Impact of Environmental Injustice on Children’s Health—Interaction between Air Pollution and Socioeconomic Status


{kind=link}
Abstract
1. Introduction
2. Impact of Environmental Injustice on Children’s Health
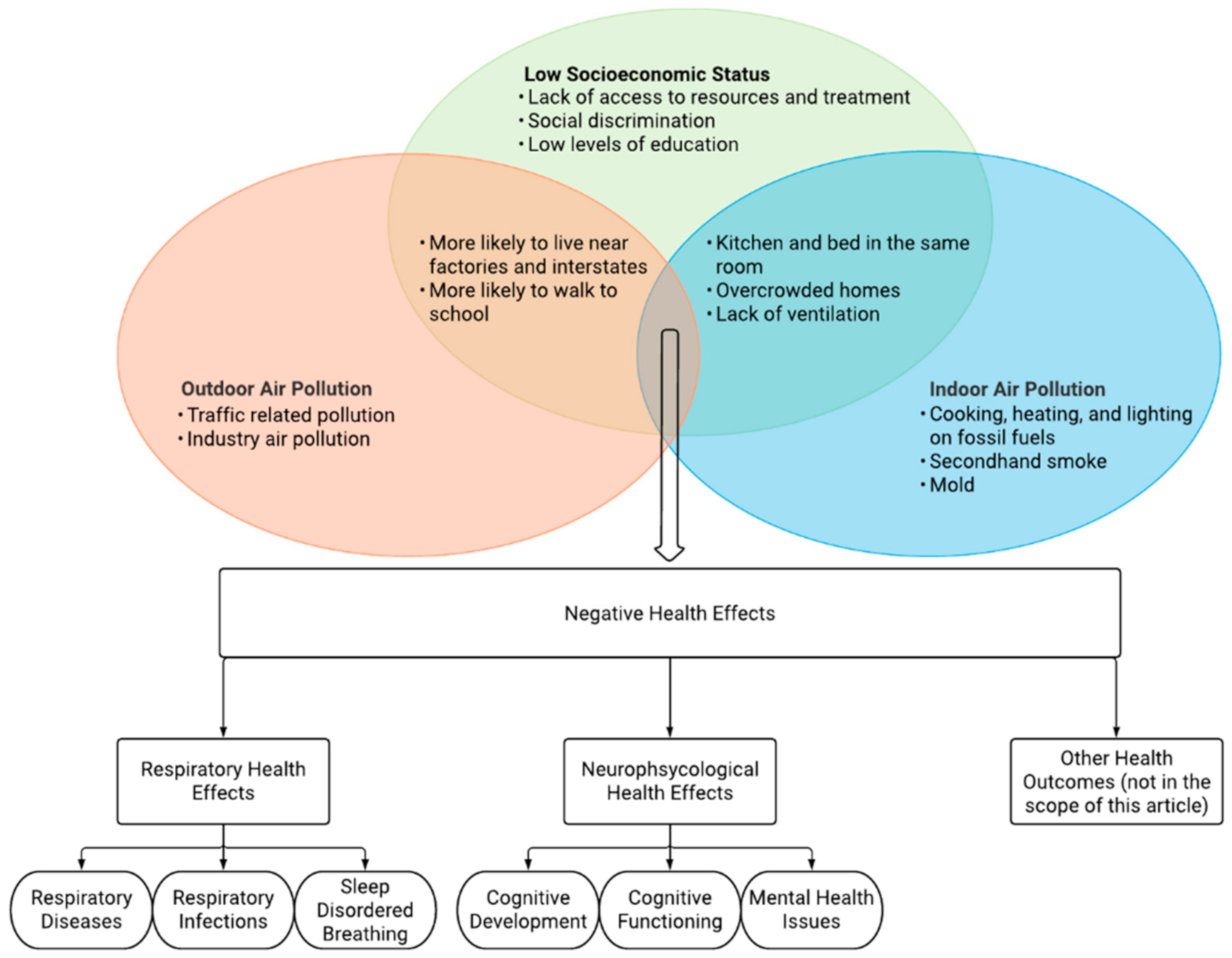
2.1. Socioeconomic Status
2.2. Air Pollution
2.2.1. Outdoor Air Pollution
2.2.2. Indoor Air Pollution
3. Biological Mechanisms
4. Discussion
4.1. Social and Racial Discrimination
4.2. Adulthood and Transgenerational Effects
4.3. Climate Change
5. Conclusions/Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xing, J.; Mathur, R.; Pleim, J.E.; Wang, S.; Hogrefe, C.; Gan, C.-M.; Wong, D.C.; Hao, J. Historical Trends in PM2.5-Related Premature Mortality during 1990–2010 across the Northern Hemisphere. Environ. Health Perspect. 2017, 125, 400–408. [Google Scholar] [CrossRef]
- Orru, H.; Ebi, K.L.; Forsberg, B. The Interplay of Climate Change and Air Pollution on Health. Curr. Environ. Health Rep. 2017, 4, 504–513. [Google Scholar] [CrossRef]
- La Grutta, S.; Indinnimeo, L.; Di Coste, A.; Ferrante, G.; Landi, M.; Pelosi, U.; Rusconi, F. Environmental risk factors and lung diseases in children: From guidelines to health effects. Early Hum. Dev. 2013, 89, S59–S62. [Google Scholar] [CrossRef]
- Forns, J.; Dadvand, P.; Esnaola, M.; Alvarez-Pedrerol, M.; López-Vicente, M.; Garcia-Esteban, R.; Cirach, M.; Basagaña, X.; Guxens, M.; Sunyer, J. Longitudinal association between air pollution exposure at school and cognitive development in school children over a period of 3.5 years. Environ. Res. 2017, 159, 416–421. [Google Scholar] [CrossRef]
- Roberts, S.; Arseneault, L.; Barratt, B.; Beevers, S.D.; Danese, A.; Odgers, C.L.; Moffitt, T.E.; Reuben, A.; Kelly, F.J.; Fisher, H.L. Exploration of NO2 and PM2.5 air pollution and mental health problems using high-resolution data in London-based children from a UK longitudinal cohort study. Psychiatry Res. 2019, 272, 8–17. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Rauh, V.A.; Galvez, M.P. Environmental Justice and the Health of Children. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2010, 77, 178–187. [Google Scholar] [CrossRef]
- Niessen, L.; Mohan, D.; Akuoku, J.K.; Mirelman, A.J.; Ahmed, S.; Koehlmoos, T.P.; Trujillo, A.; Khan, J.; Peters, D.H. Tackling socioeconomic inequalities and non-communicable diseases in low-income and middle-income countries under the Sustainable Development agenda. Lancet 2018, 391, 2036–2046. [Google Scholar] [CrossRef]
- Starfield, B.; Gérvas, J.; Mangin, D. Clinical Care and Health Disparities. Annu. Rev. Public Health 2012, 33, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Subramanian, S.V.; Almeida-Filho, N. A glossary for health inequalities. J. Epidemiol. Community Health 2002, 56, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free. Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Hajat, A.; Hsia, C.; O’Neill, M.S. Socioeconomic Disparities and Air Pollution Exposure: A Global Review. Curr. Environ. Health Rep. 2015, 2, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Liu, S.; Hou, X.; Sun, Y.; Beazley, R. Air pollution and cause-specific mortality: A comparative study of urban and rural areas in China. Chemosphere 2021, 262, 127884. [Google Scholar] [CrossRef]
