
Years of Life Lost (YLL) Due to Short-Term Exposure to Ambient Air Pollution in China: A Systematic Review and Meta-Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Collection
2.4. Methodological Quality Assessment
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
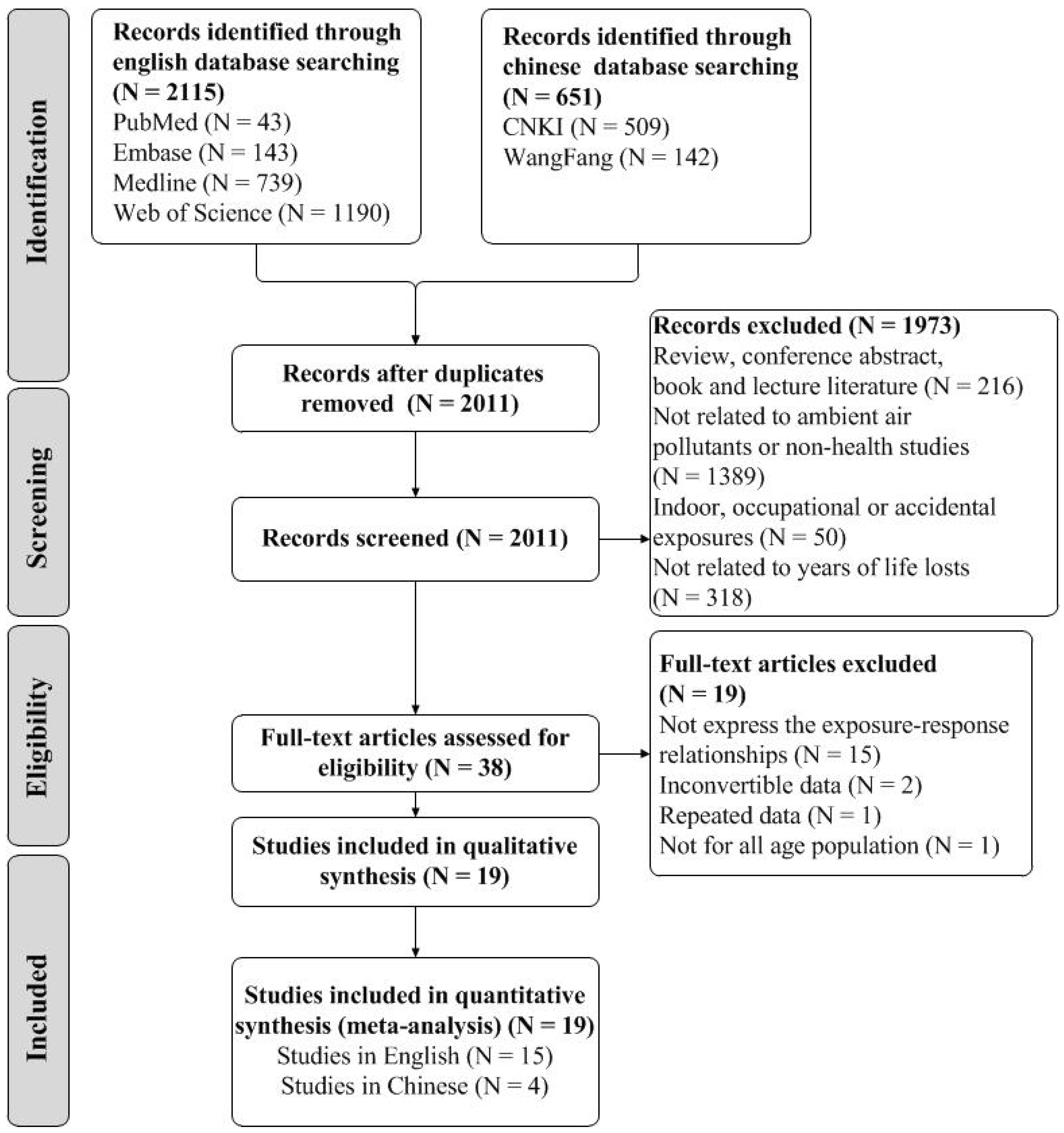
3.1. Literature Retrieval
3.2. Characteristics and Quality of the Included Studies
3.3. Risk of Bias Assessment
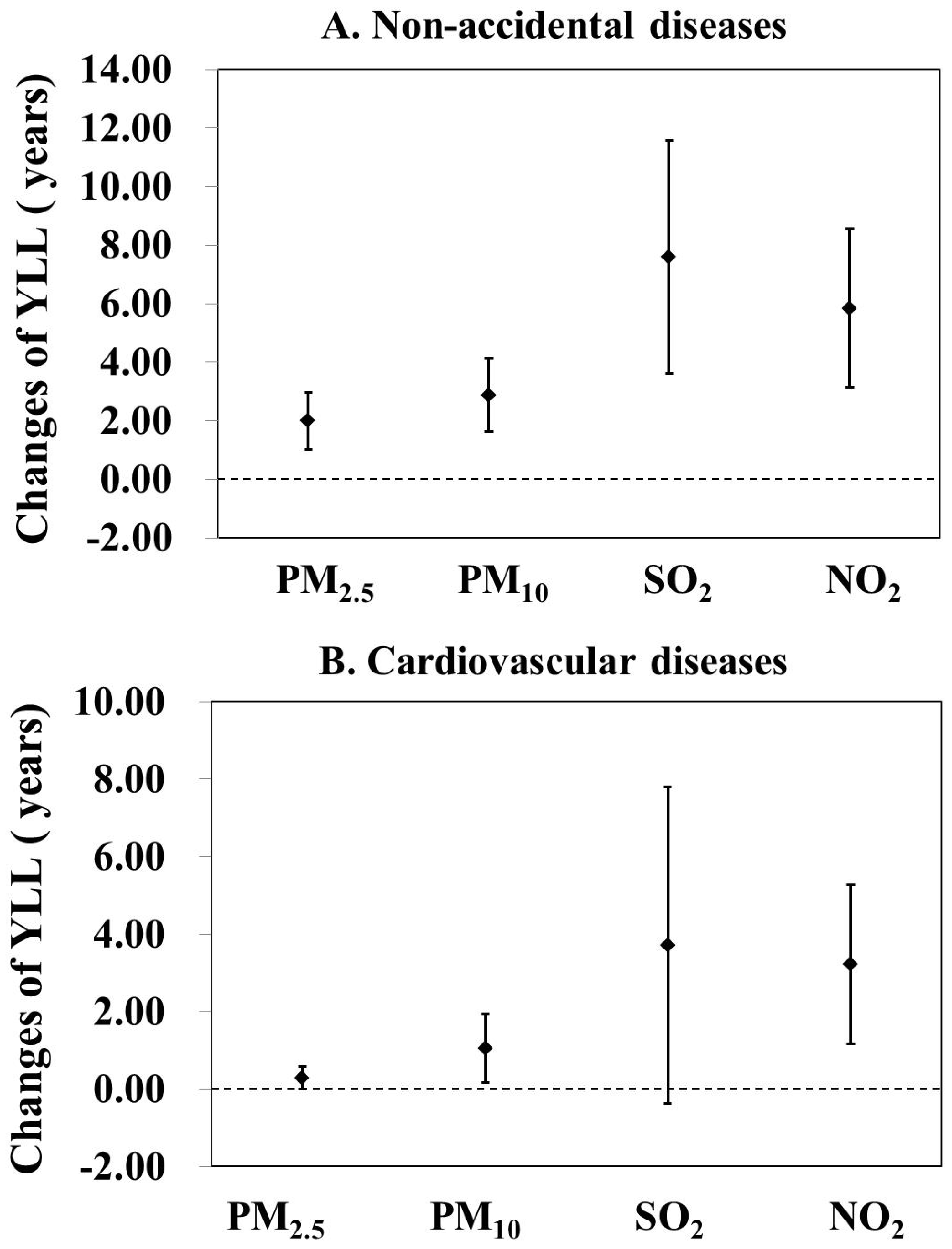
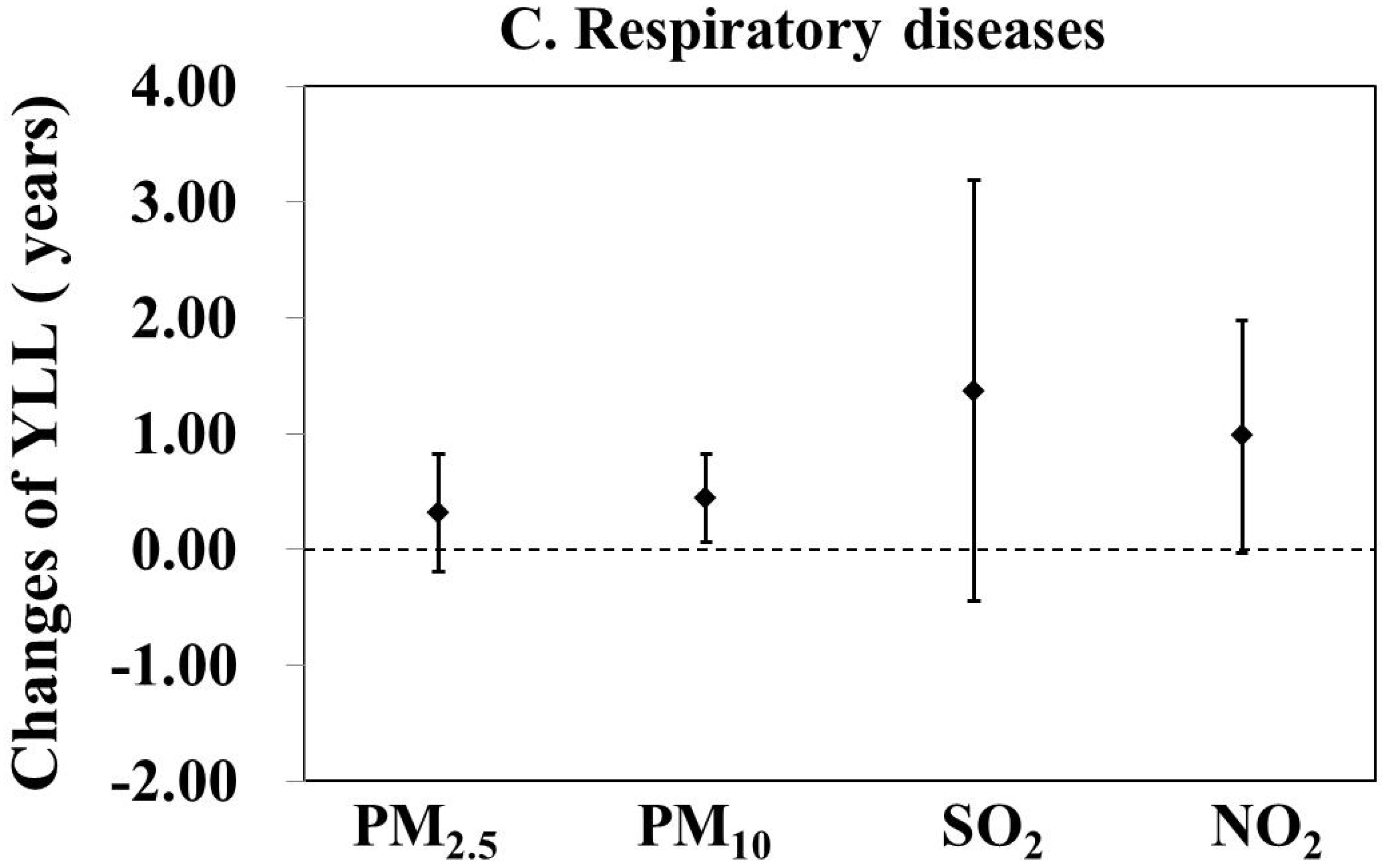
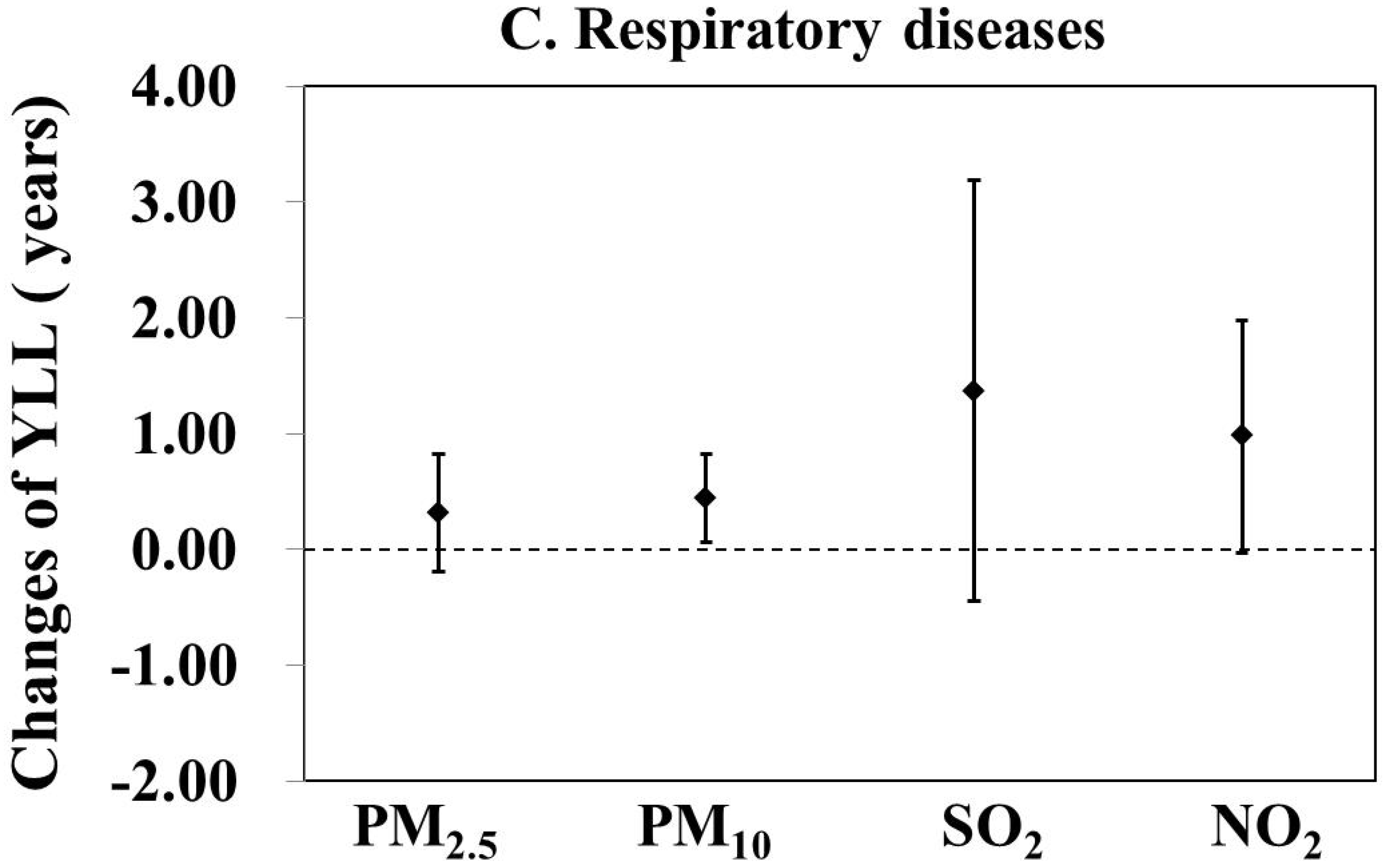
3.4. Associations between Ambient Air Pollution and Cause-Specific YLL
3.5. Subgroup Analysis by Gender and Age
3.6. Publication Bias and Sensitivity Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Z.; Wang, J.; Ma, G.; Zhang, Y. China tackles the health effects of air pollution. Lancet 2013, 382, 1959–1960. [Google Scholar] [CrossRef]
- van Donkelaar, A.; Martin, R.V.; Brauer, M.; Kahn, R.; Levy, R.; Verduzco, C.; Villeneuve, P.J. Global estimates of ambient fine particulate matter concentrations from satellite-based aerosol optical depth: Development and application. Environ. Health Perspect. 2010, 118, 847–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Mauzerall, D.L.; Zhu, T.; Liang, S.; Ezzati, M.; Remais, J.V. Environmental health in China: Progress towards clean air and safe water. Lancet 2010, 375, 1110–1119. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Wang, X.; Liu, T.; Li, X.; Xiao, J.; Zeng, W.; Ma, W. Air pollution and mortality in china. Adv. Exp. Med. Biol. 2017, 1017, 103–121. [Google Scholar] [PubMed]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.; Saldiva, P.H.; Lavigne, E.; Matus, P.; et al. Ambient particulate air pollution and daily mortality in 652 cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- Yu, Y.; Yao, S.; Dong, H.; Wang, L.; Wang, C.; Ji, X.; Ji, M.; Yao, X.; Zhang, Z. Association between short-term exposure to particulate matter air pollution and cause-specific mortality in Changzhou, China. Environ. Res. 2019, 170, 7–15. [Google Scholar] [CrossRef]
