
Dental Healthcare Amid the COVID-19 Pandemic

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. History and Evolution Novel Coronavirus
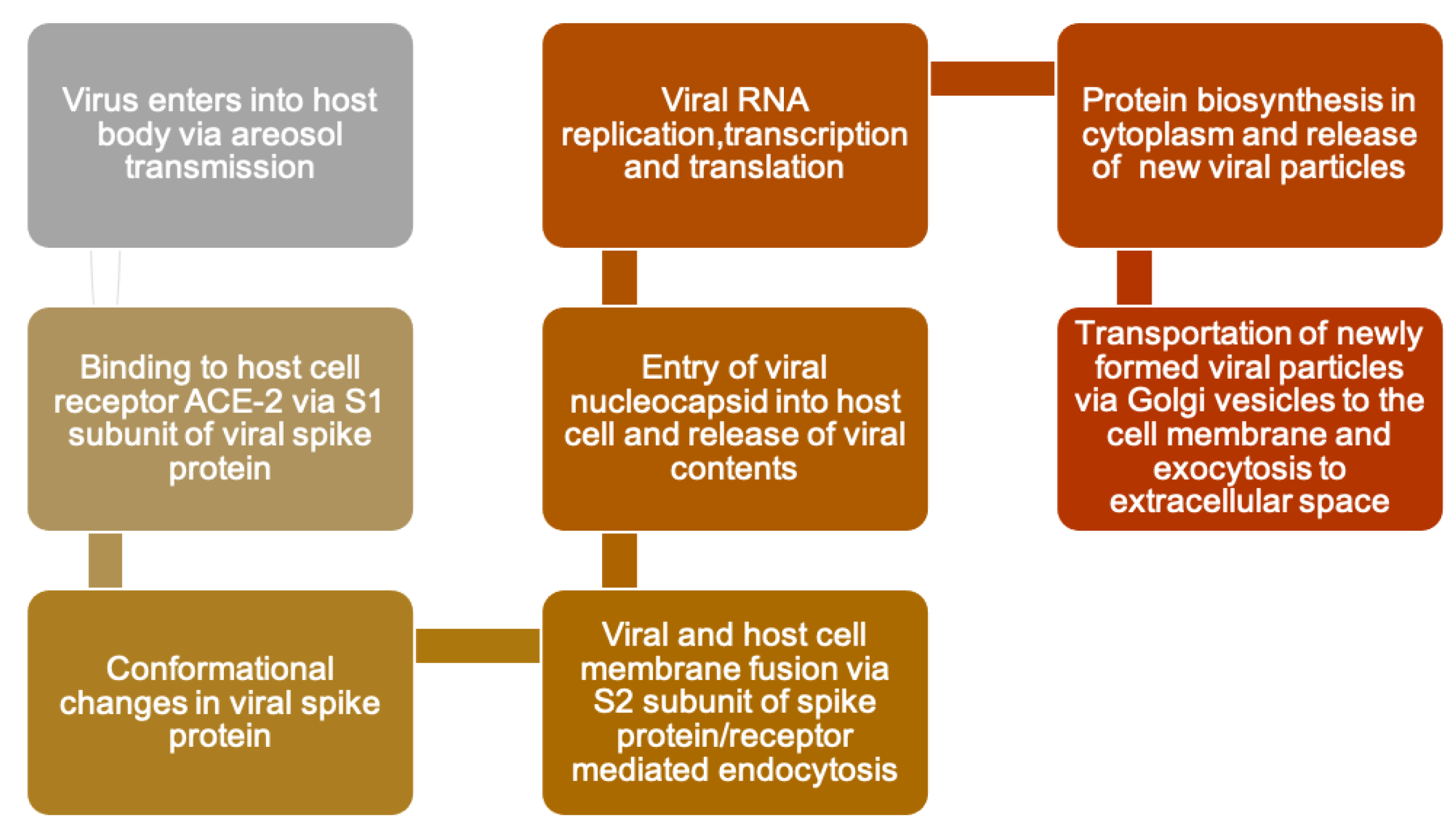
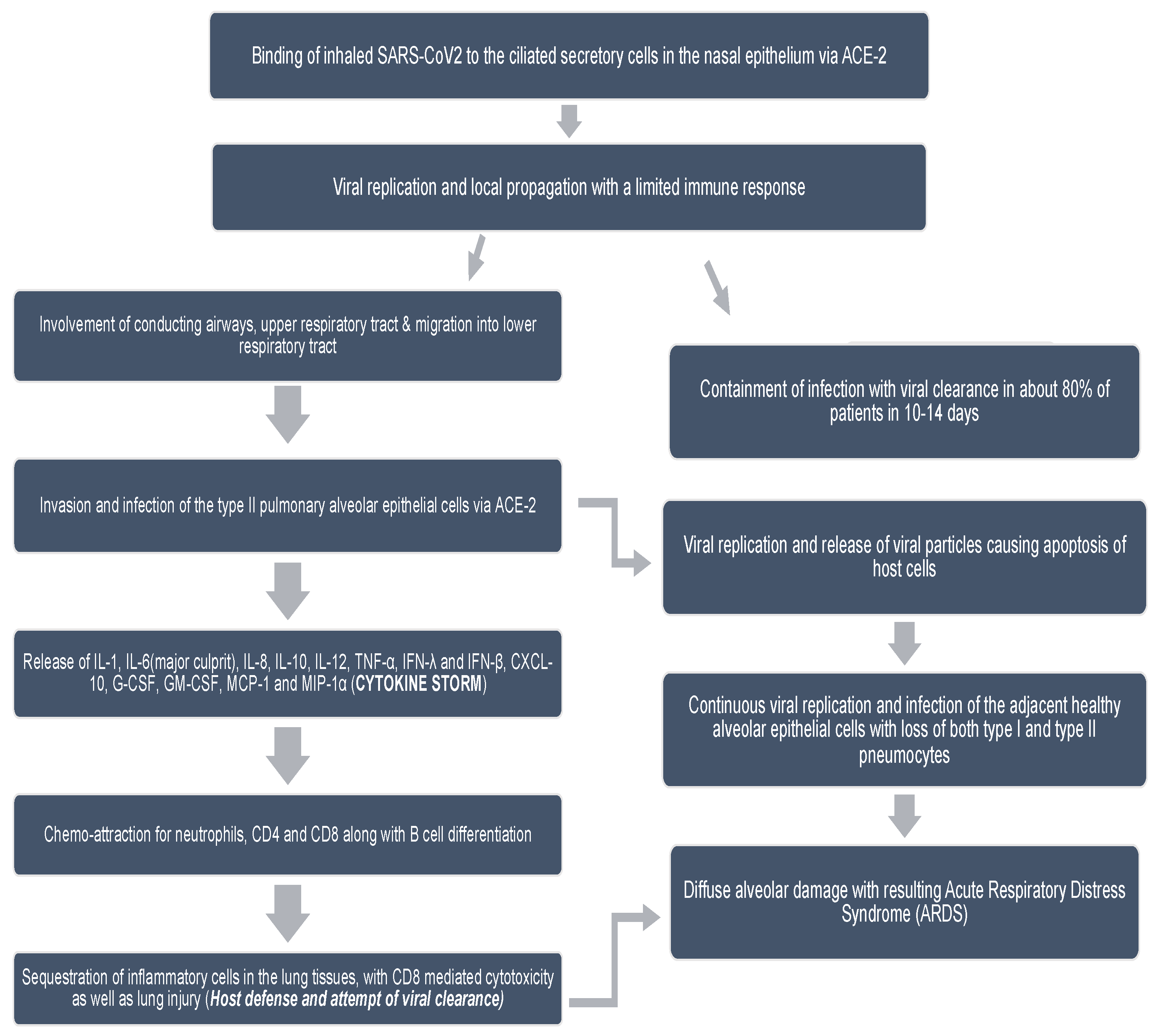
3. Specific Virology, Pathophysiology, and Life Cycle of COVID-19
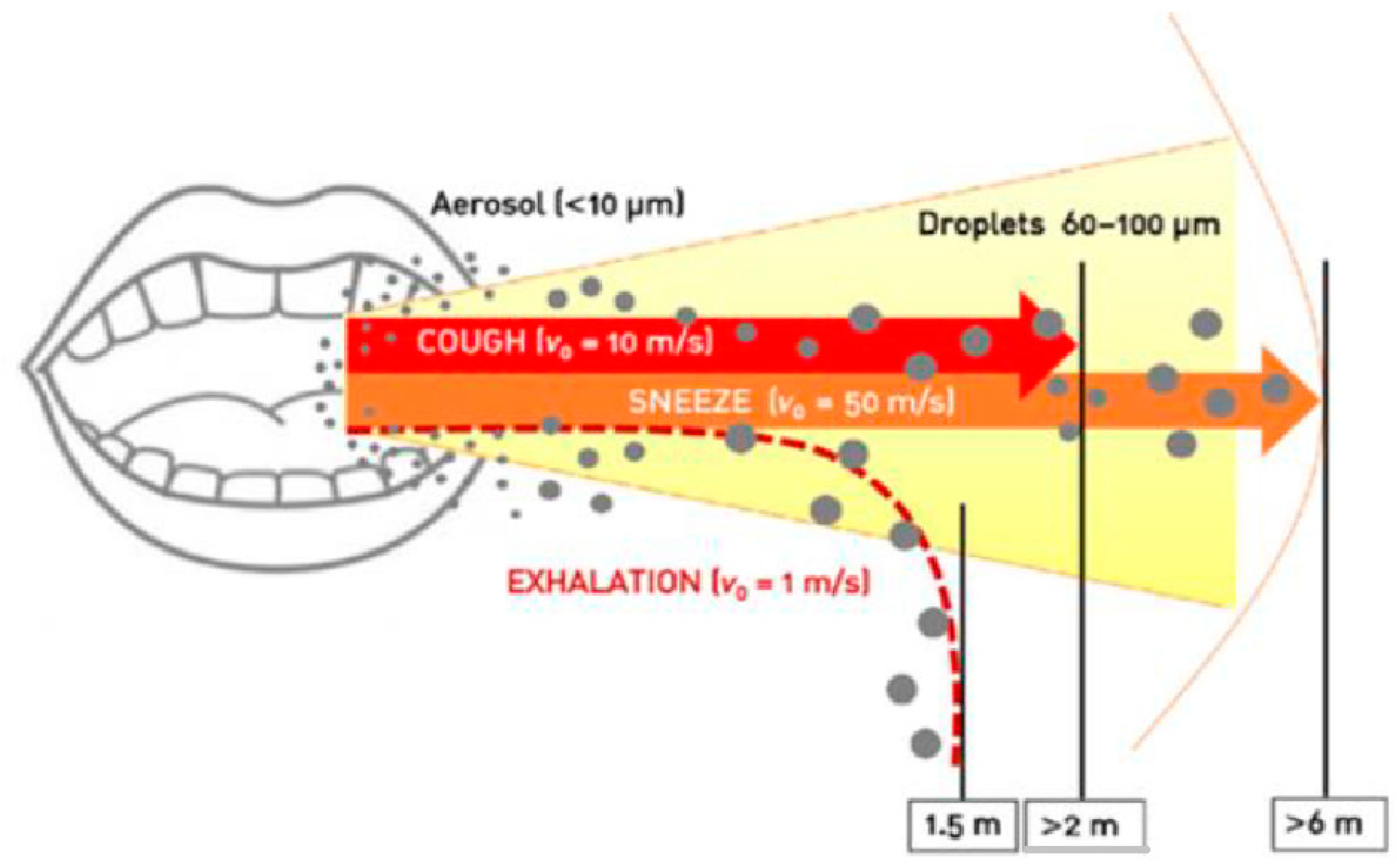
4. Transmission
5. Diagnosis and Diagnostic Methods
- Nasopharyngeal swab.
