
Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
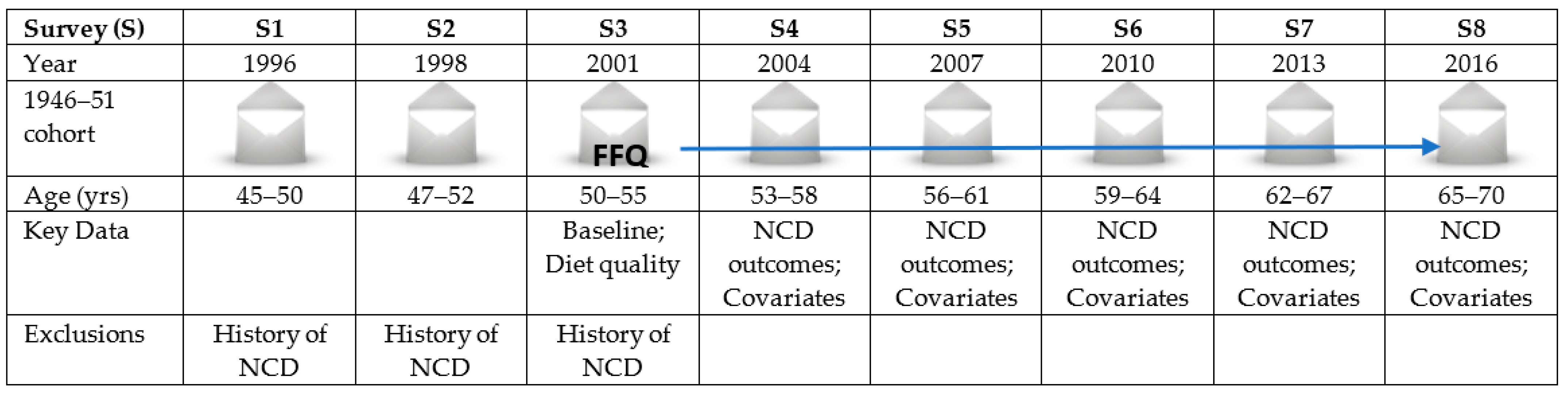
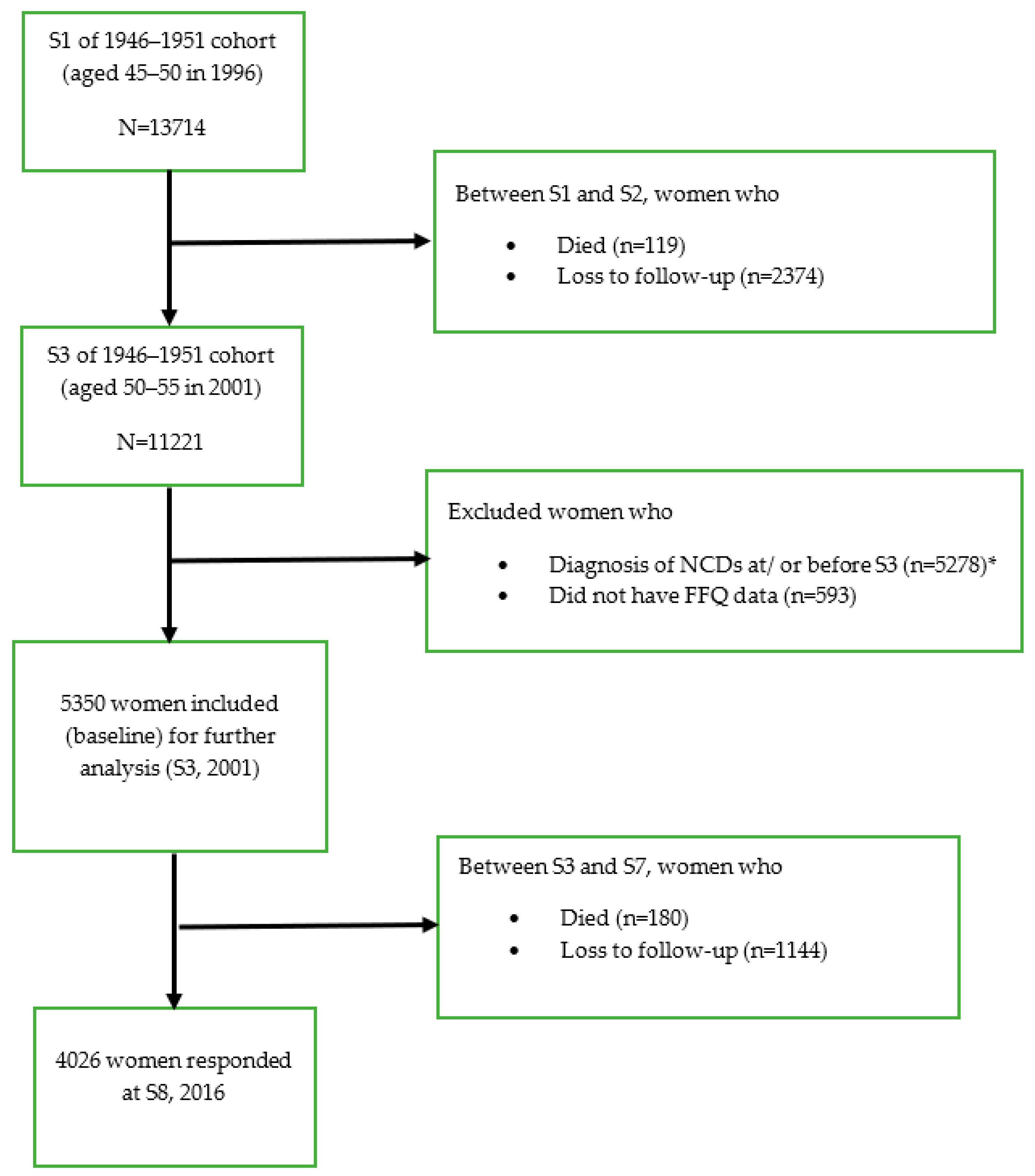
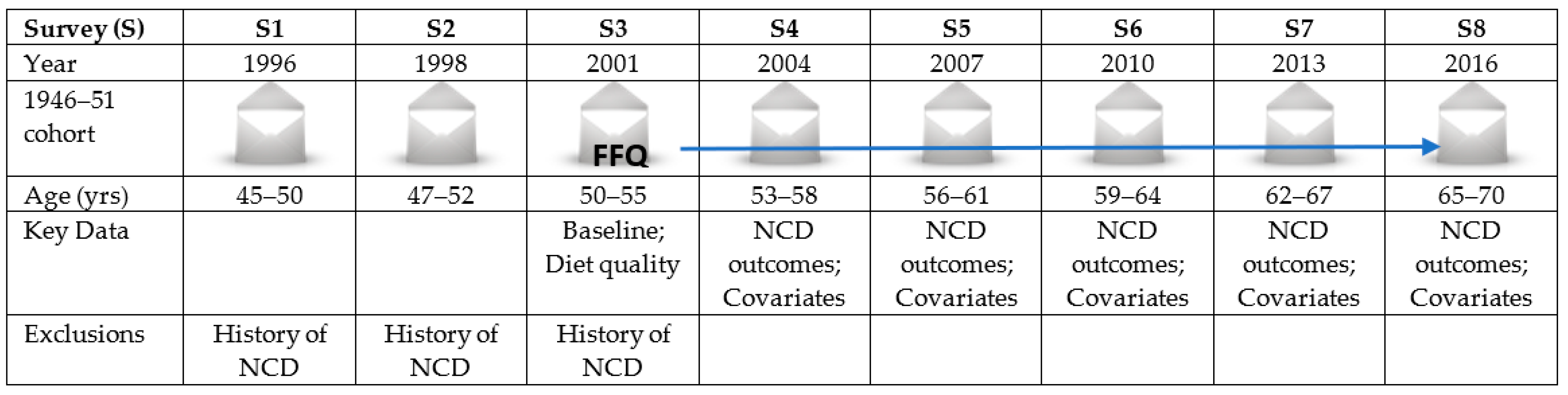
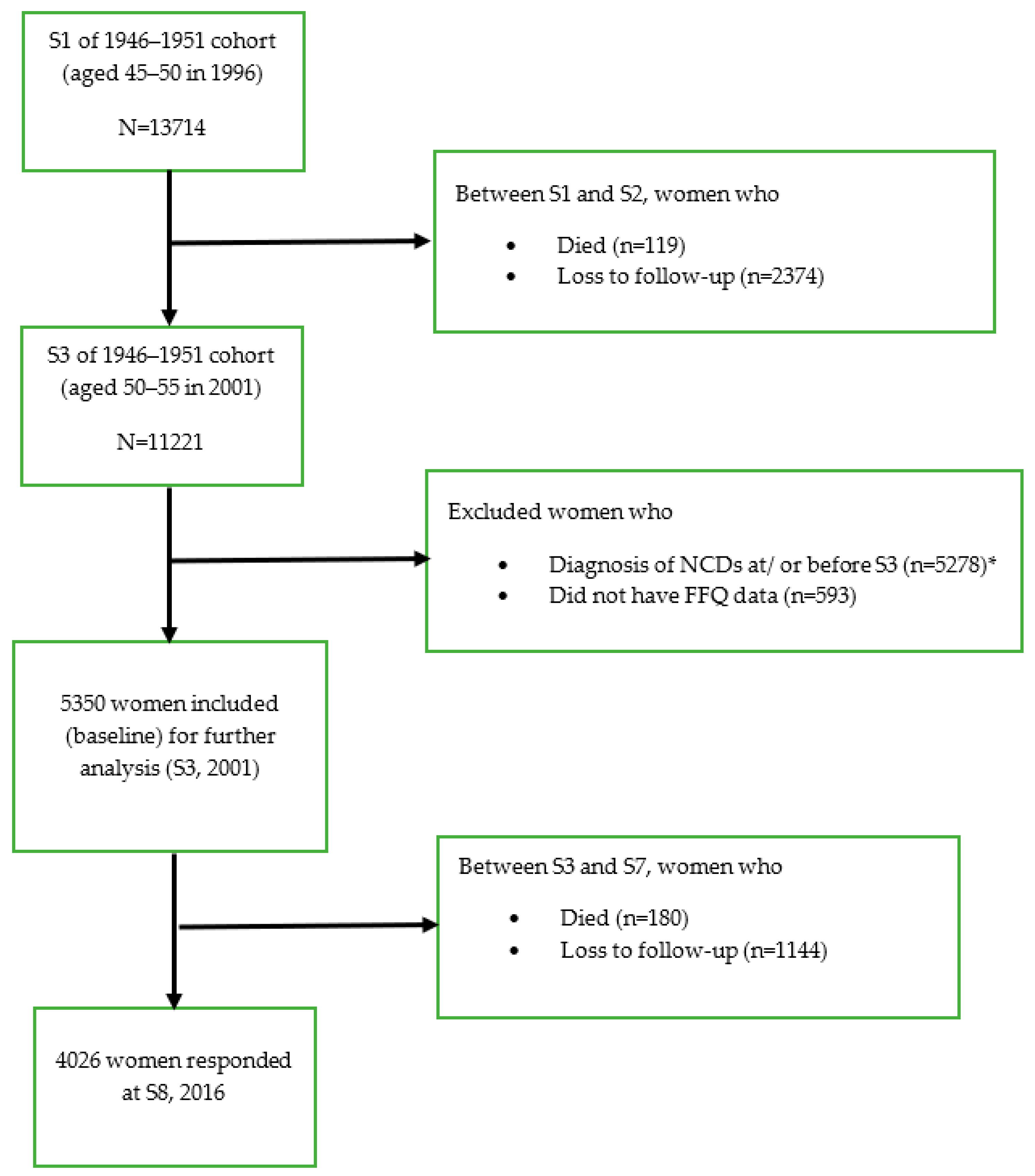
2.1. Study Population
2.2. Dietary Assessment
2.3. Exposure Variables
2.4. Outcome Variables
- The incidence of NCDs (DM, CHD, HT, asthma, cancer (excluding skin cancer), depression and/or anxiety; incident cases following S3, with cases accumulating over time);
- Multimorbidity (defined as the co-existence of two or more of the above NCDs);
- All-cause mortality (new deaths since the last survey).
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bennett, J.E.; A Stevens, G.; Mathers, C.D.; Bonita, R.; Rehm, J.; E Kruk, M.; Riley, L.M.; Dain, K.; Kengne, A.P.; Chalkidou, K.; et al. NCD Countdown 2030: Worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet 2018, 392, 1072–1088. [Google Scholar] [CrossRef] [Green Version]
- Violán, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, Determinants and Patterns of Multimorbidity in Primary Care: A Systematic Review of Observational Studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef]
- Smith, S.M.; Soubhi, H.; Fortin, M.; Hudon, C.; O’Dowd, T. Managing patients with multimorbidity: Systematic review of interventions in primary care and community settings. BMJ 2012, 345, e5205. [Google Scholar] [CrossRef] [Green Version]
- Barnett, K.; Mercer, S.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.W.; Price, K.; Gill, T.K.; Adams, R.; Pilkington, R.; Carrangis, N.; Shi, Z.; Wilson, D. Multimorbidity—Not just an older person’s issue. Results from an Australian biomedical study. BMC Public Health 2010, 10, 718. [Google Scholar] [CrossRef] [Green Version]
- Harrison, C.; Henderson, J.; Miller, G.; Britt, H. The prevalence of diagnosed chronic conditions and multimorbidity in Australia: A method for estimating population prevalence from general practice patient encounter data. PLoS ONE 2017, 12, e0172935. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund/American Institute for Cancer Research: Washington, DC, USA, 2017. [Google Scholar]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A systematic review of diet quality indices in relation to obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hruby, A.; Manson, J.E.; Qi, L.; Malik, V.S.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Hu, F.B. Determinants and Consequences of Obesity. Am. J. Public Health 2016, 106, 1656–1662. [Google Scholar] [CrossRef]
- Al-Ibrahim, A.A.; Jackson, R.T. Healthy eating index versus alternate healthy index in relation to diabetes status and health markers in U.S. adults: NHANES 2007–2010. Nutr. J. 2019, 18, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Does diet cost mediate the relation between socioeconomic position and diet quality? Eur. J. Clin. Nutr. 2011, 65, 1059–1066. [Google Scholar] [CrossRef] [Green Version]
- Dhakal, C.; Khadka, S. Heterogeneities in Consumer Diet Quality and Health Outcomes of Consumers by Store Choice and Income. Nutrients 2021, 13, 1046. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newby, P.K.; Tucker, K. Empirically Derived Eating Patterns Using Factor or Cluster Analysis: A Review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Panagiotakos, D.B. Dietary quality indices and human health: A review. Maturitas 2009, 62, 1–8. [Google Scholar] [CrossRef]
- Thorpe, M.G.; Kestin, M.; Riddell, L.J.; Keast, R.S.; A McNaughton, S. Diet quality in young adults and its association with food-related behaviours. Public Health Nutr. 2013, 17, 1767–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef]
- Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The Diet Quality Index Revised: A Measurement Instrument for Populations. J. Am. Diet. Assoc. 1999, 99, 697–704. [Google Scholar] [CrossRef]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K.; Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K.; Kennedy, E.T.; Ohls, J.; et al. The Healthy Eating Index: Design and Applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [Green Version]
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An Index of Diet and Eating Patterns Is a Valid Measure of Diet Quality in an Australian Population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Siega-Riz, A.; Gordon-Larsen, P.; Cai, J.; Adair, L.; Zhang, B.; Popkin, B. Diet quality and its association with type 2 diabetes and major cardiometabolic risk factors among adults in China. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 987–1001. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Song, X.; Chen, G.-C.; Neelakantan, N.; Van Dam, R.M.; Feng, L.; Yuan, J.-M.; Pan, A.; Koh, W.-P. Dietary pattern in midlife and cognitive impairment in late life: A prospective study in Chinese adults. Am. J. Clin. Nutr. 2019, 110, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative Dietary Indices Both Strongly Predict Risk of Chronic Disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100.e11. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, the Alternate Healthy Eating Index, the Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2015, 115, 780–800.e5. [Google Scholar] [CrossRef]
- Waijers, P.M.C.M.; Feskens, E.; Ocké, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Morze, J.; Danielewicz, A.; Hoffmann, G.; Schwingshackl, L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2020, 120, 1998–2031.e15. [Google Scholar] [CrossRef]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health: A critical review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Cowell, O.R.; Mistry, N.; Deighton, K.; Matu, J.; Griffiths, A.; Minihane, A.M.; Mathers, J.C.; Shannon, O.M.; Siervo, M. Effects of a Mediterranean diet on blood pressure: A systematic review and meta-analysis of randomized controlled trials and observational studies. J. Hypertens. 2021, 39, 729–739. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [Green Version]
- Shafiei, F.; Moghaddam, A.S.; Larijani, B.; Esmaillzadeh, A. Adherence to the Mediterranean diet and risk of depression: A systematic review and updated meta-analysis of observational studies. Nutr. Rev. 2019, 77, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Altun, A.; Brown, H.; Szoeke, C.; Goodwill, A.M. The Mediterranean dietary pattern and depression risk: A systematic review. Neurol. Psychiatry Brain Res. 2019, 33, 1–10. [Google Scholar] [CrossRef]
- Soltani, S.; Jayedi, A.; Shab-Bidar, S.; Becerra-Tomás, N.; Salas-Salvadó, J. Adherence to the Mediterranean Diet in Relation to All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2019, 10, 1029–1039. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Fayosse, A.; Sabia, S.; Tabak, A.; Shipley, M.; Dugravot, A.; Kivimäki, M. Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study. PLoS Med. 2018, 15, e1002571. [Google Scholar] [CrossRef] [PubMed]
- Freisling, H.; Viallon, V.; Lennon, H.; Bagnardi, V.; Ricci, C.; Butterworth, A.S.; Sweeting, M.; Muller, D.; Romieu, I.; Bazelle, P.; et al. Lifestyle factors and risk of multimorbidity of cancer and cardiometabolic diseases: A multinational cohort study. BMC Med. 2020, 18, 1–11. [Google Scholar] [CrossRef]
- Dobson, A.J.; Hockey, R.; Brown, W.J.; Byles, J.E.; Loxton, D.J.; McLaughlin, D.P.; Tooth, L.R.; Mishr, G.D. Cohort profile update: Australian Longitudinal Study on Women’s Health. Int. J. Epidemiol. 2015, 44, 1547. [Google Scholar] [CrossRef] [Green Version]
