
The Usefulness of Evaluating Performance of Activities in Daily Living in the Diagnosis of Mild Cognitive Disorders



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measurements
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burns, A.; Iliffe, S. Alzheimer’s disease. BMJ 2009, 338, 158. [Google Scholar] [CrossRef] [Green Version]
- Burns, A.; Iliffe, S. Dementia. BMJ 2009, 338, 75. [Google Scholar] [CrossRef]
- McKhann, G.M. Changing concepts of Alzheimer disease. JAMA 2011, 305, 2458–2459. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack Jr, C.R.; Kawas, C.H.; Phelps, C.H. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the national institute on aging-alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Dementia 2017. Available online: http://www.who.int/mediacentre/factsheets/fs362/en/ (accessed on 30 September 2021).
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report. The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimers Disease International (ADI): London, UK, 2015. [Google Scholar]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.J.; Albert, M.S.; Almkvist, O.; et al. Mild cognitive impairment—beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Tay, L.; Lim, W.S.; Chan, M.; Ali, N.; Mahanum, S.; Chew, P.; Lim, J.; Chong, M.S. New DSM-V neurocognitive disorders criteria and their impact on diagnostic classifications of mild cognitive impairment and dementia in a memory clinic setting. Am. J. Geriatr. Psychiatry 2015, 23, 768–779. [Google Scholar] [CrossRef]
- Albert, S.M.; Tabert, M.H.; Dienstag, A.; Pelton, G.; Devanand, D. The impact of mild cognitive impairment on functional abilities in the elderly. Curr. Psychiatry Rep. 2002, 4, 64–68. [Google Scholar] [CrossRef]
- Krell-Roesch, J.; Cerhan, L.P.; Machulda, M.M.; Roberts, R.O.; Mielke, M.M.; Knopman, D.S.; Geda, Y.E. Functional activity and neuropsychiatric symptoms in normal aging and mild cognitive impairment: The mayo clinic study of aging. Alzheimer Dis. Assoc. Disord. 2019, 33, 68. [Google Scholar] [CrossRef]