- Oropharyngeal swab.
- Blood sampling for antibody detection (immunization).
- Expectorated sputum in severe respiratory disease [36].
5.1. Saliva as a Diagnostic Tool
5.2. Gingival Crevicular Fluid
6. SARS-COV-2 Incubation Period in Humans
7. Management of COVID-19
- (1)
- Healthcare professionals and inhabitants of long-term care facilities.
- (2)
- Essential workers (such as transportation, food service, finance, and health) and individuals aged 75 years or older.
- (3)
- Individuals aged 65 to 74 years; individuals aged 16 to 64 years with systemic conditions.
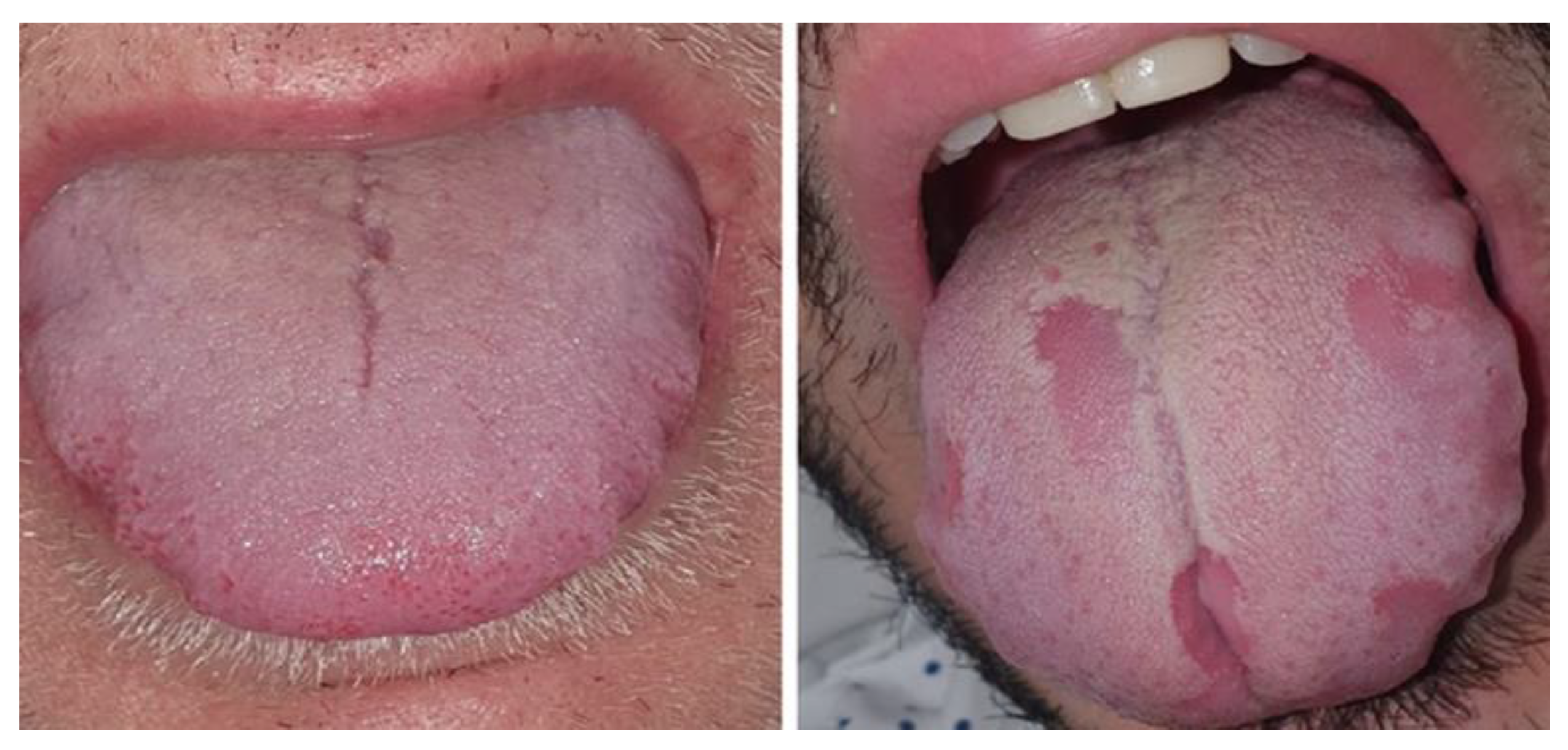
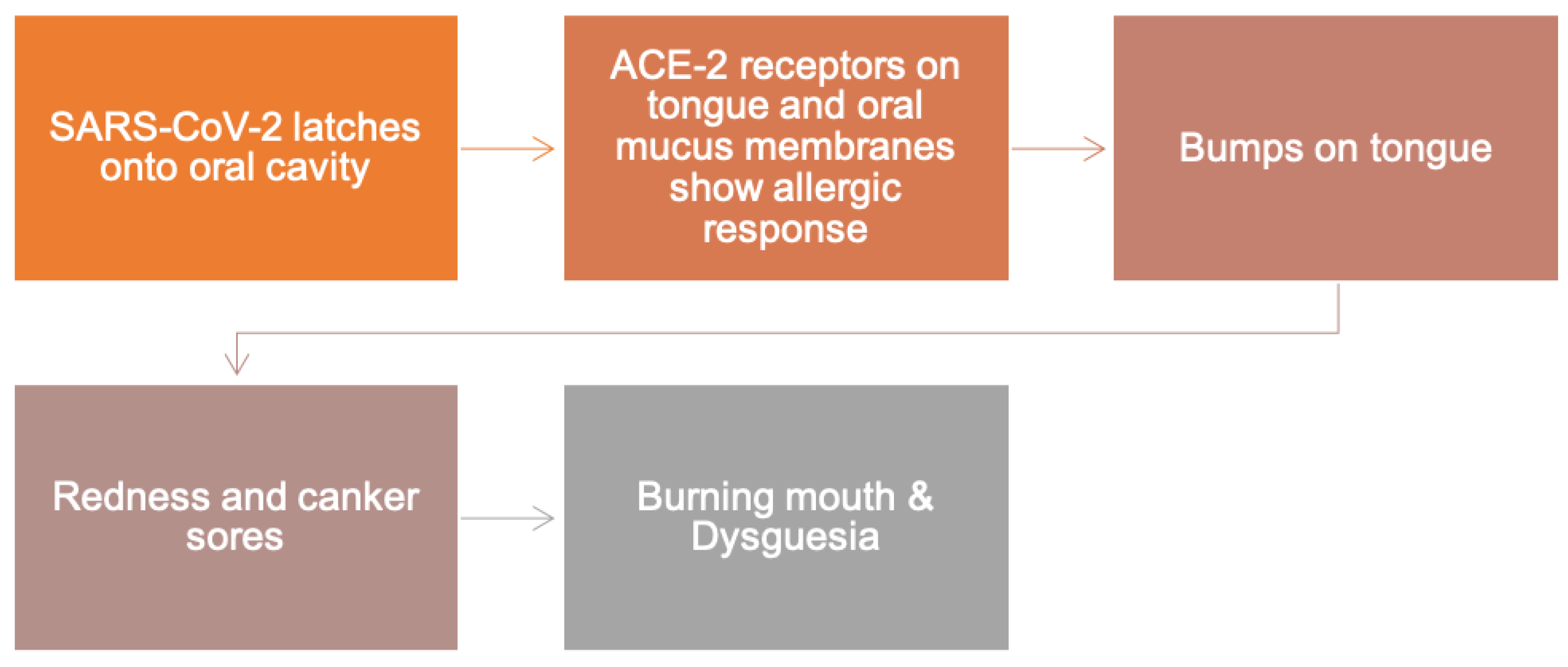
8. Oral Manifestations of COVID-19 Infection
8.1. The Role of ACE-2 in Oral Manifestations of COVID-19
8.2. Dentistry Hazards
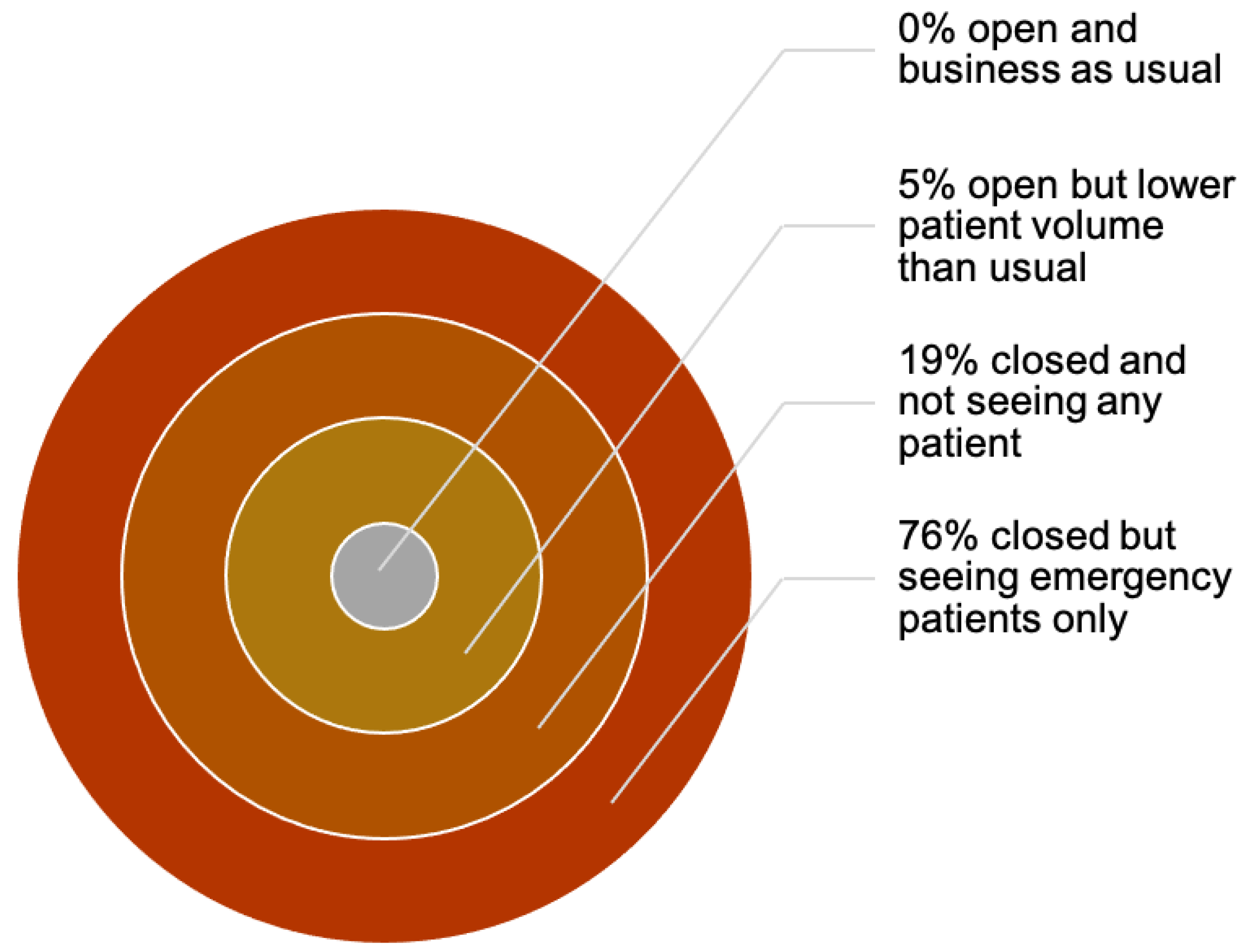
9. Economic and Emotional Impact on Dentists and Dental Practices
10. Categorization of Dental Procedures according to COVID-19 Guidelines
- Wash hands with alcohol-based soap solution for 20 s.
- Wear masks when outside.
- Avoid touching face.
- Stay 6 feet apart from each other.
- Cover your face while coughing or sneezing.
