
Risk of Aortic Aneurysm and Dissection in Patients with Tuberculosis: A Nationwide Population-Based Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
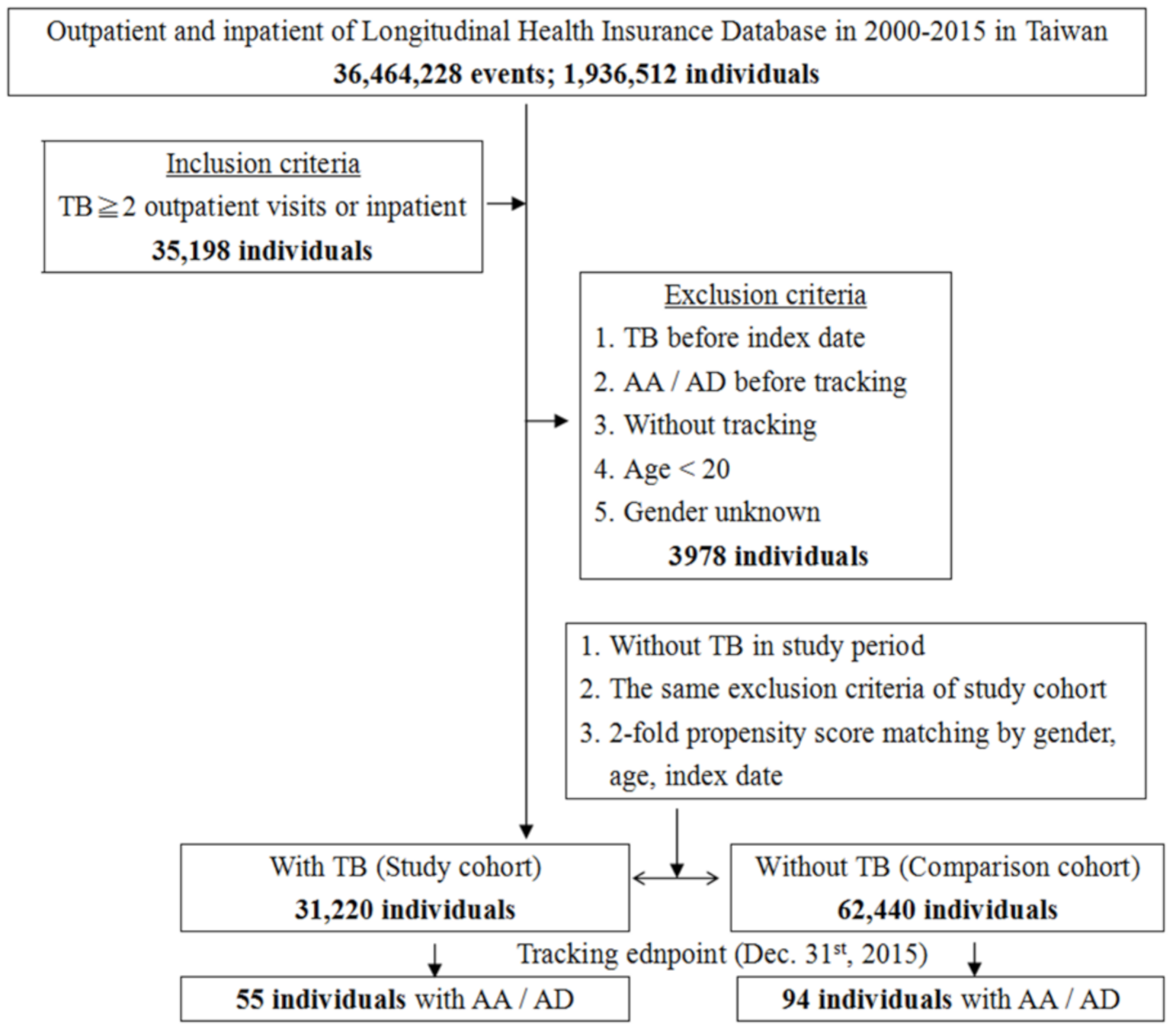
2.2. Sampled Patients
2.3. Outcome Measurement and Comorbidities
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Centers for Disease Control. Taiwan Tuberculosis Control Report 2019; Ministry of Health and Welfare: Taipei, Taiwan, 2020. [Google Scholar]
- Ravimohan, S.; Kornfeld, H.; Weissman, D.; Bisson, G.P. Tuberculosis and lung damage: From epidemiology to pathophysiology. Eur. Respir. Rev. 2018, 27, 170077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez-Lapausa, M.; Menéndez-Saldaña, A.; Noguerado-Asensio, A. Extrapulmonary tuberculosis. Rev. Esp. Sanid. Penit. 2015, 17, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, F.M.; Daugherty, A.; Lu, H.S. Updates of Recent Aortic Aneurysm Research. Arterioscler. Thromb. Vasc. Biol. 2019, 39, e83–e90. [Google Scholar] [CrossRef] [PubMed]
- Gawinecka, J.; Schönrath, F.; von Eckardstein, A. Acute aortic dissection: Pathogenesis, risk factors and diagnosis. Swiss Med. Wkly. 2017, 147, w14489. [Google Scholar]
- Yeh, T.-Y.; Chen, C.-Y.; Huang, J.-W.; Chiu, C.-C.; Lai, W.-T.; Huang, Y.-B. Epidemiology and Medication Utilization Pattern of Aortic Dissection in Taiwan: A Population-Based Study. Medicine 2015, 94, e1522. [Google Scholar] [CrossRef]
- Braverman, A.C. Acute aortic dissection: Clinician update. Circulation 2010, 122, 184–188. [Google Scholar] [CrossRef] [Green Version]
- Keisler, B.; Carter, C. Abdominal aortic aneurysm. Am. Fam. Physician 2015, 91, 538–543. [Google Scholar]
- Nienaber, C.A.; Powell, J.T. Management of acute aortic syndromes. Eur. Heart J. 2012, 33, 26–35. [Google Scholar] [CrossRef]
- Osler, W. The Gulstonian Lectures, on Malignant Endocarditis. Br. Med. J. 1885, 1, 467–470. [Google Scholar] [CrossRef] [Green Version]
- Sörelius, K.; Budtz-Lilly, J.; Mani, K.; Wanhainen, A. Systematic Review of the Management of Mycotic Aortic Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 426–435. [Google Scholar] [CrossRef]
- Peng, Y.C.; Lin, C.L.; Hsu, W.Y.; Chang, C.S.; Yeh, H.Z.; Kao, C.H. Risk of liver cirrhosis in patients with tuberculosis: A nationwide cohort study. Eur. J. Clin. Investig. 2015, 45, 663–669. [Google Scholar] [CrossRef]
- Shen, C.H.; Chou, C.H.; Liu, F.C.; Lin, T.Y.; Huang, W.Y.; Wang, Y.C.; Kao, C.H. Association Between Tuberculosis and Parkinson Disease: A Nationwide, Population-Based Cohort Study. Medicine 2016, 95, e2883. [Google Scholar] [CrossRef]
