
Detailed Analysis of Neurological Symptoms and Sensory Disturbances Due to Chronic Arsenic Exposure in Toroku, Japan

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Symptoms
2.4. Objective Sensory Disturbances
2.5. Duration between Initial Arsenic Exposure and the Onset of Each Symptom
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
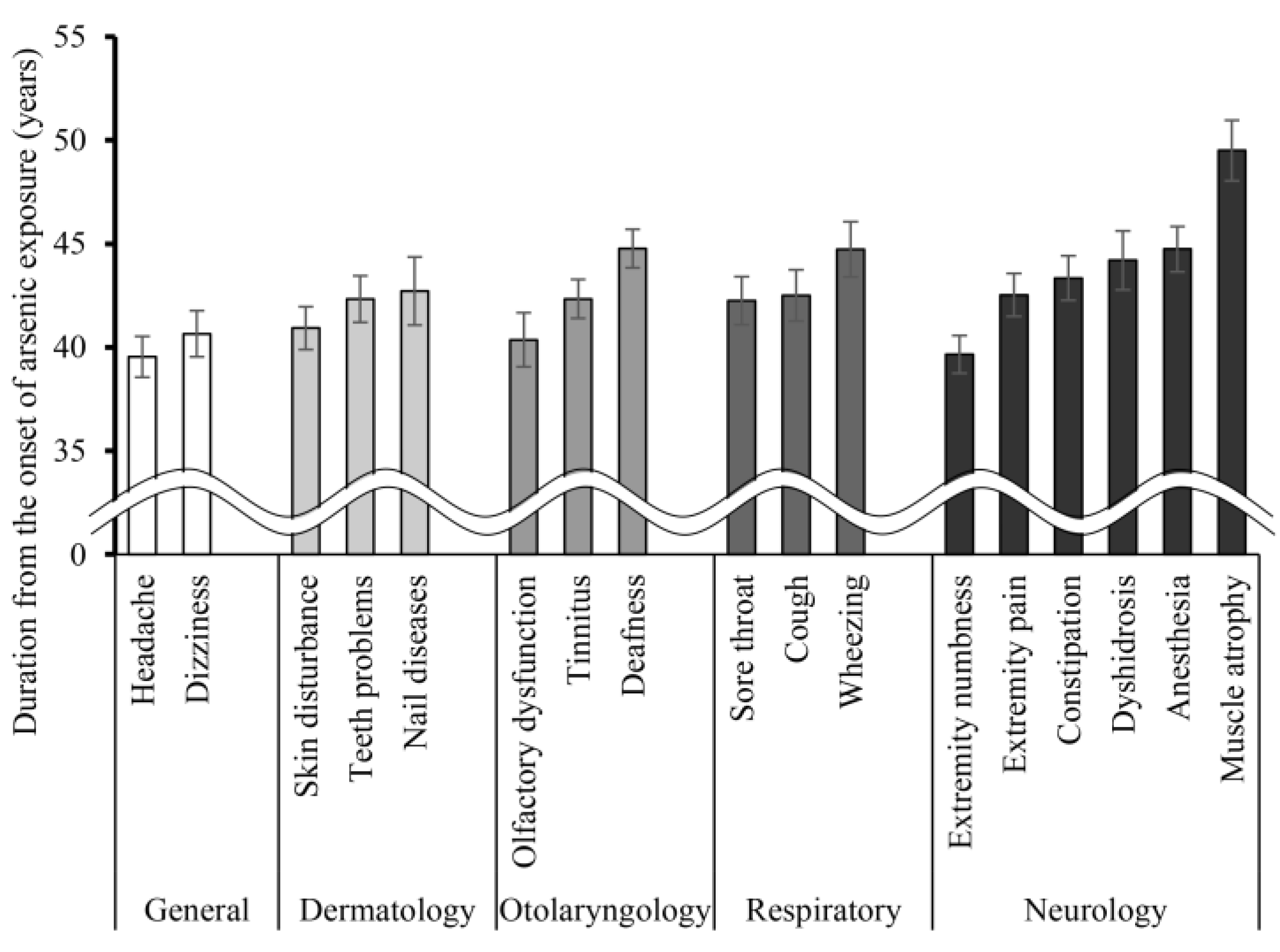
3.2. Natural History of Reported Symptoms
3.3. Numbness and Objective Sensory Disturbances
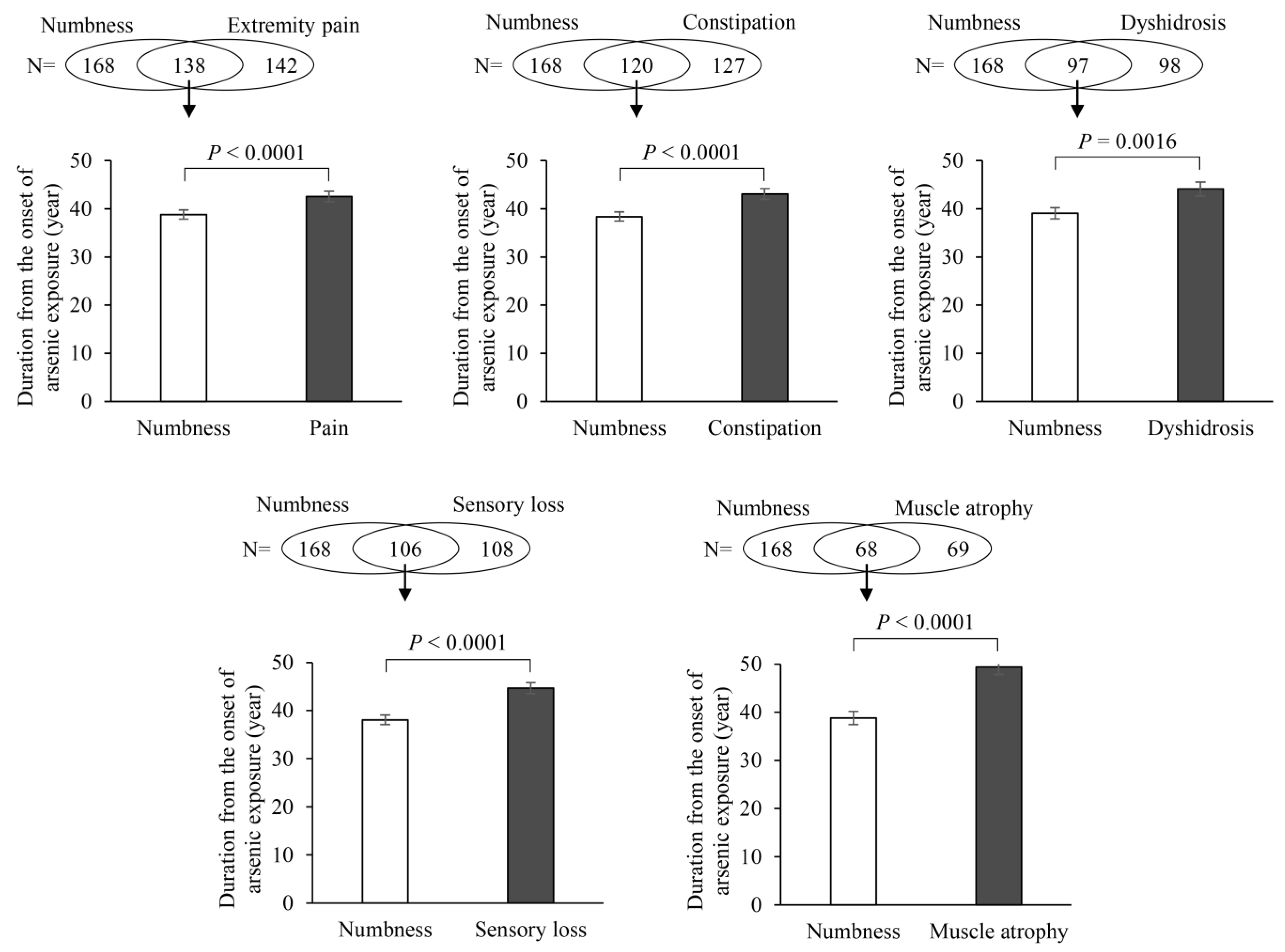
3.4. The Relationship between Numbness and Other Neurological Symptoms
4. Discussion
4.1. Extremity Numbness Is Often the First Symptom in the Natural History of Arsenic Exposure
4.2. Numbness and Small Fiber Neuropathy Due to Arsenic Exposure
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M.S.H. Prevalence of exposure of heavy metals and their impact on health consequences. J. Cell. Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Singh, S.; Parihar, P.; Singh, V.P.; Prasad, S.M. Arsenic contamination, consequences and remediation techniques: A review. Ecotoxicol. Environ. Saf. 2015, 112, 247–270. [Google Scholar] [CrossRef]
- Hughes, M.F.; Beck, B.D.; Chen, Y.; Lewis, A.S.; Thomas, D.J. Arsenic exposure and toxicology: A historical perspective. Toxicol. Sci. 2011, 123, 305–332. [Google Scholar] [CrossRef]
- Mochizuki, H. Arsenic Neurotoxicity in Humans. Int. J. Mol. Sci. 2019, 20, 3418. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, H.; Yagi, K.; Tsuruta, K.; Taniguchi, A.; Ishii, N.; Shiomi, K.; Nakazato, M. Prolonged central sensory conduction time in patients with chronic arsenic exposure. J. Neurol. Sci. 2016, 361, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki Prefecture. Toroku Chiku no Kougai ni Kakawaru Shakaiigakutekityousaseiseki; Miyazaki Prefecture: Miyazaki, Japan, 1972; pp. 1–97. (In Japanese) [Google Scholar]