- Guo, Y.; Li, S.; Tian, Z.; Pan, X.; Zhang, J.; Williams, G. The burden of air pollution on years of life lost in Beijing, China, 2004–2008: Retrospective regression analysis of daily deaths. BMJ 2013, 347, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.L.; Salomon, J.A.; Mathers, C.D.; Lopez, A.D. Summary Measures of Population Health: Concepts, Ethics, Measurement and Applications. 2002. Available online: https://apps.who.int/iris/bitstream/handle/10665/42439/9241545518.pdf;jsessionid=31F08B0B483B99037EB1733523B7A7AC?sequence=1 (accessed on 28 October 2021).
- Gao, T.; Wang, X.; Chen, R.; Ngo, H.H.; Guo, W. Disability adjusted life year (daly): A useful tool for quantitative assessment of environmental pollution. Sci. Total Environ. 2015, 511, 268–287. [Google Scholar] [CrossRef]
- Castillo-Rodríguez, L.; Díaz-Jiménez, D.; Castañeda-Orjuela, C.; De la Hoz-Restrepo, F. Years of life lost (yll) in colombia 1998–2011: Overall and avoidable causes of death analysis. PLoS ONE 2015, 10, e0125456. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.J.; Kim, H.S.; Ha, J.; Kim, E.J. Measuring the environmental burden of disease in South Korea: A population-based study. Int. J. Environ. Res. Public Health 2015, 12, 7938–7948. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). State-specific smoking-attributable mortality and years of potential life lost--united states, 2000–2004. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 29–33. [Google Scholar]
- Al-Hemoud, A.; Gasana, J.; Al-Dabbous, A.; Al-Shatti, A.; Al-Khayat, A. Disability adjusted life years (dalys) in terms of years of life lost (yll) due to premature adult mortalities and postneonatal infant mortalities attributed to pm2.5 and pm10 exposures in kuwait. Int. J. Environ. Res. Public Health 2018, 15, 2609. [Google Scholar] [CrossRef] [Green Version]