- Loxton, D.; Tooth, L.; Harris, M.L.; Forder, P.M.; Dobson, A.; Powers, J.; Brown, W.; Byles, J.; Mishra, G. Cohort Profile: The Australian Longitudinal Study on Women’s Health (ALSWH) 1989–95 cohort. Int. J. Epidemiology 2018, 47, 391–392e. [Google Scholar] [CrossRef] [PubMed]
- Women’s Health Australia. Available online: http://www.alswh.org.au (accessed on 2 January 2021).
- Ireland, P.; Jolley, D.; Giles, G.; O’Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the Mel-bourne FFQ: A food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pac. J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar]
- Lewis, J.; Milligan, G.C.; Hunt, A. Nuttab95: Nutrient Data Table for Use in Australia; Food Standards Australia New Zealand: Canberra, Australia, 1995. [Google Scholar]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. New Zealand J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef]
- Baldwin, J.N.; Forder, P.M.; Haslam, R.L.; Hure, A.J.; Loxton, D.J.; Patterson, A.J.; Collins, C.E. Change in Diet Quality over 12 Years in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. Nutrients 2020, 12, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hlaing-Hlaing, H.; Pezdirc, K.; Tavener, M.; James, E.L.; Hure, A. Diet Quality Indices Used in Australian and New Zealand Adults: A Systematic Review and Critical Appraisal. Nutrients 2020, 12, 3777. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council (Australia). Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Roy, R.; Hebden, L.; Rangan, A.; Allman-Farinelli, M. The development, application, and validation of a Healthy eating index for Australian Adults (HEIFA—2013). Nutrition 2016, 32, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Grech, A.; Sui, Z.; Siu, H.Y.; Zheng, M.; Allman-Farinelli, M.; Rangan, A. Socio-Demographic Determinants of Diet Quality in Australian Adults Using the Validated Healthy Eating Index for Australian Adults (HEIFA-2013). Healthcare 2017, 5, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food Standards Australia New Zealand. Determining the Amount of Added Sugars and Free Sugars in Foods Listed in the AUSNUT 2011-13 Dataset. Available online: https://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/foodnutrient/Pages/Determining-the-amount-of-added-sugars-and-free-sugars-in-foods-listed-in-the-AUSNUT-201113-dataset.aspx (accessed on 14 March 2021).
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-De-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; Van Der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristina, T.J.N.; Williams, J.S.; Parkinson, L.; Sibbritt, D.W.; Byles, J.E. Identification of diabetes, heart disease, hypertension and stroke in mid- and older-aged women: Comparing self-report and administrative hospital data records. Geriatr. Gerontol. Int. 2016, 16, 95–102. [Google Scholar] [CrossRef] [PubMed]
- The University of Queensland. Report 29; Women’s Health Australia; The University of Queensland: Brisbane, Australia, 2007. [Google Scholar]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal Diagrams for Epidemiologic Research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef]
- Textor, J.; Hardt, J.; Knüppel, S. DAGitty: A graphical tool for analyzing causal diagrams. Epidemiology 2011, 22, 745. [Google Scholar] [CrossRef] [Green Version]
- Brown, W.J.; Burton, N.; Marshall, A.; Miller, Y.D. Reliability and validity of a modified self-administered version of the Active Australia physical activity survey in a sample of mid-age women. Aust. N. Z. J. Public Health 2008, 32, 535–541. [Google Scholar] [CrossRef]
- Women’s Health Australia: Data Documentation. Available online: http://www.alswh.org.au/for-researchers/data (accessed on 10 March 2021).
