No Interaction Effect between Interleukin-6 Polymorphisms and Acid Ash Diet with Bone Resorption Marker in Postmenopausal Women

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
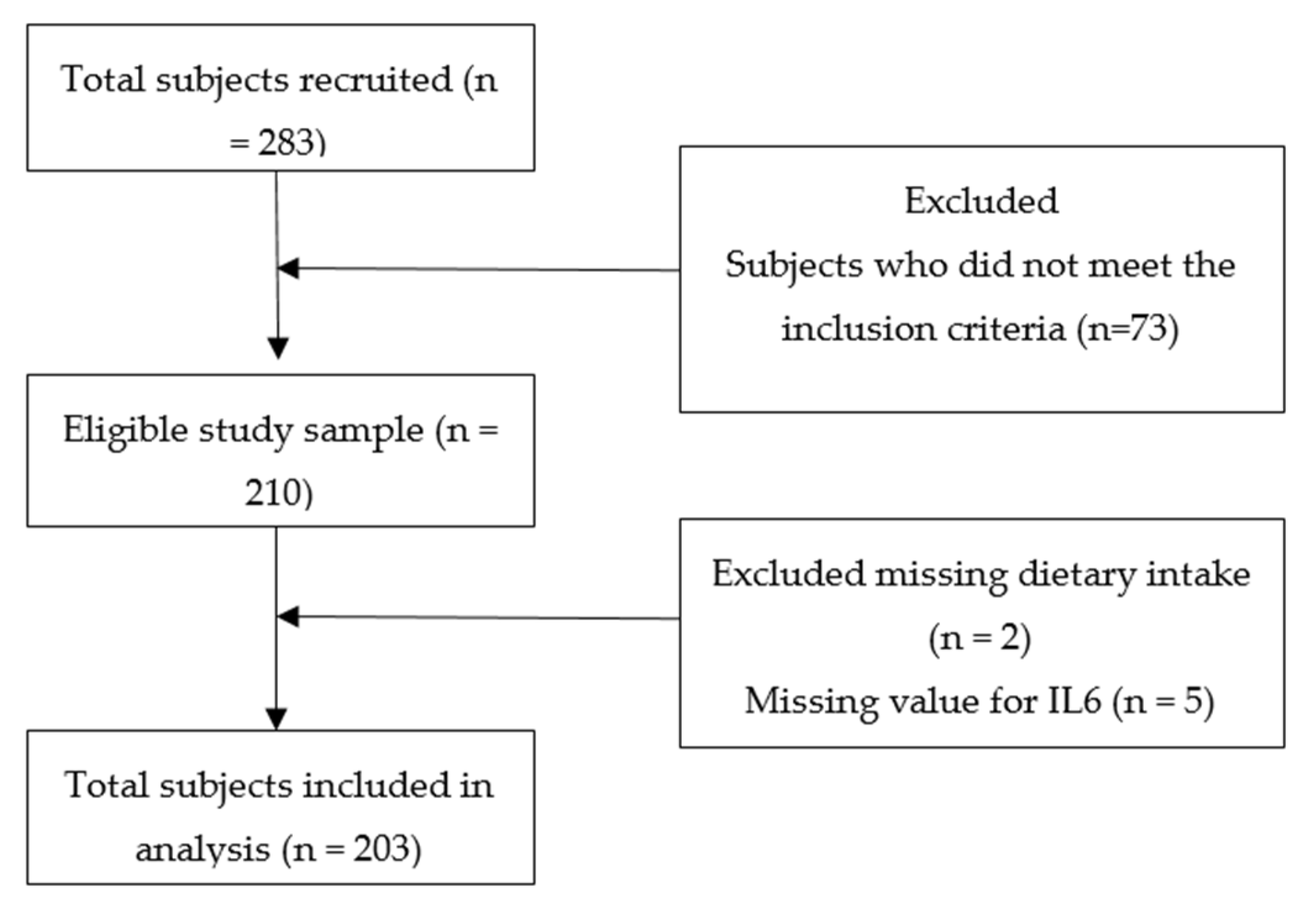
2.1. Study Population
2.2. Measurements
2.3. Dietary Assessment
2.4. Biochemical Measurements
2.5. Genetic Analysis
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Correlations between Variables and CTX1
3.3. Demographic, Anthropometrics, Lifestyle Factors, and Biochemical Analysis of Participants According to IL6 -572G/C Genotypes
3.4. Interaction of IL6 -572G/C with NEAP in Relation to CTX1
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cauley, J.A. Public health impact of osteoporosis. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1243–1251. [Google Scholar] [CrossRef]
- Taguchi, Y.; Inoue, Y.; Kido, T.; Arai, N. Treatment costs and cost drivers among osteoporotic fracture patients in Japan: A retrospective database analysis. Arch. Osteoporos. 2018, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Lloret, A.; Coiffier, G.; Couchouron, T.; Perdriger, A.; Guggenbuhl, P. Risk factors of mortality during the first year after low energy osteoporosis fracture: A retrospective case-control study. Clin. Cases Min. Bone Metab. 2016, 13, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Pisani, P.; Renna, M.D.; Conversano, F.; Casciaro, E.; Di Paola, M.; Quarta, E.; Muratore, M.; Casciaro, S. Major osteoporotic fragility fractures: Risk factor updates and societal impact. World J. Orthop. 2016, 7, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-wide projections for hip fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- LEE, J.K.; KHIR, A.S. The incidence of hip fracture in Malaysians above 50 years of age: Variation in different ethnic groups. Aplar. J. Rheumatol. 2007, 10, 300–305. [Google Scholar] [CrossRef]
- Greenwood, C.; Clement, J.; Dicken, A.; Evans, J.P.; Lyburn, I.; Martin, R.M.; Rogers, K.; Stone, N.; Zioupos, P. Towards new material biomarkers for fracture risk. Bone 2016, 93, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Vasikaran, S.D. Utility of biochemical markers of bone turnover and bone mineral density in management of osteoporosis. Crit. Rev. Clin. Lab. Sci. 2008, 45, 221–258. [Google Scholar] [CrossRef]
- Morris, H.A.; Eastell, R.; Jorgensen, N.R.; Cavalier, E.; Vasikaran, S.; Chubb, S.A.P.; Kanis, J.A.; Cooper, C.; Makris, K. Clinical usefulness of bone turnover marker concentrations in osteoporosis. Clin. Chim. Acta 2017, 467, 34–41. [Google Scholar] [CrossRef]
- Glendenning, P. Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: A need for international reference standards: Osteoporos int 2011;22:391-420. Clin. Biochem. Rev. 2011, 32, 45–47. [Google Scholar]
- Bauer, D.; Krege, J.; Lane, N.; Leary, E.; Libanati, C.; Miller, P.; Myers, G.; Silverman, S.; Vesper, H.W.; Lee, D.; et al. National Bone Health Alliance Bone Turnover Marker Project: Current practices and the need for US harmonization, standardization, and common reference ranges. Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2012, 23, 2425–2433. [Google Scholar] [CrossRef]