- Salvi, S. Health effects of ambient air pollution in children. Paediatr. Respir. Rev. 2007, 8, 275–280. [Google Scholar] [CrossRef]
- Landrigan, P.J. Children as a vulnerable population. Int. J. Occup. Med. Environ. Health 2004, 17, 175–177. [Google Scholar] [CrossRef]
- Das, J.; Mohpal, A. Socioeconomic Status and Quality of Care In Rural India: New Evidence From Provider And Household Surveys. Health Aff. 2016, 35, 1764–1773. [Google Scholar] [CrossRef]
- Landi, S.; Ivaldi, E.; Testi, A. Socioeconomic status and waiting times for health services: An international literature review and evidence from the Italian National Health System. Health Policy 2018, 122, 334–351. [Google Scholar] [CrossRef]
- Arpey, N.C.; Gaglioti, A.H.; Rosenbaum, M.E. How Socioeconomic Status Affects Patient Perceptions of Health Care: A Qualitative Study. J. Prim. Care Community Health 2017, 8, 169–175. [Google Scholar] [CrossRef]
- Togunde, D.; Carter, A. Socioeconomic causes of child labor in urban Nigeria. J. Child. Poverty 2006, 12, 73–89. [Google Scholar] [CrossRef]
- A Bhutta, Z.; Berkley, J.A.; Bandsma, R.H.; Kerac, M.; Trehan, I.; Briend, A. Severe childhood malnutrition. Nat. Rev. Dis. Prim. 2017, 3, 1–18. [Google Scholar] [CrossRef]
- Shankar, P.; Chung, R.; Frank, D.A. Association of Food Insecurity with Childrenʼs Behavioral, Emotional, and Academic Outcomes. J. Dev. Behav. Pediatr. 2017, 38, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A.; Vu, C. Understanding how discrimination can affect health. Health Serv. Res. 2019, 54, 1374–1388. [Google Scholar] [CrossRef] [PubMed]
- Rickenbacker, H.; Brown, F.; Bilec, M.M. Creating environmental consciousness in underserved communities: Implementation and outcomes of community-based environmental justice and air pollution research. Sustain. Cities Soc. 2019, 47, 101473. [Google Scholar] [CrossRef]
- Martin, W.J.; Glass, R.I.; Araj, H.; Balbus, J.; Collins, F.S.; Curtis, S.; Diette, G.B.; Elwood, W.N.; Falk, H.; Hibberd, P.L.; et al. Household Air Pollution in Low- and Middle-Income Countries: Health Risks and Research Priorities. PLoS Med. 2013, 10, e1001455. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef]
- Barnett, A.G.; Williams, G.M.; Schwartz, J.; Neller, A.H.; Best, T.L.; Petroeschevsky, A.L.; Simpson, R.W. Air Pollution and Child Respiratory Health. Am. J. Respir. Crit. Care Med. 2005, 171, 1272–1278. [Google Scholar] [CrossRef]
- Sánchez, T.; Gozal, D.; Smith, D.L.; Foncea, C.; Betancur, C.; Brockmann, P. Association between air pollution and sleep disordered breathing in children. Pediatr. Pulmonol. 2019, 54, 544–550. [Google Scholar] [CrossRef]