- Lalonde, T.L.; Wilson, J.R.; Yin, J. GMM logistic regression models for longitudinal data with time-dependent covariates and extended classifications. Stat. Med. 2014, 33, 4756–4769. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Harmon, B.E.; Boushey, C.J.; Morimoto, Y.; Wilkens, L.R.; Le Marchand, L.; Kröger, J.; Schulze, M.B.; Kolonel, L.N.; Maskarinec, G. A priori-defined diet quality indexes and risk of type 2 diabetes: The Multiethnic Cohort. Diabetologia 2015, 58, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Cespedes, E.M.; Hu, F.B.; Tinker, L.; Rosner, B.; Redline, S.; Garcia, L.; Hingle, M.; Van Horn, L.; Howard, B.V.; Levitan, E.; et al. Multiple Healthful Dietary Patterns and Type 2 Diabetes in the Women’s Health Initiative. Am. J. Epidemiol. 2016, 183, 622–633. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Hu, F.B. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients 2019, 11, 1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papier, K.; Fensom, G.K.; Knuppel, A.; Appleby, P.N.; Tong, T.; Schmidt, J.A.; Travis, R.C.; Key, T.J.; Perez-Cornago, A. Meat consumption and risk of 25 common conditions: Outcome-wide analyses in 475,000 men and women in the UK Biobank study. BMC Med. 2021, 19, 53. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Imamura, F.; Ma, W.; Wang, M.; Lemaitre, R.N.; King, I.B.; Song, X.; Biggs, M.L.; A Delaney, J.; Mukamal, K.J.; et al. Circulating and Dietary Trans Fatty Acids and Incident Type 2 Diabetes in Older Adults: The Cardiovascular Health Study. Diabetes Care 2015, 38, 1099–1107. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.J.; Brainard, J.; Song, F.; Wang, X.; Abdelhamid, A.; Hooper, L. Omega-3, omega-6, and total dietary polyunsaturated fat for prevention and treatment of type 2 diabetes mellitus: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 366, l4697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, E.A.; Steffen, L.M.; Coresh, J.; Appel, L.J.; Rebholz, C.M. Adherence to the Healthy Eating Index–2015 and Other Dietary Patterns May Reduce Risk of Cardiovascular Disease, Cardiovascular Mortality, and All-Cause Mortality. J. Nutr. 2020, 150, 312–321. [Google Scholar] [CrossRef]
- Xu, Z.; Steffen, L.M.; Selvin, E.; Rebholz, C.M. Diet quality, change in diet quality and risk of incident CVD and diabetes. Public Health Nutr. 2020, 23, 329–338. [Google Scholar] [CrossRef]
- Dilis, V.; Katsoulis, M.; Lagiou, P.; Trichopoulos, D.; Naska, A.; Trichopoulou, A. Mediterranean diet and CHD: The Greek European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Nutr. 2012, 108, 699–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Rexrode, K.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean Diet and Incidence of and Mortality from Coronary Heart Disease and Stroke in Women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, L.; Waller, M.; van der Schouw, Y.; Hébert, J.; Shivappa, N.; Schoenaker, D.; Mishra, G. A pro-inflammatory diet is associated with increased risk of developing hypertension among middle-aged women. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 564–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, J.K.; MacDonald-Wicks, L.K.; A McEvoy, M.; Forder, P.M.; Holder, C.; Oldmeadow, C.; E Byles, J.; Patterson, A.J. Better diet quality scores are associated with a lower risk of hypertension and non-fatal CVD in middle-aged Australian women over 15 years of follow-up. Public Health Nutr. 2020, 23, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, J.; Gaskin, E.; Ji, C.; Miller, M.A.; Cappuccio, F.P. The effect of plant-based dietary patterns on blood pressure: A systematic review and meta-analysis of controlled intervention trials. J. Hypertens. 2021, 39, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Godos, J.; Marventano, S.; Tieri, M.; Ghelfi, F.; Titta, L.; Lafranconi, A.; Trigueiro, H.; Gambera, A.; Alonzo, E.; et al. Nut and legume consumption and human health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2021, 72, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Xiong, K.; Cai, J.; Ma, A. Fish Consumption and Coronary Heart Disease: A Meta-Analysis. Nutrients 2020, 12, 2278. [Google Scholar] [CrossRef] [PubMed]
- Alwarith, J.; Kahleova, H.; Crosby, L.; Brooks, A.; Brandon, L.; Levin, S.M.; Barnard, N.D. The role of nutrition in asthma prevention and treatment. Nutr. Rev. 2020, 78, 928–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varraso, R.; E Chiuve, S.; Fung, T.T.; Barr, R.G.; Hu, F.B.; Willett, W.C.; A Camargo, C. Alternate Healthy Eating Index 2010 and risk of chronic obstructive pulmonary disease among US women and men: Prospective study. BMJ 2015, 350, h286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.-Y.; Jerschow, E.; Forno, E.; Hua, S.; Mossavar-Rahmani, Y.; Perreira, K.M.; Sotres-Alvarez, D.; Afshar, M.; Punjabi, N.M.; Thyagarajan, B.; et al. Dietary Patterns, Asthma, and Lung Function in the Hispanic Community Health Study/Study of Latinos. Ann. Am. Thorac. Soc. 2020, 17, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Andrianasolo, R.M.; Kesse-Guyot, E.; Adjibade, M.; Hercberg, S.; Galan, P.; Varraso, R. Associations between dietary scores with asthma symptoms and asthma control in adults. Eur. Respir. J. 2018, 52, 1702572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zurbau, A.; Au-Yeung, F.; Mejia, S.B.; Khan, T.A.; Vuksan, V.; Jovanovski, E.; Leiter, L.A.; Kendall, C.W.C.; Jenkins, D.J.A.; Sievenpiper, J.L. Relation of Different Fruit and Vegetable Sources with Incident Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Am. Hear. Assoc. 2020, 9, e017728. [Google Scholar] [CrossRef]