- Vasikaran, S.; Eastell, R.; Bruyere, O.; Foldes, A.J.; Garnero, P.; Griesmacher, A.; McClung, M.; Morris, H.A.; Silverman, S.; Trenti, T.; et al. Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: A need for international reference standards. Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2011, 22, 391–420. [Google Scholar] [CrossRef]
- Peacock, M.; Turner, C.H.; Econs, M.J.; Foroud, T. Genetics of osteoporosis. Endocr. Rev. 2002, 23, 303–326. [Google Scholar] [CrossRef] [PubMed]
- Moura, K.F.; Haidar, M.; Bonduki, C.; Feldner, P.C., Jr.; Silva, I.; Soares, J.M., Jr.; Girao, M.J. Frequencies of interleukin-6, GST and progesterone receptor gene polymorphisms in postmenopausal women with low bone mineral density. Sao Paulo Med. J. 2014, 132, 36–40. [Google Scholar] [CrossRef]
- Ferrari, S.L.; Garnero, P.; Emond, S.; Montgomery, H.; Humphries, S.E.; Greenspan, S.L. A functional polymorphic variant in the interleukin-6 gene promoter associated with low bone resorption in postmenopausal women. Arthritis Rheum. 2001, 44, 196–201. [Google Scholar] [CrossRef]
- Ni, Y.; Li, H.; Zhang, Y.; Zhang, H.; Pan, Y.; Ma, J.; Wang, L. Association of IL-6 G-174C polymorphism with bone mineral density. J. Bone Min. Metab. 2014, 32, 167–173. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, Y.; He, M.; Wang, R.; Ma, J.; Zhang, Y.; Zhao, L.; Yu, K. Association between interleukin-6 gene polymorphisms and bone mineral density: A meta-analysis. Genet. Test. Mol. Biomark. 2013, 17, 898–909. [Google Scholar] [CrossRef]
- Yan, L.; Hu, R.; Tu, S.; Cheng, W.J.; Zheng, Q.; Wang, J.W.; Kan, W.S.; Ren, Y.J. Meta-analysis of association between IL-6 -634C/G polymorphism and osteoporosis. Genet. Mol. Res. Gmr. 2015, 14, 19225–19232. [Google Scholar] [CrossRef]
- Pan, M.; Gao, S.P.; Jiang, M.H.; Guo, J.; Zheng, J.G.; Zhu, J.H. Interleukin 6 promoter polymorphisms in normal Han Chinese population: Frequencies and effects on inflammatory markers. J. Investig. Med. 2011, 59, 272–276. [Google Scholar] [CrossRef]
- Sun, G.Q.; Wu, G.D.; Meng, Y.; Du, B.; Li, Y.B. IL-6 gene promoter polymorphisms and risk of coronary artery disease in a Chinese population. Genet. Mol. Res. Gmr. 2014, 13, 7718–7724. [Google Scholar] [CrossRef]
- Welch, A.A.; MacGregor, A.J.; Skinner, J.; Spector, T.D.; Moayyeri, A.; Cassidy, A. A higher alkaline dietary load is associated with greater indexes of skeletal muscle mass in women. Osteoporos. Int. 2013, 24, 1899–1908. [Google Scholar] [CrossRef]
- Williams, R.S.; Kozan, P.; Samocha-Bonet, D. The role of dietary acid load and mild metabolic acidosis in insulin resistance in humans. Biochimie 2016, 124, 171–177. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, E.A.L.; Koromani, F.; Hofman, A.; Uitterlinden, A.G.; Franco, O.H.; Rivadeneira, F.; Kiefte-de Jong, J.C. Dietary acid load, trabecular bone integrity, and mineral density in an ageing population: The Rotterdam study. Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2017, 28, 2357–2365. [Google Scholar] [CrossRef]