- Lindbergh, C.A.; Dishman, R.K.; Miller, L.S. Functional disability in mild cognitive impairment: A systematic review and meta-analysis. Neuropsychol. Rev. 2016, 26, 129–159. [Google Scholar] [CrossRef]
- Mao, H.-F.; Chang, L.H.; Tsai, A.Y.-J.; Huang, W.-N.W.; Tang, L.-Y.; Lee, H.-J.; Sun, Y.; Chen, T.-F.; Lin, K.-N.; Wang, P.-N.; et al. Diagnostic accuracy of instrumental activities of daily living for dementia in community-dwelling older adults. Age Ageing 2018, 47, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Reuben, D.B.; Laliberte, L.; Hiris, J.; Mor, V. A hierarchical exercise scale to measure function at the advanced activities of daily living (AADL) level. J. Am. Geriatr. Soc. 1990, 38, 855–861. [Google Scholar] [CrossRef]
- De Vriendt, P.; Gorus, E.; Cornelis, E.; Velghe, A.; Petrovic, M.; Mets, T. The process of decline in advanced activities of daily living: A qualitative explorative study in mild cognitive impairment. Int. Psychogeriatr. 2012, 24, 974–986. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the aged. The index of Adl: A standard-ized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Morris, J.N.; Berg, K.; Fries, B.E.; Steel, K.; Howard, E.P. Scaling functional status within the interRAI suite of assessment in-struments. BMC Geriatr. 2013, 13, 128. [Google Scholar] [CrossRef] [Green Version]
- Schmitter-Edgecombe, M.; Parsey, C.M. Assessment of functional change and cognitive correlates in the progression from healthy cognitive aging to dementia. Neuropsychology 2014, 28, 881–893. [Google Scholar] [CrossRef] [Green Version]
- Lechowski, L.; Van Pradelles, S.; Le Crane, M.; D’Arailh, L.; Tortrat, D.; Teillet, L.; Vellas, B. Patterns of loss of basic activities of daily living in Alzheimer patients: A cross-sectional study of the french real cohort. Dement. Geriatr. Cogn. Disord. 2010, 29, 46–54. [Google Scholar] [CrossRef]