- Dhaini, H.R.; Salameh, T.; Waked, A.; Sauvage, S.; Borbon, A.; Formenti, P.; Doussin, J.; Locoge, N.; Afif, C. Quantitative cancer risk assessment and local mortality burden for ambient air pollution in an eastern mediterranean city. Environ. Sci. Pollut. Res. Int. 2017, 24, 14151–14162. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Faridi, S.; Shamsipour, M.; Krzyzanowski, M.; Künzli, N.; Amini, H.; Azimi, F.; Malkawi, M.; Momeniha, F.; Gholampour, A.; Hassanvand, M.S.; et al. Long-term trends and health impact of pm(2.5) and o(3) in tehran, iran, 2006–2015. Environ. Int. 2018, 114, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Mazroa, M.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Zhou, M.; Wang, L.; Li, Y.; Liu, Y.; Liu, J.; You, J.; Yin, P. Burden of disease attributable to ambient particulate matter pollution in 1990 and 2010 in china. Chin. J. Prev. Med. 2015, 49, 327–333. (In Chinese) [Google Scholar]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in china, 1990–2010: Findings from the global burden of disease study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Chen, F.; Qiao, Z.; Fan, Z.; Zheng, Q.; Wu, Y.; Zhang, M.; Cui, Y.; Deng, Y.; Luo, B.; Zhang, W.; et al. The effects of sulphur dioxide on acute mortality and years of life lost are modified by temperature in chengdu, china. Sci. Total Environ. 2017, 576, 775–784. [Google Scholar] [CrossRef]
- He, T.; Yang, Z.; Liu, T.; Shen, Y.; Fu, X.; Qian, X.; Zhang, Y.; Wang, Y.; Xu, Z.; Zhu, S.; et al. Ambient air pollution and years of life lost in ningbo, china. Sci. Rep. 2016, 6, 10. [Google Scholar]
- Huang, J.; Li, G.; Xu, G.; Qian, X.; Zhao, Y.; Pan, X.; Huang, J.; Cen, Z.; Liu, Q.; He, T.; et al. The burden of ozone pollution on years of life lost from chronic obstructive pulmonary disease in a city of yangtze river delta, china. Environ. Pollut. 2018, 242, 1266–1273. [Google Scholar] [CrossRef]
- Liang, H.; Qiu, H.; Tian, L. Short-term effects of fine particulate matter on acute myocardial infraction mortality and years of life lost: A time series study in hong kong. Sci. Total Environ. 2018, 615, 558–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Ou, C.; Song, Y.; Li, L.; Chen, P.; Liu, Q. Estimating years of life lost from cardiovascular mortality related to air pollution in guangzhou, china. Sci. Total Environ. 