- Jehle, S.; Hulter, H.N.; Krapf, R. Effect of potassium citrate on bone density, microarchitecture, and fracture risk in healthy older adults without osteoporosis: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Jia, T.; Byberg, L.; Lindholm, B.; Larsson, T.; Lind, L.; Michaëlsson, K.; Carrero, J.J.O.I. Dietary acid load, kidney function, osteoporosis, and risk of fractures in elderly men and women. Osteoporos. Int. 2015, 26, 563–570. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Qiao, N.; Broe, K.E.; Tucker, K.L.; Casey, V.; Cupples, L.A.; Kiel, D.P.; Hannan, M.T. Dietary acid load is not associated with lower bone mineral density except in older men. J. Nutr. 2011, 141, 588–594. [Google Scholar] [CrossRef]
- Shi, L.; Libuda, L.; Schonau, E.; Frassetto, L.; Remer, T. Long term higher urinary calcium excretion within the normal physiologic range predicts impaired bone status of the proximal radius in healthy children with higher potential renal acid load. Bone 2012, 50, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Brozek, J.; Keys, A. The evaluation of leanness-fatness in man; norms and interrelationships. Br. J. Nutr. 1951, 5, 194–206. [Google Scholar] [CrossRef]
- Harrison, G.G.; Buskirk, E.R.; Lindsay Carter, J.E.; Johnston, F.E.; Lohman, T.G.; Pollock, M.L.; Roche, A.F.; Wilmore, J. Skinfold Thicknesses and Measurement Technique: Anthropometric Standardization Reference Manual; Lohman, T.G.R., Martorell, A.F.R., Eds.; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- WHO/IOTF/IASO. International Obesity Task Force, International Association for the Study of Obesity. In The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Hong Kong, China, 2000. [Google Scholar]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Institute for Public Health Kuala. National Health and Morbidity Survey 2015—Report on Smoking Status Among Malaysian Adults; Institute for Public Health Kuala: Lumpur, Malaysia, 2015. [Google Scholar]
- Aris, T.; Ahmad, N.A.; Tee, G.H. National Health and Morbidity Survey 2014: Malaysian Adults Nutrition Survey (MANS); Institute for Public Health: Kuala Lumpur, Malaysia, 2014. [Google Scholar]
- Institut Kesihatan Umum. Album Makanan Malaysia; Tahir, A., Azli, S.A.B., Nadrah, M.H., Yuhanis Auri, A.K., Nurul Fatihah, H.G., Anim Zakiah, M., Eds.; Institut Kesihatan Umum: Kuala Lumpur, Malaysia, 2011. [Google Scholar]
- Tee, E.S. Nutrition Composition of Malaysian Foods, 4th ed.; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 1997. [Google Scholar]
- Abshirini, M.; Bagheri, F.; Mahaki, B.; Siassi, F.; Koohdani, F.; Safabakhsh, M.; Sotoudeh, G. The dietary acid load is higher in subjects with prediabetes who are at greater risk of diabetes: A case-control study. Diabetol. Metab. Syndr. 2019, 11, 52. [Google Scholar] [CrossRef]
- Ko, B.J.; Chang, Y.; Ryu, S.; Kim, E.M.; Lee, M.Y.; Hyun, Y.Y.; Lee, K.B. Dietary acid load and chronic kidney disease in elderly adults: Protein and potassium intake. PLoS ONE 2017, 12, e0185069. [Google Scholar] [CrossRef] [PubMed]