- Wang, P.; Fang, J.; Gao, Z.; Zhang, C.; Xie, S. Higher intake of fruits, vegetables or their fiber reduces the risk of type 2 diabetes: A meta-analysis. J. Diabetes Investig. 2016, 7, 56–69. [Google Scholar] [CrossRef] [PubMed]
- Seyedrezazadeh, E.; Pour Moghaddam, M.; Ansarin, K.; Vafa, M.; Sharma, S.; Kolahdooz, F. Fruit and vegetable intake and risk of wheezing and asthma: A systematic review and meta-analysis. Nutr. Rev. 2014, 72, 411–428. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Rossi, M.; Pelucchi, C.; Levi, F.; La Vecchia, C. Fruit and vegetables and cancer risk: A review of southern European studies. Br. J. Nutr. 2015, 113, S102–S110. [Google Scholar] [CrossRef]
- Saghafian, F.; Malmir, H.; Saneei, P.; Milajerdi, A.; Larijani, B.; Esmaillzadeh, A. Fruit and vegetable consumption and risk of depression: Accumulative evidence from an updated systematic review and meta-analysis of epidemiological studies. Br. J. Nutr. 2018, 119, 1087–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Wan, Y.; Zhao, M.; Zhong, H.; Zheng, J.-S.; Feng, F. Legume and soy intake and risk of type 2 diabetes: A systematic review and meta-analysis of prospective cohort studies. Am. J. Clin. Nutr. 2020, 111, 677–688. [Google Scholar] [CrossRef]
- Marventano, S.; Pulido, M.I.; Sánchez-González, C.; Godos, J.; Speciani, A.; Galvano, F.; Grosso, G. Legume consumption and CVD risk: A systematic review and meta-analysis. Public Health Nutr. 2017, 20, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viguiliouk, E.; Glenn, A.J.; Nishi, S.K.; Chiavaroli, L.; Seider, M.; Khan, T.; Bonaccio, M.; Iacoviello, L.; Mejia, S.B.; A Jenkins, D.J.; et al. Associations between Dietary Pulses Alone or with Other Legumes and Cardiometabolic Disease Outcomes: An Umbrella Review and Updated Systematic Review and Meta-analysis of Prospective Cohort Studies. Adv. Nutr. 2019, 10, S308–S319. [Google Scholar] [CrossRef] [PubMed]
- Lavalette, C.; Adjibade, M.; Srour, B.; Sellem, L.; Fiolet, T.; Hercberg, S.; Latino-Martel, P.; Fassier, P.; Deschasaux, M.; Kesse-Guyot, E.; et al. Cancer-Specific and General Nutritional Scores and Cancer Risk: Results from the Prospective NutriNet-Santé Cohort. Cancer Res. 2018, 78, 4427–4435. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Henríquez-Sánchez, P.; Ruiz-Canela, M.; Lahortiga, F.; Molero, P.; Toledo, E.; Martínez-González, M.A. A longitudinal analysis of diet quality scores and the risk of incident depression in the SUN Project. BMC Med. 2015, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rienks, J.; Dobson, A.J.; Mishra, G.D. Mediterranean dietary pattern and prevalence and incidence of depressive symptoms in mid-aged women: Results from a large community-based prospective study. Eur. J. Clin. Nutr. 2013, 67, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Villegas, A.; Delgado-Rodríguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Majem, L.S.; Martínez-González, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Almeida, O.P.; English, D.R.; Giles, G.G.; Flicker, L. Patterns of dietary intake and psychological distress in older Australians: Benefits not just from a Mediterranean diet. Int. Psychogeriatrics 2013, 25, 456–466. [Google Scholar] [CrossRef]
- Shi, Z.; Ruel, G.; Grande, E.D.; Pilkington, R.; Taylor, A. Soft drink consumption and multimorbidity among adults. Clin. Nutr. ESPEN 2015, 10, e71–e76. [Google Scholar] [CrossRef]
- Jeong, D.; Kim, J.; Lee, H.; Kim, D.-Y.; Lim, H. Association of Cardiometabolic Multimorbidity Pattern with Dietary Factors among Adults in South Korea. Nutrients 2020, 12, 2730. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.P.; Bortolotto, C.C.; Tomasi, E.; Gonzalez, M.C.; Gomes, A.P.; Gonçalves, H.; Bielemann, R.M. Food consumption and multimorbidity among non-institutionalized elderly people in Pelotas, 2014: A cross-sectional study. Epidemiol. Serviços Saúde 2020, 29, e2019050. [Google Scholar] [CrossRef]
- Ruel, G.; Shi, Z.; Zhen, S.; Zuo, H.; Kröger, E.; Sirois, C.; Lévesque, J.-F.; Taylor, A. Association between nutrition and the evolution of multimorbidity: The importance of fruits and vegetables and whole grain products. Clin. Nutr. 2014, 33, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Wikström, K.; Lindström, J.; Harald, K.; Peltonen, M.; Laatikainen, T. Clinical and lifestyle-related risk factors for incident multimorbidity: 10-year follow-up of Finnish population-based cohorts 1982–2012. Eur. J. Intern. Med. 2015, 26, 211–216. [Google Scholar] [CrossRef]
- Dekker, L.H.; De Borst, M.; Meems, L.M.G.; De Boer, R.A.; Bakker, S.J.L.; Navis, G.J. The association of multimorbidity within cardio-metabolic disease domains with dietary patterns: A cross-sectional study in 129 369 men and women from the Lifelines cohort. PLoS ONE 2019, 14, e0220368. [Google Scholar] [CrossRef] [Green Version]