- Wang, S.H.; Chung, C.H.; Huang, T.W.; Tsai, W.C.; Peng, C.K.; Huang, K.L.; Perng, W.C.; Chian, C.F.; Chien, W.C.; Shen, C.H. Bidirectional association between tuberculosis and sarcoidosis. Respirology 2019, 24, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Liang, S.J.; Liu, Y.H.; Hsu, W.H.; Shih, C.M.; Sung, F.C.; Chen, W. Tuberculosis as a risk factor for systemic lupus erythematosus: Results of a nationwide study in Taiwan. Rheumatol. Int. 2012, 32, 1669–1673. [Google Scholar] [CrossRef]
- Chung, W.S.; Lin, C.L.; Hung, C.T.; Chu, Y.H.; Sung, F.C.; Kao, C.H.; Yeh, J.J. Tuberculosis increases the subsequent risk of acute coronary syndrome: A nationwide population-based cohort study. Int. J. Tuberc. Lung Dis. 2014, 18, 79–83. [Google Scholar] [CrossRef]
- Wang, S.H.; Chien, W.C.; Chung, C.H.; Lin, F.H.; Peng, C.K.; Chian, C.F.; Shen, C.H. Tuberculosis increases the risk of peripheral arterial disease: A nationwide population-based study. Respirology 2017, 22, 1670–1676. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, S.H.; Dorhoi, A. Inflammation in tuberculosis: Interactions, imbalances and interventions. Curr. Opin. Immunol. 2013, 25, 441–449. [Google Scholar] [CrossRef]
- Galkina, E.; Ley, K. Immune and inflammatory mechanisms of atherosclerosis (*). Annu. Rev. Immunol. 2009, 27, 165–197. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Wen, D.; Zhou, X.L.; Li, J.J.; Luo, F.; Zhang, L.; Gao, L.G.; Wang, L.P.; Song, L.; Sun, K.; Zou, Y.B.; et al. Plasma concentrations of interleukin-6, C-reactive protein, tumor necrosis factor-α and matrix metalloproteinase-9 in aortic dissection. Clin. Chim. Acta 2012, 413, 198–202. [Google Scholar] [CrossRef]
- Lindholt, J.S.; Shi, G.P. Chronic inflammation, immune response, and infection in abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 453–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.K.; Mohan, A.; Sharma, A. Challenges in the diagnosis & treatment of miliary tuberculosis. Indian J. Med. Res. 2012, 135, 703–730. [Google Scholar] [PubMed]
- Ugajin, M.; Miwa, S.; Shirai, M.; Ohba, H.; Eifuku, T.; Nakamura, H.; Suda, T.; Hayakawa, H.; Chida, K. Usefulness of serum procalcitonin levels in pulmonary tuberculosis. Eur. Respir. J. 2011, 37, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, R.; Guzman, R.; Greenberg, H.; Safneck, J.; Hershfield, E. Tuberculous mycotic aneurysm of the aorta: Review of published medical and surgical experience. Chest 1999, 115, 522–531. [Google Scholar] [CrossRef]
