
Efficacy of Communication Techniques and Health Outcomes of Bushfire Smoke Exposure: A Scoping Review



{kind=link}
Abstract
:1. Introduction
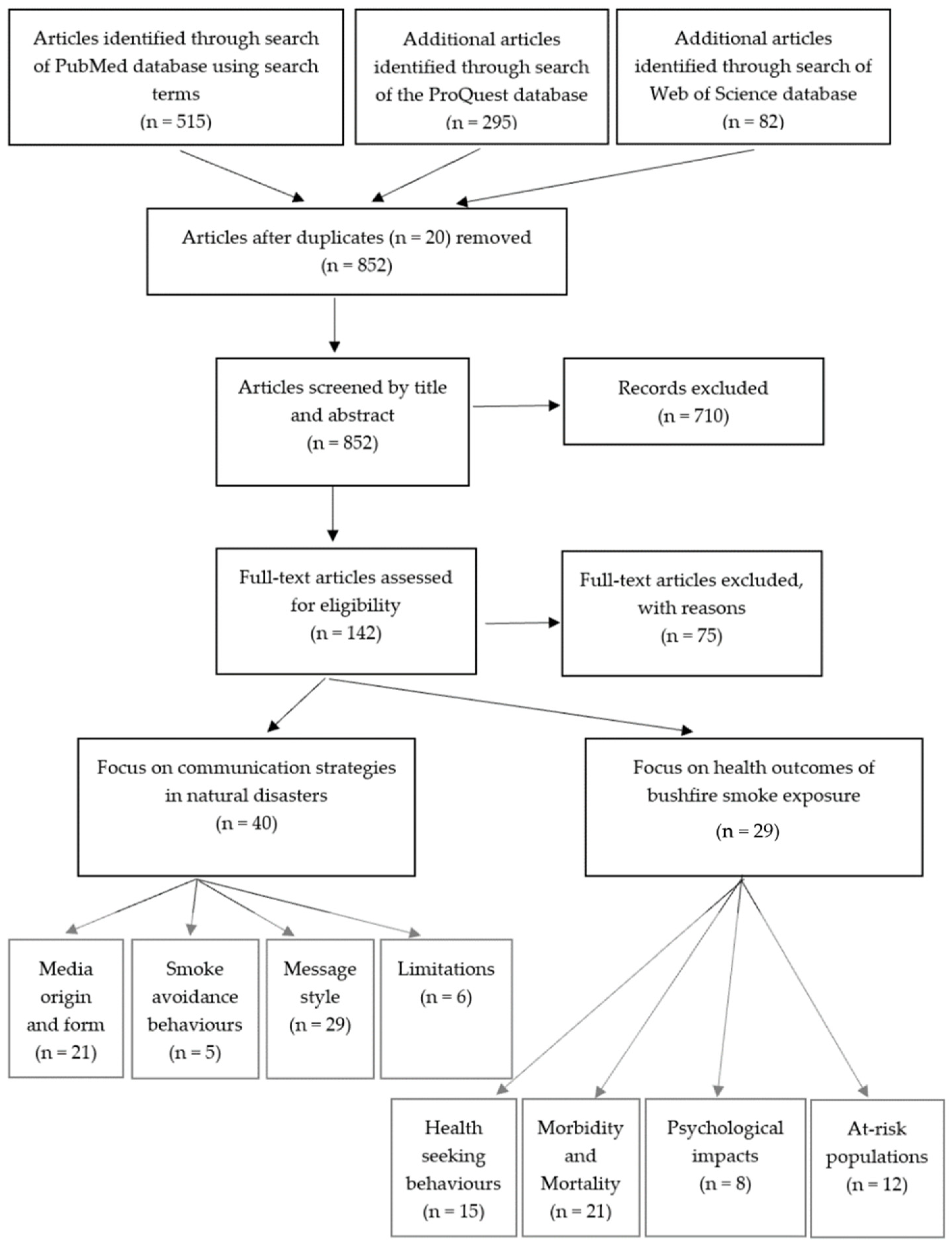
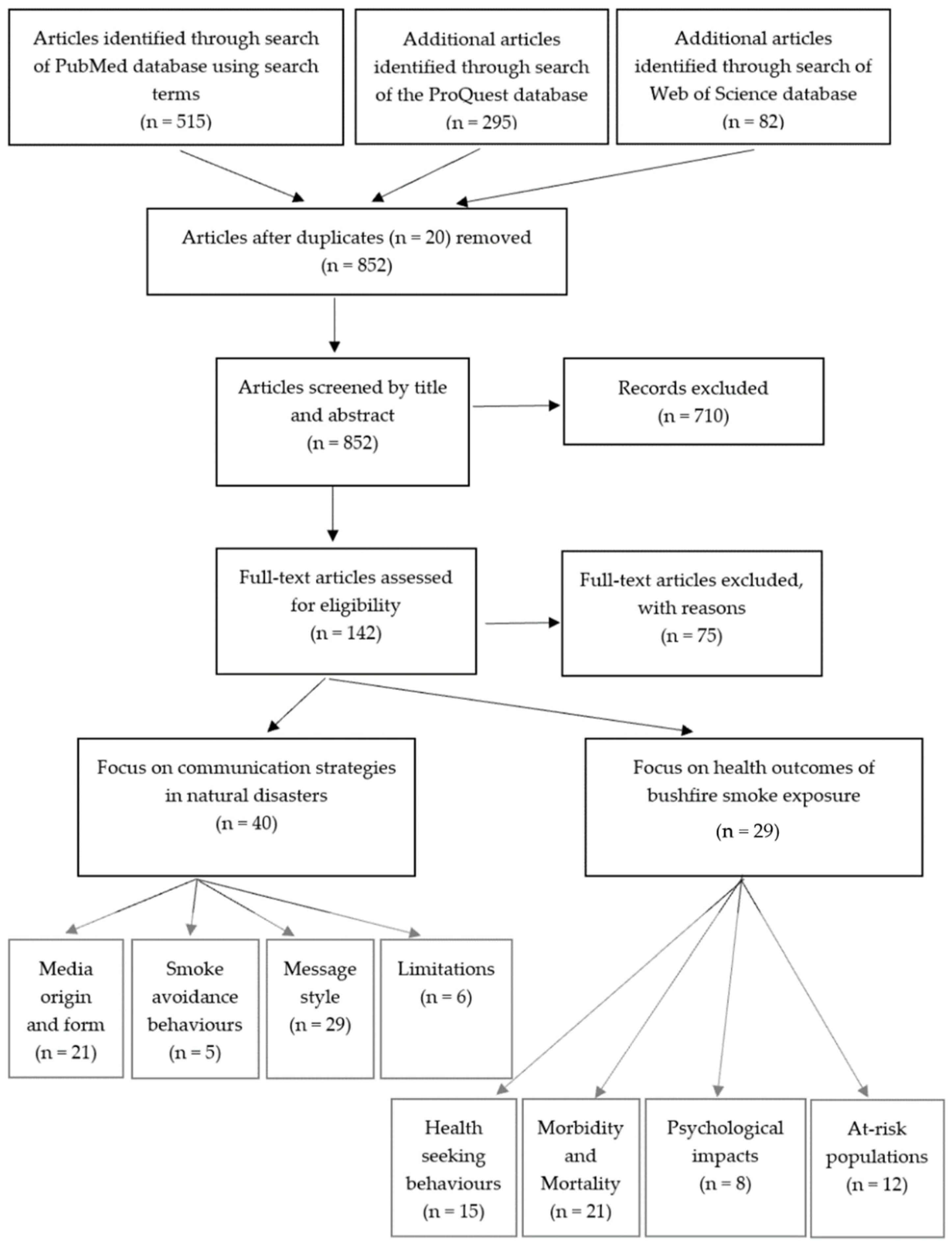
2. Materials and Methods
2.1. Study Inclusion Criteria
2.2. Search Criteria
2.3. Study Eligibility
2.4. Data Extraction
3. Results
3.1. Communication Media
3.2. Optimising Disaster Communication
3.3. Communication Limitations
3.4. Medical Admissions
3.5. Biomedical Effects of Bushfire Smoke Exposure
3.6. Psychosocial and Mental Health Effects
3.7. At-Risk Populations
3.8. Smoke Avoidance Behaviours
4. Discussion
4.1. Communication during Bushfires
4.2. Health Effects of Bushfire Smoke Exposure
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- CSIRO. The 2019–20 Bushfires: A CSIRO Explainer. Available online: https://www.csiro.au/en/Research/Environment/Extreme-Events/Bushfire/preparing-for-climate-change/2019–20-bushfires-explainer (accessed on 21 July 2021).