2016, 573, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Wu, Z.; Jiang, G.; Wu, X.; Li, P.; Ni, Y.; Xiong, X.; Wang, X.; Parasat; Li, G.; et al. The association between ambient inhalable particulate matter and the disease burden of respiratory disease: An ecological study based on ten-year time series data in tianjin, china. Environ. Res. 2017, 157, 71–77. [Google Scholar] [CrossRef]
- Zeng, Q.; Ni, Y.; Li, G.; Wang, D.; Li, P.; Zheng, W.; Wang, X.; Jiang, G. The quantitative assessment of the public excess disease burden advanced by inhalable particulate matter under different air quality standard targets in Tianjin, China. Environ. Sci. Pollut. Res. Int. 2019, 26, 6931–6938. [Google Scholar] [CrossRef]
- Zhang, Y.; Peng, M.; Yu, C.; Zhang, L. Burden of mortality and years of life lost due to ambient pm10 pollution in Wuhan, China. Environ. Pollut. 2017, 230, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Deng, Z.; Deng, Y.; Qiao, Z.; Lan, L.; Meng, Q.; Luo, B.; Zhang, W.; Ji, K.; Qiao, X.; et al. Attributable risk of ambient pm10 on daily mortality and years of life lost in chengdu, china. Sci. Total Environ. 2017, 581, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhang, X.; Zhang, X.; Dong, M.; Wu, J.; Dong, Y.; Chen, R.; Ding, X.; Huang, C.; Zhang, Q.; et al. The burden of ambient air pollution on years of life lost in wuxi, china, 2012–2015: A time-series study using a distributed lag non-linear model. Environ. Pollut. 2017, 224, 689–697. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schunemann, H.J. Identifying the peco: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Booth, A. Unpacking your literature search toolbox: On search styles and tactics. Health Inf. Libr. J. 2008, 25, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Szyszkowicz, M.; Kousha, T.; Kingsbury, M.; Colman, I. Air pollution and emergency department visits for depression: A multicity case-crossover study. Environ. Health Insights 2016, 10, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Fan, S.; Heinrich, J.; Bloom, M.S.; Zhao, T.Y.; Shi, T.; Feng, W.; Sun, Y.; Shen, J.; Yang, Z.; Yang, Y.; et al. Ambient air pollution and depression: A systematic review with meta-analysis up to 2019. Sci. Total Environ. 