- Elkington, P.T.; Ugarte-Gil, C.A.; Friedland, J.S. Matrix metalloproteinases in tuberculosis. Eur. Respir. J. 2011, 38, 456–464. [Google Scholar] [CrossRef] [Green Version]
- Sabir, N.; Hussain, T.; Mangi, M.H.; Zhao, D.; Zhou, X. Matrix metalloproteinases: Expression, regulation and role in the immunopathology of tuberculosis. Cell Prolif. 2019, 52, e12649. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Shen, Y.H.; LeMaire, S.A. Thoracic aortic dissection: Are matrix metalloproteinases involved? Vascular 2009, 17, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Maguire, E.M.; Pearce, S.W.A.; Xiao, R.; Oo, A.Y.; Xiao, Q. Matrix Metalloproteinase in Abdominal Aortic Aneurysm and Aortic Dissection. Pharmaceuticals 2019, 12, 118. [Google Scholar] [CrossRef] [Green Version]
- Wilson, W.R.; Anderton, M.; Choke, E.C.; Dawson, J.; Loftus, I.M.; Thompson, M.M. Elevated plasma MMP1 and MMP9 are associated with abdominal aortic aneurysm rupture. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 580–584. [Google Scholar] [CrossRef] [Green Version]
- Kurihara, T.; Shimizu-Hirota, R.; Shimoda, M.; Adachi, T.; Shimizu, H.; Weiss, S.J.; Itoh, H.; Hori, S.; Aikawa, N.; Okada, Y. Neutrophil-derived matrix metalloproteinase 9 triggers acute aortic dissection. Circulation 2012, 126, 3070–3080. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Zarins, C.K.; Glagov, S. Aneurysmal and occlusive atherosclerosis of the human abdominal aorta. J. Vasc. Surg. 2001, 33, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golledge, J.; Norman, P.E. Atherosclerosis and abdominal aortic aneurysm: Cause, response, or common risk factors? Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1075–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanson, A.W.; Kazmier, F.J.; Hollier, L.H.; Edwards, W.D.; Pairolero, P.C.; Sheedy, P.F.; Joyce, J.W.; Johnson, M.C. Penetrating atherosclerotic ulcers of the thoracic aorta: Natural history and clinicopathologic correlations. Ann. Vasc. Surg. 1986, 1, 15–23. [Google Scholar] [CrossRef]
- Hayashi, H.; Matsuoka, Y.; Sakamoto, I.; Sueyoshi, E.; Okimoto, T.; Hayashi, K.; Matsunaga, N. Penetrating atherosclerotic ulcer of the aorta: Imaging features and disease concept. Radiographics 2000, 20, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.A.; Rosenfeld, M.E. Infection and Atherosclerosis Development. Arch. Med. Res. 2015, 46, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pothineni, N.V.K.; Subramany, S.; Kuriakose, K.; Shirazi, L.F.; Romeo, F.; Shah, P.K.; Mehta, J.L. Infections, atherosclerosis, and coronary heart disease. Eur. Heart J. 2017, 38, 3195–3201. [Google Scholar] [CrossRef] [PubMed]