- Walter, C.; Schneider, E.; Knibbs, L.D.; Irving, L.B. Health impacts of bushfire smoke exposure in Australia. Respirology 2020, 25, 495–501. [Google Scholar] [CrossRef]
- Ambient (Outdoor) Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health#:~:text=%22WHO%20air%20quality%20guidelines%22%20estimate,related%20deaths%20by%20around%2015%25 (accessed on 29 July 2021).
- Quinn, P. Crisis Communication in Public Health Emergencies: The Limits of ‘Legal Control’ and the Risks for Harmful Outcomes in a Digital Age. Life Sci. Soc. Policy 2018, 14, 4. [Google Scholar] [CrossRef] [Green Version]
- Vardoulakis, S.; Jalaludin, B.B.; Morgan, G.G.; Hanigan, I.C.; Johnston, F.H. Bushfire smoke: Urgent need for a national health protection strategy. Med. J. Aust. 2020, 212, 349–353. [Google Scholar] [CrossRef] [Green Version]
- Australian Department of Health. Reducing the Risk of Prolonged Exposure to Smoke. Available online: https://www.health.gov.au/news/reducing-the-risk-of-prolonged-exposure-to-smoke (accessed on 21 June 2020).
- Jarraud, M.; Steiner, A.; Allen, S.K.; Burton, I.; Campbell-Lendrum, D.; Cardona, O.-D.; Cutter, S.L.; Dube, O.P.; Ebi, K.L.; Handmer, J.W.; et al. Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation. In Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation; Cambridge University Press (CUP): Cambridge, UK, 2012. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 Version); Aromataris, E., Munn, Z., Eds.; JBI Manual for Evidence Synthesis; Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Burns, R.; Robinson, P.; Smith, P. From hypothetical scenario to tragic reality: A salutary lesson in risk communication and the Victorian 2009 bushfires. Aust. N. Z. J. Public Health 2010, 34, 24–31. [Google Scholar] [CrossRef]
- Chauhan, A.; Hughes, A.L. Providing Online Crisis Information. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 3151–3162. [Google Scholar]
- Fish, J.A.; Peters, M.; Ramsey, I.; Sharplin, G.; Corsini, N.; Eckert, M. Effectiveness of public health messaging and communication channels during smoke events: A rapid systematic review. J. Environ. Manag. 2017, 193, 247–256. [Google Scholar] [CrossRef]
- Hugelius, K.; Adams, M.; Romo-Murphy, E. The Power of Radio to Promote Health and Resilience in Natural Disasters: A Review. Int. J. Environ. Res. Public Health 2019, 16, 2526. [Google Scholar] [CrossRef] [Green Version]
- Martin, N.; Rice, J. Emergency communications and warning systems. Disaster Prev. Manag. Int. J. 2012, 21, 529–540. [Google Scholar] [CrossRef]
- Olsen, C.S.; Mazzotta, D.K.; Toman, E.; Fischer, A.P. Communicating About Smoke from Wildland Fire: Challenges and Opportunities for Managers. Environ. Manag. 2014, 54, 571–582. [Google Scholar] [CrossRef]
- Prasadi Kanchana, J. Role of Facebook as a disaster communication media. Int. J. Emerg. Serv. 2019, 8, 191–204. [Google Scholar] [CrossRef]
- Robinson, M. Bushfires A rural GP’s perspective. Aust. Fam. Physician 2003, 32, 985–988. [Google Scholar]
- Ryan, B. Establishing information seeking pathways in slow and flash floods. Int. J. Disaster Risk Reduct. 2018, 31, 9–19. [Google Scholar] [CrossRef]
- Steelman, T.A.; McCaffrey, S. Best practices in risk and crisis communication: Implications for natural hazards management. Nat. Hazards 2013, 65, 683–705. [Google Scholar] [CrossRef]
- Sugerman, D.E.; Keir, J.M.; Dee, D.L.; Lipman, H.; Waterman, S.H.; Ginsberg, M.; Fishbein, D.B. Emergency Health Risk Communication During the 2007 San Diego Wildfires: Comprehension, Compliance, and Recall. J. Health Commun. 2012, 17, 698–712. [Google Scholar] [CrossRef] [PubMed]
- Van Deventer, D.; Marecaux, J.; Doubleday, A.; Errett, N.; Isaksen, T.M.B. Wildfire Smoke Risk Communication Efficacy. J. Public Health Manag. Pract. 2020. [Google Scholar] [CrossRef]