- Wynn, E.; Lanham-New, S.A.; Krieg, M.A.; Whittamore, D.R.; Burckhardt, P. Low estimates of dietary acid load are positively associated with bone ultrasound in women older than 75 years of age with a lifetime fracture. J. Nutr. 2008, 138, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Frassetto, L.A.; Todd, K.M.; Morris, R.C., Jr.; Sebastian, A. Estimation of net endogenous noncarbonic acid production in humans from diet potassium and protein contents. Am. J. Clin. Nutr. 1998, 68, 576–583. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F. Estimation of the renal net acid excretion by adults consuming diets containing variable amounts of protein. Am. J. Clin. Nutr. 1994, 59, 1356–1361. [Google Scholar] [CrossRef]
- Ho, R. Handbook of Univariate and Multivariate Data Analysis with IBM SPSS; Chapman and Hall/CRC: Boca Raton, FL, USA, 2013. [Google Scholar]
- Weaver, C.; Gordon, C.; Janz, K.; Kalkwarf, H.; Lappe, J.; Lewis, R.; O’Karma, M.; Wallace, T.; Zemel, B.J.O.I. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 2016, 27, 1281–1386. [Google Scholar] [CrossRef]
- Chan, R.; Leung, J.; Woo, J. Association Between Estimated Net Endogenous Acid Production and Subsequent Decline in Muscle Mass Over Four Years in Ambulatory Older Chinese People in Hong Kong: A Prospective Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; New, S.A.; Fraser, W.D.; Campbell, M.K.; Reid, D.M. Low dietary potassium intakes and high dietary estimates of net endogenous acid production are associated with low bone mineral density in premenopausal women and increased markers of bone resorption in postmenopausal women. Am. J. Clin. Nutr. 2005, 81, 923–933. [Google Scholar] [CrossRef]
- Engberink, M.F.; Bakker, S.J.; Brink, E.J.; van Baak, M.A.; van Rooij, F.J.; Hofman, A.; Witteman, J.C.; Geleijnse, J.M. Dietary acid load and risk of hypertension: The Rotterdam Study. Am. J. Clin. Nutr. 2012, 95, 1438–1444. [Google Scholar] [CrossRef]
- Gannon, R.H.; Millward, D.J.; Brown, J.E.; Macdonald, H.M.; Lovell, D.P.; Frassetto, L.A.; Remer, T.; Lanham-New, S.A. Estimates of daily net endogenous acid production in the elderly UK population: Analysis of the National Diet and Nutrition Survey (NDNS) of British adults aged 65 years and over. Br. J. Nutr. 2008, 100, 615–623. [Google Scholar] [CrossRef]
- Soon, J.M.; Tee, E.S. Changing trends in dietary pattern and implications to food and nutrition security in Association of Southeast Asian Nations (ASEAN). Int. J. Nutr. Food Sci. 2014, 3, 259–269. [Google Scholar] [CrossRef]
- Fajar, J.K.; Azharuddin, A. The association between interleukin 6 -174 G/C gene polymorphism and the risk of osteoporosis: A meta-analysis. J. Taibah Univ. Med. Sci. 2017, 12, 212–220. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, J.S.; Suh, K.T.; Eun, I.S. Polymorphism in interleukin-6 gene is associated with bone mineral density in patients with adolescent idiopathic scoliosis. J. Bone Jt. Surg. Br. 2010, 92, 1118–1122. [Google Scholar] [CrossRef][Green Version]
- Zhai, R.; Liu, G.; Yang, C.; Huang, C.; Wu, C.; Christiani, D.C. The G to C polymorphism at -174 of the interleukin-6 gene is rare in a Southern Chinese population. Pharmacogenetics 2001, 11, 699–701. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Wang, Z.; Geng, Y.; Liu, J.; Zhang, R.; Lin, Q.; Li, X.; Huang, D.; Gao, S.; Hu, D.; et al. The association of functional polymorphisms of IL-6 gene promoter with ischemic stroke: Analysis in two Chinese populations. Biochem. Biophys. Res. Commun. 2010, 391, 481–485. [Google Scholar] [CrossRef]