- Japan Federation of Bar Associations. Closed Mine Pollution Report; Japan Federation of Bar Associations: Tokyo, Japan, 1975; pp. 44–108. (In Japanese) [Google Scholar]
- Ishii, N.; Mochizuki, H.; Ebihara, Y.; Shiomi, K.; Nakazato, M. Clinical Symptoms, Neurological Signs, and Electrophysiological Findings in Surviving Residents with Probable Arsenic Exposure in Toroku, Japan. Arch. Environ. Contam. Toxicol. 2018, 75, 521–529. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Guha Mazumder, D.; Dasgupta, U.B. Chronic arsenic toxicity: Studies in West Bengal, India. Kaohsiung J. Med. Sci. 2011, 27, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, H.; Phyu, K.P.; Aung, M.N.; Zin, P.W.; Yano, Y.; Myint, M.Z.; Thit, W.M.; Yamamoto, Y.; Hishikawa, Y.; Thant, K.Z.; et al. Peripheral neuropathy induced by drinking water contaminated with low-dose arsenic in Myanmar. Environ. Health Prev. Med. 2019, 24, 23. [Google Scholar] [CrossRef] [PubMed]
- Guha Mazumder, D.N. Chronic arsenic toxicity & human health. Indian J. Med. Res. 2008, 128, 436–447. [Google Scholar] [PubMed]
- Mukherjee, S.C.; Rahman, M.M.; Chowdhury, U.K.; Sengupta, M.K.; Lodh, D.; Chanda, C.R.; Saha, K.C.; Chakraborti, D. Neuropathy in arsenic toxicity from groundwater arsenic contamination in West Bengal, India. J. Environ. Sci. Health A Tox. Hazard. Subst. Environ. Eng. 2003, 38, 165–183. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Chowdhury, U.K.; Mukherjee, S.C.; Mondal, B.K.; Paul, K.; Lodh, D.; Biswas, B.K.; Chanda, C.R.; Basu, G.K.; Saha, K.C.; et al. Chronic arsenic toxicity in Bangladesh and West Bengal, India—A review and commentary. J. Toxicol. Clin. Toxicol. 2001, 39, 683–700. [Google Scholar] [CrossRef]