- Wang, Z.; Ye, X.; Tsou, M.-H. Spatial, temporal, and content analysis of Twitter for wildfire hazards. Nat. Hazards 2016, 83, 523–540. [Google Scholar] [CrossRef]
- Abedin, B.; Babar, A. Institutional vs. Non-institutional use of Social Media during Emergency Response: A Case of Twitter in 2014 Australian Bush Fire. Inf. Syst. Front. 2018, 20, 729–740. [Google Scholar] [CrossRef] [Green Version]
- Brengarth, L.B.; Mujkic, E. WEB 2.0: How social media applications leverage nonprofit responses during a wildfire crisis. Comput. Hum. Behav. 2016, 54, 589–596. [Google Scholar] [CrossRef]
- Mosites, E.; Lujan, E.; Brook, M.; Brubaker, M.; Roehl, D.; Tcheripanoff, M.; Hennessy, T. Environmental observation, social media, and One Health action: A description of the Local Environmental Observer (LEO) Network. One Health 2018, 6, 29–33. [Google Scholar] [CrossRef]
- Rappold, A.; Hano, M.; Prince, S.; Wei, L.; Huang, S.; Baghdikian, C.; Stearns, B.; Gao, X.; Hoshiko, S.; Cascio, W.; et al. Smoke Sense Initiative Leverages Citizen Science to Address the Growing Wildfire-Related Public Health Problem. GeoHealth 2019, 3, 443–457. [Google Scholar] [CrossRef] [Green Version]
- Sachdeva, S.; McCaffrey, S.; Locke, D. Social media approaches to modeling wildfire smoke dispersion: Spatiotemporal and social scientific investigations. Inf. Commun. Soc. 2016, 20, 1146–1161. [Google Scholar] [CrossRef]
- Slavkovikj, V.; Verstockt, S.; Van Hoecke, S.; Van De Walle, R. Review of wildfire detection using social media. Fire Saf. J. 2014, 68, 109–118. [Google Scholar] [CrossRef]
- Neaves, A.T.T.; Mann, S.C.; Myers, L.B.; Cosby, A.G. Assessing Reverse 911®: A case study of the 2007 San Diego wildfires. J. Emerg. Manag. 2014, 12, 315–325. [Google Scholar] [CrossRef]
- Xu, D.; Zhuang, L.; Deng, X.; Qing, C.; Yong, Z. Media Exposure, Disaster Experience, and Risk Perception of Rural Households in Earthquake-Stricken Areas: Evidence from Rural China. Int. J. Environ. Res. Public Health 2020, 17, 3246. [Google Scholar] [CrossRef]
- D’Antoni, D.; Smith, L.; Auyeung, V.; Weinman, J. Psychosocial and demographic predictors of adherence and non-adherence to health advice accompanying air quality warning systems: A systematic review. Environ. Health 2017, 16, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Lyth, A.; Spinaze, A.; Watson, P.; Johnston, F.H. Place, human agency and community resilience—Considerations for public health management of smoke from prescribed burning. Local Environ. 2018, 23, 975–990. [Google Scholar] [CrossRef]
- Andrulis, D.P.; Siddiqui, N.J.; Purtle, J.P. Integrating Racially and Ethnically Diverse Communities Into Planning for Disasters: The California Experience. Disaster Med. Public Health Prep. 2011, 5, 227–234. [Google Scholar] [CrossRef]
- McCool, S.F.; Burchfield, J.A.; Williams, D.R.; Carroll, M.S. An Event-Based Approach for Examining the Effects of Wildland Fire Decisions on Communities. Environ. Manag. 2006, 37, 437–450. [Google Scholar] [CrossRef]
- Sutton, J.; Spiro, E.S.; Johnson, B.; Fitzhugh, S.; Gibson, B.; Butts, C.T. Warning tweets: Serial transmission of messages during the warning phase of a disaster event. Inf. Commun. Soc. 2014, 17, 765–787. [Google Scholar] [CrossRef]
- Vaidyanathan, A.; Yip, F.; Garbe, P. Developing an online tool for identifying at-risk populations to wildfire smoke hazards. Sci. Total Environ. 2018, 619–620, 376–383. [Google Scholar] [CrossRef]
- Anderson-Berry, L.; Achilles, T.; Panchuk, S.; Mackie, B.; Canterford, S.; Leck, A.; Bird, D.K. Sending a message: How significant events have influenced the warnings landscape in Australia. Int. J. Disaster Risk Reduct. 2018, 30, 5–17. [Google Scholar] [CrossRef]