- Meenagh, A.; Williams, F.; Ross, O.A.; Patterson, C.; Gorodezky, C.; Hammond, M.; Leheny, W.A.; Middleton, D. Frequency of cytokine polymorphisms in populations from western Europe, Africa, Asia, the Middle East and South America. Hum. Immunol. 2002, 63, 1055–1061. [Google Scholar] [CrossRef]
- Migita, K.; Miyazoe, S.; Maeda, Y.; Daikoku, M.; Abiru, S.; Ueki, T.; Yano, K.; Nagaoka, S.; Matsumoto, T.; Nakao, K.; et al. Cytokine gene polymorphisms in Japanese patients with hepatitis B virus infection--association between TGF-beta1 polymorphisms and hepatocellular carcinoma. J. Hepatol. 2005, 42, 505–510. [Google Scholar] [CrossRef]
- Gan, G.G.; Subramaniam, R.; Lian, L.H.; Nadarajan, V. Ethnic variation in interleukin-6 -174 (g/c) polymorphism in the malaysian population. Balk. J. Med. Genet. 2013, 16, 53–58. [Google Scholar] [CrossRef]
- Ururahy, M.A.; de Souza, K.S.; Oliveira, Y.M.; Loureiro, M.B.; da Silva, H.P.; Freire-Neto, F.P.; Bezerra, J.F.; Luchessi, A.D.; Doi, S.Q.; Hirata, R.D.; et al. Association of polymorphisms in IL6 gene promoter region with type 1 diabetes and increased albumin-to-creatinine ratio. Diabetes/Metab. Res. Rev. 2015, 31, 500–506. [Google Scholar] [CrossRef]
- Hanai, Y.; Sugita, N.; Wang, Y.; Yoshihara, A.; Iwasaki, M.; Miyazaki, H.; Nakamura, K.; Yoshie, H. Relationships between IL-6 gene polymorphism, low BMD and periodontitis in postmenopausal women. Arch. Oral Biol. 2015, 60, 533–539. [Google Scholar] [CrossRef]
- Yamada, Y.; Ando, F.; Niino, N.; Miki, T.; Shimokata, H. Association of polymorphisms of paraoxonase 1 and 2 genes, alone or in combination, with bone mineral density in community-dwelling Japanese. J. Hum. Genet. 2003, 48, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Ota, N.; Nakajima, T.; Nakazawa, I.; Suzuki, T.; Hosoi, T.; Orimo, H.; Inoue, S.; Shirai, Y.; Emi, M. A nucleotide variant in the promoter region of the interleukin-6 gene associated with decreased bone mineral density. J. Hum. Genet. 2001, 46, 267–272. [Google Scholar] [CrossRef]
- Krieger, N.S.; Sessler, N.E.; Bushinsky, D.A. Acidosis inhibits osteoblastic and stimulates osteoclastic activity in vitro. Am. J. Physiol. 1992, 262, F442–F448. [Google Scholar] [CrossRef]
- Frick, K.K.; Bushinsky, D.A. Effect of metabolic and respiratory acidosis on intracellular calcium in osteoblasts. Am. J. Physiol Ren. Physiol. 2010, 299, F418–F425. [Google Scholar] [CrossRef]
- Fenton, T.R.; Eliasziw, M.; Lyon, A.W.; Tough, S.C.; Hanley, D.A. Meta-analysis of the quantity of calcium excretion associated with the net acid excretion of the modern diet under the acid-ash diet hypothesis. Am. J. Clin. Nutr. 2008, 88, 1159–1166. [Google Scholar] [CrossRef]
- New, S.A.; MacDonald, H.M.; Campbell, M.K.; Martin, J.C.; Garton, M.J.; Robins, S.P.; Reid, D.M. Lower estimates of net endogenous non-carbonic acid production are positively associated with indexes of bone health in premenopausal and perimenopausal women. Am. J. Clin. Nutr. 2004, 79, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Shariati-Bafghi, S.E.; Nosrat-Mirshekarlou, E.; Karamati, M.; Rashidkhani, B. Higher Dietary Acidity is Associated with Lower Bone Mineral Density in Postmenopausal Iranian Women, Independent of Dietary Calcium Intake. Int. J. Vitam. Nutr. Res. 2014, 84, 206–217. [Google Scholar] [CrossRef]