- Kyprianidou, M.; Panagiotakos, D.; Faka, A.; Kambanaros, M.; Makris, K.C.; A Christophi, C. Adherence to the Mediterranean diet in Cyprus and its relationship to multi-morbidity: An epidemiological study. Public Health Nutr. 2021, 24, 4546–4555. [Google Scholar] [CrossRef]
- Harmon, B.E.; Boushey, C.J.; Shvetsov, Y.B.; Ettienne, R.; Reedy, J.; Wilkens, L.R.; Le Marchand, L.; E Henderson, B.; Kolonel, L.N. Associations of key diet-quality indexes with mortality in the Multiethnic Cohort: The Dietary Patterns Methods Project. Am. J. Clin. Nutr. 2015, 101, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Brandt, P.A.V.D. The impact of a Mediterranean diet and healthy lifestyle on premature mortality in men and women. Am. J. Clin. Nutr. 2011, 94, 913–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassale, C.; Gunter, M.J.; Romaguera, D.; Peelen, L.M.; Van Der Schouw, Y.T.; Beulens, J.W.J.; Freisling, H.; Muller, D.C.; Ferrari, P.; Huybrechts, I.; et al. Diet Quality Scores and Prediction of All-Cause, Cardiovascular and Cancer Mortality in a Pan-European Cohort Study. PLoS ONE 2016, 11, e0159025. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Bassett, J.; Dugué, P.-A.; Shivappa, N.; Hébert, J.; Milne, R.; English, D.; Giles, G. Dietary inflammatory index or Mediterranean diet score as risk factors for total and cardiovascular mortality. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 461–469. [Google Scholar] [CrossRef]
- Cuenca-García, M.; Artero, E.G.; Sui, X.; Lee, D.-C.; Hebert, J.R.; Blair, S.N. Dietary indices, cardiovascular risk factors and mortality in middle-aged adults: Findings from the Aerobics Center Longitudinal Study. Ann. Epidemiol. 2014, 24, 297–303.e292. [Google Scholar] [CrossRef]
- Vormund, K.; Braun, J.; Rohrmann, S.; Bopp, M.; Ballmer, P.; Faeh, D. Mediterranean diet and mortality in Switzerland: An alpine paradox? Eur. J. Nutr. 2015, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Ponzo, V.; Goitre, I.; Fadda, M.; Pezzana, A.; Beccuti, G.; Gambino, R.; Cassader, M.; Soldati, L.; Broglio, F. Predictive role of the Mediterranean diet on mortality in individuals at low cardiovascular risk: A 12-year follow-up population-based cohort study. J. Transl. Med. 2016, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.; Hershey, M.S.; Zazpe, I.; Trichopoulou, A. Transferability of the Mediterranean Diet to Non-Mediterranean Countries. What Is and What Is Not the Mediterranean Diet. Nutrients 2017, 9, 1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stavrou, E.; Vajdic, C.M.; Loxton, D.; Pearson, S.-A. The validity of self-reported cancer diagnoses and factors associated with accurate reporting in a cohort of older Australian women. Cancer Epidemiol. 2011, 35, e75–e80. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| HEIFA-2013 | MDS | AHEI-2010 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics * | Q1 (n = 1056) | Q5 (n = 1059) | p-Value | Q1 (n = 1769) | Q5 (n = 642) | p-Value | Q1 (n = 1059) | Q5 (n = 1139) | p-Value |
| Mean age in years (sd) | 52.38 (1.43) | 52.58 (1.45) | 0.004 ** | 52.42 (1.45) | 52.58 (1.44) | 0.15 | 52.34 (1.45) | 52.53 (1.43) | 0.004 ** |
| Marital status | 0.072 | 0.47 | 0.13 | ||||||
| Never married | 30 (2.8) | 33 (3.1) | 49 (2.8) | 25 (3.9) | 29 (2.7) | 44 (3.9) | |||
| Married/de facto | 865 (82.0) | 866 (81.9) | 1451 (82.2) | 536 (83.8) | 897 (84.7) | 918 (80.9) | |||
| Separated/divorced/widowed | 160 (15.2) | 159 (15.0) | 266 (15.0) | 79 (12.3) | 133 (12.6) | 173 (15.2) | |||
| Area of residence | 0.070 | 0.063 | 0.003 ** | ||||||
| Urban | 389 (37.0) | 334 (31.7) | 576 (32.7) | 235 (36.6) | 334 (31.7) | 446 (39.3) | |||
| Inner regional | 440 (41.9) | 438 (41.5) | 739 (42.0) | 257 (40.0) | 451 (42.7) | 438 (38.6) | |||
| Outer regional/rural | 222 (21.1) | 283 (26.8) | 446 (25.3) | 150 (23.4) | 270 (25.6) | 252 (22.1) | |||
| Education | <0.001** | <0.001 ** | <0.001 ** | ||||||
| No formal education | 168 (15.9) | 120 (11.3) | 267 (15.1) | 61 (9.5) | 181 (17.1) | 106 (9.2) | |||
| High school certificate | 489 (46.4) | 454 (42.9) | 899 (50.9) | 235 (36.6) | 525 (49.7) | 441 (38.8) | |||
| Apprenticeship/diploma) | 201 (19.1) | 251 (23.7) | 342 (19.4) | 155 (24.1) | 217 (20.5) | 275 (24.2) | |||
| University/higher degree | 196 (18.6) | 233 (22.1) | 257 (14.6) | 191 (29.8) | 134 (12.7) | 316 (27.8) | |||
| Occupation | 0.032 ** | 0.14 | <0.001 ** | ||||||
| No paid job | 263 (26.1) | 207 (20.4) | 407 (24.1) | 129 (20.7) | 275 (27.1) | 203 (18.5) | |||
| Paid job | 744 (73.9) | 808 (79.6) | 1283 (75.9) | 495 (79.3) | 739 (72.9) | 892 (81.5) | |||
| Ability to manage income | <0.001 ** | <0.001 ** | <0.001 ** | ||||||
| Easy/not bad | 644 (61.3) | 744 (70.5) | 1082 (61.7) | 447 (70.0) | 622 (59.4) | 806 (71.1) | |||
| Sometimes/always difficult | 406 (38.7) | 311 (29.5) | 672 (38.3) | 192 (30.0) | 425 (40.6) | 327 (28.9) | |||
| Physical activity | <0.001 ** | <0.001 ** | <0.001 ** | ||||||
| Nil/sedentary | 205 (20.1) | 101 (9.8) | 344 (20.2) | 48 (7.6) | 228 (22.4) | 85 (7.7) | |||
| Low | 362 (35.6) | 297 (28.8) | 576 (33.9) | 165 (26.3) | 367 (36.1) | 318 (28.8) | |||
| Moderate | 191 (18.8) | 255 (24.7) | 345 (20.3) | 152 (24.2) | 187 (18.4) | 284 (25.7) | |||
| High | 260 (25.5) | 379 (36.7) | 436 (25.6) | 263 (41.9) | 236 (23.2) | 419 (37.8) | |||
