
Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review


Abstract
:1. Introduction
1.1. Targeting Retirement Communities
1.2. Peer-Led Interventions
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Type of Intervention
2.3. Inclusion/Exclusion Criteria
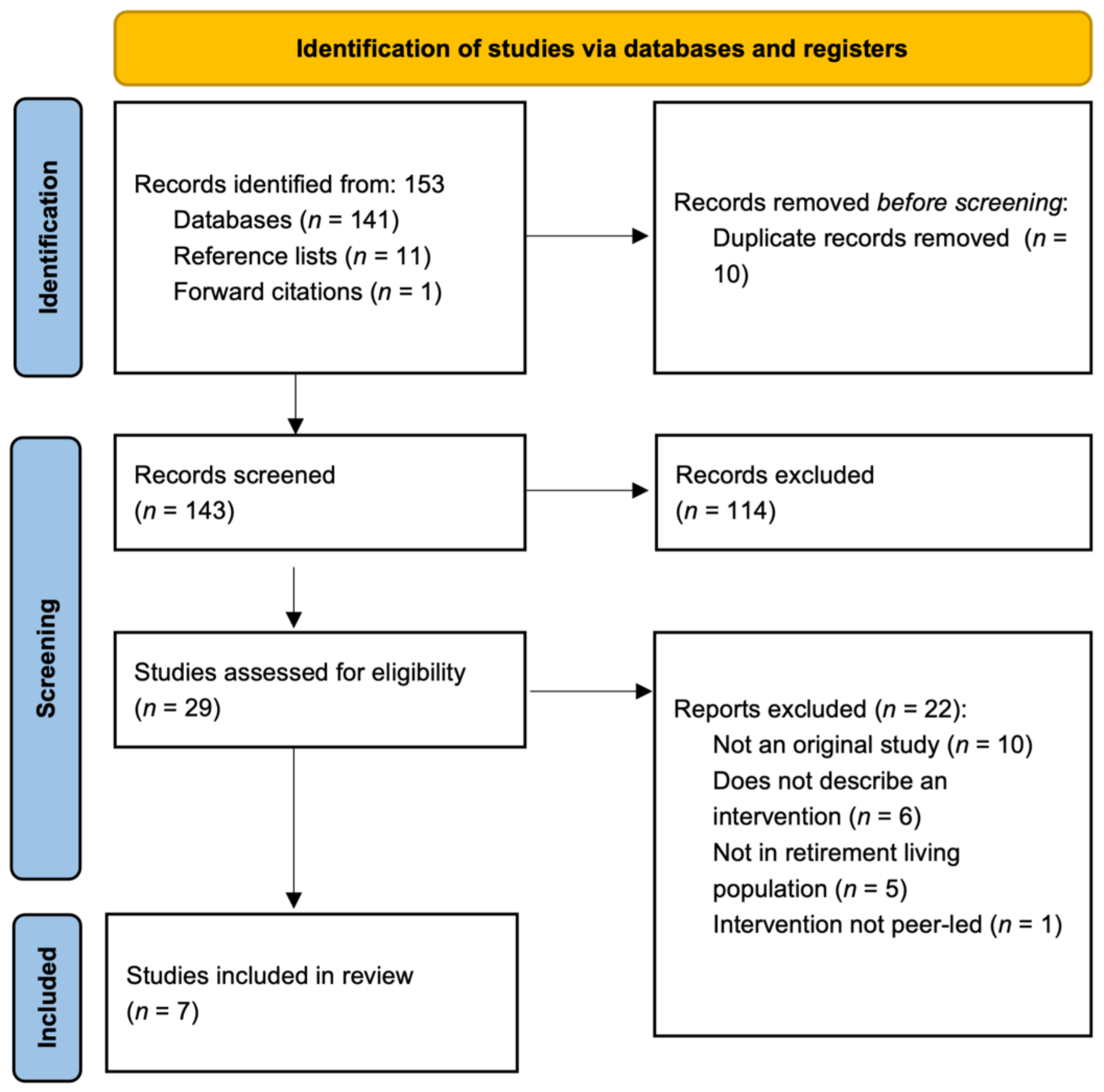
2.4. Study Selection
2.5. Reporting Quality and Risk of Bias Assessment
2.6. Data Extraction and Synthesis
3. Results
3.1. Overview of Studies
3.2. Reporting Quality and Risk of Bias Assessments
3.2.1. Reporting Quality
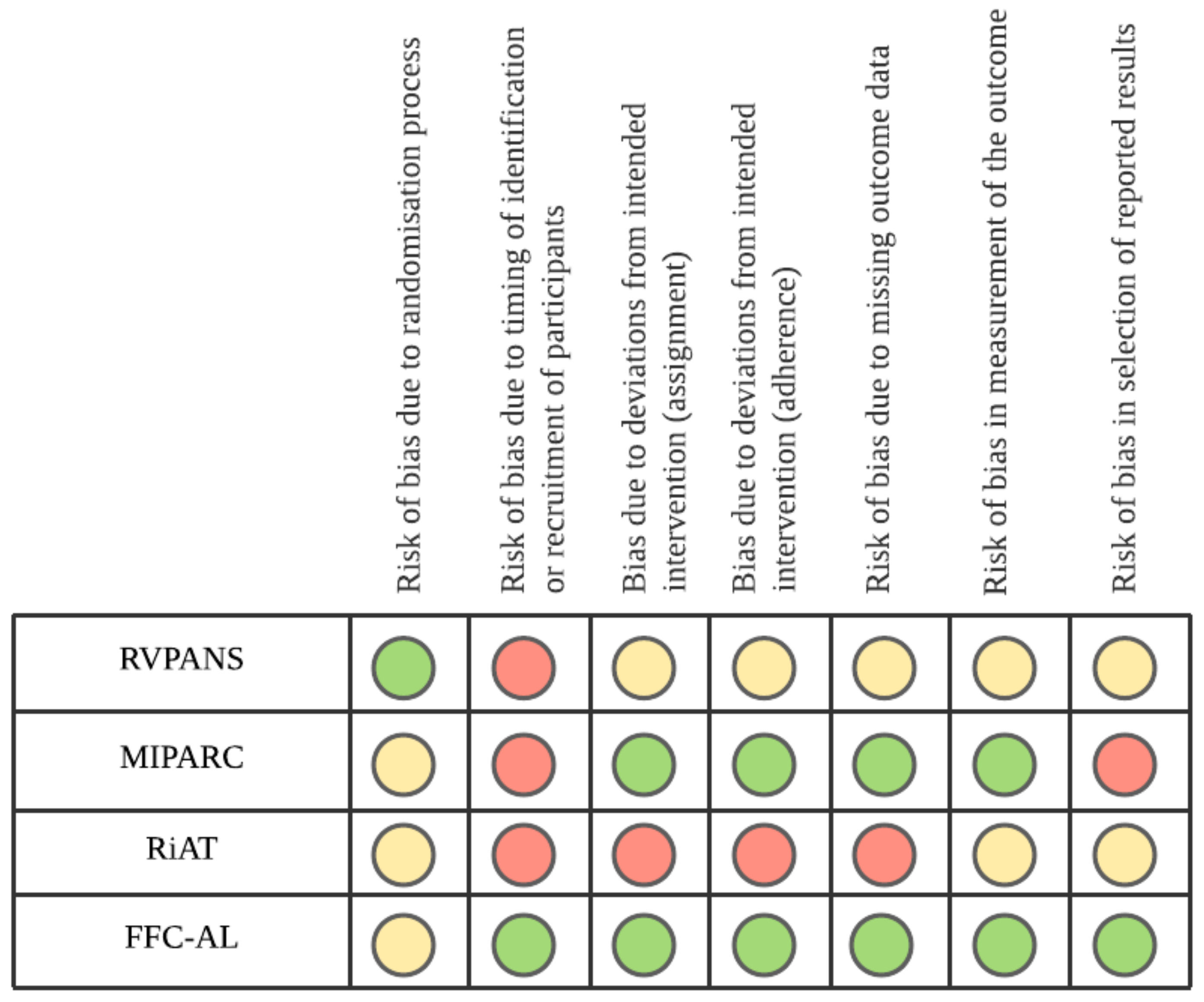
3.2.2. Risk of Bias in Cluster RCTs
Qualitative Assessment of Bias in Pre-Post Studies
3.3. Description of Interventions and Target Outcomes
Intervention Parameters
3.4. Effectiveness of Interventions to Change Health Behavior
3.5. Effectiveness of Interventions to Change Health Indicators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs—Population Division. World Population Ageing 2020 Highlights: Living Arrangements of Older Persons (ST/ESA/SER.A/451); United Nations: New York, NY, USA, 2020. [Google Scholar]
- Australian Institute of Health Welfare. Older Australia at a Glance; AIHW: Canberra, Australia, 2018.