- Disinfect the surfaces used repeatedly (doorknobs, tables, and mobile phones).
- Avoid crowded areas.
- Isolate yourself if sick or at greater risk.
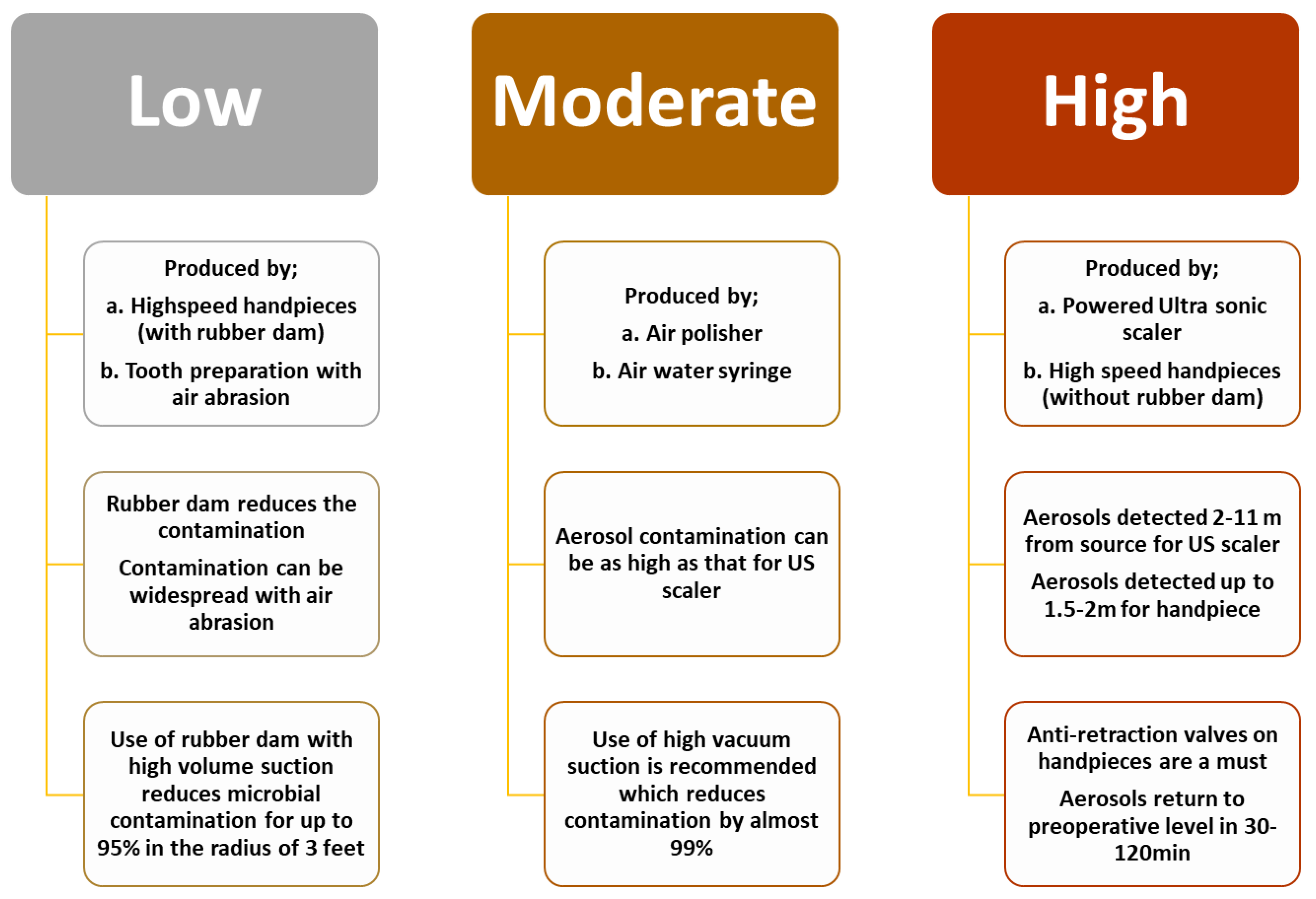
11. Aerosol Generating Procedures
- Risks associated with different modes of transmission (i.e., droplets, aerosols, and fomites).
- The sources, nature, kinetics, and the quantity of microbial load in such aerosols.
- The efficacy of current and emerging practices in mitigating aerosol-generated microbial load.
- Cataloguing of suspicious or high-risk patients (history of fever, respiratory problems, travel history, and contact with a COVID-19 patient during the past 14 days) [143].
- Repetition of triage [144].
- Accommodation of patient in an isolated ward or room [144].
- Scalpel use over monopolar cautery for skin/mucosal incision.
- Avoid intra-oral incision, repeated suctioning, and irrigation.
- Elective surgery must be delayed for non-critical cancer patients unless it does not affect the prognosis.
- Substitution of power saw by a low-speed drill or osteotome.
- Application of a low power bipolar cautery for haemostasis.
