Ethylene Oxide Exposure in U.S. Populations Residing Near Sterilization and Other Industrial Facilities: Context Based on Endogenous and Total Equivalent Concentration Exposures

Abstract
1. Introduction
- Development of distribution of percentiles of the nonsmoking general population endogenous equivalent concentrations and total equivalent concentrations.
- Characterization of recently measured ambient EO concentrations in the vicinity of sterilization and other EO emitting facilities and at corresponding representative background sites to assess exogenous exposure concentration above background levels.
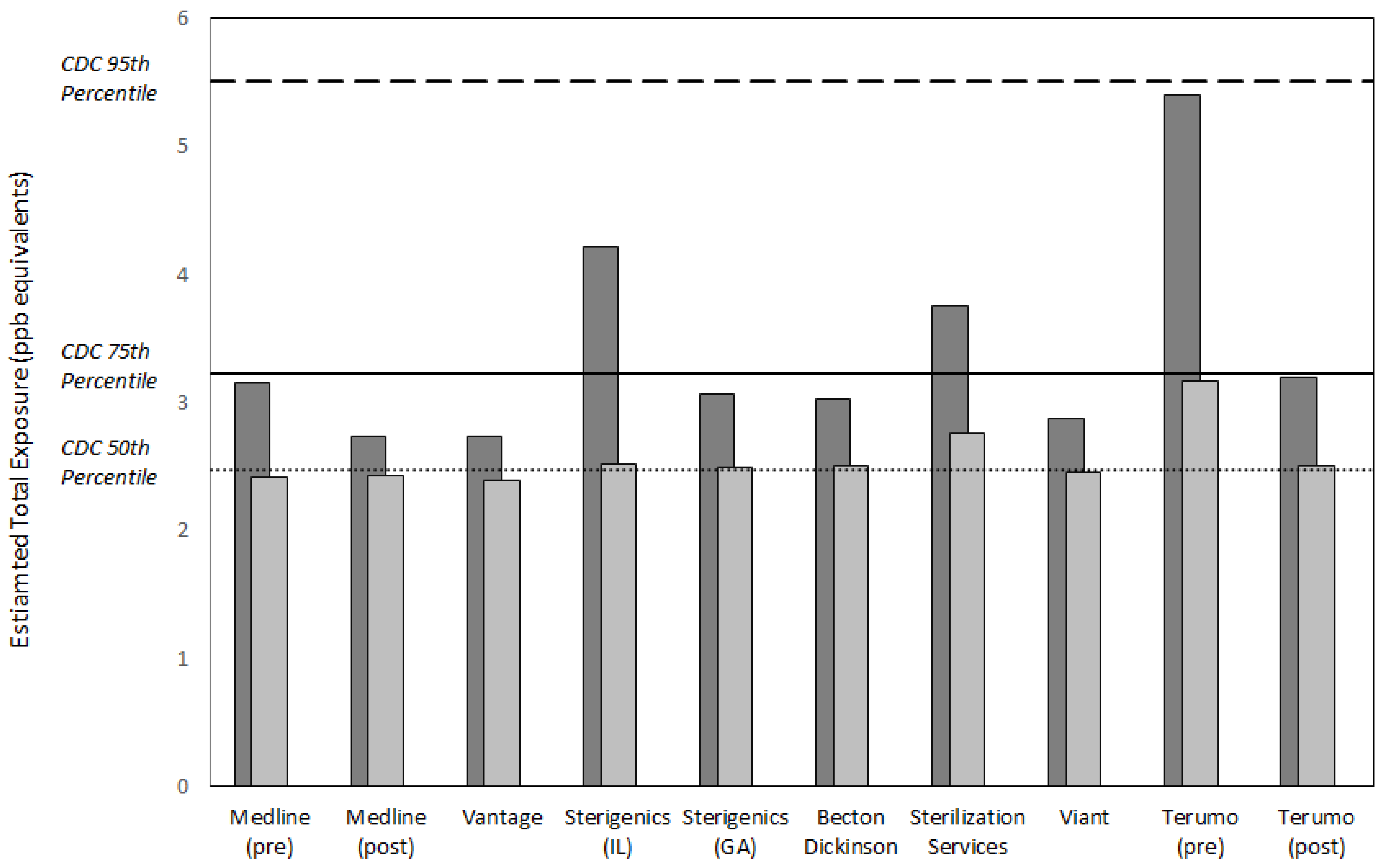
- Assessment of the relative importance of excess EO concentrations in the vicinity of emitting facilities by comparing a central tendency or upper bound ambient air EO concentration added to the general population 50th percentile endogenous equivalent concentration, measures of total exposure, to the normal percentile range of nonsmoking general population total equivalent concentrations.