- Kerr, J.; Rosenberg, D.; Millstein, R.A.; Bolling, K.; Crist, K.; Takemoto, M.; Godbole, S.; Moran, K.; Natarajan, L.; Castro-Sweet, C.; et al. Cluster randomized controlled trial of a multilevel physical activity intervention for older adults. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafortune, L.; Martin, S.; Kelly, S.; Kuhn, I.; Remes, O.; Cowan, A.; Brayne, C. Behavioural Risk Factors in Mid-Life Associated with Successful Ageing, Disability, Dementia and Frailty in Later Life: A Rapid Systematic Review. PLoS ONE 2016, 11, e0144405. [Google Scholar]
- Australian Institute of Health Welfare. Insufficient Physical Activity; AIHW: Canberra, Australia, 2020.
- Layne, J.E.; Sampson, S.E.; Mallio, C.J.; Hibberd, P.L.; Griffith, J.L.; Das, S.K.; Flanagan, W.J.; Castaneda-Sceppa, C. Successful Dissemination of a Community-Based Strength Training Program for Older Adults by Peer and Professional Leaders: The People Exercising Program. J. Am. Geriatr. Soc. 2008, 56, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Crosland, P.; Ananthapavan, J.; Davison, J.; Lambert, M.; Carter, R. The economic cost of preventable disease in Australia: A systematic review of estimates and methods. Aust. N. Z. J. Public Health 2019, 43, 484–495. [Google Scholar] [CrossRef]
- Australian Institute of Health Welfare. Mental Health Services in Australia; AIHW: Canberra, Australia, 2021.
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport Health Sci. 2021, 10, 29–47. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health Welfare. Physical Activity across the Life Stages; AIHW: Canberra, Australia, 2018.
- Conn, V.S.; Minor, M.A.; Burks, K.J.; Rantz, M.J.; Pomeroy, S.H. Integrative Review of Physical Activity Intervention Research with Aging Adults. J. Am. Geriatr. Soc. 2003, 51, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Lawson, P.J.; Flocke, S.A. Teachable moments for health behavior change: A concept analysis. Patient Educ. Couns. 2009, 76, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Holt, A.; Lee, A.H.; Jancey, J.; Kerr, D.; Howard, P. Are Retirement Villages Promoting Active Aging? J. Aging Phys. Act. 2016, 24, 407–411. [Google Scholar] [CrossRef]
- Jancey, J.; Holt, A.-M.; Lee, A.; Kerr, D.; Robinson, S.; Tang, L.; Anderson, A.; Hills, A.P.; Howat, P. Effects of a physical activity and nutrition program in retirement villages: A cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 92. [Google Scholar] [CrossRef] [Green Version]
- Thornton, G. National Overview of the Retirement Village Sector; Property Council of Australia: Adelaide, Australia, 2014. [Google Scholar]
- Kang, K.-H.; White, K.N.; Hayes, W.C.; Snow, C.M. Agility and Balance Differ between Older Community and Retirement Facility Residents. J. Appl. Gerontol. 2004, 23, 457–468. [Google Scholar] [CrossRef]
- Maher, C.A.; Burton, N.W.; Van Uffelen, J.G.; Brown, W.J.; Sprod, J.A.; Olds, T.S. Changes in use of time, activity patterns, and health and wellbeing across retirement: Design and methods of the life after work study. BMC Public Health 2013, 13, 952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webel, A.R.; Okonsky, J.; Trompeta, J.; Holzemer, W.L. A systematic review of the effectiveness of peer-based interventions on health-related behaviors in adults. Am. Public Health Assoc. 2010, 100, 247–253. [Google Scholar] [CrossRef]
- Posavac, E.J.; Kattapong, K.R.; Dew, D.E., Jr. Peer-Based Interventions to Influence Health-Related Behaviors and Attitudes: A Meta-Analysis. Psychol. Rep. 1999, 85, 1179–1194. [Google Scholar] [CrossRef] [PubMed]
- Ginis, K.A.M.; Nigg, C.; Smith, A. Peer-delivered physical activity interventions: An overlooked opportunity for physical activity promotion. Transl. Behav. Med. 2013, 3, 434–443. [Google Scholar] [CrossRef] [Green Version]
- Buman, M.; Giacobbi, P.R.; Dzierzewski, J.M.; Morgan, A.A.; McCrae, C.; Roberts, B.L.; Marsiske, M. Peer volunteers improve long-term maintenance of physical activity with older adults: A randomized controlled trial. J. Phys. Act. Health 2011, 8, S257–S266. [Google Scholar] [CrossRef] [Green Version]
- Grysztar, M.; Duplaga, M.; Wojcik, S.; Rodzinka, M. Effectiveness of peer-led health promotion interventions addressed to the elderly: Systematic review. Eur. J. Public Health 2017, 27, 3. [Google Scholar] [CrossRef] [Green Version]
- Salmon, J.; Hesketh, K.D.; Arundell, L.; Downing, K.L.; Biddle, S.J.H.; Hagger, M.S.; Cameron, L.D.; Hamilton, K.; Hankonen, N.; Lintunen, T. Changing behavior using ecological models. In The Handbook of Behavior Change; Hamilton, K., Cameron, L.D., Hagger, M.S., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: Cambridge, UK, 2020; pp. 237–250. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Reid, N.; Neuhaus, M.; Cyarto, L.V.; Barras, L. Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review PROSPERO 2021 CRD42021240589. 2021. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021240589 (accessed on 15 January 2021).