2020, 701, 134721. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Qian, Z.; Howard, S.W.; Vaughn, M.G.; Fan, S.; Liu, K.; Dong, G. Global association between ambient air pollution and blood pressure: A systematic review and meta-analysis. Environ. Pollut. 2018, 235, 576–588. [Google Scholar] [CrossRef] [PubMed]
- Achilleos, S.; Kioumourtzoglou, M.A.; Wu, C.; Schwartz, J.D.; Koutrakis, P.; Papatheodorou, S.I. Acute effects of fine particulate matter constituents on mortality: A systematic review and meta-regression analysis. Environ. Int. 2017, 109, 89–100. [Google Scholar] [CrossRef]
- Li, X.; Chen, Q.; Zheng, X.; Li, Y.; Han, M.; Liu, T.; Xiao, J.; Guo, L.; Zeng, W.; Zhang, J.; et al. Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis. Sci. Total Environ. 2019, 691, 549–561. [Google Scholar] [CrossRef]
- Mustafic, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Périer, M.; Marijon, E.; Vernerey, D.; Empana, J.; et al. Main air pollutants and myocardial infarction: A systematic review and meta-analysis. JAMA 2012, 307, 713–721. [Google Scholar] [CrossRef]
- Zheng, X.; Ding, H.; Jiang, L.; Chen, S.; Zheng, J.; Qiu, M.; Zhou, Y.; Chen, Q.; Guan, W. Association between air pollutants and asthma emergency room visits and hospital admissions in time series studies: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Sutton, P.; Kalkbrenner, A.; Windham, G.; Halladay, A.; Koustas, E.; Lawler, C.; Davidson, L.; Daniels, N.; Newschaffer, C.; et al. A systematic review and meta-analysis of multiple airborne pollutants and autism spectrum disorder. PLoS ONE 2016, 11, e0161851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OHAT (Office of Health Assessment and Translation). Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration. 2019. Available online: https://ntp.niehs.nih.gov/ntp/ohat/pubs/handbookmarch2019_508.pdf (accessed on 28 October 2021).