- Chakraborti, D.; Rahman, M.M.; Ahamed, S.; Dutta, R.N.; Pati, S.; Mukherjee, S.C. Arsenic contamination of groundwater and its induced health effects in Shahpur block, Bhojpur district, Bihar state, India: Risk evaluation. Environ. Sci. Pollut. Res. Int. 2016, 23, 9492–9504. [Google Scholar] [CrossRef] [PubMed]
- Fujino, Y.; Guo, X.; Shirane, K.; Liu, J.; Wu, K.; Miyatake, M.; Tanabe, K.; Kusuda, T.; Yoshimura, T. Arsenic in drinking water and peripheral nerve conduction velocity among residents of a chronically arsenic-affected area in Inner Mongolia. J. Epidemiol. 2006, 16, 207–213. [Google Scholar] [CrossRef][Green Version]
- Koszewicz, M.; Markowska, K.; Waliszewska-Prosol, M.; Poreba, R.; Gac, P.; Szymanska-Chabowska, A.; Mazur, G.; Wieczorek, M.; Ejma, M.; Slotwinski, K.; et al. The impact of chronic co-exposure to different heavy metals on small fibers of peripheral nerves. A study of metal industry workers. J. Occup. Med. Toxicol. 2021, 16, 12. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Total (N = 190) |
|---|---|
| Male/female, n | 100/90 |
| Participants with active arsenic exposure | |
| from birth | 26 (13.7) (1) |
| after infancy | 164 (86.3) (1) |
| Initial age of first arsenic exposure | 16.6 (1–44) (2) |
| Age in 1962 when the mine closed | 42.7 (16–73) (2) |
| Parameters | Total (N = 190) |
|---|---|
| General | |
| Headache | 155 (81.6) |
| Dizziness | 144 (75.8) |
| Dermatology | |
| Skin disturbance | 155 (81.6) |
| Teeth problems | 128 (67.4) |
| Nail diseases | 89 (46.8) |
| Otolaryngology | |
| Tinnitus | 141 (74.2) |
| Deafness | 134 (70.5) |
| Olfactory dysfunction | 114 (60.0) |
| Respiratory | |
| Cough | 128 (67.4) |
| Sore throat | 107 (56.3) |
| Wheezing | 106 (55.8) |
| Neurology | |
| Extremity numbness | 168 (88.4) |