| Smoking status | <0.001 ** | <0.001 ** | <0.001 ** | ||||||
| Never smoked | 561 (53.2) | 720 (68.4) | 1046 (59.2) | 405 (63.5) | 618 (58.4) | 722 (63.8) | |||
| History of smoking | 256 (24.2) | 246 (23.4) | 362 (20.5) | 177 (27.7) | 209 (19.8) | 324 (28.6) | |||
| Currently smoke | 239 (22.6) | 87 (8.2) | 360 (20.3) | 56 (8.8) | 231 (21.8) | 86 (7.6) | |||
| Taking prescribed medicine | 0.92 | 0.56 | 0.005 ** | ||||||
| Not taken | 582 (55.5) | 597 (56.5) | 955 (54.3) | 357 (55.9) | 586 (55.8) | 663 (58.6) | |||
| Taken | 467 (44.5) | 459 (43.5) | 803 (45.7) | 282 (44.1) | 465 (44.2) | 469 (41.4) | |||
| Taking over the counter medicine | 0.12 | <0.001 ** | <0.001 ** | ||||||
| Not taken | 288 (27.4) | 240 (22.7) | 505 (28.6) | 133 (20.8) | 326 (30.9) | 248 (21.9) | |||
| Taken | 763 (72.6) | 815 (77.3) | 1258 (71.4) | 506 (79.2) | 728 (69.1) | 887 (78.1) | |||
| Diet Quality Index | S4 (n = 4347) b | S5 (n = 4168) b | S6 (n = 4015) b | S7 (n = 3948) b | S8 (n = 3905) b |
|---|---|---|---|---|---|
| Number of missing values | 519 | 598 | 532 | 306 | 121 |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| DM | n = 42 | n = 119 | n = 206 | n = 281 | n = 375 |
| HEIFA-2013: Univariate | 0.54 (0.18–1.63) | 0.77 (0.42–1.39) | 0.93 (0.59–1.46) | 0.86 (0.58–1.27) | 0.70 (0.49–1.00) |
| : Multivariate | 0.71 (0.20–2.51) | 1.03 (0.52–2.05) | 1.06 (0.63–1.77) | 0.95 (0.62–1.43) | 0.76 (0.52–1.10) |
| MDS: Univariate | 1.33 (0.40–4.44) | 0.62 (0.28–1.34) | 0.96 (0.57–1.62) | 0.74 (0.46–1.21) | 0.60 (0.39–0.94) * |
| : Multivariate | 1.70 (0.42–6.88) | 0.94 (0.42–2.11) | 1.30 (0.73–2.31) | 0.95 (0.57–1.60) | 0.76 (0.48–1.21) |
| AHEI-2010: Univariate | 0.71 (0.26–1.92) | 0.34 (0.18–0.66) * | 0.44 (0.27–0.73) * | 0.43 (0.28–0.67) * | 0.35 (0.23–0.51) * |
| : Multivariate | 1.00 (0.30–3.29) | 0.50 (0.25–0.99) * | 0.58 (0.33–0.99) * | 0.51 (0.31–0.84) * | 0.44 (0.29–0.66) * |
| CHD | n = 58 | n = 136 | n = 214 | n = 320 | n = 409 |
| HEIFA-2013: Univariate | 1.21 (0.58–2.53) | 1.12 (0.65–1.93) | 0.63 (0.40–0.97) * | 0.92 (0.63–1.33) | 0.92 (0.65–1.29) |
| : Multivariate | 1.34 (0.60–3.00) | 1.11 (0.62–1.98) | 0.72 (0.44–1.18) | 1.21 (0.81–1.82) | 1.01 (0.70–1.46) |
| MDS: Univariate | 0.94 (0.37–2.39) | 0.48 (0.24–0.99) * | 0.53 (0.31–0.91) * | 0.77 (0.50–1.18) | 0.79 (0.54–1.15) |
| : Multivariate | 0.88 (0.28–2.73) | 0.58 (0.28–1.20) | 0.68 (0.38–1.22) | 0.99 (0.63–1.56) | 0.94 (0.64–1.39) |
| AHEI-2010: Univariate | 1.12 (0.46–2.72) | 0.67 (0.38–1.18) | 0.50 (0.32–0.81) * | 0.58 (0.40–0.84) * | 0.65 (0.46–0.91) * |
| : Multivariate | 1.24 (0.48–3.25) | 0.72 (0.39–1.33) | 0.63 (0.38–1.06) | 0.74 (0.50–1.11) | 0.78 (0.54–1.12) |
| HT | n = 244 | n = 604 | n = 924 | n = 1194 | n = 1419 |
| HEIFA-2013: Univariate | 0.83 (0.55–1.24) | 0.69 (0.53–0.90) * | 0.76 (0.60–0.96) * | 0.75 (0.60–0.93) * | 0.71 (0.57–0.88) * |
| : Multivariate | 0.93 (0.59–1.44) | 0.77 (0.57–1.04) | 0.83 (0.64–1.09) | 0.74 (0.58–0.94) * | 0.65 (0.51–0.82) * |
| MDS: Univariate | 1.01 (0.66–1.56) | 0.86 (0.64–1.17) | 0.65 (0.50–0.85) * | 0.68 (0.53–0.87) * | 0.73 (0.58–0.91) * |
| : Multivariate | 1.23 (0.77–1.97) | 1.19 (0.85–1.66) | 0.73 (0.55–0.98) * | 0.75 (0.57–0.98) * | 0.76 (0.59–0.97) * |
| AHEI-2010: Univariate | 0.54 (0.36–0.81) * | 0.64 (0.49–0.85) * | 0.65 (0.51–0.82) * | 0.69 (0.56–0.86) * | 0.66 (0.54–0.82) * |
| : Multivariate | 0.67 (0.43–1.04) | 0.77 (0.57–1.05) | 0.82 (0.63–1.07) | 0.79 (0.62–1.01) | 0.74 (0.59–0.94) * |
| Asthma | n = 76 | n = 159 | n = 243 | n = 314 | n = 374 |
| HEIFA-2013: Univariate | 0.73 (0.37–1.44) | 0.99 (0.62–1.59) | 1.18 (0.78–1.78) | 0.97 (0.67–1.40) | 0.98 (0.69–1.39) |
| : Multivariate | 1.03 (0.49–2.17) | 1.05 (0.63–1.77) | 1.09 (0.69–1.71) | 1.14 (0.77–1.71) | 1.09 (0.75–1.57) |
| MDS: Univariate | 0.63 (0.26–1.56) | 1.20 (0.68–2.11) | 0.92 (0.57–1.47) | 0.82 (0.53–1.26) | 0.89 (0.60–1.32) |
| : Multivariate | 0.93 (0.37–2.35) | 1.49 (0.81–2.73) | 1.11 (0.67–1.83) | 0.99 (0.63–1.57) | 1.05 (0.70–1.58) |
| AHEI-2010: Univariate | 0.56 (0.28–1.13) | 0.76 (0.46–1.25) | 0.68 (0.45–1.03) | 0.56 (0.38–0.83) * | 0.56 (0.38–0.81) * |
| : Multivariate | 0.84 (0.39–1.80) | 0.76 (0.44–1.31) | 0.72 (0.46–1.13) | 0.65 (0.43–0.99) * | 0.63 (0.43–0.93) * |
| Cancer (excludes skin cancer) | n = 86 | n = 199 | n = 304 | n = 417 | n = 555 |
| HEIFA-2013: Univariate | 0.87 (0.44–1.72) | 1.44 (0.91–2.27) | 1.31 (0.89–1.91) | 1.31 (0.93–1.83) | 1.18 (0.87–1.60) |
| : Multivariate | 0.94 (0.46–1.95) | 1.52 (0.90–2.56) | 1.25 (0.82–1.90) | 1.40 (0.97–2.00) | 1.25 (0.91–1.72) |
| MDS: Univariate | 0.62 (0.27–1.41) | 0.83 (0.49–1.40) | 0.88 (0.57–1.36) | 1.06 (0.73–1.52) | 1.03 (0.75–1.42) |
| : Multivariate | 0.58 (0.24–1.43) | 0.85 (0.48–1.51) | 0.90 (0.56–1.43) | 1.13 (0.77–1.66) | 1.10 (0.79–1.53) |
| AHEI-2010: Univariate | 1.64 (0.82–3.25) | 1.20 (0.76–1.91) | 1.02 (0.69–1.51) | 1.11 (0.78–1.59) | 1.21 (0.88–1.65) |
| : Multivariate | 1.62 (0.78–3.36) | 1.30 (0.78–2.18) | 0.94 (0.61–1.46) | 1.19 (0.81–1.74) | 1.28 (0.93–1.77) |
| Depression/anxiety | n = 622 | n = 670 | n = 644 | n = 602 | n = 559 |
| HEIFA-2013: Univariate | 0.78 (0.60–1.03) | 0.87 (0.67–1.13) | 0.79 (0.60–1.03) | 0.80 (0.61–1.04) | 0.77 (0.58–1.03) |
| : Multivariate a | 0.96 (0.69–1.35) | 1.03 (0.74–1.41) | 0.70 (0.51–0.98) * | 0.81 (0.58–1.12) | 0.78 (0.55–1.10) |