12. Association of Rhino-Cerebral Fungal Infections with COVID-19
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Hamid, H.; Khurshid, Z.; Adanir, N.; Zafar, M.S.; Zohaib, S. COVID-19 pandemic and role of human saliva as a testing biofluid in point-of-care technology. Eur. J. Dent. 2020, 14 (Suppl. 1), S123–S129. [Google Scholar] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Chin, A.W.; Poon, L.L. Stability of SARS-CoV-2 in different environmental conditions—Authors’ reply. Lancet Microbe 2020, 1, e146. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, D.; Yang, P.; Poon, L.L.; Wang, Q. Viral load of SARS-CoV-2 in clinical samples. Lancet Infect. Dis. 2020, 20, 411–412. [Google Scholar] [CrossRef]
- Saqlain, M.; Munir, M.M.; Rehman, S.U.; Gulzar, A.; Naz, S.; Ahmed, Z.; Tahir, A.H.; Mashhood, M. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: A cross-sectional survey from Pakistan. J. Hosp. Infect. 2020, 105, 419–423. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- He, S.; Han, J.; Lichtfouse, E. Backward transmission of COVID-19 from humans to animals may propagate reinfections and induce vaccine failure. Environ. Chem. Lett. 2021, 19, 763–768. [Google Scholar] [CrossRef]
- Oreshkova, N.; Molenaar, R.J.; Vreman, S.; Harders, F.; Munnink, B.B.O.; Hakze-van Der Honing, R.W.; Gerhards, N.; Tolsma, P.; Bouwstra, R.; Sikkema, R.S. SARS-CoV-2 infection in farmed minks, the Netherlands, April and May 2020. Euro Surveill. 2020, 25, 2001005. [Google Scholar] [CrossRef]
- Sit, T.H.; Brackman, C.J.; Ip, S.M.; Tam, K.W.; Law, P.Y.; To, E.M.; Veronica, Y.; Sims, L.D.; Tsang, D.N.; Chu, D.K. Infection of dogs with SARS-CoV-2. Nature 2020, 586, 776–778. [Google Scholar] [CrossRef]
- Tyrrell, D.A.J.; Fielder, M. Cold Wars: The Fight against the Common Cold; Oxford University Press: New York, NY, USA, 2002. [Google Scholar]
- Rota, P.A.; Oberste, M.S.; Monroe, S.S.; Nix, W.A.; Campagnoli, R.; Icenogle, J.P.; Penaranda, S.; Bankamp, B.; Maher, K.; Chen, M.-H. Characterization of a novel coronavirus associated with severe acute respiratory syndrome. Science 2003, 300, 1394–1399. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- De Groot, R.J.; Baker, S.C.; Baric, R.S.; Brown, C.S.; Drosten, C.; Enjuanes, L.; Fouchier, R.A.; Galiano, M.; Gorbalenya, A.E.; Memish, Z.A. Commentary: Middle east respiratory syndrome coronavirus (mers-cov): Announcement of the coronavirus study group. J. Virol. 2013, 87, 7790–7792. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.; Zhao, X.; Ma, X.; Wang, W.; Niu, P.; Xu, W. A novel coronavirus genome identified in a cluster of pneumonia cases—Wuhan, China 2019–2020. China CDC Wkly. 2020, 2, 61–62. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Pandit, P.; McArthur, A.G.; Banerjee, A.; Mossman, K. Evolutionary trajectory of SARS-CoV-2 and emerging variants. Virol. J. 2021, 18, 166. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Hutchinson, D.; Stone, H. Watching Brief: The evolution and impact of COVID-19 variants B. 1.1. 7, B. 1.351, P. 1 and B. 1.617. Glob. Biosecur. 2021, 3. [Google Scholar] [CrossRef]
- Graham, R.L.; Baric, R.S. Recombination, reservoirs, and the modular spike: Mechanisms of coronavirus cross-species transmission. J. Virol. 2010, 84, 3134–3146. [Google Scholar] [CrossRef] [Green Version]
- Khade, S.M.; Yabaji, S.M.; Srivastava, J. An update on COVID-19: SARS-CoV-2 life cycle, immunopathology, and BCG vaccination. Prep. Biochem. Biotechnol. 2021, 51, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and taste dysfunction in patients with COVID-19: A systematic review and meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Aragão, M.d.F.V.V.; Leal, M.; Cartaxo Filho, O.; Fonseca, T.; Valença, M. Anosmia in COVID-19 associated with injury to the olfactory bulbs evident on MRI. Am. J. Neuroradiol. 2020, 41, 1703–1706. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Wang, M.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; Li, Y.; Jin, H. Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: A retrospective case series study. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.-M.; Fu, J.-F.; Shu, Q.; Chen, Y.-H.; Hua, C.-Z.; Li, F.-B.; Lin, R.; Tang, L.-F.; Wang, T.-L.; Wang, W. Diagnosis and treatment recommendations for pediatric respiratory infection caused by the 2019 novel coronavirus. World J. Clin. Pediatr. 2020, 16, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. J. Am. Dent. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Hierholzer, J.C.; Tannock, G.A. Coronaviridae: The coronaviruses. In Laboratory Diagnosis of Infectious Diseases Principles and Practice; Springer: New York, NY, USA, 1988; pp. 451–483. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Franki, R. Comorbidities the Rule in New York’s COVID-19 Deaths. Available online: https://www.mdedge.com/chestphysician/article/220457/coronavirus-updates/comorbidities-rule-new-yorks-covid-19-deaths (accessed on 1 May 2021).
- Xie, X.; Li, Y.; Sun, H.; Liu, L. Exhaled droplets due to talking and coughing. J. R. Soc. Interface 2009, 6, S703–S714. [Google Scholar] [CrossRef] [Green Version]
- Checchi, V.; Bellini, P.; Bencivenni, D.; Consolo, U. COVID-19 dentistry-related aspects: A literature overview. Int. Dent. J. 2021, 71, 21–26. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.-W.; Tsang, O.T.-Y.; Yip, C.C.-Y.; Chan, K.-H.; Wu, T.-C.; Chan, J.M.-C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H. Consistent detection of 2019 novel coronavirus in saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Novel Coronavirus—China (Emergencies Preparedness, Response). Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 1 May 2021).
- Habibzadeh, P.; Mofatteh, M.; Silawi, M.; Ghavami, S.; Faghihi, M.A. Molecular diagnostic assays for COVID-19: An overview. Crit. Rev. Clin. Lab. Sci. 2021, 58, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Kubina, R.; Dziedzic, A. Molecular and serological tests for COVID-19 a comparative review of SARS-CoV-2 coronavirus laboratory and point-of-care diagnostics. Diagnostics 2020, 10, 434. [Google Scholar] [CrossRef]
- Yang, L.; Tu, L. Implications of gastrointestinal manifestations of COVID-19. Lancet Gastroenterol. Hepatol. 2020, 5, 629–630. [Google Scholar] [CrossRef]
- Silva-Boghossian, C.M.; Colombo, A.P.V.; Tanaka, M.; Rayo, C.; Xiao, Y.; Siqueira, W.L. Quantitative proteomic analysis of gingival crevicular fluid in different periodontal conditions. PLoS ONE 2013, 8, e75898. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Wei, Q.; Alvarez, X.; Wang, H.; Du, Y.; Zhu, H.; Jiang, H.; Zhou, J.; Lam, P.; Zhang, L. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in the upper respiratory tracts of rhesus macaques. J. Virol. 2011, 85, 4025–4030. [Google Scholar] [CrossRef] [Green Version]
- Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human saliva collection devices for proteomics: An update. Int. J. Mol. Sci. 2016, 17, 846. [Google Scholar] [CrossRef] [Green Version]
- Khurshid, Z.; Zafar, M.; Khan, E.; Mali, M.; Latif, M. Human saliva can be a diagnostic tool for Zika virus detection. J. Infect. Public Health 2019, 12, 601–604. [Google Scholar] [CrossRef]
- Abdul Rehman, S.; Khurshid, Z.; Hussain Niazi, F.; Naseem, M.; Al Waddani, H.; Sahibzada, H.A.; Sannam Khan, R. Role of salivary biomarkers in detection of cardiovascular diseases (CVD). Proteomes 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Sahibzada, H.A.; Khurshid, Z.; Khan, R.S.; Naseem, M.; Siddique, K.M.; Mali, M.; Zafar, M.S. Salivary IL-8, IL-6 and TNF-α as potential diagnostic biomarkers for oral cancer. Diagnostics 2017, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurshid, Z.; Zafar, M.S.; Khan, R.S.; Najeeb, S.; Slowey, P.D.; Rehman, I.U. Role of salivary biomarkers in oral cancer detection. Adv. Clin. Chem. 2018, 86, 23–70. [Google Scholar]
- Khurshid, Z.; Moin, S.F.; Khan, R.S.; Agwan, M.A.S.; Alwadaani, A.H.; Zafar, M.S. Human salivary protein extraction from RNAPro· SAL™, Pure· SAL™, and passive drooling method. Eur. J. Dent. 2017, 11, 385–389. [Google Scholar] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.V.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y. Detection of 2019-nCoV in saliva and characterization of oral symptoms in COVID-19 patients. Cell Prolif. 2020, 53, e12923. [Google Scholar] [PubMed]
- Shaikh, M.S.; Lone, M.A.; Kabir, R.; Apu, E.H. Periodontal connections to the coronavirus disease 2019: An unexplored novel path? Adv. Hum. Biol. 2020, 10, 197–198. [Google Scholar]
- Lin, P.-H.; Yeh, S.-K.; Huang, W.-C.; Chen, H.-Y.; Chen, C.-H.; Sheu, J.-R.; Lin, C.-T.; Huang, Y.-K. Research performance of biomarkers from biofluids in periodontal disease publications. J. Dent. Sci. 2015, 10, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Grenier, G.; Gagnon, G.; Grenier, D. Detection of herpetic viruses in gingival crevicular fluid of patients suffering from periodontal diseases: Prevalence and effect of treatment. Oral Microbiol. Immunol. 2009, 24, 506–509. [Google Scholar] [CrossRef]
- Majeed, Z.N.; Philip, K.; Alabsi, A.; Pushparajan, S.; Swaminathan, D. Identification of gingival crevicular fluid sampling, analytical methods, and oral biomarkers for the diagnosis and monitoring of periodontal diseases: A systematic review. Dis. Markers 2016, 2016, 1804727. [Google Scholar] [CrossRef] [Green Version]
- Zimmer, C.; Corum, J.; Wee, S. Coronavirus Vaccine Tracker. Available online: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html (accessed on 1 May 2021).
