
How Physicians Renew Electronic Prescriptions in Primary Care: Therapeutic Decision or Technical Task?


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Context
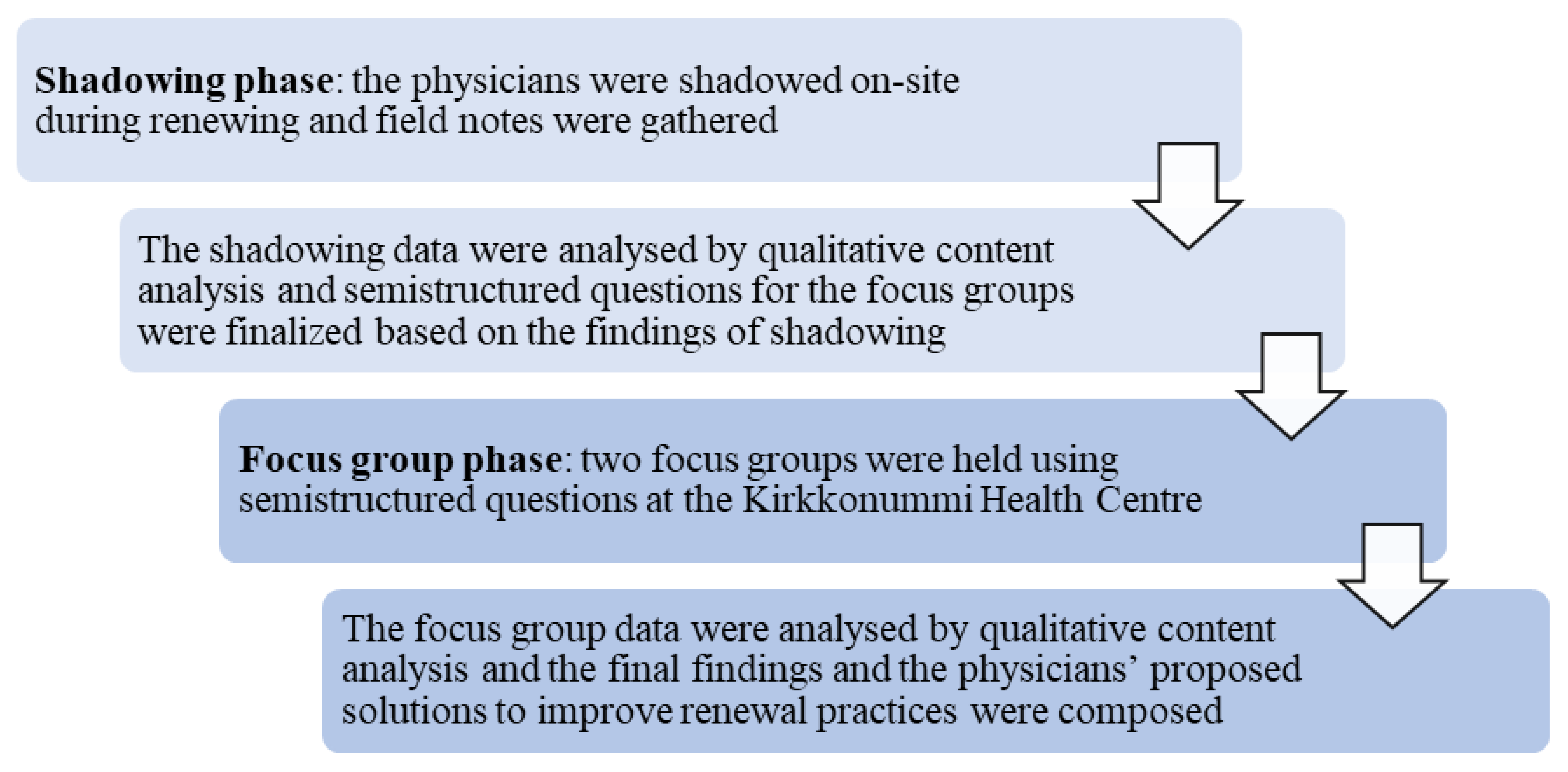
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Statement
3. Results
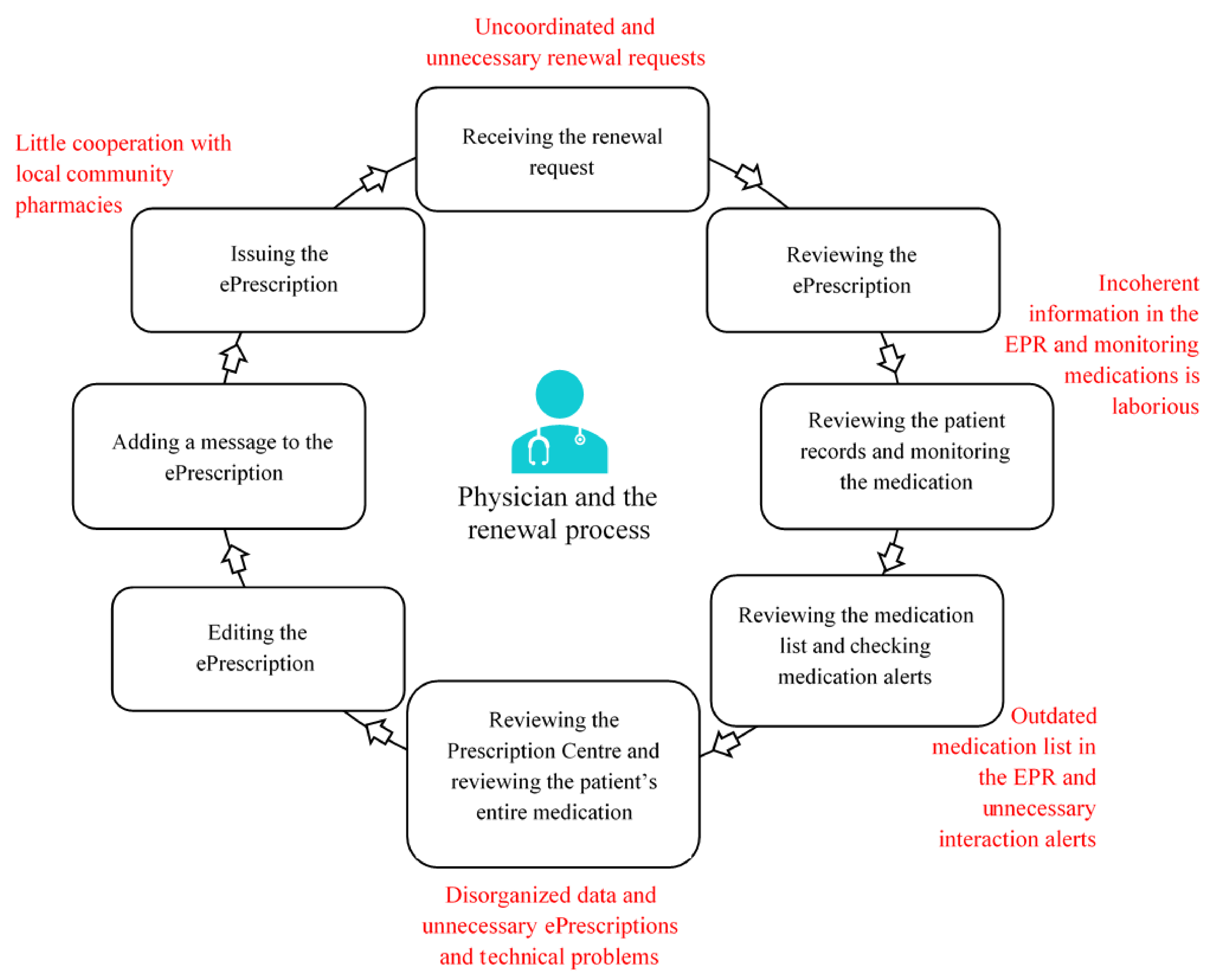
3.1. The Renewal Process
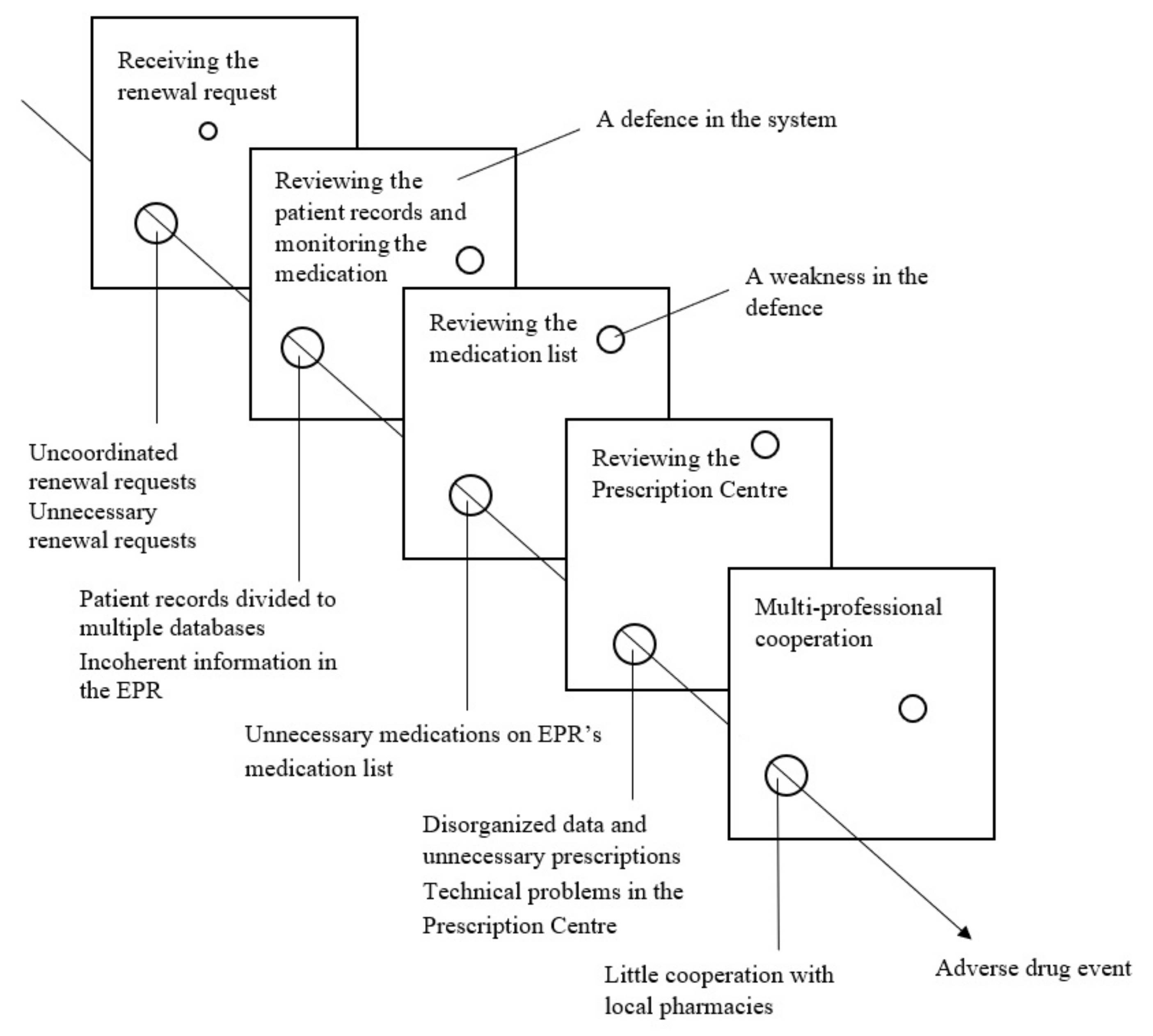
3.2. Challenges with the Renewal Process
3.2.1. Therapeutic and Communicational Challenges
3.2.2. Technical Challenges
3.3. Development Proposals to Improve the Renewal Process
4. Discussion
4.1. Main Findings
4.2. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Esmaeil Zadeh, P.; Tremblay, M.C. A review of the literature and proposed classification on e-prescribing: Functions, assimilation stages, benefits, concerns, and risks. Res. Soc. Adm. Pharm. 2016, 12, 1–19. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Schnell-Inderst, P.; Machan, C.; Siebert, U. The Effect of Electronic Prescribing on Medication Errors and Adverse Drug Events: A Systematic Review. J. Am. Med. Inform. Assoc. 2008, 15, 585–600. [Google Scholar] [CrossRef]
- Stroetmann, K.; Artmann, J.; Stroetmann, V.; Denis, P.; Jos, J.D.; Sarah, G.; Uta, W.; Diane, W. European Countries on their Journey towards National eHealth Infrastructures. eHealth Strategies Report. European Commission, 2011. Available online: www.ehealthnews.eu/images/stories/pdf/ehstrategies_final_report.pdf (accessed on 1 April 2019).