- De Vriendt, P.; Cornelis, E.; Gorus, E. The usefulness of evaluating performance of activities of daily living in the diagnosis of mild cognitive disorders. In Diagnosis and Management in Dementia; Academic Press: London, UK, 2020. [Google Scholar]
- De Vriendt, P.; Gorus, E.; Cornelis, E.; Bautmans, I.; Petrovic, M.; Mets, T. The advanced activities of daily living: A tool allowing the evaluation of subtle functional decline in mild cognitive impairment. J. Nutr. Health Aging 2013, 17, 64–71. [Google Scholar] [CrossRef] [Green Version]
- De Vriendt, P.; Mets, T.; Petrovic, M.; Gorus, E. Discriminative power of the advanced activities of daily living (a-ADL) tool in the diagnosis of mild cognitive impairment in an older population. Int. Psychogeriatr. 2015, 27, 1419–1427. [Google Scholar] [CrossRef]
- Cornelis, E.; Gorus, E.; Beyer, I.; Bautmans, I.; De Vriendt, P. Early diagnosis of mild cognitive impairment and mild dementia through basic and instrumental activities of daily living: Development of a new evaluation tool. PLoS Med. 2017, 14, e1002250. [Google Scholar] [CrossRef]
- Cornelis, E.; Gorus, E.; Van Weverbergh, K.; Beyer, I.; De Vriendt, P. Convergent and concurrent validity of a report- versus performance-based evaluation of everyday functioning in the diagnosis of cognitive disorders in a geriatric population. Int. Psychogeriatr. 2018, 30, 1837–1848. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Gallagher, D.; Mhaolain, A.N.; Coen, R.; Walsh, C.; Kilroy, D.; Belinski, K.; Lawlor, B.A. Detecting prodromal Alzheimer’s disease in mild cognitive impairment: Utility of the CAMCOG and other neuropsychological predictors. Int. J. Geriatr. Psychiatry 2010, 25, 1280–1287. [Google Scholar] [CrossRef]
- Reppermund, S.; Birch, R.C.; Crawford, J.D.; Wesson, J.; Draper, B.; Kochan, N.A.; Sachdev, P.S. Performance-based assessment of instrumental activities of daily living: Validation of the sydney test of activities of daily living in memory disorders (STAM). J. Am. Med. Dir. Assoc. 2017, 18, 117–122. [Google Scholar] [CrossRef]