- Sheahan, T.P.; Sims, A.C.; Zhou, S.; Graham, R.L.; Pruijssers, A.J.; Agostini, M.L.; Leist, S.R.; Schäfer, A.; Dinnon, K.H.; Stevens, L.J. An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Sci. Transl. Med. 2020, 12, eabb5883. [Google Scholar] [CrossRef] [Green Version]
- Agostini, M.L.; Pruijssers, A.J.; Chappell, J.D.; Gribble, J.; Lu, X.; Andres, E.L.; Bluemling, G.R.; Lockwood, M.A.; Sheahan, T.P.; Sims, A.C. Small-molecule antiviral β-d-N4-hydroxycytidine inhibits a proofreading-intact coronavirus with a high genetic barrier to resistance. J. Virol. 2019, 93, e01348-19. [Google Scholar] [CrossRef] [Green Version]
- Bakadia, B.M.; He, F.; Souho, T.; Lamboni, L.; Ullah, M.W.; Boni, B.O.; Ahmed, A.A.Q.; Mukole, B.M.; Yang, G. Prevention and treatment of COVID-19: Focus on interferons, chloroquine/hydroxychloroquine, azithromycin, and vaccine. Biomed. Pharmacother. 2020, 133, 111008. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, G. The role of type I interferons in the pathogenesis and treatment of COVID-19. Front. Immunol. 2020, 11, 595739. [Google Scholar] [CrossRef] [PubMed]
- Abdolvahab, M.H.; Moradi-Kalbolandi, S.; Zarei, M.; Bose, D.; Majidzadeh-A, K.; Farahmand, L. Potential role of interferons in treating COVID-19 patients. Int. Immunopharmacol. 2021, 90, 107171. [Google Scholar] [CrossRef] [PubMed]
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; De-Antonio Cuscó, M.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti-Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef] [PubMed]
- Bleyzac, N.; Goutelle, S.; Bourguignon, L.; Tod, M. Azithromycin for COVID-19: More than just an antimicrobial? Clin. Drug Investig. 2020, 40, 683–686. [Google Scholar] [CrossRef]
- Wei, Q.; Lin, H.; Wei, R.-G.; Chen, N.; He, F.; Zou, D.-H.; Wei, J.-R. Tocilizumab treatment for COVID-19 patients: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 71. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Kashour, Z.; Damlaj, M.; Riaz, M.; Tlayjeh, H.; Altannir, M.; Altannir, Y.; Al-Tannir, M.; Tleyjeh, R.; Hassett, L. Efficacy and safety of tocilizumab in COVID-19 patients: A living systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 27, 215–227. [Google Scholar] [CrossRef]
- Campochiaro, C.; Della-Torre, E.; Cavalli, G.; De Luca, G.; Ripa, M.; Boffini, N.; Tomelleri, A.; Baldissera, E.; Rovere-Querini, P.; Ruggeri, A. Efficacy and safety of tocilizumab in severe COVID-19 patients: A single-centre retrospective cohort study. Eur. J. Intern. Med. 2020, 76, 43–49. [Google Scholar] [CrossRef]
- Chatterjee, K.; Wu, C.-P.; Bhardwaj, A.; Siuba, M. Steroids in COVID-19: An overview. Cleve. Clin. J. Med. 2020, 87, 715. [Google Scholar] [CrossRef]
- Waterer, G.W.; Rello, J. Steroids and COVID-19: We need a precision approach, not one size fits all. Infect. Dis. Ther. 2020, 9, 701–705. [Google Scholar] [CrossRef]
- Halpin, D.M.; Singh, D.; Hadfield, R.M. Inhaled corticosteroids and COVID-19: A systematic review and clinical perspective. Eur. Respir. J. 2020, 55, 2001009. [Google Scholar] [CrossRef]
- Madsen, L.W. Remdesivir for the Treatment of Covid-19-Final Report. N. Engl. J. Med. 2020, 338, 1813–1826. [Google Scholar]
- Nichols, B.E.; Jamieson, L.; Zhang, S.R.; Rao, G.A.; Silal, S.; Pulliam, J.R.; Sanne, I.; Meyer-Rath, G. The Role of Remdesivir in South Africa: Preventing COVID-19 Deaths Through Increasing Intensive Care Unit Capacity. Clin. Infect. Dis. 2021, 72, 1642–1644. [Google Scholar] [CrossRef] [PubMed]
- Belete, T.M. Review on up-to-date status of candidate vaccines for COVID-19 disease. Infect. Drug Resist. 2021, 14, 151–161. [Google Scholar] [CrossRef] [PubMed]
- CDC. How CDC Is Making COVID-19 Vaccine Recommendations. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-process.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fvaccines%2Frecommendations.html (accessed on 1 May 2021).
- Malik, J.A.; Mulla, A.H.; Farooqi, T.; Pottoo, F.H.; Anwar, S.; Rengasamy, K.R. Targets and strategies for vaccine development against SARS-CoV-2. Biomed. Pharmacother. 2021, 137, 111254. [Google Scholar] [CrossRef] [PubMed]
- Nag, K.; Baray, J.C.; Khan, M.R.; Mahmud, A.; Islam, J.; Myti, S.; Ali, R.; Sarker, E.H.; Kumar, S.; Chowdhury, M.H. An mRNA-based vaccine candidate against SARS-CoV-2 elicits stable immuno-response with single dose. Vaccine 2021, 39, 3745–3755. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K. Immunogenicity of the Ad26. COV2. S Vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase ½ clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Liu, Z.; Xu, W.; Xia, S.; Gu, C.; Wang, X.; Wang, Q.; Zhou, J.; Wu, Y.; Cai, X.; Qu, D. RBD-Fc-based COVID-19 vaccine candidate induces highly potent SARS-CoV-2 neutralizing antibody response. Signal Transduct. Target Ther. 2020, 5, 282. [Google Scholar] [CrossRef]
- NantKwest. ImmunityBio and NantKwest Announce FDA Authorization to Study hAd5 T-Cell COVID-19 Vaccine for Combination of Subcutaneous, Oral and Sublingual Boost to Induce T-Cell, Mucosal, and Antibody Immunity. Available online: https://www.businesswire.com/news/home/20210211005960/en/ImmunityBio-and-NantKwest-Announce-FDA-Authorization-to-Study-hAd5-T-Cell-COVID-19-Vaccine-for-Combination-of-Subcutaneous-Oral-and-Sublingual-Boost-to-Induce-T-Cell-Mucosal-and-Antibody-Immunity (accessed on 1 May 2021).
- ClinicalTrials.gov. Safety and Immunogenicity of AdCOVID in Healthy Adults (COVID-19 Vaccine Study). Available online: https://clinicaltrials.gov/ct2/show/NCT04679909 (accessed on 1 May 2021).
- O’Hare, R. Landmark Coronavirus Study to Trial Inhaled Imperial and Oxford Vaccines. Available online: https://www.imperial.ac.uk/news/203653/landmark-coronavirus-study-trial-inhaled-imperial/ (accessed on 1 May 2021).
- Nuno-Gonzalez, A.; Martin-Carrillo, P.; Magaletsky, K.; Martin Rios, M.; Herranz Mañas, C.; Artigas Almazan, J.; García Casasola, G.; Perez Castro, E.; Gallego Arenas, A.; Mayor Ibarguren, A. Prevalence of mucocutaneous manifestations in 666 patients with COVID-19 in a field hospital in Spain: Oral and palmoplantar findings. Br. J. Dermatol. 2020, 184, 184–185. [Google Scholar] [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef]
- Alikhani, M.; Khalighinejad, N.; Ghalaiani, P.; Khaleghi, M.A.; Askari, E.; Gorsky, M. Immunologic and psychologic parameters associated with geographic tongue. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 68–71. [Google Scholar] [CrossRef]
- Hathway, R. COVID tongue. Br. Dent. J. 2021, 230, 114. [Google Scholar] [CrossRef] [PubMed]
- Farid, H.; Khan, M.; Jamal, S.; Ghafoor, R. Oral manifestations of Covid-19-A literature review. Rev. Med. Virol. 2021, e2248. [Google Scholar] [CrossRef]
- Iranmanesh, B.; Khalili, M.; Amiri, R.; Zartab, H.; Aflatoonian, M. Oral manifestations of COVID-19 disease: A review article. Dermatol. Ther. 2021, 34, e14578. [Google Scholar] [CrossRef]
- Halepas, S.; Lee, K.C.; Myers, A.; Yoon, R.K.; Chung, W.; Peters, S.M. Oral manifestations of COVID-2019-related multisystem inflammatory syndrome in children: A review of 47 pediatric patients. J. Am. Dent. Assoc. 2021, 152, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Halboub, E.; Al-Maweri, S.A.; Alanazi, R.H.; Qaid, N.M.; Abdulrab, S. Orofacial manifestations of COVID-19: A brief review of the published literature. Braz. Oral Res. 2020, 34, e124. [Google Scholar] [CrossRef] [PubMed]
- Amorim Dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; Acevedo, A.C.; De Luca Canto, G.; Sugaya, N.; Santos-Silva, A.R.; Guerra, E.N.S. Oral Manifestations in Patients with COVID-19: A Living Systematic Review. J. Dent. Res. 2021, 100, 141–154. [Google Scholar] [CrossRef]
- Farook, F.F.; Nuzaim, M.N.M.; Ababneh, K.T.; Alshammari, A.; Alkadi, L. Covid-19 Pandemic and Challenges of Dentistry: COVID-19 Pandemic: Oral Health Challenges and Recommendations. Eur. J. Dent. 2020, 14, S165–S170. [Google Scholar] [CrossRef] [PubMed]
- Guy, J.; Lambert, D.; Warner, F.; Hooper, N.; Turner, A. Membrane-associated zinc peptidase families: Comparing ACE and ACE2. Biochim. Biophys. Acta 2005, 1751, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Zheng, S.; Chen, Y.; Zheng, M. Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCoV, in the nasal tissue. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Krüger, N.; Mueller, M.A.; Drosten, C.; Pöhlmann, S. The novel coronavirus 2019 (2019-nCoV) uses the SARS-coronavirus receptor ACE2 and the cellular protease TMPRSS2 for entry into target cells. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Martín Carreras-Presas, C.; Amaro Sánchez, J.; López-Sánchez, A.F.; Jané-Salas, E.; Somacarrera Pérez, M.L. Oral vesiculobullous lesions associated with SARS-CoV-2 infection. Oral Dis. 2020, 27 (Suppl. 3), 710–712. [Google Scholar] [CrossRef] [PubMed]
- Legnani, P.; Checchi, L.; Pelliccioni, G.; D’Achille, C. Atmospheric contamination during dental procedures. Quintessence Int. 1994, 25, 435–439. [Google Scholar]
- Veena, H.; Mahantesha, S.; Joseph, P.A.; Patil, S.R.; Patil, S.H. Dissemination of aerosol and splatter during ultrasonic scaling: A pilot study. J. Infect. Public Health 2015, 8, 260–265. [Google Scholar] [CrossRef]
- ADA. COVID-19 Economic Impacts on Dental Practices by American Dental Association. Available online: https://www.ada.org/en/science-research/health-policy-institute/covid-19-dentists-economic-impact/survey-results (accessed on 1 May 2021).