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V.E. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane. 2021. Available online: www.training.cochrane.org/handbook (accessed on 15 January 2021).
- Nanduri, A.P.; Fullman, S.; Morell, L.; Buyske, S.; Wagner, M.L. Pilot Study for Implementing an Osteoporosis Education and Exercise Program in an Assisted Living Facility and Senior Community. J. Appl. Gerontol. 2018, 37, 745–762. [Google Scholar] [CrossRef] [PubMed]
- Resnick, B.; Galik, E.; Vigne, E.; Carew, A.P. Dissemination and Implementation of Function Focused Care for Assisted Living. Health Educ. Behav. 2015, 43, 296–304. [Google Scholar] [CrossRef]
- Zlatar, Z.Z.; Godbole, S.; Takemoto, M.; Crist, K.; Sweet, C.M.C.; Kerr, J.; Rosenberg, D.E. Changes in Moderate Intensity Physical Activity Are Associated With Better Cognition in the Multilevel Intervention for Physical Activity in Retirement Communities (MIPARC) Study. Am. J. Geriatr. Psychiatry 2019, 27, 1110–1121. [Google Scholar] [CrossRef] [PubMed]
- Thøgersen-Ntoumani, C.; Quested, E.; Biddle, S.J.; Kritz, M.; Olson, J.; Burton, E.; Cerin, E.; Hill, K.D.; McVeigh, J.; Ntoumanis, N. Trial feasibility and process evaluation of a motivationally-embellished group peer led walking intervention in retirement villages using the RE-AIM framework: The residents in action trial (RiAT). Health Psychol. Behav. Med. 2019, 7, 202–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnick, B.; Galik, E.; Gruber-Baldini, A.; Zimmerman, S. Testing the Effect of Function-Focused Care in Assisted Living. J. Am. Geriatr. Soc. 2011, 59, 2233–2240. [Google Scholar] [CrossRef]
- Burton, E.; Farrier, K.; Hill, K.D.; Codde, J.; Airey, P.; Hill, A.-M. Effectiveness of peers in delivering programs or motivating older people to increase their participation in physical activity: Systematic review and meta-analysis. J. Sports Sci. 2018, 36, 666–678. [Google Scholar] [CrossRef] [Green Version]
- Kritz, M.; Thøgersen-Ntoumani, C.; Mullan, B.; McVeigh, J.; Ntoumanis, N. Effective Peer Leader Attributes for the Promotion of Walking in Older Adults. Gerontologist 2020, 60, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.E.; Brennan, G.; Matthews, A.; McAdam, C.; Fitzsimons, C.; Mutrie, N. Recruiting participants to walking intervention studies: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 137. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
|
|
|
|
| Program | n | Design | Main Results |
|---|---|---|---|
| PBH | 40 | Pilot pre-post | Better performance on:
|
| FFC-AL | 3676 | Pre-post | Reduction in falls |
| FF-AL | 171 | Pilot RCT | Improvement in physical function (Barthel Index) at 12-months |
| RiAT | 116 | Quasi-RCT | Higher daily step count and total stepping time |
| RVPANS | 363 | Cluster RCT | Decreased:
|
| MIPARC | 307 | Cluster RCT | Increased participation in moderate-to-vigorous physical activity, and improved blood pressure. Increases in physical activity, regardless of group, led to improvements in cognition |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barras, L.; Neuhaus, M.; Cyarto, E.V.; Reid, N. Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11557. https://doi.org/10.3390/ijerph182111557
Barras L, Neuhaus M, Cyarto EV, Reid N. Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(21):11557. https://doi.org/10.3390/ijerph182111557
Chicago/Turabian StyleBarras, Lilian, Maike Neuhaus, Elizabeth V. Cyarto, and Natasha Reid. 2021. "Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 21: 11557. https://doi.org/10.3390/ijerph182111557
APA StyleBarras, L., Neuhaus, M., Cyarto, E. V., & Reid, N. (2021). Effectiveness of Peer-Led Wellbeing Interventions in Retirement Living: A Systematic Review. International Journal of Environmental Research and Public Health, 18(21), 11557. https://doi.org/10.3390/ijerph182111557