- Kong, S.H.; Kim, J.H.; Hong, A.R.; Lee, J.H.; Kim, S.W.; Shin, C.S. Dietary potassium intake is beneficial to bone health in a low calcium intake population: The Korean National Health and Nutrition Examination Survey (KNHANES) (2008-2011). Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2017, 28, 1577–1585. [Google Scholar] [CrossRef]
- Fenton, T.R.; Tough, S.C.; Lyon, A.W.; Eliasziw, M.; Hanley, D.A. Causal assessment of dietary acid load and bone disease: A systematic review & meta-analysis applying Hill’s epidemiologic criteria for causality. Nutr. J. 2011, 10, 41. [Google Scholar] [CrossRef]
- Kaneshiro, S.; Ebina, K.; Shi, K.; Higuchi, C.; Hirao, M.; Okamoto, M.; Koizumi, K.; Morimoto, T.; Yoshikawa, H.; Hashimoto, J. IL-6 negatively regulates osteoblast differentiation through the SHP2/MEK2 and SHP2/Akt2 pathways in vitro. J. Bone Min. Metab. 2014, 32, 378–392. [Google Scholar] [CrossRef]
- Nguyen, H.T.; von Schoultz, B.; Nguyen, T.V.; Thang, T.X.; Chau, T.T.; Duc, P.T.; Hirschberg, A.L. Sex hormone levels as determinants of bone mineral density and osteoporosis in Vietnamese women and men. J. Bone Miner. Metab. 2015, 33, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.W.; Seo, J.S.; Hur, S.E.; Kim, H.L.; Kim, J.Y.; Jung, J.H.; Kim, L.H.; Park, B.L.; Shin, H.D. Association of interleukin-6 promoter variant with bone mineral density in pre-menopausal women. J. Hum. Genet. 2003, 48, 243–248. [Google Scholar] [CrossRef]
- Berardi, J.M.; Logan, A.C.; Rao, A.V. Plant based dietary supplement increases urinary pH. J. Int. Soc. Sports Nutr. 2008, 5, 20. [Google Scholar] [CrossRef]
- Dargent-Molina, P.; Sabia, S.; Touvier, M.; Kesse, E.; Breart, G.; Clavel-Chapelon, F.; Boutron-Ruault, M.C. Proteins, dietary acid load, and calcium and risk of postmenopausal fractures in the E3N French women prospective study. J. Bone Min. Res. 2008, 23, 1915–1922. [Google Scholar] [CrossRef]
- Garcia, A.H.; Franco, O.H.; Voortman, T.; de Jonge, E.A.; Gordillo, N.G.; Jaddoe, V.W.; Rivadeneira, F.; van den Hooven, E.H. Dietary acid load in early life and bone health in childhood: The Generation R Study. Am. J. Clin. Nutr. 2015, 102, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Jafar, T.; Mahdi, F.; Arshad, M.; Das, S.K.; Waliullah, S.; Mahdi, A.A. Association of Vitamin D Receptor (FokI and BsmI) Gene Polymorphism with Bone Mineral Density and Their Effect on 25-Hydroxyvitamin D Level in North Indian Postmenopausal Women with Osteoporosis. Indian J. Clin. Biochem. 2018, 33, 429–437. [Google Scholar] [CrossRef]
- Geng, L.; Yao, Z.; Yang, H.; Luo, J.; Han, L.; Lu, Q. Association of CA repeat polymorphism in estrogen receptor beta gene with postmenopausal osteoporosis in Chinese. J. Genet. Genom. Yi Chuan Xue Bao 2007, 34, 868–876. [Google Scholar] [CrossRef]