- Kiviluoto, K. Selvitys Keinoista Lääkkeenmääräämisen Järkevöittämiseksi Viidessä Esimerkkimaassa (Report on Ways to Streamline Prescribing in Five Example Countries); Ministry of Social Affairs and Health: Helsinki, Finland, 2016. (In Finnish)
- Canada Health Infoway: Annual Report 2017–2018. 2018. Available online: www.infoway-inforoute.ca/en/component/edocman/3556-annualreport-2017-2018/view-document?Itemid=0 (accessed on 1 April 2019).
- Surescripts: National Progress Report 2017. 2018. Available online: surescripts.com/docs/default-source/national-progressreports/2151_npr_2017_finalB.pdf (accessed on 1 April 2019).
- Finnish Government. Electronic Prescription Act 61/2007; Finnish Government: Helsinki, Finland, 2007. (In Finnish)
- Goldman, R.E.; Dubé, C.; Lapane, K.L. Beyond the basics: Refills by electronic prescribing. Int. J. Med. Inform. 2010, 79, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Abramson, E.L.; Patel, V.; Pfoh, E.R.; Kaushal, R. How physician perspectives on E-prescribing evolve over time: A case study following the transition between EHRs in an outpatient clinic. Appl. Clin. Inform. 2016, 7, 994–1006. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kivekäs, E.; Enlund, H.; Borycki, E.; Saranto, K. General practitioners’ attitudes towards electronic prescribing and the use of the national prescription centre. J. Eval. Clin. Pract. 2016, 22, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Kauppinen, H.; Ahonen, R.; Mäntyselkä, P.; Timonen, J. Medication safety and the usability of electronic prescribing as perceived by physicians—A semistructured interview among primary health care physicians in Finland. J. Eval. Clin. Pract. 2017, 23, 1187–1194. [Google Scholar] [CrossRef]
- Thomas, C.P.; Kim, M.; Kelleher, S.J.; Nikitin, R.V.; Kreiner, P.W.; McDonald, A.; Carrow, G.M. Early experience with electronic prescribing of controlled substances in a community setting. J. Am. Med. Inform. Assoc. 2013, 20, e44–e51. [Google Scholar] [CrossRef] [PubMed]
- Lapane, K.L.; Rosen, R.K.; Dubé, C. Perceptions of e-prescribing efficiencies and inefficiencies in ambulatory care. Int. J. Med. Inform. 2011, 80, 39–46. [Google Scholar] [CrossRef]
- Wang, C.J.; Patel, M.H.; Schueth, A.J.; Bradley, M.; Wu, S.; Crosson, J.C.; Glassman, P.A.; Bell, D.S. Perceptions of Standards-based Electronic Prescribing Systems as Implemented in Outpatient Primary Care: A Physician Survey. J. Am. Med. Inform. Assoc. 2009, 16, 493–502. [Google Scholar] [CrossRef]
- Lapane, K.L.; Waring, M.E.; Dubé, C.; Schneider, K.L. E-prescribing and patient safety: Results from a mixed method study. Am. J. Pharm. Benefits 2011, 3, e24–e34. [Google Scholar] [PubMed]
- World Health Organization. Guide to Good Prescribing. A Practical Manual; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Pattin, A.J.; Devore, N.; Fowler, J.; Weldy, D. An Examination of the Prescription Renewal Process and Implications for Primary Care Physicians and Community Pharmacists. J. Pharm. Pract. 2020, 33, 187–191. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Promoting Rational Use of Medicines: Core Components—WHO Policy Perspectives on Medicines, No. 005; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Panesar, S.S.; de Silva, D.; Carson-Stevens, A.; Cresswell, K.M.; Salvilla, S.A.; Slight, S.P.; Javad, S.; Netuveli, G.; Larizgoitia, I.; Donaldson, L.J.; et al. How safe is primary care? A systematic review. BMJ Qual. Saf. 2016, 25, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Social Affairs and Health. Vanhusten Turvallinen Lääkehoito: Kuntien Velvoitteet (Safe Pharmacotherapy for the Elderly: Obligations of the Municipalities); Kuntainfo 6/2007; Ministry of Social Affairs and Health: Helsinki, Finland, 2007. (In Finnish)
- Ministry of Social Affairs and Health. Rationaalisen Lääkehoidon Toimeenpano-Ohjelma (Rational Pharmacotherapy Action Plan); Reports and Memorandums of the Ministry of Social Affairs and Health 12/2018; Ministry of Social Affairs and Health: Helsinki, Finland, 2018; (In Finnish, summary in English).