- Elkarim, I.; Abdulla, Z.; Yahia, N.; AlQudah, A.; Ibrahim, Y. Basic infection control procedures in dental practice in Khartoum—Sudan. Int. Dent. J. 2004, 54, 413–417. [Google Scholar] [CrossRef]
- Loeb, M.; Dafoe, N.; Mahony, J.; John, M.; Sarabia, A.; Glavin, V.; Webby, R.; Smieja, M.; Earn, D.J.; Chong, S. Surgical mask vs. N95 respirator for preventing influenza among health care workers: A randomized trial. J. Am. Dent. Assoc. 2009, 302, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Nagaraja, C.; Hungund, S.A. A study of different modes of disinfection and their effect on bacterial load in dental unit waterlines. Eur. J. Gen. Dent. 2013, 2, 246–251. [Google Scholar] [CrossRef]
- Sarfaraz, S.; Shabbir, J.; Mudasser, M.A.; Khurshid, Z.; Al-Quraini, A.A.A.; Abbasi, M.S.; Ratnayake, J.; Zafar, M.S. Knowledge and attitude of dental practitioners related to disinfection during the COVID-19 pandemic. Proc. Healthc. 2020, 8, 232. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Radonovich, L.J.; Simberkoff, M.S.; Bessesen, M.T.; Brown, A.C.; Cummings, D.A.; Gaydos, C.A.; Los, J.G.; Krosche, A.E.; Gibert, C.L.; Gorse, G.J. N95 respirators vs. medical masks for preventing influenza among health care personnel: A randomized clinical trial. J. Am. Dent. Assoc. 2019, 322, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Khanagar, S.B.; Alfadley, A. Psychological Impact of the COVID-19 Pandemic on Dental Interns in Riyadh, Saudi Arabia: A Cross-sectional Survey. Int. J. Clin. Pediatr. Dent. 2020, 13, 508–512. [Google Scholar]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and practice modifications among dentists to combat novel coronavirus disease (COVID-19) outbreak. Int. J. Environ. Res. Public Health. 2020, 17, 2821. [Google Scholar] [CrossRef]
- Uhlen, M.; Ansteinsson, V.; Stangvaltaite-Mouhat, L.; Korzeniewska, L.; Skudutyte-Rysstad, R.; Shabestari, M.; Mdala, I.; Hovden, E. Psychological impact of the COVID-19 pandemic on dental health personnel in Norway. BMC Health Serv. Res. 2021, 21, 420. [Google Scholar] [CrossRef] [PubMed]
- Hakami, Z.; Khanagar, S.B.; Vishwanathaiah, S.; Hakami, A.; Bokhari, A.M.; Jabali, A.H.; Alasmari, D.; Aldrees, A.M. Psychological impact of the coronavirus disease 2019 (COVID-19) pandemic on dental students: A nationwide study. J. Dent. Educ. 2021, 85, 494–503. [Google Scholar] [CrossRef]
- Ranka, M.S.; Ranka, S.R. Survey of Mental Health of Dentists in the COVID-19 Pandemic in the UK. J. Int. Soc. Prev. Community Dent. 2021, 11, 104–108. [Google Scholar]
- Ahmadi, H.; Ebrahimi, A.; Ghorbani, F. The impact of COVID-19 pandemic on dental practice in Iran: A questionnaire-based report. BMC Oral Health 2020, 20, 354. [Google Scholar] [CrossRef] [PubMed]
- Kamran, R.; Saba, K.; Azam, S. Impact of COVID-19 on Pakistani dentists: A nationwide cross sectional study. BMC Oral Health 2021, 21, 59. [Google Scholar] [CrossRef]
- Niazi, M.I.K.; Ghafoor, S. Teledentistry and COVID-19: Today and Tomorrow. Biomedica 2020, 36, 81–83. [Google Scholar] [CrossRef]
- Chopra, S.S.; Sahoo, N.K. Protocol for teledentistry during COVID-19 in Armed Forces dental establishments. Med. J. Armed Forces India 2020, 76, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.A.; Ali, B.; Aslam, K.; Hasan, A.; Ali, A.; Charania, A.; Phil, B. Dental Care During COVID-19 Pandemic: Guidelines for Teaching Hospital OPDs. J. Pak. Dent. Assoc. 2020, 29, S43–S52. [Google Scholar] [CrossRef]
- Izzetti, R.; Nisi, M.; Gabriele, M.; Graziani, F. COVID-19 transmission in dental practice: Brief review of preventive measures in Italy. J. Dent. Res. 2020, 99, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Razmara, F.; Khayamzadeh, M.; Shabankare, G. Dental practice in the era of COVID-19: A review of literature. J. Fam. Med. Prim. Care 2021, 10, 41–47. [Google Scholar]
- Bhanushali, P.; Katge, F.; Deshpande, S.; Chimata, V.K.; Shetty, S.; Pradhan, D. COVID-19: Changing trends and its impact on future of dentistry. Int. J. Dent. 2020, 2020, 8817424. [Google Scholar] [CrossRef] [PubMed]
- Peditto, M.; Scapellato, S.; Marcianò, A.; Costa, P.; Oteri, G. Dentistry during the COVID-19 epidemic: An Italian workflow for the management of dental practice. Int. J. Environ. Res. Public Health 2020, 17, 3325. [Google Scholar] [CrossRef] [PubMed]
- Parihar, A.V.; Sahoo, R.; Parihar, S. Dental practice in Covid times—An overview. Indian J. Prev. Soc. Med. 2020, 51, 48–60. [Google Scholar]
- Patel, M. Infection control in dentistry during COVID–19 pandemic: What has changed? Heliyon 2020, 6, e05402. [Google Scholar] [CrossRef]
- Villani, F.A.; Aiuto, R.; Paglia, L.; Re, D. COVID-19 and dentistry: Prevention in dental practice, a literature review. Int. J. Environ. Res. 2020, 17, 4609. [Google Scholar] [CrossRef]
- Shi, A.H.; Guo, W.; Chng, C.K.; Chan, B.H. Precautions when providing dental care during Coronavirus Disease 2019 (COVID-19) pandemic. Ann. Acad. Med. Singap. 2020, 49, 312–319. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Parhar, H.S.; Tasche, K.; Brody, R.M.; Weinstein, G.S.; O’Malley, B.W., Jr.; Shanti, R.M.; Newman, J.G. Topical preparations to reduce SARS-CoV-2 aerosolization in head and neck mucosal surgery. Head Neck 2020, 42, 1268–1272. [Google Scholar] [CrossRef]
- Kirk-Bayley, J.; Sunkaraneni, S.; Challacombe, S. The Use of Povidone Iodine Nasal Spray and Mouthwash During the Current COVID-19 Pandemic May Reduce Cross Infection and Protect Healthcare Workers. SSRN 2020. Available online: https://ssrn.com/abstract=3563092 (accessed on 1 May 2021). [CrossRef]
- Hui, D.S. Epidemic and emerging coronaviruses (severe acute respiratory syndrome and Middle East respiratory syndrome). Clin. Chest Med. 2017, 38, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. Potential role of inanimate surfaces for the spread of coronaviruses and their inactivation with disinfectant agents. J. Infect. Prev. 2020, 2, 100044. [Google Scholar] [CrossRef] [PubMed]
- ADA Develops Guidance on Dental Emergency, Nonemergency Care: Recommendations Part of Dentists’ Response over COVID-19 Concerns. Available online: https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-develops-guidance-on-dental-emergency-nonemergency-care (accessed on 1 May 2021).
- Malik, Y.S.; Kumar, N.; Sircar, S.; Kaushik, R.; Bhat, S.; Dhama, K.; Gupta, P.; Goyal, K.; Singh, M.P.; Ghoshal, U. Coronavirus disease pandemic (COVID-19): Challenges and a global perspective. Pathogens 2020, 9, 519. [Google Scholar] [CrossRef]
- TFSS. Practitioners specialized in oral health and coronavirus disease 2019: Professional guidelines from the French society of stomatology, maxillofacial surgery and oral surgery, to form a common front against the infectious risk. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Li, T. Interpretation of “Guidelines for the diagnosis and treatment of novel coronavirus (2019-nCoV) infection by the national health commission (Trial version 5)”. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 100, E001. [Google Scholar]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- RCSLT. The Royal College of Speech and Language Therapists Guidance on Reducing the Risk of Transmission and Use of Personal Protective Equipment (PPE) in the Context of COVID-19. Available online: https://www.rcslt.org/wp-content/uploads/2020/11/RCSLT-guidance-on-reducing-risk-of-transmission-PPE_Jan-2021-update.pdf (accessed on 1 May 2021).
- Speech Pathology Australia Guidance for Service Delivery, clinical procedures and infection control during COVID-19 pandemic. Aerosol Generating Procedures and Exposure to Aerosols. Available online: https://www.speechpathologyaustralia.org.au/SPAweb/About_us/COVID-19_News_and_Information/COVID-19_-_Guidance_for_Service_Delivery/SPAweb/About_Us/COVID-19/Guidance_for_Service_Delivery.aspx?hkey=fc19a880-e7a8-4246-8631-a474fc43d4ae (accessed on 1 May 2021).
- El-Boghdadly, K.; Wong, D.; Owen, R.; Neuman, M.; Pocock, S.; Carlisle, J.; Johnstone, C.; Andruszkiewicz, P.; Baker, P.; Biccard, B. Risks to healthcare workers following tracheal intubation of patients with COVID-19: A prospective international multicentre cohort study. Anaesthesia 2020, 75, 1437–1447. [Google Scholar] [CrossRef]
- Jackson, T.; Deibert, D.; Wyatt, G.; Durand-Moreau, Q.; Adisesh, A.; Khunti, K.; Khunti, S.; Smith, S.; Chan, X.H.S.; Ross, L. Classification of aerosol-generating procedures: A rapid systematic review. BMJ Open Respir. Res. 2020, 7, e000730. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.; Cimon, K.; Severn, M.; Pessoa-Silva, C.L.; Conly, J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: A systematic review. PLoS ONE 2012, 7, e35797. [Google Scholar] [CrossRef] [Green Version]
- Geisinger, M. Into the Unknown: Emerging Evidence Regarding Risks of Aerosols in the Dental Office. Available online: https://orthopracticeus.com/into-the-unknown-emerging-evidence-regarding-risks-of-aerosols-in-the-dental-office/ (accessed on 1 May 2021).