| MDS: Univariate | 0.91 (0.68–1.21) | 1.01 (0.77–1.32) | 0.87 (0.65–1.15) | 0.66 (0.49–0.90) * | 0.72 (0.53–0.97) * |
| : Multivariate a | 1.03 (0.72–1.47) | 1.09 (0.78–1.52) | 0.84 (0.59–1.18) | 0.70 (0.49–0.96) * | 0.66 (0.46–0.94) * |
| AHEI-2010: Univariate | 0.95 (0.72–1.26) | 1.05 (0.80–1.37) | 0.94 (0.71–1.25) | 0.99 (0.74–1.32) | 0.93 (0.69–1.25) |
| : Multivariate a | 1.12 (0.80–1.58) | 1.09 (0.78–1.51) | 0.95 (0.67–1.35) | 1.07 (0.76–1.50) | 1.07 (0.75–1.53) |
| Multimorbidity | n = 133 | n = 300 | n = 473 | n = 657 | n = 857 |
| HEIFA-2013: Univariate | 0.65 (0.37–1.12) | 0.65 (0.44–0.94) * | 0.76 (0.56–1.04) | 0.77 (0.59–1.01) | 0.70 (0.54–0.90) * |
| : Multivariate a | 0.86 (0.47–1.59) | 0.70 (0.46–1.08) | 0.78 (0.54–1.10) | 0.90 (0.66–1.21) | 0.73 (0.55–0.96) * |
| MDS: Univariate | 1.13 (0.60–2.13) | 0.80 (0.51–1.26) | 0.64 (0.44–0.92) * | 0.66 (0.48–0.90) * | 0.75 (0.57–0.98) * |
| : Multivariate a | 1.25 (0.60–2.59) | 1.09 (0.66–1.80) | 0.76 (0.51–1.14) | 0.83 (0.58–1.17) | 0.87 (0.65–1.17) |
| AHEI-2010: Univariate | 0.72 (0.41–1.26) | 0.68 (0.46–1.00) | 0.74 (0.54–1.02) | 0.56 (0.43–0.74) * | 0.63 (0.49–0.81) * |
| : Multivariate a | 0.93 (0.50–1.74) | 0.73 (0.47–1.12) | 0.89 (0.63–1.26) | 0.70 (0.51–0.96) * | 0.75 (0.57–0.99) * |
| Diet Quality Index | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) |
|---|---|---|---|---|---|
| All-Cause Mortality in all Women | |||||
| Number of deaths at each survey | n = 32 | n = 28 | n = 49 | n = 55 | n = 31 |
| HEIFA-2013 | S4 (n = 5334) a | S5 (n = 5302) a | S6 (n = 5274) a | S7 (n= 5225) a | S8 (n = 5170) a |
| Univariate | 0.98 (0.37–2.61) | 0.73 (0.30–1.79) | 0.93 (0.45–1.94) | 0.54 (0.28–1.07) | 0.37 (0.14–1.01) |
| S4 (n = 3618) b | S5 (n = 4180) b | S6 (n = 4024) b | S7 (n= 3955) b | S8 (n = 3906) b | |
| Multivariate * | 2.03 (0.53–7.77) | 0.69 (0.21–2.24) | 0.72 (0.27–1.93) | 0.63 (0.26–1.50) | 0.44 (0.13–1.48) |
| MDS | S4 (n = 5334) a | S5 (n = 5302) a | S6 (n = 5274) a | S7 (n= 5225) a | S8 (n = 5170) a |
| Univariate | 0.57 (0.20–1.64) | 0.57 (0.22–1.52) | 0.45 (0.20–1.01) | 0.80 (0.37–1.71) | 0.38 (0.14–1.05) |
| S4 (n = 3618) b | S5 (n = 4180) b | S6 (n = 3240) b | S7 (n= 3955) b | S8 (n = 3906) b | |
| Multivariate * | 1.64 (0.48–5.67) | 0.33 (0.07–1.57) | 0.42 (0.16–1.10) | 0.92 (0.32–2.63) | 0.61 (0.18–2.01) |
| AHEI-2010 | S4 (n = 5334) a | S5 (n = 5302) a | S6 (n = 5274) a | S7 (n= 5225) a | S8 (n = 5170) a |
| Univariate | 0.26 (0.09–0.78) ** | 0.94 (0.32–2.76) | 0.98 (0.48–2.02) | 0.62 (0.32–1.22) | 0.51 (0.22–1.21) |
| S4 (n = 3618) b | S5 (n = 4180) b | S6 (n = 4024) b | S7 (n= 3955) b | S8 (n = 3906) b | |
| Multivariate * | 0.88 (0.23–3.41) | 0.55 (0.12–2.61) | 0.89 (0.34–2.36) | 1.43 (0.52–3.88) | 1.14 (0.37–3.46) |
| All-cause Mortality in women with NCD | |||||
| HEIFA-2013 | S4 (n = 1241) c | S5 (n = 1709) c | S6 (n = 2085) c | S7 (n= 2414) c | S8 (n = 2660) c |
| Univariate | 0.86 (0.20–3.63) | 0.53 (0.15–1.84) | 0.83 (0.32–2.16) | 0.67 (0.30–1.49) | 0.38 (0.13–1.10) |
| S4 (n = 573) d | S5 (n = 827) d | S6 (n = 1394) d | S7 (n = 1923) d | S8 (n = 2139) d | |
| Multivariate | 1.02 (0.16–6.54) | 0.19 (0.03–1.05) | 0.63 (0.19–2.15) | 0.76 (0.29–1.95) | 0.52 (0.15–1.80) |
| MDS | S4 (n = 1241) c | S5 (n = 1709) c | S6 (n = 2085) c | S7 (n = 2414) c | S8 (n = 2660) c |
| Univariate | 0.41 (0.04–3.99) | 0.74 (0.21–2.53) | 0.41 (0.13–1.26) | 0.87 (0.31–2.44) | 0.50 (0.18–1.42) |
| S4 (n = 713) d | S5 (n = 827) d | S6 (n = 1131) d | S7 (n = 1923) d | S8 (n = 2139) d | |
| Multivariate | 0.93 (0.07–11.88) | 0.21 (0.02–1.94) | 0.35 (0.09–1.29) | 0.96 (0.29–3.12) | 0.68 (0.20–2.29) |
| AHEI-2010 | S4 (n = 1241) c | S5 (n = 1709) c | S6 (n = 2085) c | S7 (n= 2414) c | S8 (n = 2660) c |
| Univariate | 0.32 (0.05–1.92) | 0.70 (0.16–3.16) | 0.66 (0.26–1.69) | 1.64 (0.60–4.49) | 0.46 (0.18–1.20) |
| S4 (n = 713) d | S5 (n = 827) d | S6 (n = 1394) d | S7 (n = 1923) d | S8 (n = 2139) d | |
| Multivariate | 0.97 (0.08–11.75) | 0.17 (0.02–1.80) | 0.54 (0.16–1.80) | 3.61 (0.79–16.54) | 1.05 (0.34–3.28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hlaing-Hlaing, H.; Dolja-Gore, X.; Tavener, M.; James, E.L.; Hodge, A.M.; Hure, A.J. Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. Int. J. Environ. Res. Public Health 2021, 18, 11375. https://doi.org/10.3390/ijerph182111375
Hlaing-Hlaing H, Dolja-Gore X, Tavener M, James EL, Hodge AM, Hure AJ. Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. International Journal of Environmental Research and Public Health. 2021; 18(21):11375. https://doi.org/10.3390/ijerph182111375
Chicago/Turabian StyleHlaing-Hlaing, Hlaing, Xenia Dolja-Gore, Meredith Tavener, Erica L. James, Allison M. Hodge, and Alexis J. Hure. 2021. "Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health" International Journal of Environmental Research and Public Health 18, no. 21: 11375. https://doi.org/10.3390/ijerph182111375
APA StyleHlaing-Hlaing, H., Dolja-Gore, X., Tavener, M., James, E. L., Hodge, A. M., & Hure, A. J. (2021). Diet Quality and Incident Non-Communicable Disease in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. International Journal of Environmental Research and Public Health, 18(21), 11375. https://doi.org/10.3390/ijerph182111375