- Huaman, M.A.; Henson, D.; Ticona, E.; Sterling, T.R.; Garvy, B.A. Tuberculosis and Cardiovascular Disease: Linking the Epidemics. Trop. Dis. Travel Med. Vaccines 2015, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gruber, R.; Lederer, S.; Bechtel, U.; Lob, S.; Riethmüller, G.; Feucht, H.E. Increased antibody titers against mycobacterial heat-shock protein 65 in patients with vasculitis and arteriosclerosis. Int. Arch. Allergy Immunol. 1996, 110, 95–98. [Google Scholar] [CrossRef]
- Zhu, J.; Katz, R.J.; Quyyumi, A.A.; Canos, D.A.; Rott, D.; Csako, G.; Zalles-Ganley, A.; Ogunmakinwa, J.; Wasserman, A.G.; Epstein, S.E. Association of serum antibodies to heat-shock protein 65 with coronary calcification levels: Suggestion of pathogen-triggered autoimmunity in early atherosclerosis. Circulation 2004, 109, 36–41. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Total | With TB | Without TB | p | ||||
|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | |
| Overall | 93,660 | 31,220 | 33.33 | 62,440 | 66.67 | ||
| Sex | 0.999 | ||||||
| Male | 66,657 | 71.17 | 22,219 | 71.17 | 44,438 | 71.17 | |
| Female | 27,003 | 28.83 | 9001 | 28.83 | 18,002 | 28.83 | |
| Age (years) | 63.67 ± 17.32 | 63.74 ± 17.33 | 63.64 ± 17.32 | 0.405 | |||
| Age group (years) | 0.999 | ||||||
| 20–44 | 16,314 | 17.42 | 5438 | 17.42 | 10,876 | 17.42 | |
| 45–69 | 33,876 | 36.17 | 11,292 | 36.17 | 22,584 | 36.17 | |
| ≥70 | 43,470 | 46.41 | 14,490 | 46.41 | 28,980 | 46.41 | |
| Insured premium (NT$) | 0.003 | ||||||
| <18,000 | 92,378 | 98.63 | 30,768 | 98.55 | 61,610 | 98.67 | |
| 18,000–34,999 | 1032 | 1.10 | 385 | 1.23 | 647 | 1.04 | |
| ≥35,000 | 250 | 0.27 | 67 | 0.21 | 183 | 0.29 | |
| DM | <0.001 | ||||||
| Without | 70,368 | 75.13 | 23,042 | 73.81 | 47,326 | 75.79 | |
| With | 23,292 | 24.87 | 8178 | 26.19 | 15,114 | 24.21 | |
| HTN | <0.001 | ||||||
| Without | 59,003 | 63.00 | 21,732 | 69.61 | 37,271 | 59.69 | |
| With | 34,657 | 37.00 | 9488 | 30.39 | 25,169 | 40.31 | |
| Hyperlipidemia | <0.001 | ||||||
| Without | 87,769 | 93.71 | 30,159 | 96.60 | 57,610 | 92.26 | |
| With | 5891 | 6.29 | 1061 | 3.40 | 4830 | 7.74 | |
| IHD | <0.001 | ||||||