2. Materials and Methods
2.1. Equivalent Exposure Concentrations
2.2. EO Concentrations in Ambient Air Near Emitting U.S. Facilities and Associated Background Locations
2.2.1. Available Data
2.2.2. EO Collection and Analytical Methods Applied to EO Monitoring
2.2.3. Statistical Methods
2.3. Comparing EO Exposure Concentrations to Endogenous Equivalent Concentration Benchmarks
3. Results
3.1. Total Equivalent and Endogenous Equivalent Concentrations
3.2. Facility Vicinity and Background EO Concentrations
3.3. National Background and Local Background EO Concentrations
3.4. Risk Management Context for Near Facility Potential Population Exposure Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Environmental Protection Agency. Evaluation of the Inhalation Carcinogenicity of Ethylene Oxide (CASRN 75-21-8) in Support of Summary Information on the Integrated Risk Information System, EPA/635/R-16/350Fa; U.S. Environmental Protection Agency: Washington, DC, USA, 2016.
- Kirman, C.R.; Hays, S.M. Derivation of endogenous equivalent values to support risk assessment and risk management decisions for an endogenous carcinogen: Ethylene oxide. Regul. Toxicol. Pharmacol. 2017, 91, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Kirman, C.R.; Li, A.A.; Sheehan, P.J.; Bus, J.S.; Lewis, R.C.; Hays, S.M. Ethylene oxide review: Characterization of total exposure via endogenous and exogenous pathways and their implications to risk assessment and risk management. J. Toxicol. Environ. Health Part B Crit. Rev. 2021, 24, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Report on Human Exposure to Environmental Chemicals: Ethylene Oxide Hemoglobin Adducts. Available online: https://www.cdc.gov/exposurereport/index.html (accessed on 31 January 2019).
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Ethylene Oxide, Draft for Public Comment; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2020.
- Texas Commission on Environmental Quality. Ethylene Oxide Carcinogenic Dose-Response Assessment, Final Development Support Document; Texas Commission on Environmental Quality: Austin, TX, USA, 2020.
- Bogen, K.T.; Sheehan, P.J.; Valdez-Flores, C.; Li, A.A. Reevaluation of historical exposures to ethylene oxide among U.S. sterilization workers in the National Institute of Occupational Safety and Health (NIOSH) Study Cohort. Int. J. Environ. Res. Public Health 2019, 16, 1738. [Google Scholar] [CrossRef] [PubMed]
- Törnqvist, M.; Mowrer, J.; Jensen, S.; Ehrenberg, L. Monitoring of environmental cancer initiators through hemoglobin adducts by a modified Edman degradation method. Anal. Biochem. 1986, 154, 255–266. [Google Scholar] [CrossRef]
- Tates, A.D.; Grummt, T.; Törnqvist, M.; Farmer, P.B.; van Dam, F.J.; van Mossel, H.; Schoemaker, H.M.; Osterman-Golkar, S.; Uebel, C.; Tang, Y.S.; et al. Biological and chemical monitoring of occupational exposure to ethylene oxide. Mutat. Res. 1991, 250, 483–497. [Google Scholar] [CrossRef]
- Tavares, R.; Ramos, R.; Palminha, J.; Bispo, M.A.; Paz, I.; Bras, A.; Rueff, J.; Farmer, P.B.; Bailey, E. Transplacental exposure to genotoxins. Evaluation in haemoglobin of hydroxyethylvaline adduct levels in smoking and non-smoking mothers and their newborns. Carcinogenesis 1994, 15, 1271–1274. [Google Scholar] [CrossRef] [PubMed]
- Farmer, P.B.; Cordero, R.; Autrup, H. Monitoring human exposure to 2-hydroxyethylating carcinogens. Environ. Health Perspect. 1996, 104, 449–452. [Google Scholar] [PubMed]
- Farmer, P.B.; Sepai, O.; Lawrence, R.; Autrup, H.; Sabro Nielsen, P.; Vestergård, A.B.; Waters, R.; Leuratti, C.; Jones, N.J.; Stone, J.; et al. Biomonitoring human exposure to environmental carcinogenic chemicals. Mutagenesis 1996, 11, 363–381. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Krämer, A.; Angerer, J.; Hallier, E. Ethylene oxide-protein adduct formation in humans: Influence of glutathione-S-transferase polymorphisms. Int. Arch. Occup. Environ. Health 1998, 71, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Bono, R.; Vincenti, M.; Meineri, V.; Pignata, C.; Saglia, U.; Giachino, O.; Scursatone, E. Formation of N-(2-hydroxyethyl)valine due to exposure to ethylene oxide via tobacco smoke: A risk factor for onset of cancer. Environ. Res. 1999, 81, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Bono, R.; Vincent, M.; Saglia, U.; Pignata, C.; Russo, R.; Gilli, G. Tobacco smoke and formation of N-(2-hydroxyethyl)valine in human hemoglobin. Arch. Environ. Health 2002, 57, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Fennell, T.R.; MacNeela, J.P.; Morris, R.W.; Watson, M.; Thompson, C.L.; Bell, D.A. Hemoglobin adducts from acrylonitrile and ethylene oxide in cigarette smokers: Effects of glutathione S-transferase T1-null and M1-null genotypes. Cancer Epidemiol. Biomarkers Prev. 2000, 9, 705–712. [Google Scholar] [PubMed]
- Wu, K.Y.; Chiang, S.Y.; Huang, T.H.; Tseng, Y.S.; Chen, Y.L.; Kuo, H.W.; Hsieh, C.L. Formation of N-(2-hydroxyethyl)valine in human hemoglobin-effect of lifestyle factors. Mutat. Res. 2004, 559, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Sterigenics International. Sterigenics Announces Plan to Exit Willowbrook Operations Following Approval from State and Illinois EPA to Implement Changes; Sterigenics International: Broadview Heights, OH, USA, 2019. [Google Scholar]
- Michigan Department of Environment, Great Lakes, and Energy. In the Matter of Administrative Proceedings against Viant Medical, Inc. Stipulation for Entry of Final Order by Consent; Michigan Department of Environment, Great Lakes, and Energy: Lansing, MI, USA, 2019.