- Knibbs, L.D.; Johnson, G.R.; Kidd, T.J.; Cheney, J.; Grimwood, K.; Kattenbelt, J.A.; O’Rourke, P.K.; Ramsay, K.A.; Sly, P.D.; Wainwright, C.E. Viability of Pseudomonas aeruginosa in cough aerosols generated by persons with cystic fibrosis. Thorax 2014, 69, 740–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrel, S.K.; Molinari, J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J. Am. Dent. Assoc. 2004, 135, 429–437. [Google Scholar] [CrossRef]
- Hatagishi, E.; Okamoto, M.; Ohmiya, S.; Yano, H.; Hori, T.; Saito, W.; Miki, H.; Suzuki, Y.; Saito, R.; Yamamoto, T. Establishment and clinical applications of a portable system for capturing influenza viruses released through coughing. PLoS ONE 2014, 9, e103560. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Grantham, M.; Pantelic, J.; De Mesquita, P.J.B.; Albert, B.; Liu, F.; Ehrman, S.; Milton, D.K.; Consortium, E. Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Proc. Natl. Acad. Sci. USA 2018, 115, 1081–1086. [Google Scholar] [CrossRef] [Green Version]
- Wood, M.E.; Stockwell, R.E.; Johnson, G.R.; Ramsay, K.A.; Sherrard, L.J.; Jabbour, N.; Ballard, E.; O’Rourke, P.; Kidd, T.J.; Wainwright, C.E. Face masks and cough etiquette reduce the cough aerosol concentration of Pseudomonas aeruginosa in people with cystic fibrosis. Am. J. Respir. Crit. Care Med. 2018, 197, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Micik, R.E.; Miller, R.L.; Mazzarella, M.A.; Ryge, G. Studies on dental aerobiology: I. Bacterial aerosols generated during dental procedures. J. Dent. Res. 1969, 48, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Co, B.; Lu, J.; Yang, Y.; Ding, M.; Ma, J.; Chen, Y.; Li, Q.; Tian, L. Clinical analysis of 25 oral and maxillofacial emergency patients during the period of COVID-19 epidemic. Chin. J. Oral Maxillofac. Surg. 2020, 18, 105. [Google Scholar]
- Barca, I.; Cordaro, R.; Kallaverja, E.; Ferragina, F.; Cristofaro, M.G. Management in oral and maxillofacial surgery during the COVID-19 pandemic: Our experience. Br. J. Oral Maxillofac. Surg. 2020, 58, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Soh, H.Y.; Cai, Z.G.; Peng, X.; Zhang, Y.; Guo, C.B. Experience of diagnosing and managing patients in oral maxillofacial surgery during the prevention and control period of the new coronavirus pneumonia. Chin. J. Dent. Res. 2020, 23, 57–62. [Google Scholar] [PubMed]
- National Health Service, England. Clinical Guide for Management of Patients Requiring Oral and Maxillofacial Surgery during the Coronavirus Pandemic; 2020; Available online: https://www.baoms.org.uk/_userfiles/pages/files/professionals/covid_19/specialty_guide_omfs_and_coronavirus_v1_20_march.pdf (accessed on 1 May 2021).
- Kariwa, H.; Fujii, N.; Takashima, I. Inactivation of SARS coronavirus by means of povidone-iodine, physical conditions and chemical reagents. Dermatology 2006, 212, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In vitro bactericidal and virucidal efficacy of povidone-iodine gargle/mouthwash against respiratory and oral tract pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Y.; Han, B.; Pan, J.; Zhou, H.; Zhou, Q.; Zhao, J.; Chen, S.; Zhang, W.; Hu, K. Suggestions for how to prevent coronavirus disease 2019 during oral surgeries. Chin. J. Oral Maxillofac. Surg. 2020, 18, 198–203. [Google Scholar]
- Hsieh, T.-Y.; Dedhia, R.D.; Chiao, W.; Dresner, H.; Barta, R.J.; Lyford-Pike, S.; Hamlar, D.; Stephan, S.J.; Schubert, W.; Hilger, P.A. A guide to facial trauma triage and precautions in the COVID-19 pandemic. Facial Plast. Surg. Aesthet. Med. 2020, 22, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Chinese Society of Oral and Maxillofacial Surgery. Expert proposal for the management of oral maxillofacial surgery during the epidemic period of 2019-nCoV. Chin. J. Oral Maxillofac. Surg. 2020, 18, 97–99. [Google Scholar]
- Ma, S.; Yuan, Z.; Peng, Y.; Luo, Q.; Song, H.; Xiang, F.; Tan, J.; Zhou, J.; Li, N.; Hu, G. Recommendations for the regulation of medical practices of burn treatment during the outbreak of the coronavirus disease 2019. Zhonghua Shao Shang Za Zhi 2020, 36, E004. [Google Scholar]
- Givi, B.; Schiff, B.A.; Chinn, S.B.; Clayburgh, D.; Iyer, N.G.; Jalisi, S.; Moore, M.G.; Nathan, C.-A.; Orloff, L.A.; O’Neill, J.P. Safety recommendations for evaluation and surgery of the head and neck during the COVID-19 pandemic. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 579–584. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.; Buchbinder, D.; Dodson, T.B.; Fusetti, S.; Leung, M.Y.Y.; Aniceto, G.S.; Schramm, A.; Strong, E.B.; Wolvius, E. AO CMF international task force recommendations on best practices for maxillofacial procedures during COVID-19 pandemic. Craniomaxillofac. Trauma Reconstr. 2020, 13, 151–156. [Google Scholar] [CrossRef]
- Patel, Z.M.; Fernandez-Miranda, J.; Hwang, P.H.; Nayak, J.V.; Dodd, R.; Sajjadi, H.; Jackler, R.K. Precautions for endoscopic transnasal skull base surgery during the COVID-19 pandemic. Neurosurgery 2020, 87, E66–E67. [Google Scholar] [CrossRef] [Green Version]
- Licina, A.; Silvers, A.; Stuart, R.L. Use of powered air-purifying respirator (PAPR) by healthcare workers for preventing highly infectious viral diseases—A systematic review of evidence. Syst. Rev. 2020, 9, 173. [Google Scholar] [CrossRef]
- Canelli, R.; Connor, C.W.; Gonzalez, M.; Nozari, A.; Ortega, R. Barrier enclosure during endotracheal intubation. N. Engl. J. Med. 2020, 382, 1957–1958. [Google Scholar] [CrossRef] [PubMed]
- DeSerres, J.J.; Al-Shaqsi, S.Z.; Antonyshyn, O.M.; Fialkov, J.A. Best practice guidelines for the management of acute craniomaxillofacial trauma during the COVID-19 pandemic. J. Craniofac. Surg. 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7282404/ (accessed on 1 May 2021).
- Song, G.; Liang, G.; Liu, W. Fungal co-infections associated with global COVID-19 pandemic: A clinical and diagnostic perspective from China. Mycopathologia 2020, 185, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Rabagliati, R.; Rodríguez, N.; Núñez, C.; Huete, A.; Bravo, S.; Garcia, P. COVID-19–Associated Mold Infection in Critically Ill Patients, Chile. Emerg. Infect. Dis. 2021, 27, 1454–1456. [Google Scholar] [CrossRef] [PubMed]
- Waizel-Haiat, S.; Guerrero-Paz, J.A.; Sanchez-Hurtado, L.; Calleja-Alarcon, S.; Romero-Gutierrez, L. A case of fatal rhino-orbital mucormycosis associated with new onset diabetic ketoacidosis and COVID-19. Cureus 2021, 13, e13163. [Google Scholar] [PubMed]
- Saldanha, M.; Reddy, R.; Vincent, M.J. Paranasal Mucormycosis in COVID-19 Patient. Indian J. Otolaryngol. Head Neck Surg. 2021, 22, 1–4. Available online: https://link.springer.com/article/10.1007/s12070-021-02574-0 (accessed on 1 May 2021).