| Without | 71,662 | 76.51 | 26,219 | 83.98 | 45,443 | 72.78 | |
| With | 21,998 | 23.49 | 5001 | 16.02 | 16,997 | 27.22 | |
| COPD | <0.001 | ||||||
| Without | 69,531 | 74.24 | 21,719 | 69.57 | 47,812 | 76.57 | |
| With | 24,129 | 25.76 | 9501 | 30.43 | 14,628 | 23.43 | |
| Stroke | <0.001 | ||||||
| Without | 73,991 | 79.00 | 26,519 | 84.94 | 47,472 | 76.03 | |
| With | 19,669 | 21.00 | 4701 | 15.06 | 14,968 | 23.97 | |
| CKD | <0.001 | ||||||
| Without | 89,710 | 95.78 | 30,153 | 96.58 | 59,557 | 95.38 | |
| With | 3950 | 4.22 | 1067 | 3.42 | 2883 | 4.62 | |
| PAOD | 0.053 | ||||||
| Without | 93,603 | 99.94 | 31,208 | 99.96 | 62,395 | 99.93 | |
| With | 57 | 0.06 | 12 | 0.04 | 45 | 0.07 | |
| Obesity | 0.002 | ||||||
| Without | 93,632 | 99.97 | 31,218 | 99.99 | 62,414 | 99.96 | |
| With | 28 | 0.03 | 2 | 0.01 | 26 | 0.04 | |
| Urbanization level | <0.001 | ||||||
| 1 (The highest) | 28,768 | 30.72 | 8960 | 28.70 | 19,808 | 31.72 | |
| 2 | 41,696 | 44.52 | 13,732 | 43.98 | 27,964 | 44.79 | |
| 3 | 7425 | 7.93 | 2565 | 8.22 | 4860 | 7.78 | |
| 4 (The lowest) | 15,771 | 16.84 | 5963 | 19.10 | 9808 | 15.71 | |
| Variables | Crude HR | 95% CI | p | aHR | 95% CI | p | ||
|---|---|---|---|---|---|---|---|---|
| TB | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.064 | 1.154 | 2.875 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| Sex | ||||||||
| Male | 1.501 | 0.905 | 2.408 | 0.110 | 1.440 | 0.899 | 2.306 | 0.129 |
| Female | Reference | Reference | ||||||
| Age group (years) | ||||||||
| 20–44 | Reference | Reference | ||||||
| 45–69 | 1.786 | 0.772 | 2.345 | 0.512 | 1.518 | 0.565 | 2.103 | 0.533 |
| ≥70 | 2.065 | 0.989 | 3.397 | 0.668 | 1.669 | 0.789 | 3.020 | 0.696 |
| Insured premium (NT$) | ||||||||
| <18,000 | Reference | Reference | ||||||
| 18,000–34,999 | 0.000 | - | - | 0.997 | 0.000 | - | - | 0.998 |
| ≥35,000 | 0.000 | - | - | 0.997 | 0.000 | - | - | 0.998 |
| DM | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.589 | 1.062 | 2.267 | 0.020 | 1.336 | 0.828 | 2.154 | 0.236 |
| HTN | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.309 | 1.498 | 3.020 | <0.001 | 1.471 | 1.311 | 1.711 | <0.001 |
| Hyperlipidemia | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | - | - | 0.972 | 0.000 | - | - | 0.786 |
| IHD | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.903 | 1.564 | 2.303 | <0.001 | 1.825 | 1.555 | 2.225 | <0.001 |
| COPD | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.986 | 0.387 | 1.567 | 0.084 | 1.087 | 0.460 | 1.626 | 0.067 |