- World Health Organization. Medication without Harm. WHO Global Patient Safety Challenge; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Adherence to Long-Term Therapies. Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Finnish Government. Decree of the Ministry of Social Affairs and Health on Prescribing 1088/2010; Finnish Government: Helsinki, Finland, 2010. (In Finnish)
- Kanta. Medical Records. Available online: https://www.kanta.fi/en/medical-records (accessed on 6 October 2021).
- The Association of Finnish Pharmacies. Annual Review 2020. 2020. Available online: https://www.apteekkariliitto.fi/media/3-apteekkariliitto.fi/liitto/vuosikatsaukset/annual_review_2020_final.pdf (accessed on 30 August 2021).
- Kanta. Renewing a Prescription. Available online: https://www.kanta.fi/en/professionals/renewing-a-prescription-healthcare-services (accessed on 13 April 2021).
- McDonald, S. Studying actions in context: A qualitative shadowing method for organizational research. Qual. Res. 2005, 5, 455–473. [Google Scholar] [CrossRef]
- Kangas, S.; Lämsä, E.; Timonen, J.; Ahonen, R. Sähköisten Reseptien Uudistamiskäytännöt—Hastattelututkimus Suomalaisen Kunnan Terveyskeskuksessa ja Apteekeissa (Electronic Prescription Renewal Procedures—An Interview Study in a Finnish Health Center and Pharmacies); Dosis, Suomen Farmasialiitto: Espoo, Finland, 2018; Volume 3, pp. 210–223, (In Finnish, summary in English). [Google Scholar]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef]
- Finnish National Board on Research Integrity TENK. The Ethical Principles of Research with Human Participants and Ethical Review in the Human Sciences in Finland. Finnish National Board on Research Integrity TENK Guidelines 2019, Finnish National Board on Research Integrity TENK Publications 3/2019. 2019. Available online: https://tenk.fi/sites/default/files/2021-01/Ethical_review_in_human_sciences_2020.pdf (accessed on 26 August 2021).
- Kallio, S.; Kumpusalo-Vauhkonen, A.; Järvensivu, T.; Mäntylä, A.; Pohjanoksa-Mäntylä, M.; Airaksinen, M. Towards interprofessional networking in medication management of the aged: Current challenges and potential solutions in Finland. Scand. J. Prim. Health Care 2016, 34, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Kvarnström, K.; Airaksinen, M.; Liira, H. Barriers and facilitators to medication adherence: A qualitative study with general practitioners. BMJ Open 2018, 8, e015332. [Google Scholar] [CrossRef] [PubMed]
- Weingart, S.N.; Massagli, M.; Cyrulik, A.; Isaac, T.; Morway, L.; Sands, D.Z.; Weissman, J.S. Assessing the value of electronic prescribing in ambulatory care: A focus group study. Int. J. Med. Inform. 2009, 78, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Social Affairs and Health. Lääkehoidon Tiedonhallinnan Kokonaisarkkitehtuurin Esiselvitys. Työryhmämuistio (Preliminary Study on the Enterprise Architecture for Pharmacotherapy Information Management. Working Group Memorandum); Reports and Memorandums of the Ministry of Social Affairs and Health 2019:58; Ministry of Social Affairs and Health: Helsinki, Finland, 2019; (In Finnish, summary in English).