- Rodakowski, J.; Skidmore, E.R.; Reynolds, C.F., 3rd; Dew, M.A.; Butters, M.A.; Holm, M.B.; Rogers, J.C. Can performance on daily activities discriminate between older adults with normal cognitive function and those with mild cognitive impairment? J. Am. Geriatr. Soc. 2014, 62, 1347–1352. [Google Scholar] [CrossRef]
- Suchy, Y.; Kraybill, M.L.; Franchow, E. Instrumental activities of daily living among community-dwelling older adults: Discrepancies between self-report and performance are mediated by cognitive reserve. J. Clin. Exp. Neuropsychol. 2011, 33, 92–100. [Google Scholar] [CrossRef]
- Malhotra, R.; Haaland, B.A.; Chei, C.-L.; Chan, A.; Malhotra, C.; Matchar, D.B. Presence of and correction for interviewer error on an instrument assessing cognitive function of older adults. Geriatr. Gerontol. Int. 2014, 15, 372–380. [Google Scholar] [CrossRef]
- Malhotra, C.; Chan, A.; Malhotra, R.; Ostbye, T. Prevalence, correlates and perceived causes of limitations in activities of daily living among older Singaporeans. Aging Clin. Exp. Res. 2012, 24, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Farias, S.T.; Lau, K.; Harvey, D.; Denny, K.G.; Barba, C.; Mefford, A.N. Early functional limitations in cognitively normal older adults predict diagnostic conversion to mild cognitive impairment. J. Am. Geriatr. Soc. 2017, 65, 1152–1158. [Google Scholar] [CrossRef]
- McAlister, C.; Schmitter-Edgecombe, M. Everyday functioning and cognitive correlates in healthy older adults with sub-jective cognitive concerns. Clin. Neuropsychol. 2016, 30, 1087–1103. [Google Scholar] [CrossRef]
- Monaci, L.; Morris, R.G. Neuropsychological screening performance and the association with activities of daily living and instrumental activities of daily living in dementia: Baseline and 18- to 24-month follow-up. Int. J. Geriatr. Psychiatry 2011, 27, 197–204. [Google Scholar] [CrossRef]