| Stroke | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.976 | 1.876 | 4.021 | <0.001 | 2.027 | 1.690 | 2.529 | <0.001 |
| CKD | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.768 | 1.001 | 2.897 | 0.050 | 1.563 | 0.881 | 2.670 | 0.323 |
| PAOD | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | - | - | 0.913 | 0.000 | - | - | 0.958 |
| Obesity | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | - | - | 0.984 | 0.000 | - | - | 0.982 |
| Urbanization level | ||||||||
| 1 (The highest) | 1.726 | 1.329 | 2.676 | <0.001 | 1.637 | 1.278 | 2.461 | <0.001 |
| 2 | 1.682 | 1.345 | 2.443 | <0.001 | 1.606 | 1.259 | 2.368 | <0.001 |
| 3 | 1.201 | 1.006 | 1.703 | 0.045 | 1.186 | 0.936 | 1.694 | 0.287 |
| 4 (The lowest) | Reference | Reference | ||||||
| TB | With | Without | With vs. without (Reference) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Event | Rate (per 103 PYs) | Event | Rate (per 103 PYs) | IRR | 95% CI | p | aHR | 95% CI | p | ||
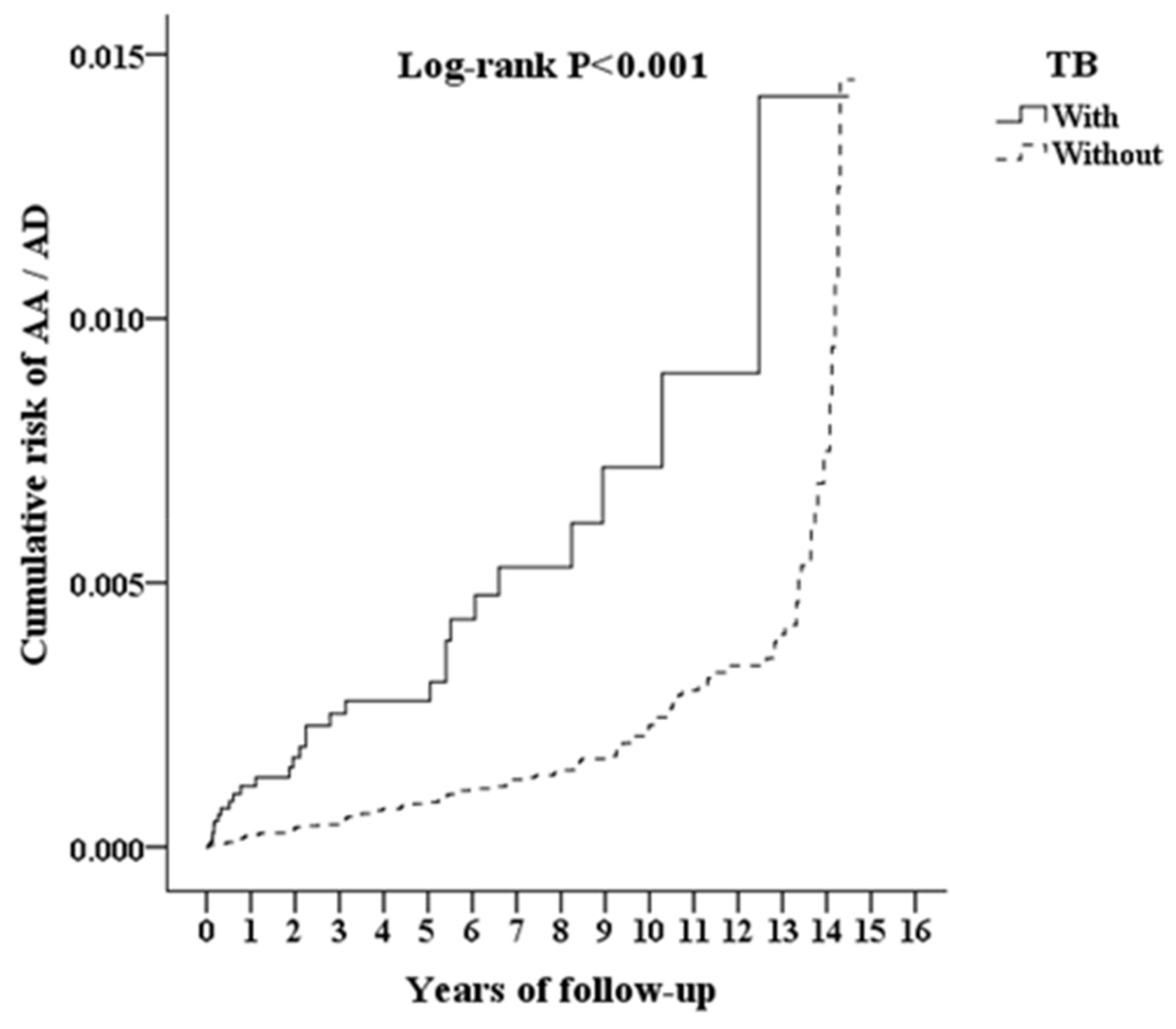
| Overall | 55 | 0.185 | 94 | 0.150 | 1.235 | 1.071 | 1.567 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| Sex | ||||||||||||
| Male | 43 | 0.202 | 72 | 0.161 | 1.254 | 1.139 | 1.631 | <0.001 | 1.738 | 1.115 | 2.702 | <0.001 |
| Female | 12 | 0.143 | 22 | 0.123 | 1.165 | 1.032 | 1.868 | 0.006 | 1.616 | 1.034 | 2.518 | 0.008 |
| Age group (years) | ||||||||||||
| 20–44 | 2 | 0.061 | 3 | 0.051 | 1.188 | 1.046 | 2.976 | 0.002 | 1.645 | 1.051 | 2.553 | 0.002 |
| 45–69 | 12 | 0.125 | 18 | 0.098 | 1.270 | 1.088 | 2.000 | <0.001 | 1.760 | 1.129 | 2.712 | <0.001 |
| ≥70 | 41 | 0.244 | 73 | 0.189 | 1.287 | 1.148 | 1.669 | <0.001 | 1.784 | 1.153 | 2.789 | <0.001 |
| Insured premium (NT$) | ||||||||||||
| <18,000 | 55 | 0.188 | 94 | 0.152 | 1.238 | 1.178 | 1.571 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| 18,000–34,999 | 0 | 0.000 | 0 | 0.000 | - | - | - | - | - | - | - | - |
| ≥35,000 | 0 | 0.000 | 0 | 0.000 | - | - | - | - | - | - | - | - |
| DM | ||||||||||||
| Without | 40 | 0.204 | 73 | 0.169 | 1.208 | 1.070 | 1.594 | 0.003 | 1.672 | 1.074 | 2.609 | 0.001 |
| With | 15 | 0.149 | 21 | 0.108 | 1.374 | 1.218 | 2.036 | <0.001 | 1.911 | 1.223 | 2.972 | <0.001 |
| HTN | ||||||||||||
| Without | 22 | 0.141 | 39 | 0.139 | 1.018 | 1.006 | 1.541 | 0.036 | 1.411 | 0.995 | 2.194 | 0.053 |
| With | 33 | 0.234 | 55 | 0.159 | 1.468 | 1.347 | 1.899 | <0.001 | 2.034 | 1.314 | 3.287 | <0.001 |
| Hyperlipidemia | ||||||||||||