- Bearman, C.; Grunwald, J.A.; Brooks, B.P.; Owen, C. Breakdowns in coordinated decision making at and above the incident management team level: An analysis of three large scale Australian wildfires. Appl. Ergon. 2015, 47, 16–25. [Google Scholar] [CrossRef]
- Damon, S.A.; Naylor, R.; Therriault, S. Public communication in unplanned biomass burning events. Inhal. Toxicol. 2009, 22, 113–116. [Google Scholar] [CrossRef]
- Shittu, E.; Parker, G.; Mock, N. Improving communication resilience for effective disaster relief operations. Environ. Syst. Decis. 2018, 38, 379–397. [Google Scholar] [CrossRef]
- Kain, N.A.; Jardine, C.G. “Keep it short and sweet”: Improving risk communication to family physicians during public health crises. Can. Fam. Physician 2020, 66, e99–e106. [Google Scholar]
- Liu, B.F.; Iles, I.A.; Herovic, E. Leadership under Fire: How Governments Manage Crisis Communication. Commun. Stud. 2019, 71, 128–147. [Google Scholar] [CrossRef]
- MacIntyre, E.; Khanna, S.; Darychuk, A.; Copes, R.; Schwartz, B. Evidence synthesis Evaluating risk communication during extreme weather and climate change: A scoping review. Health Promot. Chronic Dis. Prev. Can. 2019, 39, 142–156. [Google Scholar] [CrossRef]
- Neuhauser, L.; Ivey, S.L.; Huang, D.; Engelman, A.; Tseng, W.; Dahrouge, D.; Gurung, S.; Kealey, M. Availability and Readability of Emergency Preparedness Materials for Deaf and Hard-of-Hearing and Older Adult Populations: Issues and Assessments. PLoS ONE 2013, 8, e55614. [Google Scholar] [CrossRef] [Green Version]
- Sharp, E.A.; Thwaites, R.; Curtis, A.; Millar, J. Factors affecting community-agency trust before, during and after a wildfire: An Australian case study. J. Environ. Manag. 2013, 130, 10–19. [Google Scholar] [CrossRef]
- Steelman, T.A.; McCaffrey, S.M.; Velez, A.-L.K.; Briefel, J.A. What information do people use, trust, and find useful during a disaster? Evidence from five large wildfires. Nat. Hazards 2015, 76, 615–634. [Google Scholar] [CrossRef]
- Hano, M.C.; Baghdikian, C.L.; Prince, S.; Lazzarino, E.; Hubbell, B.; Sams, E.; Stone, S.; Davis, A.; Cascio, W.E. Illuminating Stakeholder Perspectives at the Intersection of Air Quality Health Risk Communication and Cardiac Rehabilitation. Int. J. Environ. Res. Public Health 2019, 16, 3603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medford-Davis, L.N.; Kapur, G.B. Preparing for effective communications during disasters: Lessons from a World Health Organization quality improvement project. Int. J. Emerg. Med. 2014, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniz-Rodriguez, K.; Ofori, S.K.; Bayliss, L.C.; Schwind, J.S.; Diallo, K.; Liu, M.; Yin, J.; Chowell, G.; Fung, I.C.-H. Social Media Use in Emergency Response to Natural Disasters: A Systematic Review With a Public Health Perspective. Disaster Med. Public Health Prep. 2020, 14, 139–149. [Google Scholar] [CrossRef]
- Bernstein, A.S.; Rice, M.B. Lungs in a warming world: Climate change and respiratory health. Chest 2013, 143, 1455–1459. [Google Scholar] [CrossRef] [Green Version]
- Borchers Arriagada, N.; Horsley, J.A.; Palmer, A.J.; Morgan, G.G.; Tham, R.; Johnston, F.H. Association between fire smoke fine particulate matter and asthma-related outcomes: Systematic review and meta-analysis. Environ. Res. 2019, 179, 108777. [Google Scholar] [CrossRef]
- Cascio, W.E. Wildland fire smoke and human health. Sci. Total Environ. 2018, 624, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.H.; Ngiam, N.J.; Morgan, G.G.; Pek, P.P.; Tan, B.; Lai, J.W.; Koh, J.M.; Ong, M.E.H.; Ho, A.F.W. Acute Health Impacts of the Southeast Asian Transboundary Haze Problem—A Review. Int. J. Environ. Res. Public Health 2019, 16, 3286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finlay, S.E.; Moffat, A.; Gazzard, R.; Baker, D.; Murray, V. Health Impacts of Wildfires. PLoS Curr. 2012, 4, e4f959951cce2c. [Google Scholar] [CrossRef] [PubMed]