- Sun, J.; Zhang, C.; Xu, L.; Yang, M.; Yang, H. The transforming growth factor-β1 (TGF-β1) gene polymorphisms (TGF-β1 T869C and TGF-β1 T29C) and susceptibility to postmenopausal osteoporosis: A meta-analysis. Medicine 2015, 94, e461. [Google Scholar] [CrossRef]
- Lim, H.S.; Park, Y.H.; Kim, S.K. Relationship between Serum Inflammatory Marker and Bone Mineral Density in Healthy Adults. J. Bone Metab. 2016, 23, 27–33. [Google Scholar] [CrossRef]
- Huang, J.; Lin, D.; Wei, Z.; Li, Q.; Zheng, J.; Zheng, Q.; Cai, L.; Li, X.; Yuan, Y.; Li, J. Parathyroid Hormone Derivative with Reduced Osteoclastic Activity Promoted Bone Regeneration via Synergistic Bone Remodeling and Angiogenesis. Small 2020, 16, e1905876. [Google Scholar] [CrossRef] [PubMed]
- Wein, M.N. Parathyroid Hormone Signaling in Osteocytes. JBMR Plus 2018, 2, 22–30. [Google Scholar] [CrossRef]
- Wein, M.N.; Kronenberg, H.M. Regulation of Bone Remodeling by Parathyroid Hormone. Cold Spring Harb. Perspect. Med. 2018, 8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) | Mean ± SD | |
|---|---|---|
| Social demographics | ||
| Age (year) | 67 ± 7 | |
| Years of menopause (year) | 16 ± 8 | |
| Educational level (years) | 8 ± 5 | |
| Anthropometrics | ||
| Weight (kg) | 57.91 ± 9.6 | |
| Height (m) | 1.54 ± 0.1 | |
| Waist circumference (cm) | 80.3 ± 9.1 | |
| Body fat percentage (%) | 35.1 ± 5.2 | |
| BMI (kg/m2) | 24.3 ± 3.8 | |
| Underweight (<18.5) | 10 (5.0) | |
| Normal (18.5–24.9) | 113 (55.9) | |
| Overweight (25.0–29.9) | 64 (31.7) | |
| Obese (≥ 30) | 15 (7.4) | |
| Lifestyles | ||
| Physical activity (MET-min/week) | ||
| Below recommendation (<600 MET) | 77 (37.9) | |
| Meeting recommendation (≥600 MET) | 126 (62.1) | |
| NEAP score (mEq/day) | 72.8 ± 28.7 | |
| Normal (<72.8) | 114 (56.2) | |
| Elevated (≥72.8) | 89 (43.8) | |
| Biochemical analysis | ||
| Fasting blood glucose (mmol/L) | 5.89 ± 0.93 | |
| Serum of 25(OH)D (nmol/L) | ||
| Deficiency (<30) | 66 (32.5) | |
| Inadequate (30–50) | 100 (49.3) | |
| Adequate (>50) | 37 (18.2) | |
| CTX-1 (ng/mL) | 0.445 ± 0.198 | |
| Normal (<0.445) | 116 (57.1) | |
| Elevated (≥0.445) | 87 (42.9) | |
| Genetic analysis | ||
| IL6 gene -174G/C (genotype) | ||
| CC | 0 | |
| CG | 0 | |
| GG | 203 (100) | |
| IL6 gene -572G/C (genotype) | ||
| GG | 5 (2.5) | |
| CG | 84 (41.4) | |
| CC | 114 (56.1) |
| r | p | |
|---|---|---|
| NEAP | 0.084 | 0.24 |
| Age (year) | −0.189 | 0.01 * |
| Height (m) | 0.133 | 0.06 |
| Serum of 25(OH)D (nmol/L) | −0.105 | 0.14 |
| Educational level (year) | 0.108 | 0.13 |
| Fasting blood glucose (mmol/L) | −0.101 | 0.15 |
| Waist circumference (cm) | −0.098 | 0.16 |
| IL6 rs1800796 | ||||
|---|---|---|---|---|
| GG + CG (n = 89) | CC (n = 114) | t-test | p | |
| Social demographics | ||||
| Age (year) | 65.91 ± 5.7 | 67.17 ± 7.1 | −1.36 | 0.18 |
| Years of menopause (year) | 15.47 ± 6.8 | 16.63 ± 8.4 | −1.08 | 0.28 |
| Marital status | ||||
| Single | 8 (9) | 10 (8.8) | ||
| Married | 67 (75.3) | 90 (78.9) | ||
| Divorced | 2 (2.2) | 4 (3.5) | ||
| Others (widow or widower) | 12 (13.5) | 10 (8.8) | ||
| Educational level (years) | 8.54 ± 4.7 | 7.45 ± 4.5 | 1.24 | 0.22 |
| Anthropometrics | ||||
| Weight (kg) | 57.23 ± 9.4 | 58.44 ± 9.8 | −0.883 | 0.38 |