| Without | 55 | 0.200 | 94 | 0.172 | 1.163 | 1.057 | 1.747 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| With | 0 | 0.000 | 0 | 0.000 | - | - | - | - | - | - | - | - |
| IHD | ||||||||||||
| Without | 35 | 0.164 | 52 | 0.131 | 1.257 | 1.105 | 1.685 | <0.001 | 1.672 | 1.092 | 2.585 | <0.001 |
| With | 20 | 0.237 | 42 | 0.183 | 1.296 | 1.198 | 1.828 | <0.001 | 1.797 | 1.153 | 2.801 | <0.001 |
| COPD | ||||||||||||
| Without | 31 | 0.192 | 68 | 0.154 | 1.249 | 1.098 | 1.674 | <0.001 | 1.633 | 1.065 | 2.598 | 0.003 |
| With | 24 | 0.177 | 26 | 0.141 | 1.256 | 1.125 | 1.810 | <0.001 | 1.740 | 1.117 | 2.712 | <0.001 |
| Stroke | ||||||||||||
| Without | 37 | 0.162 | 57 | 0.130 | 1.242 | 1.069 | 1.655 | <0.001 | 1.666 | 1.004 | 2.635 | 0.045 |
| With | 18 | 0.264 | 37 | 0.196 | 1.348 | 1.199 | 1.911 | <0.001 | 1.869 | 1.118 | 3.012 | <0.001 |
| CKD | ||||||||||||
| Without | 50 | 0.178 | 88 | 0.148 | 1.202 | 1.104 | 1.549 | <0.001 | 1.675 | 1.068 | 2.596 | 0.007 |
| With | 5 | 0.302 | 6 | 0.179 | 1.681 | 1.297 | 2.866 | <0.001 | 2.330 | 1.486 | 3.631 | <0.001 |
| PAOD | ||||||||||||
| Without | 55 | 0.185 | 94 | 0.150 | 1.234 | 1.211 | 1.581 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| With | 0 | 0.000 | 0 | 0.000 | - | - | - | - | - | - | - | - |
| Obesity | ||||||||||||
| Without | 55 | 0.185 | 94 | 0.150 | 1.234 | 1.194 | 1.566 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| With | 0 | 0.000 | 0 | 0.000 | - | - | - | - | - | - | - | - |
| Urbanization level | ||||||||||||
| 1 (The highest) | 13 | 0.163 | 20 | 0.113 | 1.441 | 1.115 | 2.139 | <0.001 | 1.997 | 1.297 | 3.121 | <0.001 |
| 2 | 14 | 0.110 | 25 | 0.087 | 1.263 | 1.096 | 1.917 | 0.001 | 1.750 | 1.125 | 2.784 | <0.001 |
| 3 | 5 | 0.220 | 10 | 0.210 | 1.048 | 0.964 | 2.121 | 0.067 | 1.452 | 0.917 | 2.266 | 0.154 |
| 4 (The lowest) | 23 | 0.341 | 39 | 0.337 | 1.011 | 0.646 | 1.526 | 0.294 | 1.400 | 0.896 | 2.101 | 0.297 |
| TB | With | Without | With vs. without (Reference) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TB Subgroup | Event | Rate (per 103 PYs) | Event | Rate (per 103 PYs) | IRR | 95% CI | p | aHR | 95% CI | p | ||
| Pulmonary TB | 42 | 0.169 | 94 | 0.150 | 1.126 | 1.058 | 1.490 | 0.001 | 1.561 | 1.005 | 2.431 | 0.044 |
| Extrapulmonary TB | 9 | 0.205 | 94 | 0.150 | 1.365 | 1.160 | 2.049 | <0.001 | 1.892 | 1.214 | 2.936 | <0.001 |
| Miliary TB | 4 | 0.902 | 94 | 0.150 | 6.013 | 4.870 | 8.802 | <0.001 | 8.334 | 5.348 | 12.896 | <0.001 |