- Forouzanfar, M.H.; Lily, A.; Anderson, H.R.; Bachman, V.F.; Stan, B.; Michael, B.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, V.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 386, 36. [Google Scholar] [CrossRef] [Green Version]
- Thurston, G.D.; Ito, K. Epidemiological studies of acute ozone exposures and mortality. J. Exposure Anal. Environ. Epidemiol. 2001, 11, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, P.; Chen, R.; Wang, L.; Meng, X.; Liu, C.; Niu, Y.; Lin, Z.; Liu, Y.; Liu, J.; Qi, J.; et al. Ambient ozone pollution and daily mortality: A nationwide study in 272 chinese cities. Environ. Health Perspect. 2017, 125, 117006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G.M. Advances in the meta-analysis of heterogeneous clinical trials i: The inverse variance heterogeneity model. Contemp. Clin. Trials 2015, 45, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Doi, S.A.; Furuya-Kanamori, L.; Thalib, L.; Barendregt, J.J. Meta-analysis in evidence-based healthcare: A paradigm shift away from random effects is overdue. Int. J. Evid. Based Healthc. 2017, 15, 152–160. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Dzhambov, A.M.; Dimitrova, D.D. Residential road traffic noise as a risk factor for hypertension in adults: Systematic review and meta-analysis of analytic studies published in the period 2011–2017. Environ. Pollut. 2018, 240, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef]
- Huang, J.; Li, G.; Qian, X.; Xu, G.; Zhao, Y.; Huang, J.; Liu, Q.; He, T.; Guo, X. The burden of ischemic heart disease related to ambient air pollution exposure in a coastal city in south china. Environ. Res. 2018, 164, 255–261. [Google Scholar] [CrossRef]
- Li, G.; Huang, J.; Xu, G.; Pan, X.; Qian, X.; Xu, J.; Zhao, Y.; Zhang, T.; Liu, Q.; Guo, X.; et al. The short term burden of ambient fine particulate matter on chronic obstructive pulmonary disease in Ningbo, China. Environ. Health 2017, 16, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, F.; Zhou, L.; Xu, Y.; Zheng, T.; Guo, Y.; Wellenius, G.; Bryan, A.; Chen, X.; Wang, H.; Zheng, X. Short-term effects of air pollution on daily mortality and years of life lost in Nanjing, China. Sci. Total Environ. 2015, 536, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Ni, Y.; Jiang, G.; Li, G.; Pan, X. The short term burden of ambient particulate matters on non-accidental mortality and years of life lost: A ten-year multi-district study in Tianjin, China. Environ. Pollut. 2017, 220, 713–719. [Google Scholar] [CrossRef]
- Zeng, Q.; Wu, Z.; Jiang, G.; Li, P.; Ni, Y.; Li, G.; Pan, X. The association between inhalable particulate matter and YLL caused by copd in a typical city in northern china. Atmos. Environ. 2018, 172, 26–31. [Google Scholar] [CrossRef]
- Li, J.; Wang, H.; Qu, L.; Zhao, M.; Ding, X.; Xie, C.; Liu, Q. Short term effect of pm2.5 on cardiovascular mortality inresidents in changping district, Beijing. Zhonghua Liu Xing Bing Xue Za Zhi 2019, 40, 331–334. (In Chinese) [Google Scholar]
- Ni, Y.; Zeng, Q.; Li, G. Time-series study of the influence of sulfur dioxide on years of life lost due to premature mortality in nankai districts, tianjin. J. Publ. Health Prev. Med. 2017, 28, 8–12. (In Chinese) [Google Scholar]
- Ni, Y.; Zeng, Q.; Li, G. Health effects of nitrogen dioxide based on burden of disease in six urban areas of Tianjin. J. Environ. Health 2017, 34, 408–411. (In Chinese) [Google Scholar]
- Zeng, Q.; Li, P.; Ni, Y.; Li, G.; Wang, D.; Pan, X.; Jiang, G. Research on the relationship between atmospheric inhalable particulate mater and cardiovascular disease burden in Tianjin. Zhonghua Xin Xue Guan Bing Za Zhi 2018, 46, 50–55. (In Chinese) [Google Scholar]
- Lai, H.K.; Tsang, H.; Wong, C.M. Meta-analysis of adverse health effects due to air pollution in chinese populations. BMC Public Health 2013, 13, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, Y.; Sun, Z.; Cao, J.; Wang, X.; Zhong, L.; Bi, X.; Li, H.; Liu, W.; Zhu, T.; Huang, W. Systematic review of chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 2013, 54, 100–111. [Google Scholar] [CrossRef]