- Beaver, J.; Wilson, K.B.; Schmitter-Edgecombe, M. Characterising omission errors in everyday task completion and cognitive correlates in individuals with mild cognitive impairment and dementia. Neuropsychol. Rehabil. 2017, 29, 804–820. [Google Scholar] [CrossRef]
- Royall, D.R.; Chiodo, L.K.; Mouton, C.; Polk, M.J. Cognitive predictors of mortality in elderly retirees: Results from the freedom house study. Am. J. Geriatr. Psychiatry 2007, 15, 243–251. [Google Scholar] [CrossRef]
- Jekel, K.; Damian, M.; Wattmo, C.; Hausner, L.; Bullock, R.; Connelly, P.J.; Frölich, L. Mild cognitive impairment and deficits in in-strumental activities of daily living: A systematic review. Alzheimers Res. Ther. 2015, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, I.; Ntlholang, O.; Crosby, L.; Cunningham, C.; Lawlor, B. The clinical utility of naturalistic action test in differentiating mild cognitive impairment from early dementia in memory clinic. Int. J. Geriatr. Psychiatry 2016, 31, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Puente, A.N.; Terry, D.P.; Faraco, C.C.; Brown, C.L.; Miller, L.S. Functional impairment in mild cognitive impairment evidenced using performance-based measurement. J. Geriatr. Psychiatry Neurol. 2014, 27, 253–258. [Google Scholar] [CrossRef]
- Rueda, A.D.; Lau, K.M.; Saito, N.; Harvey, D.; Risacher, S.L.; Aisen, P.S.; Alzheimer’s Disease Neuroimaging Initiative. Self-rated and informant-rated everyday function in comparison to objective markers of Alzheimer’s disease. Alzheimers Dement. 2015, 11, 1080–1089. [Google Scholar] [CrossRef] [Green Version]
- Devi, J. The scales of functional assessment of activities of daily living in geriatrics. Age Ageing 2018, 47, 500–502. [Google Scholar] [CrossRef] [Green Version]
- Webster, L.; Groskreutz, D.; Grinbergs-Saull, A.; Howard, R.; O’Brien, J.T.; Mountain, G.; Livingston, G. Core outcome measures for in-terventions to prevent or slow the progress of dementia for people living with mild to moderate dementia: Systematic re-view and consensus recommendations. PLoS ONE 2017, 12, e0179521. [Google Scholar] [CrossRef] [Green Version]