- Yuan, R.; Wang, J.; Guo, L.-L. The Effect of Sleep Deprivation on Coronary Heart Disease. Chin. Med Sci. J. 2016, 31, 247–253. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Malaspina, D.; Boden-Albala, B.; Heymsfield, S.B. Inadequate Sleep as a Risk Factor for Obesity: Analyses of the NHANES I. Sleep 2005, 28, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.L.; Oberdorster, G.; Morris-Schaffer, K.; Wong, C.; Klocke, C.; Sobolewski, M.; Conrad, K.; Mayerproschel, M.; A Coryslechta, D. Developmental neurotoxicity of inhaled ambient ultrafine particle air pollution: Parallels with neuropathological and behavioral features of autism and other neurodevelopmental disorders. NeuroToxicology 2017, 59, 140–154. [Google Scholar] [CrossRef] [PubMed]
- Bugueño, M.; Curihual, C.; Olivares, P.; Wallace, J.; López-Alegría, F.; Rivera-López, G.; Oyanedel, J.C. Calidad de sueño y rendimiento académico en alumnos de educación secundaria. Rev. Med. Chile 2017, 145, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Beckwith, T.J.; Cecil, K.; Altaye, M.; Severs, R.; Wolfe, C.; Percy, Z.; Maloney, T.; Yolton, K.; Lemasters, G.; Brunst, K.; et al. Reduced gray matter volume and cortical thickness associated with traffic-related air pollution in a longitudinally studied pediatric cohort. PLoS ONE 2020, 15, e0228092. [Google Scholar] [CrossRef]
- Sunyer, J.; Esnaola, M.; Alvarez-Pedrerol, M.; Forns, J.; Rivas, I.; López-Vicente, M.; Suades-González, E.; Foraster, M.; Garcia-Esteban, R.; Basagaña, X.; et al. Association between Traffic-Related Air Pollution in Schools and Cognitive Development in Primary School Children: A Prospective Cohort Study. PLoS Med. 2015, 12, e1001792. [Google Scholar] [CrossRef]
- Ritz, B.; Liew, Z.; Yan, Q.; Cuia, X.; Virk, J.; Ketzel, M.; Raaschou-Nielsen, O. Air pollution and autism in Denmark. Environ. Epidemiol. 2018, 2, e028. [Google Scholar] [CrossRef]
- Chun, H.; Leung, C.; Wen, S.W.; McDonald, J.; Shin, H.H. Maternal exposure to air pollution and risk of autism in children: A systematic review and meta-analysis. Environ. Pollut. 2020, 256, 113307. [Google Scholar] [CrossRef]
- Park, J.; Sohn, J.H.; Cho, S.J.; Seo, H.Y.; Hwang, I.-U.; Hong, Y.-C.; Kim, K.-N. Association between short-term air pollution exposure and attention-deficit/hyperactivity disorder-related hospital admissions among adolescents: A nationwide time-series study. Environ. Pollut. 2020, 266, 115369. [Google Scholar] [CrossRef]
- Shih, P.; Huang, C.-C.; Pan, S.-C.; Chiang, T.-L.; Guo, Y.L. Hyperactivity disorder in children related to traffic-based air pollution during pregnancy. Environ. Res. 2020, 188, 109588. [Google Scholar] [CrossRef]
- Su, J.G.; Jerrett, M.; McConnell, R.; Berhane, K.; Dunton, G.; Shankardass, K.; Reynolds, K.; Chang, R.; Wolch, J. Factors influencing whether children walk to school. Health Place 2013, 22, 153–161. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K.; Peng, R.D.; Dominici, F. Adverse Health Effects of Particulate Air Pollution. Epidemiology 2009, 20, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Loucaides, C.A.; Chedzoy, S.M.; Bennett, N. Differences in physical activity levels between urban and rural school children in Cyprus. Health Educ. Res. 2004, 19, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Rana, J.; Uddin, J.; Peltier, R.E.; Oulhote, Y. Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter? Int. J. Environ. Res. Public Health 2019, 16, 2910. [Google Scholar] [CrossRef] [PubMed]