- Lapane, K.L.; Waring, M.E.; Schneider, K.L.; Dubé, C.; Quilliam, B.J. A mixed method study of the merits of e-prescribing drug alerts in primary care. J. Gen. Intern. Med. 2008, 23, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Hume, A.L.; Quilliam, B.J.; Goldman, R.; Eaton, C.; Lapane, K.L. Alternatives to potentially inappropriate medications for use in e-prescribing software: Triggers and treatment algorithms. BMJ Qual. Saf. 2011, 20, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Abramson, E.L.; Patel, V.; Malhotra, S.; Pfoh, E.R.; Nena Osorio, S.; Cheriff, A.; Cole, C.L.; Bunce, A.; Ash, J.; Kaushal, R. Physician experiences transitioning between an older versus newer electronic health record for electronic prescribing. Int. J. Med. Inform. 2012, 81, 539–548. [Google Scholar] [CrossRef] [PubMed]
- The Finnish Institute for Health and Welfare. Valtakunnallinen lääkityslista (Nationwide Medication List). Available online: https://thl.fi/fi/web/tiedonhallinta-sosiaali-ja-terveysalalla/tiedonhallinnan-ohjaus/terveydenhuollon-tiedonhallinta/laakehoidon-tiedonhallinta/valtakunnallinen-laakityslista (accessed on 8 August 2021). (In Finnish).
- Kallio, S.; Eskola, T.; Pohjanoksa-Mäntylä, M.; Airaksinen, M. Medication Risk Management in Routine Dispensing in Community Pharmacies. Int. J. Environ. Res. Public Health 2020, 17, 8186. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Social Affairs and Health. Rationaalinen Lääkkeen Määrääminen, Toimittaminen ja Käyttö Nykyisissä ja Tulevissa SOTE-Rakenteissa (Rational Prescribing, Dispensing and Use of Medicines in Current and Future Healthcare and Social Welfare Structures); Reports and Memorandums of the Ministry of Social Affairs and Health 12/2018; Ministry of Social Affairs and Health: Helsinki, Finland, 2018; (In Finnish, summary in English).




{kind=link}
{kind=link}
{kind=link}
| Complaints | Development Proposals |
|---|---|
| Receiving the renewal request | |
|
|
| Reviewing the patient records and monitoring the medication | |
|
|
| Reviewing the medication list and checking medication alerts | |
|
|
| Reviewing the Prescription Centre and reviewing the patient’s entire medication regimen | |
|
|
| Interprofessional cooperation | |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oravainen, T.; Airaksinen, M.; Hannula, K.; Kvarnström, K. How Physicians Renew Electronic Prescriptions in Primary Care: Therapeutic Decision or Technical Task? Int. J. Environ. Res. Public Health 2021, 18, 10937. https://doi.org/10.3390/ijerph182010937
Oravainen T, Airaksinen M, Hannula K, Kvarnström K. How Physicians Renew Electronic Prescriptions in Primary Care: Therapeutic Decision or Technical Task? International Journal of Environmental Research and Public Health. 2021; 18(20):10937. https://doi.org/10.3390/ijerph182010937
Chicago/Turabian StyleOravainen, Taina, Marja Airaksinen, Kaija Hannula, and Kirsi Kvarnström. 2021. "How Physicians Renew Electronic Prescriptions in Primary Care: Therapeutic Decision or Technical Task?" International Journal of Environmental Research and Public Health 18, no. 20: 10937. https://doi.org/10.3390/ijerph182010937
APA StyleOravainen, T., Airaksinen, M., Hannula, K., & Kvarnström, K. (2021). How Physicians Renew Electronic Prescriptions in Primary Care: Therapeutic Decision or Technical Task? International Journal of Environmental Research and Public Health, 18(20), 10937. https://doi.org/10.3390/ijerph182010937