- Wolfs, C.A.; Kessels, A.; Dirksen, C.D.; Severens, J.L.; Verhey, F.R. Integrated multidisciplinary diagnostic approach for dementia care: Randomised controlled trial. Br. J. Psychiatry 2008, 192, 300–305. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| CHP (n = 47) | MCI (n = 39) | AD (n = 44) | Post Hoc p-Values | |||
|---|---|---|---|---|---|---|
| HC vs. MCI | MCI vs. AD | HC vs. AD | ||||
| Demographics | ||||||
| Age Mean (±SD) Range | 77.94 (5.26) 68–91 | 82.08 (5.24) 71–96 | 82.41 (4.80) 74–92 | <0.001 | <0.001 | <0.001 |
| Gender * Female/male (n) | 26/21 | 11/28 | 12/32 | NS | ||
| Education, yrs Mean (±SD) Range | 12.40 (2.92) 8–16 | 11.95 (2.88) 6–16 | 10.52 (2.79) 6–16 | NS | NS | .007 |
| Cognition | ||||||
| MMSE TOTAL (./30) Mean (±SD) Range | 28.28 (1.40) 25 1–30 | 26.96 (1.70) 23–30 | 22.20 (22.45) 18–27 | <0.001 | <0.001 | <0.001 |
| CAMCOG TOTAL (./105) Mean (±SD) Range | 92.94 (4.46) 80–101 | 85.68 (3.93) 79–95 | 72.02 (8.93) 47–87 | <0.001 | <0.001 | <0.001 |
| CAMCOG MEMORY (./27) Mean (±SD) Range | 21.66 (1.72) 18–25 | 18.11 (2.98) 12–27 | 12.82 (3.50) 4–20 | <0.001 | <0.001 | <0.001 |
| ADL Indices b-ADL % | ||||||
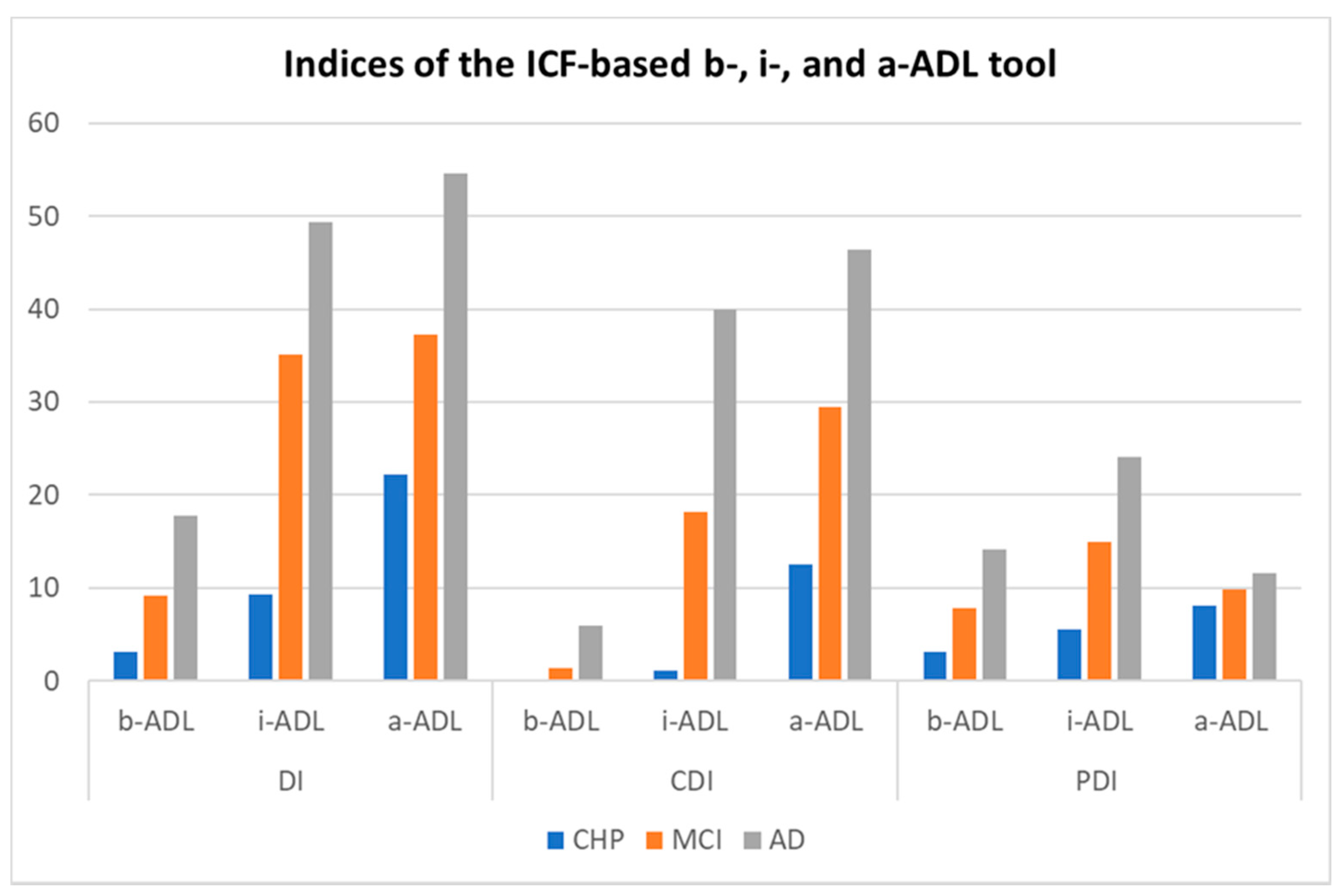
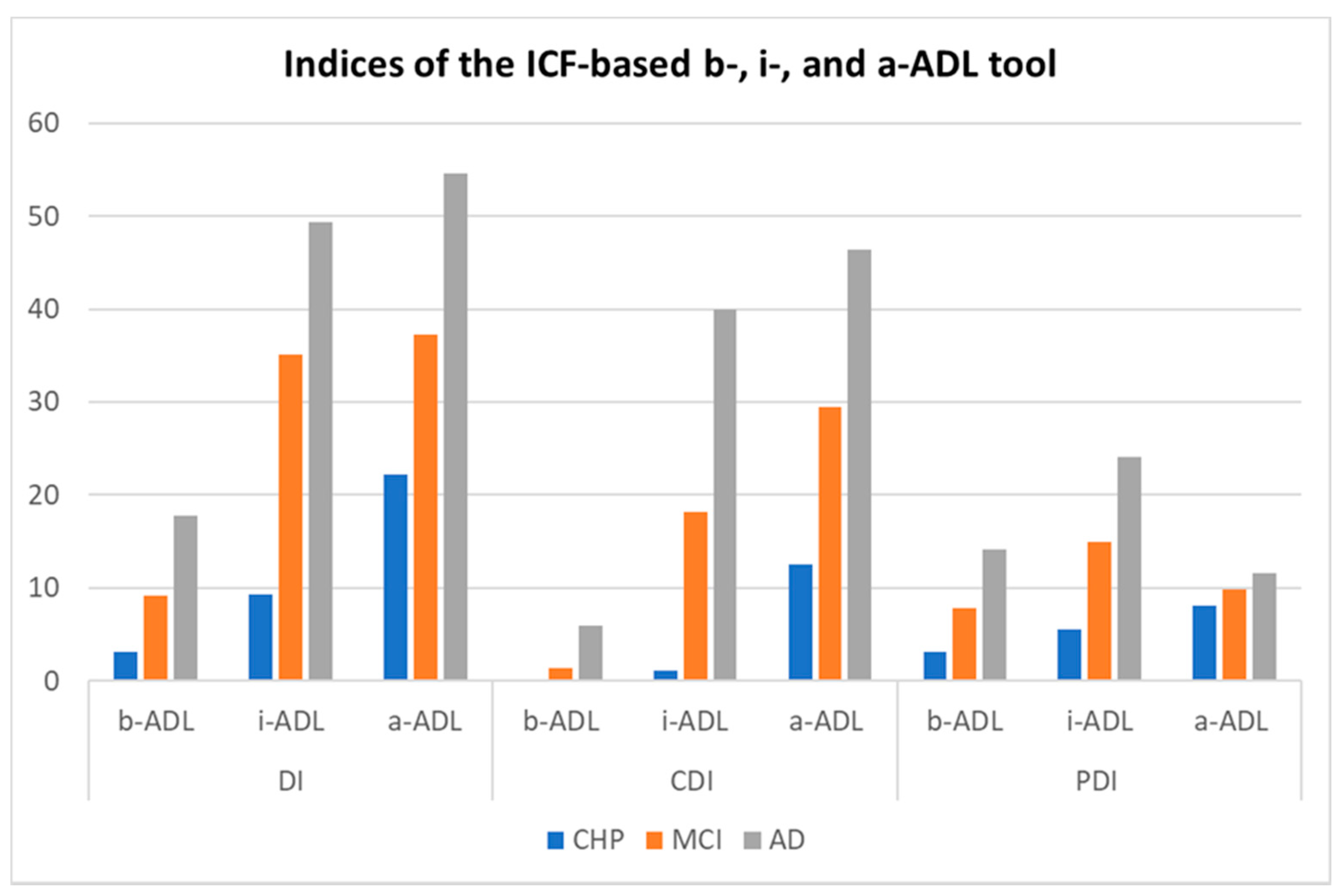
| b-ADL-DI Mean (±SD) Range | 2.30 (6.83) 0–42 | 9.19 (12.29) 0–38 | 18.66 (17.46) 0–75 | 0.044 | 0.003 | <0.001 |
| b-ADL-CDI Mean (±SD) Range | 0 (0) 0–0 | 1.83 (4.95) 0–17 | 6.53 (11.24) 0–54 | NS | 0.009 | <0.001 |
| b-ADL-PDI Mean (±SD) Range | 2.30 (6.83) 0–42 | 7.91 (11.58) 0–38 | 14.68 (17.25) 0–75 | NS | 0.047 | <0.001 |
| ADL Indices i-ADL % | ||||||
| i-ADL-DI Mean (±SD) Range | 9.47 (9.87) 0–50 | 35.76 (24.14) 0–86 | 51.70 (18.05) 6–94 | <0.001 | <0.001 | <0.001 |
| i-ADL-CDI Mean (±SD) Range | 1.19 (4.04) 0–25 | 19.31 (21.19) 0–72 | 36.09 (19.32) 0–86 | <0.001 | <0.001 | <0.001 |
| i-ADL-PDI Mean (±SD) Range | 5.57 (7.89) 0–28 | 14.26 (16.56) 0–64 | 20.46 (18.35) 0–83 | 0.023 | NS | <0.001 |