- Vanker, A.; Barnett, W.; Workman, L.; Nduru, P.M.; Sly, P.D.; Gie, R.P.; Zar, H.J. Early-life exposure to indoor air pollution or tobacco smoke and lower respiratory tract illness and wheezing in African infants: A longitudinal birth cohort study. Lancet Planet. Health 2017, 1, e328–e336. [Google Scholar] [CrossRef]
- Budhathoki, S.S.; Tinkari, B.S.; Bhandari, A.; Dhimal, M.; Zhou, H.; Ghimire, A.; Basnet, O.; Wrammert, J.; Kc, A. The Association of Childhood Pneumonia with Household Air Pollution in Nepal: Evidence from Nepal Demographic Health Surveys. Matern. Child Health J. 2020, 24 (Suppl. 1), 48–56. [Google Scholar] [CrossRef]
- Huels, A.; Vanker, A.; Gray, D.; Koen, N.; MacIsaac, J.L.; Lin, D.T.; Ramadori, K.E.; Sly, P.D.; Stein, D.J.; Kobor, M.S.; et al. Genetic susceptibility to asthma increases the vulnerability to indoor air pollution. Eur. Respir. J. 2020, 55, 1901831. [Google Scholar] [CrossRef]
- Chaudhuri, N. Interventions to improve children’s health by improving the housing environment. Rev. Environ. Health 2005, 19, 197–222. [Google Scholar]
- Fiorito, G.; Vlaanderen, J.; Polidoro, S.; Gulliver, J.; Galassi, C.; Ranzi, A.; Krogh, V.; Grioni, S.; Agnoli, C.; Sacerdote, C.; et al. Oxidative stress and inflammation mediate the effect of air pollution on cardio- and cerebrovascular disease: A prospective study in nonsmokers. Environ. Mol. Mutagen. 2018, 59, 234–246. [Google Scholar] [CrossRef]
- Pope, C.A.; Bhatnagar, A.; McCracken, J.P.; Abplanalp, W.; Conklin, D.J.; O’Toole, T. Exposure to Fine Particulate Air Pollution Is Associated With Endothelial Injury and Systemic Inflammation. Circ. Res. 2016, 119, 1204–1214. [Google Scholar] [CrossRef]
- Huels, A.; Krämer, U.; Herder, C.; Fehsel, K.; Luckhaus, C.; Stolz, S.; Vierkötter, A.; Schikowski, T. Genetic susceptibility for air pollution-induced airway inflammation in the SALIA study. Environ. Res. 2017, 152, 43–50. [Google Scholar] [CrossRef]
- Vossoughi, M.; Schikowski, T.; Vierkötter, A.; Sugiri, D.; Hoffmann, B.; Teichert, T.; Herder, C.; Schulte, T.; Luckhaus, C.; Raulf-Heimsoth, M.; et al. Air pollution and subclinical airway inflammation in the SALIA cohort study. Immun. Ageing 2014, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Han, Y.; Chen, W.; Wang, Y.; Qiu, X.; Li, W.; Hu, M.; Wu, Y.; Wang, Q.; Zhang, H.; et al. Respiratory Inflammation and Short-Term Ambient Air Pollution Exposures in Adult Beijing Residents with and without Prediabetes: A Panel Study. Environ. Health Perspect. 2020, 128, 067004. [Google Scholar] [CrossRef] [PubMed]
- Hiltermann, T.J.N.; De Bruijne, C.R.; Stolk, J.; Zwinderman, A.H.; Spieksma, F.T.M.; Roemer, W.; Steerenberg, P.A.; Fischer, P.H.; Van Bree, L.; Hiemstra, P.S. Effects of Photochemical Air Pollution and Allergen Exposure on Upper Respiratory Tract Inflammation in Asthmatics. Am. J. Respir. Crit. Care Med. 1997, 156, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Block, M.L.; Calderón-Garcidueñas, L. Air pollution: Mechanisms of neuroinflammation and CNS disease. Trends Neurosci. 