- Huang, J.; Pan, X.; Guo, X.; Li, G. Health impact of china’s air pollution prevention and control action plan: An analysis of national air quality monitoring and mortality data. Lancet Planet. Health 2018, 2, e313–e323. [Google Scholar] [CrossRef] [Green Version]
- Kan, H.; Chen, B.; Zhao, N.; London, S.J.; Song, G.; Chen, G.; Zhang, Y.; Jiang, L. Part 1. A time-series study of ambient air pollution and daily mortality in Shanghai, China. Res. Rep. Health Eff. Inst. 2010, 154, 17–78. [Google Scholar]
- Ohlwein, S.; Kappeler, R.; Kutlar, J.M.; Künzli, N.; Hoffmann, B. Health effects of ultrafine particles: A systematic literature review update of epidemiological evidence. Int. J. Public Health 2019, 64, 547–559. [Google Scholar] [CrossRef] [PubMed]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Envirion. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef]
- Yang, J.; Zhou, M.; Li, M.; Yin, P.; Hu, J.; Zhang, C.; Wang, H.; Liu, Q.; Wang, B. Fine particulate matter constituents and cause-specific mortality in china: A nationwide modelling study. Environ. Int. 2020, 143, 105927. [Google Scholar] [CrossRef]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient pm2.5 and pm10 pollution in the chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef]
- Bell, M.L.; Zanobetti, A.; Dominici, F. Evidence on vulnerability and susceptibility to health risks associated with short-term exposure to particulate matter: A systematic review and meta-analysis. Am. J. Epidemiol. 2013, 178, 865–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, W.D.; Zeman, K.L.; Kim, C. Variability of fine particle deposition in healthy adults: Effect of age and gender. Am. J. Respir. Crit. Care Med. 1996, 153, 1641–1647. [Google Scholar] [CrossRef]
- Goldberg, M.S.; Burnett, R.T.; Stieb, D.M.; Brophy, J.M.; Daskalopoulou, S.S.; Valois, M.F.; Brook, J.R. Associations between ambient air pollution and daily mortality among elderly persons in montreal, quebec. Sci. Total Environ. 2013, 463–464, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Wuthrich, B.; Schmid-Grendelmeier, P.; Schindler, C.; Imboden, M.; Bircher, A.; Zemp, E.; Probst-Hensch, N.; SAPALDIA Team. Prevalence of atopy and respiratory allergic diseases in the elderly sapaldia population. Int. Arch. Allergy Immunol. 2013, 162, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Mayvaneh, F.; Baaghideh, M.; Entezari, A.; Ho, H.C.; Xiang, Q.; Jiao, A.; Zhang, F.; Hu, K.; Chen, G.; et al. Utilizing daily excessive concentration hours to estimate cardiovascular mortality and years of life lost attributable to fine particulate matter in tehran, iran. Sci. Total Environ. 2020, 703, 134909. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; Dandona, L.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Sun, M.; Yan, W.; Fang, K.; Chen, D.; Liu, J.; Chen, Y.; Duan, J.; Chen, R.; Sun, Z.; Wang, X.; et al. The correlation between pm2.5 exposure and hypertensive disorders in pregnancy: A meta-analysis. Sci. Total Environ. 2020, 703, 134985. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, K.; Mathers, C.D.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J. Global and regional estimates of cancer mortality and incidence by site: Ii. Results for the global burden of disease 2000. BMC Cancer 2002, 2, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Li, R.; Li, W.; Wang, M.; Cao, Y.; Wu, Z.; Xu, Q. The association between ambient air pollution and daily mortality in beijing after the 2008 olympics: A time series study. PLoS ONE 2013, 8, e76759. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Air Pollutants | No. of Studies | Effect Estimates (95% CI) (Years) | I2 (%) | τ2 | |
|---|---|---|---|---|---|
| COPD | PM2.5 | 2 | 1.37 (0.24, 2.50) R | 57.6 | 0.401 |
| PM10 | 2 | 0.50 (0.01, 0.99) R | 67.7 | 0.088 | |
| O3 | 1 | 1.21 (0.12, 2.30) | — | 0.000 | |
| IHD | PM2.5 | 1 | 0.71 (−0.21, 1.64) | — | 0.000 |
| PM10 | 3 | 0.84 (0.12, 1.57) R | 86.2 | 0.349 | |
| SO2 | 2 | 1.67 (−0.93, 4.27) R | 75.6 | 2.775 | |
| NO2 | 2 | 1.18 (−0.24, 2.59) R | 54.1 | 0.667 | |
| Stroke | PM10 | 3 | 0.71 (0.44, 1.00) F | 20.2 | 0.018 |
| SO2 | 1 | 0.90 (0.10, 1.60) | — | 0.000 | |
| NO2 | 1 | 0.60 (0.10, 1.20) | — | 0.000 | |
| AMI | PM2.5 | 1 | 1.69 (0.01, 3.37) | — | 0.000 |
| SO2 | 1 | 4.97 (0.28, 9.66) | — | 0.000 | |