| ADL Indices a-ADL % | ||||||
| a-ADL-DI Mean (±SD) Range | 21.75 (12.13) 3–54 | 37.63 (21.89) 3–82 | 56.84 (17.71) 17–98 | <0.001 | <0.001 | <0.001 |
| a-ADL-CDI Mean (±SD) Range | 12.20 (16.34) 0–100 | 30.53 (21.41) 0–75 | 49.05 (19.40) 12–93 | <0.001 | <0.001 | <0.001 |
| a-ADL-PDI Mean (±SD) Range | 7.77 (8.44) 0–33 | 9.40 (10.80) 0–41 | 12.12 (12.60) 0–64 | NS | NS | NS |
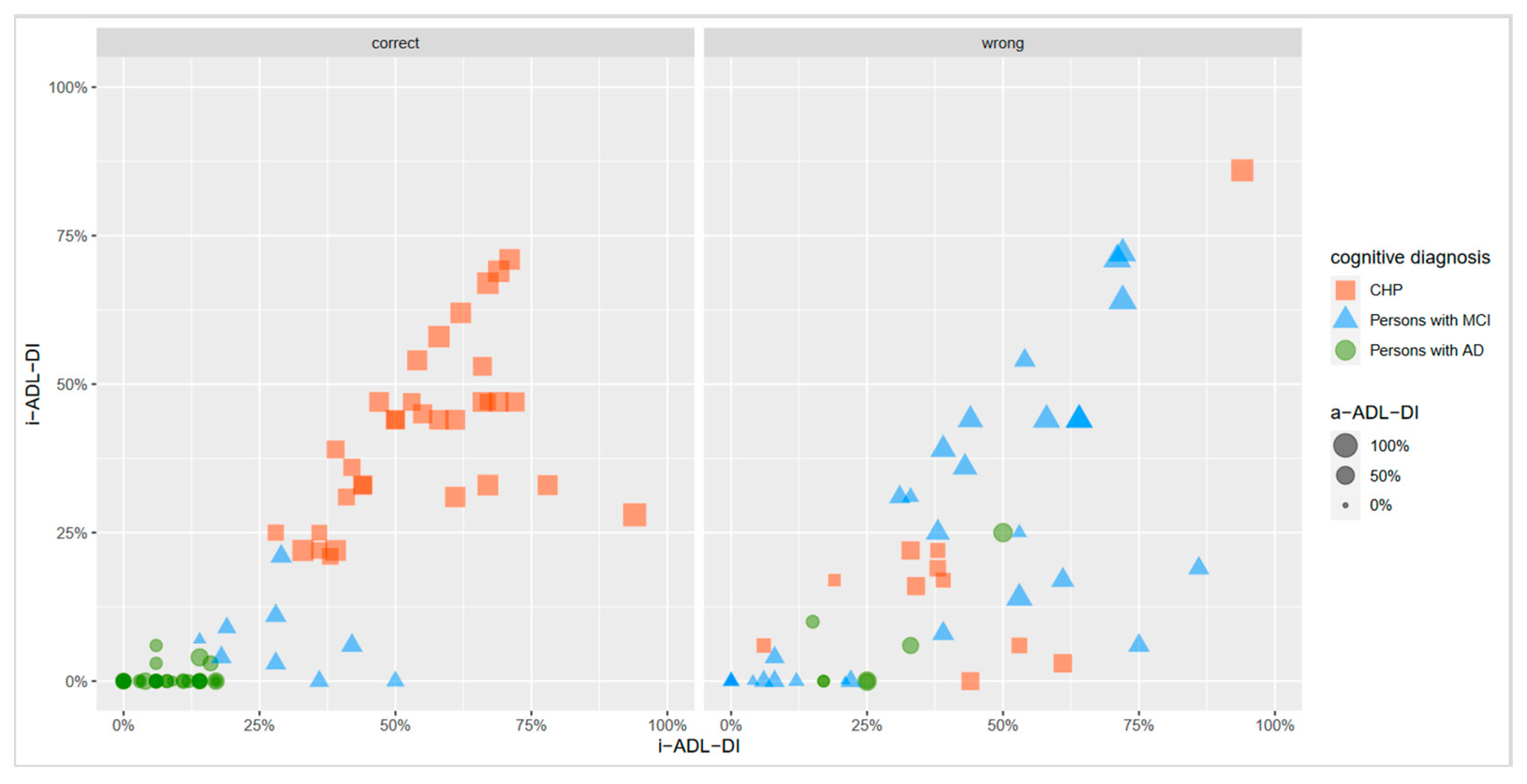
| Predicted Diagnosis | ||||
|---|---|---|---|---|
| CHP (n/%) | MCI (n/%) | AD (n/%) | ||
| Observed Diagnosis | CHP (n = 47) | 40 (85.10) | 6 (12.76) | 1 (2.13) |
| MCI (n = 39) | 11 (28.20) | 9 (23.10) | 19 (48.72) | |
| AD (n = 44) | 1 (2.27) | 10 (22.73) | 33 (75.00) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vriendt, P.; Cornelis, E.; Cools, W.; Gorus, E. The Usefulness of Evaluating Performance of Activities in Daily Living in the Diagnosis of Mild Cognitive Disorders. Int. J. Environ. Res. Public Health 2021, 18, 11623. https://doi.org/10.3390/ijerph182111623
De Vriendt P, Cornelis E, Cools W, Gorus E. The Usefulness of Evaluating Performance of Activities in Daily Living in the Diagnosis of Mild Cognitive Disorders. International Journal of Environmental Research and Public Health. 2021; 18(21):11623. https://doi.org/10.3390/ijerph182111623
Chicago/Turabian StyleDe Vriendt, Patricia, Elise Cornelis, Wilfried Cools, and Ellen Gorus. 2021. "The Usefulness of Evaluating Performance of Activities in Daily Living in the Diagnosis of Mild Cognitive Disorders" International Journal of Environmental Research and Public Health 18, no. 21: 11623. https://doi.org/10.3390/ijerph182111623
APA StyleDe Vriendt, P., Cornelis, E., Cools, W., & Gorus, E. (2021). The Usefulness of Evaluating Performance of Activities in Daily Living in the Diagnosis of Mild Cognitive Disorders. International Journal of Environmental Research and Public Health, 18(21), 11623. https://doi.org/10.3390/ijerph182111623