| Extremity pain | 142 (74.7) |
| Constipation | 127 (66.8) |
| Sensory loss | 108 (56.8) |
| Dyshidrosis | 98 (51.6) |
| Muscle atrophy | 69 (36.3) |
| Numbness | Pearson’s Chi-Square Test | |||||
|---|---|---|---|---|---|---|
| Positive | Negative | Value | df | p | ||
| Superficial sensory disturbance | positive | 104 | 7 | |||
| negative | 55 | 11 | 4.863 | 1 | 0.027 | |
| Vibratory sensory disturbance | positive | 118 | 12 | |||
| negative | 41 | 6 | 0.472 | 1 | 0.492 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugiyama, T.; Ishii, N.; Ebihara, Y.; Shiomi, K.; Mochizuki, H. Detailed Analysis of Neurological Symptoms and Sensory Disturbances Due to Chronic Arsenic Exposure in Toroku, Japan. Int. J. Environ. Res. Public Health 2021, 18, 10749. https://doi.org/10.3390/ijerph182010749
Sugiyama T, Ishii N, Ebihara Y, Shiomi K, Mochizuki H. Detailed Analysis of Neurological Symptoms and Sensory Disturbances Due to Chronic Arsenic Exposure in Toroku, Japan. International Journal of Environmental Research and Public Health. 2021; 18(20):10749. https://doi.org/10.3390/ijerph182010749
Chicago/Turabian StyleSugiyama, Takashi, Nobuyuki Ishii, Yuka Ebihara, Kazutaka Shiomi, and Hitoshi Mochizuki. 2021. "Detailed Analysis of Neurological Symptoms and Sensory Disturbances Due to Chronic Arsenic Exposure in Toroku, Japan" International Journal of Environmental Research and Public Health 18, no. 20: 10749. https://doi.org/10.3390/ijerph182010749
APA StyleSugiyama, T., Ishii, N., Ebihara, Y., Shiomi, K., & Mochizuki, H. (2021). Detailed Analysis of Neurological Symptoms and Sensory Disturbances Due to Chronic Arsenic Exposure in Toroku, Japan. International Journal of Environmental Research and Public Health, 18(20), 10749. https://doi.org/10.3390/ijerph182010749