| NO2 | 1 | 0.62 (−0.92, 2.17) | — | 0.000 | |
| O3 | 1 | −0.15 (−1.28, 0.09) | — | 0.000 | |
| Diabetes mellitus | PM2.5 | 1 | 0.06 (−0.31, 0.43) | — | 0.000 |
| PM10 | 1 | 0.01 (−0.29, 0.30) | — | 0.000 | |
| SO2 | 1 | 0.11 (−0.98, 1.20) | — | 0.000 | |
| NO2 | 1 | 0.94 (−0.04, 1.92) | — | 0.000 |
| Diseases | Air Pollutants | Subgroup | n | Effect Estimate (95% CI) (Years) | I2(%) | τ2 |
|---|---|---|---|---|---|---|
| Non-accidental diseases | PM2.5 | Female | 3 | 1.30 (0.70, 1.90) F | 0.0% | 0.000 |
| Male | 3 | 0.67 (−0.05, 1.39) F | 0.0% | 0.000 | ||
| Younger | 3 | 1.16 (0.32, 2.00) F | 0.0% | 0.000 | ||
| Elder | 3 | 1.80 (0.02, 3.58) R | 83.5% | 1.919 | ||
| PM10 | Female | 7 | 0.97 (0.61, 1.33) F | 28.3% | 0.113 | |
| Male | 7 | 1.48 (0.64, 2.32) R | 58.7% | 0.626 | ||
| Younger | 8 | 0.45 (0.16, 0.75) R | 56.2% | 0.127 | ||
| Elder | 8 | 0.75 (0.54, 0.97) R | 60.4% | 0.082 | ||
| SO2 | Female | 5 | 4.71 (1.59, 7.83) R | 83.8% | 9.104 | |
| Male | 5 | 4.39 (1.83, 6.96) R | 63.3% | 4.477 | ||
| Younger | 5 | 4.58 (1.76, 7.41) R | 58.4% | 5.135 | ||
| Elder | 5 | 4.87 (2.23, 7.50) R | 90.4% | 6.969 | ||
| NO2 | Female | 5 | 4.27 (1.93, 6.61) R | 67.1% | 4.342 | |
| Male | 5 | 3.98 (2.57, 5.39) F | 34.6% | 1.659 | ||
| Younger | 5 | 4.26 (2.59, 5.93) F | 0.0% | 0.000 | ||
| Elder | 5 | 4.33 (1.93, 6.74) R | 85.8% | 5.845 | ||
| CVD | PM2.5 | Female | 2 | 0.62 (0.16, 1.09) F | 0.0% | 0.000 |
| Male | 2 | 0.39 (−0.87, 1.65) R | 74.6% | 0.621 | ||
| Younger | 2 | 0.88 (−0.15, 1.91) F | 0.0% | 0.000 | ||
| Elder | 2 | 0.48 (0.10, 0.86) F | 0.0% | 0.000 | ||
| PM10 | Female | 3 | 0.84 (0.45, 1.23) F | 0.0% | 0.000 | |
| Male | 3 | 1.16 (−0.54, 2.87) R | 86.9% | 1.648 | ||
| Younger | 3 | 1.04 (−0.42, 2.50) R | 79.4% | 1.055 | ||
| Elder | 3 | 0.63 (0.29, 0.96) F | 44.1% | 0.092 | ||
| SO2 | Female | 2 | 2.39 (0.38, 4.39) R | 77.1% | 1.652 | |
| Male | 2 | 1.00 (0.08, 1.91) F | 0.0% | 0.000 | ||
| Younger | 2 | 1.32 (0.29, 2.34) F | 0.0% | 0.000 | ||
| Elder | 2 | 1.39 (0.82, 1.96) F | 0.0% | 0.000 | ||
| NO2 | Female | 2 | 1.95 (−0.32, 4.23) R | 86.1% | 2.337 | |
| Male | 2 | 0.75 (0.00, 1.49) F | 5.9% | 0.043 | ||
| Younger | 2 | 0.77 (0.38, 1.17) F | 0.0% | 0.000 | ||
| Elder | 2 | 1.82 (0.12, 3.51) R | 69.4% | 1.077 | ||
| RD | PM2.5 | Female | 1 | 0.25 (−0.06, 0.56) | — | 0.000 |
| Male | 1 | 0.07 (−0.33, 0.47) | — | 0.000 | ||
| Younger | 1 | −0.01 (−0.35, 0.34) | — | 0.000 | ||
| Elder | 1 | 0.33 (−0.04, 0.69) | — | 0.000 | ||
| PM10 | Female | 3 | 0.42 (−0.00, 0.84) R | 77.1% | 0.096 | |
| Male | 3 | 0.17 (−0.19, 0.53) R | 51.7% | 0.047 | ||
| Younger | 3 | 0.14 (−0.04, 0.31) F | 43.9% | 0.025 | ||
| Elder | 3 | 0.49 (−0.03, 1.01) R | 74.2% | 0.128 | ||
| SO2 | Female | 1 | 0.50 (−0.41, 1.41) | — | 0.000 | |
| Male | 1 | 0.37 (−0.82, 1.54) | — | 0.000 | ||
| Younger | 1 | −0.24 (−1.25, 0.77) | — | 0.000 | ||
| Elder | 1 | 1.11 (0.04, 2.18) | — | 0.000 | ||
| NO2 | Female | 1 | 0.91 (0.09, 1.73) | — | 0.000 | |
| Male | 1 | 0.02 (−1.04, 1.09) | — | 0.000 | ||
| Younger | 1 | −0.37 (−1.29, 0.54) | — | 0.000 | ||
| Elder | 1 | 1.30 (0.34, 2.27) | — | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ni, Y.; Song, W.; Bai, Y.; Liu, T.; Li, G.; Bian, Y.; Zeng, Q. Years of Life Lost (YLL) Due to Short-Term Exposure to Ambient Air Pollution in China: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11467. https://doi.org/10.3390/ijerph182111467
Ni Y, Song W, Bai Y, Liu T, Li G, Bian Y, Zeng Q. Years of Life Lost (YLL) Due to Short-Term Exposure to Ambient Air Pollution in China: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(21):11467. https://doi.org/10.3390/ijerph182111467
Chicago/Turabian StyleNi, Yang, Wang Song, Yu Bai, Tao Liu, Guoxing Li, Ying Bian, and Qiang Zeng. 2021. "Years of Life Lost (YLL) Due to Short-Term Exposure to Ambient Air Pollution in China: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 21: 11467. https://doi.org/10.3390/ijerph182111467
APA StyleNi, Y., Song, W., Bai, Y., Liu, T., Li, G., Bian, Y., & Zeng, Q. (2021). Years of Life Lost (YLL) Due to Short-Term Exposure to Ambient Air Pollution in China: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(21), 11467. https://doi.org/10.3390/ijerph182111467