- Haikerwal, A.; Reisen, F.; Sim, M.R.; Abramson, M.J.; Meyer, C.P.; Johnston, F.H.; Dennekamp, M. Impact of smoke from prescribed burning: Is it a public health concern? J. Air Waste Manag. Assoc. 2015, 65, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesterberg, T.W.; Bunn, W.B.; McClellan, R.O.; Hamade, A.K.; Long, C.M.; Valberg, P.A. Critical review of the human data on short-term nitrogen dioxide (NO2) exposures: Evidence for NO2no-effect levels. Crit. Rev. Toxicol. 2009, 39, 743–781. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Purdie, S.; Jalaludin, B.; Martin, K.L.; Henderson, S.B.; Morgan, G.G. Air pollution events from forest fires and emergency department attendances in Sydney, Australia 1996–2007: A case-crossover analysis. Environ. Health 2014, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondo, M.C.; De Roos, A.J.; White, L.S.; Heilman, W.E.; Mockrin, M.H.; Gross-Davis, C.A.; Burstyn, I. Meta-Analysis of Heterogeneity in the Effects of Wildfire Smoke Exposure on Respiratory Health in North America. Int. J. Environ. Res. Public Health 2019, 16, 960. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.C.; Pereira, G.; Uhl, S.A.; Bravo, M.A.; Bell, M.L. A systematic review of the physical health impacts from non-occupational exposure to wildfire smoke. Environ. Res. 2015, 136, 120–132. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, M.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Environmental Particulate Matter Levels during 2017 Large Forest Fires and Megafires in the Center Region of Portugal: A Public Health Concern? Int. J. Environ. Res. Public Health 2020, 17, 1032. [Google Scholar] [CrossRef] [Green Version]
- Tham, R.; Erbas, B.; Akram, M.; Dennekamp, M.; Abramson, M.J. The impact of smoke on respiratory hospital outcomes during the 2002-2003 bushfire season, Victoria, Australia. Respirology 2009, 14, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Jin, Y.; Carlsten, C. Inflammatory health effects of indoor and outdoor particulate matter. J. Allergy Clin. Immunol. 2018, 141, 833–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrieri, M.L.; Roy, N.C.; Rose-Davison, K.N.; Roy, C.J. Wildfire Associated Health Risks Impacting Farmers and Ranchers. J. Agromed. 2019, 24, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.; Stieb, D.M.; Taylor, E.; Henderson, S.B. Assessment of the Air Quality Health Index (AQHI) and four alternate AQHI-Plus amendments for wildfire seasons in British Columbia. Can. J. Public Health 2020, 111, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Beggs, P.J.; Zhang, Y.; Bambrick, H.; Berry, H.L.; Linnenluecke, M.K.; Trueck, S.; Bi, P.; Boylan, S.M.; Green, D.; Guo, Y.; et al. The 2019 report of theMJA–LancetCountdown on health and climate change: A turbulent year with mixed progress. Med. J. Aust. 2019, 211, 490–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doubleday, A.; Schulte, J.; Sheppard, L.; Kadlec, M.; Dhammapala, R.; Fox, J.; Isaksen, T.B. Mortality associated with wildfire smoke exposure in Washington state, 2006–2017: A case-crossover study. Environ. Health 2020, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennekamp, M.; Straney, L.D.; Erbas, B.; Abramson, M.J.; Keywood, M.; Smith, K.; Sim, M.R.; Glass, D.; DEL Monaco, A.; Haikerwal, A.; et al. Forest Fire Smoke Exposures and Out-of-Hospital Cardiac Arrests in Melbourne, Australia: A Case-Crossover Study. Environ. Health Perspect. 2015, 123, 959–964. [Google Scholar] [CrossRef] [Green Version]