| Height (m) | 1.54 ± 0.1 | 1.54 ± 0.1 | 0.155 | 0.88 |
| Waist circumference (cm) | 79.74 ± 8.7 | 80.72 ± 9.4 | −0.753 | 0.45 |
| Body fat percentage (%) | 34.96 ± 5.5 | 35.26 ± 5.04 | −0.400 | 0.69 |
| BMI (kg/m2) | 24.1 ± 3.7 | 24.5 ± 3.9 | −0.628 | 0.53 |
| Lifestyles factors | ||||
| Physical activity (MET-min/week) | ||||
| Below recommendation (<600 MET) | 30 (33.7) | 47 (41.2) | ||
| Meeting recommendation (≥600 MET) | 59 (66.3) | 67 (58.8) | ||
| NEAP (mEq/day) | 74.97 ± 29.4 | 71.12 ± 28.2 | 0.945 | 0.35 |
| Biochemical analysis | ||||
| Fasting blood glucose (mmol/L) | 5.92 ± 0.95 | 5.87 ± 0.9 | 0.397 | 0.69 |
| Serum of 25(OH) D (nmol/L) | ||||
| Deficiency | 28 (31.5) | 38 (33.3) | ||
| Inadequate | 44 (49.4) | 56 (49.1) | ||
| Adequate | 17 (19.1) | 20 (17.5) | ||
| CTX-1 (ng/mL) | 0.42 ± 0.19 | 0.46 ± 0.21 | −1.54 | 0.12 |
| Variables | Step 1 | Step 2 | Step 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Beta | t | p | Beta | t | p | Beta | t | p | |
| Age (year) | −0.143 | −1.91 | 0.057 | −0.168 | −2.26 | 0.025 | −0.166 | −2.21 | 0.028 |
| Height (m) | 0.083 | 1.16 | 0.25 | 0.083 | 1.17 | 0.24 | 0.084 | 1.19 | 0.24 |
| Serum of 25(OH)D (nmol/L) | −0.108 | −1.54 | 0.13 | −0.114 | −1.64 | 0.10 | −0.115 | −1.64 | 0.10 |
| Educational level (years) | 0.036 | 0.494 | 0.62 | 0.072 | 0.978 | 0.33 | 0.075 | 1.004 | 0.32 |
| Fasting blood glucose (mmol/L) | −0.053 | −0.728 | 0.47 | −0.058 | −0.797 | 0.43 | −0.055 | −0.756 | 0.45 |
| Waist circumference (cm) | −0.077 | −1.03 | 0.30 | −0.079 | −1.07 | 0.28 | −0.080 | −1.09 | 0.28 |
| NEAP (mEq/day) | 0.153 | 2.18 | 0.031 | 0.173 | 1.66 | 0.098 | |||
| IL6 gene -572G/C (GG + CG = 0, CC = 1) | 0.140 | 2.03 | 0.044 | 0.188 | 0.977 | 0.33 | |||
| NEAP x IL6 gene -572G/C | −0.054 | −0.266 | 0.79 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.Y.; Chan, Y.M.; Ramachandran, V.; Shariff, Z.M.; Chin, Y.S.; Arumugam, M. No Interaction Effect between Interleukin-6 Polymorphisms and Acid Ash Diet with Bone Resorption Marker in Postmenopausal Women. Int. J. Environ. Res. Public Health 2021, 18, 827. https://doi.org/10.3390/ijerph18020827
Lim SY, Chan YM, Ramachandran V, Shariff ZM, Chin YS, Arumugam M. No Interaction Effect between Interleukin-6 Polymorphisms and Acid Ash Diet with Bone Resorption Marker in Postmenopausal Women. International Journal of Environmental Research and Public Health. 2021; 18(2):827. https://doi.org/10.3390/ijerph18020827
Chicago/Turabian StyleLim, Sook Yee, Yoke Mun Chan, Vasudevan Ramachandran, Zalilah Mohd Shariff, Yit Siew Chin, and Manohar Arumugam. 2021. "No Interaction Effect between Interleukin-6 Polymorphisms and Acid Ash Diet with Bone Resorption Marker in Postmenopausal Women" International Journal of Environmental Research and Public Health 18, no. 2: 827. https://doi.org/10.3390/ijerph18020827
APA StyleLim, S. Y., Chan, Y. M., Ramachandran, V., Shariff, Z. M., Chin, Y. S., & Arumugam, M. (2021). No Interaction Effect between Interleukin-6 Polymorphisms and Acid Ash Diet with Bone Resorption Marker in Postmenopausal Women. International Journal of Environmental Research and Public Health, 18(2), 827. https://doi.org/10.3390/ijerph18020827