- Mekonnen, Z.K.; Ashraf, D.C.; Jankowski, T.; Grob, S.R.; Vagefi, M.R.; Kersten, R.C.; Simko, J.P.; Winn, B.J. Acute invasive rhino-orbital mucormycosis in a patient with COVID-19-associated acute respiratory distress syndrome. Ophthalmic Plast. Reconstr. Surg. 2021, 37, e40–e80. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Most Common | Less Common | Most Dangerous |
|---|---|---|
| Pyrexia Fatigue Dry cough | Anosmia and ageusia [22,23] Headache [24] Sore throat Diarrhoea Conjunctivitis Skin rash Fingers and toes discoloration | Dyspnoea Chest pain/pressure Loss of movement/speech Heart attack Epilepsy [24] Blood coagulation [25] Cerebral infarction [26] Kidney failure Disseminated intravascular coagulation Acute respiratory distress syndrome and multiple organ failure because of cytokine storm |
|
| Clinical Features | Population Experiencing (%) | |
|---|---|---|
| 1 to 3 day(s) Onset of symptoms |
| 80% of patients get these mild symptoms |
| 4 to 9 days In the lungs |
| 14% of those infected experience these severe symptoms |
| 8 to 15 days In the blood |
| 5% of those infected need admissions to an intensive care unit |
| Name of Drug | Potential Role in COVID-19 | Problems/Issues/Remarks |
|---|---|---|
| β-D-N4-hydroxycytidine (NHC) [54] | Ribonucleoside analogue with broad-spectrum antiviral activity (oral route) Effective against Remdesivir-resistant virus, MERS-CoV, SARS-CoV-2, and SARS-CoV in primary HAE cell cultures Reduces virus titres in a dose-dependent manner | Coronavirus may achieve 2-fold resistance after 30 passages [55]. |
| Interferons (IFN-I and III) [56] | Produces innate immune response in human cells and stimulates IFN-stimulated genes (ISGs) through JAK/STAT pathway, affecting viral replication at all stages of its replicative cycle. Early administration can decrease the viral spread and can produce extended-lasting responses without inflammatory side effects. | Virus adapts to IFNs by turning over interferon receptors, leading to a diminished response by helper T cells and NK cells. IFNs can produce flu-like symptoms on their own [57,58]. |
| Chloroquine (CQ), Hydroxychloroquine (HCQ) [56] | Inhibits intracellular replication of viral particles. It prevents the interaction between the virus and its receptor, thus blocking its effect. Both drugs are immunomodulatory and downregulate Toll-like receptors, thus suppressing the cytokine storm. | HCQ is a less toxic derivative of CQ; hence it is favoured in the treatment of COVID-19. Both these drugs produce reactive oxygen species, which can damage host cells. |
| Azithromycin (AZM) [56,59,60] | Inhibits replication of virus in bronchial cells by decreasing the synthesis of adhesion molecules like ICAM-1. Downregulates cytokine production (IL2, 6, 8), maintains alveolar cell integrity and reduces lung fibrosis Acts synergistically with HCQ in reducing viral load It also prevents bacterial co-infection by Prevotella, which can enhance the pathogenicity of SARS-CoV-2 by internalizing it. | It can cause gastrointestinal upset, nausea, headache, hepatotoxicity, and bacterial resistance. It can prolong QTc interval, ventricular tachycardia, and sudden cardiac arrest by causing intracellular sodium overdose. |
| Tocilizumab [61,62] | Recombinant humanized anti-IL-6 receptor monoclonal antibody, which is a competitive blocker of membrane-bound and soluble IL-6. Potential role in patients presenting with symptoms associated with cytokine storm. | Compochiaro et al. found no statistically significant survival benefit with a slightly increased propensity towards the development of fungal infections; however, it may reduce the need for ventilatory support in hospitalized COVID-19 patients [63]. |
| Steroids [64,65,66] | Usually administered steroids include methylprednisolone (32 mg/day), dexamethasone (6 mg/day), and hydrocortisone. Dexamethasone is favoured as it causes minimal fluid retention. It may have a role in reducing the tissue injury due to cytokine storm. | Conflicting body of evidence regarding improvement in survival and decreased hospital stay. May be beneficial but should not be given to all the patients. It can lead towards the development of hyperglycaemia, hypernatremia and mucormycosis and aspergillosis. It can reduce the duration of fever but has no overall effect on the duration of hospitalization. |
| Remdesvir [67,68] | Broad-spectrum antiviral which is an inhibitor of viral RNA-dependent RNA polymerase | Conflicting data on improvement in symptoms with no significant impact on mortality, however, may offer a survival benefit if given early in mild to moderately ill COVID-19 patients. |
| Vitamins | A high dose of vitamin C can prevent cytokine storm in COVID-19 patients, which reduces lung injury and inflammatory damage. |
| Company | Type | Doses | Route | Efficacy | Storage | Approval/Development | Mechanism of Action |
|---|---|---|---|---|---|---|---|
| Pfizer–BioNTech | Nucleoside modified mRNA (BNT162a1 and BNT162b2) | 2 shots 21 days apart | I.M inj. | 95% | −70 °C | UK approved | Spike proteins and RBD fragments are introduced into the body producing the desired immune response [71]. |
| Oxford–AstraZeneca | Viral vector (genetically altered nonreplicating chimpanzee adenovirus) | 2 shots 4 to 12 weeks apart | I.M inj. | 70% | Regular fridge temperature | UK approved | Specifically deliver genes to the target cells thus providing a trigger to cytotoxic T-cells resulting in killing of infected cells [69]. |
| Moderna | Based on lipid nanoparticle-encapsulated mRNA | 2 shots 28 days apart | I.M inj. | 94.1% | −20 °C | UK approved | Encodes stable form of spike protein of SARS-CoV-2 and educates CD4+ immune cells of the body [72]. |
| Novavax (NVX-CoV2373) | Full-length S (spike) Protein-based | 2 | I.M inj. | Regular fridge temperature | Pending | Promotes migration of leukocytes into lymph nodes thus increasing T-cell, B-cell, and NK cell response [69]. | |
| Janssen (Johnson & Johnson’s) | Viral vector based using adenovirus or pox virus | 1 | I.M inj. | 66.3% | Regular fridge temperature | Pending | DNA of the adenovirus is modified which helps the body to develop humoral and T-cell based cellular immune response against COVID-19 [73]. |
| CoronaVac (Sinopharm/Sinovac) (BBIBP-CorV) | Inactivated virus vaccine | I.M inj. | 79% | Regular fridge temperature | Approved by China, Singapore, Saudi Arabia, and Pakistan | Contains virus has been inactivated through UV light/chemicals and elicits antigen-specific antibody response producing plasma cells, T-cells, and memory B-cells [74]. | |
| CanSino Bioloics (Ad5-nCoV) Convidecia | Non-replicating adenovirus based vaccine | 1 | I.M inj. | 66% to 91% | Regular fridge temperature | Approved by Hungary, China, Mexico, and Pakistan | RBD and spike proteins produce T cell response conferring immunity against virus [69]. |
| Sputnik V | Using two non-replicating adenovirus based vector (Ad26, Ad5) | 2 doses 21 days apart | Undergoing phase 3 trials | Gamaleya Institute, Moscow. | Dose 1 injects Ad26, and in dose 2 Ad5 is given. This produces an enhanced immune response [69]. | ||
| KBP-201 (NCT04473690) | Protein (RBD-based) subunit vaccine | 2 doses 21 days apart | I.M inj. | Currently undergoing phase II trials | - | Pending | RBD in the spike protein binds to ACE-2 receptor producing neutralizing monoclonal antibodies towards SARS-CoV-2 [75]. |
| Covaxin | Inactivated virus vaccine | Currently undergoing trials in India | Same as mentioned above under CoronaVac (sinopharm) | ||||
| BHPIV3/SARS-S | Live attenuated virus vaccine | 1 | I.M. Inj | Currently undergoing phase 2 animal trials | Currently undergoing trials in India and China | Induces production of SARS-CoV neutralizing serum antibodies [69]. | |
| DelNS1-SARS-CoV2-RBD | Live attenuated vaccine with deletion of NS1 influenza strain | 1 | Intra-nasal | Currently undergoing phase 2 animal trials | Modified to include SARS-CoV-2 spike protein and is considered more immunogenic than other LAVs [69]. | ||
| LUNAR-COV19 | Lipid enabled and unlocked nucleomonomer agent-modified RNA (LUNAR) | 1 | Currently undergoing phase 1 and 2 trials | Biospace, Singapore | Entry into host cells and mRNA is translated into protiein, s leading to the production of the immune response against SARS-CoV-2 [69]. |
| 1—Teledentistry and Triage Protocols |
|
| 2—Screening Zone |
|
| 3—Waiting Area |
|
| 4—Donning Zone | Clean area PPE wearing sequence including the hand disinfection:
|
| 5—Doffing Zone | Dirty area PPE removing sequence:
|
| 6—Dental Surgery Room for Aerosol Generating Procedures |
|
| 7—Procedure Infection Control |
|
| 8—Dental Surgery Disinfection |
|
| 9—Dental Surgery Ventilation |
|
| 10—Dental Equipment Maintenance | Follow the guidelines of IFU for the maintenance of dental unit water-lines, autoclave, compressors, radiography equipment, and suctions [116]. |
| Dental Non-Emergency Procedures | Dental Emergency Procedures |
|---|---|
| New/periodic oral examinations | Uncontrolled bleeding |
| Routine x-rays | Cellulitis/bacterial facial space infection |
| Routine dental cleaning as well as preventive therapies | Severe dental pain (pulpitis) |
| Extraction of asymptomatic teeth | Pericoronitis/3rd molar pain |
| Restorative dental procedures (fillings, crowning) | Dry socket |
| Recall/revisit | Tooth fracture |
| Dento-alveolar trauma | |
| Painful broken filling | |
| Adjustment of ortho-wire damaging gums | |
| Post-surgery treatment |
| 1. Tracheostomy and tracheal intubation procedures | 2. Positive-pressure mechanical ventilation and CPAP |
| 3. Bronchoscopy | 4. Intubation and extubation procedures |
| 5. Surgery, autopsy, or post-mortem procedures with high-speed devices | 6. High frequency oscillatory ventilation |
| 7. Cardiopulmonary resuscitation | 8. High-flow oxygen therapy |
| 9. Sputum induction | 10. Airway suctioning |
| 11. FEES and VFSS | 12. Nebulized or aerosol therapy |
| CPAP (Continuous positive airway pressure); FEES (Fibreoptic endoscopic evaluation of swallowing); VFSS (Video fluoroscopic swallowing study) | |
| Droplet Type | Description |
|---|---|
| Splatter droplets | Particle size ≥ 50 µm, briefly airborne, and spread by close contact (typically within 1 m) with the host. |
| Aerosols | Particle size < 50 µm, carry viable pathogens, remain airborne for prolonged period, and spread to distant surfaces. |
| Droplets > 5 µm | Remain in the upper respiratory tract. |
| Droplets ≤ 5 µm | Might be inhaled into the lower respiratory tract. |
| Droplets ≤ 1 µm | Can enter alveoli. |
| Pre-Procedure Protocols | During Procedure Protocols | Post-Procedure Protocols |
|---|---|---|
|
| |
| personal protective equipment (PPE); powered air purifying respirator (PAPR) | ||
| Urgency for operation | Emergent (require surgical intervention in ≤24 h) | Urgent (require surgical intervention for bone union) |
| Patient presentation | Compromised airway or vision, uncontrolled bleeding, or combined intracranial or upper facial fracture | Facial fracture causing functional or cosmetic deformity including displaced cranio-orbital fractures, orbital dystopia, and naso-orbito-ethmoid fractures |
| COVID-19 screening | RT-PCR or rapid COVID test | RT-PCR or rapid COVID-19 test |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butt, R.T.; Janjua, O.S.; Qureshi, S.M.; Shaikh, M.S.; Guerrero-Gironés, J.; Rodríguez-Lozano, F.J.; Zafar, M.S. Dental Healthcare Amid the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11008. https://doi.org/10.3390/ijerph182111008
Butt RT, Janjua OS, Qureshi SM, Shaikh MS, Guerrero-Gironés J, Rodríguez-Lozano FJ, Zafar MS. Dental Healthcare Amid the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(21):11008. https://doi.org/10.3390/ijerph182111008
Chicago/Turabian StyleButt, Rabia Tariq, Omer Sefvan Janjua, Sana Mehmood Qureshi, Muhammad Saad Shaikh, Julia Guerrero-Gironés, Francisco J. Rodríguez-Lozano, and Muhammad Sohail Zafar. 2021. "Dental Healthcare Amid the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 21: 11008. https://doi.org/10.3390/ijerph182111008
APA StyleButt, R. T., Janjua, O. S., Qureshi, S. M., Shaikh, M. S., Guerrero-Gironés, J., Rodríguez-Lozano, F. J., & Zafar, M. S. (2021). Dental Healthcare Amid the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(21), 11008. https://doi.org/10.3390/ijerph182111008