- Jalaludin, B.; Smith, M.; O’Toole, B.; Leeder, S. Acute effects of bushfires on peak expiratory flow rates in children with wheeze: A time series analysis. Aust. N. Z. J. Public Health 2000, 24, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Afifi, W.A.; Felix, E.D.; Afifi, T.D. The impact of uncertainty and communal coping on mental health following natural disasters. Anxiety Stress. Coping 2012, 25, 329–347. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Sinnott, V.; Ireton, G.; et al. Longitudinal study of changing psychological outcomes following the Victorian Black Saturday bushfires. Aust. N. Z. J. Psychiatry 2018, 52, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Molyneaux, R.; Gibbs, L.; Bryant, R.A.; Humphreys, C.; Hegarty, K.; Kellett, C.; Gallagher, H.C.; Block, K.; Harms, L.; Richardson, J.F.; et al. Interpersonal violence and mental health outcomes following disaster. BJPsych Open 2019, 6, e1. [Google Scholar] [CrossRef]
- Cox, R.S.; Perry, K.-M.E. Like a Fish Out of Water: Reconsidering Disaster Recovery and the Role of Place and Social Capital in Community Disaster Resilience. Am. J. Community Psychol. 2011, 48, 395–411. [Google Scholar] [CrossRef]
- Dodd, W.; Scott, P.; Howard, C.; Scott, C.; Rose, C.; Cunsolo, A.; Orbinski, J. Lived experience of a record wildfire season in the Northwest Territories, Canada. Can. J. Public Health 2018, 109, 327–337. [Google Scholar] [CrossRef]
- Felix, E.; Afifi, T.; Kia-Keating, M.; Brown, L.; Afifi, W.; Reyes, G. Family functioning and posttraumatic growth among parents and youth following wildfire disasters. Am. J. Orthopsychiatry 2015, 85, 191–200. [Google Scholar] [CrossRef]
- Liu, J.C.; Wilson, A.; Mickley, L.J.; Ebisu, K.; Sulprizio, M.P.; Wang, Y.; Peng, R.D.; Yue, X.; Dominici, F.; Bell, M. Who Among the Elderly Is Most Vulnerable to Exposure to and Health Risks of Fine Particulate Matter From Wildfire Smoke? Am. J. Epidemiol. 2017, 186, 730–735. [Google Scholar] [CrossRef]
- Dong, T.T.; Hinwood, A.L.; Callan, A.; Zosky, G.; Stock, W.D. In vitro assessment of the toxicity of bushfire emissions: A review. Sci. Total Environ. 2017, 603-604, 268–278. [Google Scholar] [CrossRef]
- Arriagada, N.B.; Palmer, A.J.; Bowman, D.M.; Morgan, G.; Jalaludin, B.B.; Johnston, F.H. Unprecedented smoke-related health burden associated with the 2019–20 bushfires in eastern Australia. Med. J. Aust. 2020, 213, 282–283. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Marks, G.; Abramson, M.J. Lessons Learned from the Australian Bushfires. JAMA Intern. Med. 2020, 180, 635. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heaney, E.; Hunter, L.; Clulow, A.; Bowles, D.; Vardoulakis, S. Efficacy of Communication Techniques and Health Outcomes of Bushfire Smoke Exposure: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 10889. https://doi.org/10.3390/ijerph182010889
Heaney E, Hunter L, Clulow A, Bowles D, Vardoulakis S. Efficacy of Communication Techniques and Health Outcomes of Bushfire Smoke Exposure: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(20):10889. https://doi.org/10.3390/ijerph182010889
Chicago/Turabian StyleHeaney, Emily, Laura Hunter, Angus Clulow, Devin Bowles, and Sotiris Vardoulakis. 2021. "Efficacy of Communication Techniques and Health Outcomes of Bushfire Smoke Exposure: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 20: 10889. https://doi.org/10.3390/ijerph182010889
APA StyleHeaney, E., Hunter, L., Clulow, A., Bowles, D., & Vardoulakis, S. (2021). Efficacy of Communication Techniques and Health Outcomes of Bushfire Smoke Exposure: A Scoping Review. International Journal of Environmental Research and Public Health, 18(20), 10889. https://doi.org/10.3390/ijerph182010889