| TB | With | Without | With vs. without (Reference) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AA/AD Subgroup | Event | Rate (per 103 PYs) | Event | Rate (per 103 PYs) | IRR | 95% CI | p | aHR | 95% CI | p | ||
| Overall | 55 | 0.185 | 94 | 0.150 | 1.235 | 1.071 | 1.567 | <0.001 | 1.711 | 1.098 | 2.666 | <0.001 |
| Thoracic | 16 | 0.054 | 29 | 0.046 | 1.164 | 1.039 | 1.498 | 0.015 | 1.615 | 1.044 | 2.511 | 0.007 |
| Abdominal | 13 | 0.044 | 24 | 0.038 | 1.143 | 1.015 | 1.435 | 0.038 | 1.588 | 1.025 | 2.469 | 0.024 |
| Thoracoabdominal | 1 | 0.003 | 1 | 0.002 | 2.110 | 1.753 | 2.525 | <0.001 | 2.910 | 1.876 | 4.557 | <0.001 |
| Unspecified site | 25 | 0.084 | 40 | 0.064 | 1.319 | 1.188 | 1.682 | <0.001 | 1.823 | 1.175 | 2.843 | <0.001 |
| TB | With | Without | With vs. without (Reference) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Follow-Up Period | Event | Rate (per 103 PYs) | Event | Rate (per 103 PYs) | IRR | 95% CI | p | aHR | 95% CI | p | ||
| <6 months | 17 | 1.192 | 7 | 0.236 | 5.061 | 4.267 | 7.106 | <0.001 | 6.896 | 5.010 | 8.226 | <0.001 |
| 6 months–12 months | 4 | 0.283 | 5 | 0.169 | 1.671 | 1.335 | 1.986 | <0.001 | 2.671 | 1.675 | 3.145 | <0.001 |
| 1–5 years | 20 | 0.136 | 28 | 0.092 | 1.481 | 1.198 | 1.875 | <0.001 | 2.371 | 1.486 | 2.884 | <0.001 |
| >5 years | 14 | 0.115 | 54 | 0.206 | 0.560 | 0.042 | 0.989 | 0.041 | 1.276 | 0.375 | 1.790 | 0.385 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-T.; Chung, C.-H.; Ke, H.-Y.; Peng, C.-K.; Chien, W.-C.; Shen, C.-H. Risk of Aortic Aneurysm and Dissection in Patients with Tuberculosis: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 11075. https://doi.org/10.3390/ijerph182111075
Chen M-T, Chung C-H, Ke H-Y, Peng C-K, Chien W-C, Shen C-H. Risk of Aortic Aneurysm and Dissection in Patients with Tuberculosis: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11075. https://doi.org/10.3390/ijerph182111075
Chicago/Turabian StyleChen, Ming-Tsung, Chi-Hsiang Chung, Hung-Yen Ke, Chung-Kan Peng, Wu-Chien Chien, and Chih-Hao Shen. 2021. "Risk of Aortic Aneurysm and Dissection in Patients with Tuberculosis: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 21: 11075. https://doi.org/10.3390/ijerph182111075
APA StyleChen, M.-T., Chung, C.-H., Ke, H.-Y., Peng, C.-K., Chien, W.-C., & Shen, C.-H. (2021). Risk of Aortic Aneurysm and Dissection in Patients with Tuberculosis: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 18(21), 11075. https://doi.org/10.3390/ijerph182111075