2009, 32, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Olvera-Álvarez, H.A.; Kubzansky, L.D.; Campen, M.J.; Slavich, G.M. Early life stress, air pollution, inflammation, and disease: An integrative review and immunologic model of social-environmental adversity and lifespan health. Neurosci. Biobehav. Rev. 2018, 92, 226–242. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, M.A.; Harrell, H.L.; Marchant, G.E. Transgenerational epigenetics and environmental justice. Environ. Epigenet. 2017, 3, 1–12. [Google Scholar] [CrossRef]
- Rider, C.F.; Carlsten, C. Air pollution and DNA methylation: Effects of exposure in humans. Clin. Epigenet. 2019, 11, 1–15. [Google Scholar] [CrossRef]
- Amigo, H.; Ale, D.; Varela, N.; Peruga, A.; Bustos, P. Patrón de tabaquismo y nivel socioeconómico en dos cohortes de adultos jóvenes. Rev. Med. Chile 2018, 146, 168–174. [Google Scholar] [CrossRef]
- Jiang, C.-L.; He, S.-W.; Zhang, Y.-D.; Duan, H.-X.; Huang, T.; Huang, Y.-C.; Li, G.-F.; Wang, P.; Ma, L.-J.; Zhou, G.-B.; et al. Air pollution and DNA methylation alterations in lung cancer: A systematic and comparative study. Oncotarget 2017, 8, 1369–1391. [Google Scholar] [CrossRef]
- Lee, M.K.; Xu, C.J.; Carnes, M.U.; Nichols, C.E.; Ward, J.M.; Kwon, S.O.; Kim, S.Y.; Kim, W.J.; London, S.J. Genome-wide DNA methylation and long-term ambient air pollution exposure in Korean adults. Clin. Epigenet. 2019, 11, 37. [Google Scholar] [CrossRef]
- Vukojević, M.; Zovko, A.; Talić, I.; Tanović, M.; Resić, B.; Vrdoljak, I.; Splavski, B. Parental Socioeconomic Status as a Predictor of Physical and Mental Health Outcomes In Children—Literature Review. Acta Clin. Croat. 2017, 56, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Patki, G.; Solanki, N.; Atrooz, F.; Allam, F.; Salim, S. Depression, anxiety-like behavior and memory impairment are associated with increased oxidative stress and inflammation in a rat model of social stress. Brain Res. 2013, 1539, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R. Race, Socioeconomic Status, and Health The Added Effects of Racism and Discrimination. Ann. N. Y. Acad. Sci. 1999, 896, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.L.; Airhihenbuwa, C.O. Critical Race Theory, Race Equity, and Public Health: Toward Antiracism Praxis. Am. J. Public Health 2010, 100, S30–S35. [Google Scholar] [CrossRef] [PubMed]
- Dubrowski, A.; Kliś, K.; Żurawiecka, M.; Dereń, K.; Barszcz, M.; Nowakowski, D.; Wronka, I. Long-Term Exposure to Ambient Air Pollution in Childhood-Adolescence and Lung Function in Adulthood. Adv. Exp. Med. Biol. 2019, 1113, 19–26. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Roux, A.V.D.; Hoffman, E.A.; Kawut, S.M.; Jacobs, D.R.; Barr, R.G. Association of Environmental Tobacco Smoke Exposure in Childhood With Early Emphysema in Adulthood Among Nonsmokers: The MESA-Lung Study. Am. J. Epidemiol. 2010, 171, 54–62. [Google Scholar] [CrossRef]
- Anyamele, O.D. Urban and Rural Differences Across Countries in Child Mortality in Sub-Saharan Africa. J. Health Care Poor Underserved 2009, 20 (Suppl. 4), 90–98. [Google Scholar] [CrossRef]
