lereya et al. | Morales-Munoz et al. | Slykerman et al. | |
| Sleep Problems | Common Symptoms of Sleep Disorders | Short Duration of Sleep (<7.5 h/Night) | Persistent Insomnia | Common Symptoms of Sleep Disorders | Persistent Nightmares | Irregular Sleep Routine | Sleep Duration |
| Mental Health Problems | |||||||
| Anxiety/Depression | + | − | + | ||||
| ADHD | + | + | + | ||||
| Externalizing behaviors | + | + | |||||
| BPD | + | ||||||
| Psychotic symptoms | + | ||||||
| Emotional/Behaviral difficulties | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, L.T.; Lam, M.K. Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies. Int. J. Environ. Res. Public Health 2021, 18, 11782. https://doi.org/10.3390/ijerph182211782
Lam LT, Lam MK. Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies. International Journal of Environmental Research and Public Health. 2021; 18(22):11782. https://doi.org/10.3390/ijerph182211782
Chicago/Turabian StyleLam, Lawrence T, and Mary K Lam. 2021. "Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies" International Journal of Environmental Research and Public Health 18, no. 22: 11782. https://doi.org/10.3390/ijerph182211782
APA StyleLam, L. T., & Lam, M. K. (2021). Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies. International Journal of Environmental Research and Public Health, 18(22), 11782. https://doi.org/10.3390/ijerph182211782