- Ebi, K.L.; Ogden, N.H.; Semenza, J.C.; Woodward, A. Detecting and Attributing Health Burdens to Climate Change. Environ. Health Perspect. 2017, 125, 085004. [Google Scholar] [CrossRef]
- D’Amato, G.; Holgate, S.T.; Panwankar, R.; Ledford, D.K.; Cecchi, L.; Al-Ahmad, M.; Al-Enezi, F.; Al-Muhsen, S.; Ansotegui, I.; Baena-Cagnani, C.E.; et al. Meteorological conditions, climate change, new emerging factors, and asthma and related allergic disorders. A statement of the World Allergy Organization. World Allergy Organ. J. 2015, 8, 25–52. [Google Scholar] [CrossRef]
- Feng, X.; Wei, S.; Wang, S. Temperature inversions in the atmospheric boundary layer and lower troposphere over the Sichuan Basin, China: Climatology and impacts on air pollution. Sci. Total. Environ. 2020, 726, 138579. [Google Scholar] [CrossRef]
- Ziegler, C.; Morelli, V.; Fawibe, O. Climate Change and Underserved Communities. Prim. Care 2017, 44, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Di Cicco, M.; Ferrante, G.; Amato, D.; Capizzi, A.; De Pieri, C.; Ferraro, V.A.; Furno, M.; Tranchino, V.; La Grutta, S. Climate Change and Childhood Respiratory Health: A Call to Action for Paediatricians. Int. J. Environ. Res. Public Health 2020, 17, 5344. [Google Scholar] [CrossRef] [PubMed]
- Zuurbier, M.; Lundqvist, C.; Salines, G.; Stansfeld, S.; Hanke, W.; Babisch, W.; Bistrup, M.; Hazel, P.V.D.; Moshammer, H. The Environmental Health of Children: Priorities in Europe. Int. J. Occup. Med. Environ. Health 2007, 20, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Hazel, P.V.D.; Zuurbier, M.; Bistrup, M.L.; Busby, C.; Fučić, A.; Koppe, J.G.; Lundqvist, C.; Ronchetti, R.; Tusscher, G.T. Policy and science in children’s health and environment: Recommendations from the PINCHE project. Acta Paediatr. 2006, 95, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Hazel, P.V.D.; Zuurbier, M.; Bistrup, M.L. Policy interpretation network on children’s health and environment. Acta Paediatr. 2006, 95, 6–12. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathiarasan, S.; Hüls, A. Impact of Environmental Injustice on Children’s Health—Interaction between Air Pollution and Socioeconomic Status. Int. J. Environ. Res. Public Health 2021, 18, 795. https://doi.org/10.3390/ijerph18020795
Mathiarasan S, Hüls A. Impact of Environmental Injustice on Children’s Health—Interaction between Air Pollution and Socioeconomic Status. International Journal of Environmental Research and Public Health. 2021; 18(2):795. https://doi.org/10.3390/ijerph18020795
Chicago/Turabian StyleMathiarasan, Sahana, and Anke Hüls. 2021. "Impact of Environmental Injustice on Children’s Health—Interaction between Air Pollution and Socioeconomic Status" International Journal of Environmental Research and Public Health 18, no. 2: 795. https://doi.org/10.3390/ijerph18020795
APA StyleMathiarasan, S., & Hüls, A. (2021). Impact of Environmental Injustice on Children’s Health—Interaction between Air Pollution and Socioeconomic Status. International Journal of Environmental Research and Public Health, 18(2), 795. https://doi.org/10.3390/ijerph18020795