- Lake County Health Department and Community Health Center. EtO Monitoring Results. Available online: https://www.lakecountyil.gov/4188/EtO-Monitoring-Results (accessed on 19 October 2020).
- U.S. Environmental Protection Agency. EPA in Illinois: Outdoor Air Monitoring Data in the Willowbrook Community. Available online: https://www.epa.gov/il/outdoor-air-monitoring-data-willowbrook-community (accessed on 19 October 2020).
- Ramboll US Corporation. Ambient Air Monitoring Report: Ethylene Oxide Background Concentrations in Chicago Metro Area; Sterigenics US, LLC: Oak Brook, IL, USA, 2019. [Google Scholar]
- Georgia Department of Natural Resources. Cobb County Air Quality Monitoring Test Results. Available online: https://epd.georgia.gov/cobb-county-air-quality-monitoring (accessed on 19 October 2020).
- Georgia Department of Natural Resources. Covington Air Quality Monitoring Test Results. Available online: https://epd.georgia.gov/covington-monitoring-results (accessed on 19 October 2020).
- Georgia Department of Natural Resources. Fulton County Air Quality Monitoring Test Results. Available online: https://epd.georgia.gov/fulton-county-monitoring-results (accessed on 19 October 2020).
- Georgia Department of Natural Resources. General Coffee State Park Air Quality Monitoring Test Results. Available online: https://epd.georgia.gov/gneral-coffee-monitoring-results (accessed on 19 October 2020).
- Georgia Department of Natural Resources. South DeKalb Air Quality Monitoring Test Results. Available online: https://epd.georgia.gov/south-dekalb-monitoring-results (accessed on 19 October 2020).
- Michigan Department of Environment, Great Lakes, and Energy. Viant Medical, Inc. Available online: https://www.michigan.gov/egle/0,9429,7-135-3310_70314_89277---,00.html (accessed on 19 October 2020).
- Colorado Department of Public Health & Environment. Ethylene Oxide/Terumo BCT Air Sampling Study: Pre- and Post-Control Air Monitoring Report; Colorado Department of Public Health & Environment, Air Pollution Control Division: Denver, CO, USA, 2018.
- Battelle. Technical Assistance Document for the National Air Toxics Trends Stations Program; U.S. Environmental Protection Agency, Office of Air Quality Planning and Standards (C304-06): Washington, DC, USA, 2016.
- U.S. Environmental Protection Agency. Ethylene Oxide Measurements by TO-15 Method. Available online: https://www3.epa.gov/ttnamti1/files/ambient/airtox/EtO-Method-for-NATTS-labs-2019.pdf (accessed on 30 November 2020).
- Barnard, J.A.; Lee, R.K. Combustion of n-pentane in a shock tube. Combust. Sci. Technol. 1972, 6, 143–150. [Google Scholar] [CrossRef]
- Jain, R.B. Associations between observed concentrations of ethylene oxide in whole blood and smoking, exposure to environmental tobacco smoke, and cancers including breast cancer: Data for US children, adolescents, and adults. Environ. Sci. Pollut. Res. Int. 2020, 27, 20912–20919. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Facility | Location | Year | Season 1 | n (sites) 2,3 | Dist. 4 | Dur. 5 |
|---|---|---|---|---|---|---|
| Medline 6 [20] | Waukegan, IL | 19/20 | A, B, C | 174 (5) | ~190–1660 | 24 |
| Vantage [20] | Gurnee, IL | 19/20 | A, B, C | 250 (5) | ~260–1130 | 24 |
| Background [20] | Gurnee, IL | 19/20 | A, B, C, D | 98 (2) | >2440 | 24 |
| Sterigenics [21] | Willowbrook, IL | 18/19 | C, D | 237 (8) | ~100–1700 | 24 |
| Background [22] | Chicago, IL area | 18/19 | C | 28 (14) | >9600 | 12 |
| Sterigenics [23] | Smyrna, GA | 19/20 | A, B, C, D | 211 (7) | ~280–1970 | 24 |
| BD 7 [24] | Covington, GA | 19/20 | A, B, C, D | 267 (8) | ~60–1980 | 24 |
| SS 8 [25] | Atlanta, GA | 19/20 | A, B, D | 64 (3) | ~150–840 | 24 |
| Background [26] | General Coffee, GA | 19/20 | A, B, C, D | 25 (1) | >290,000 | 24 |
| Background [27] | South DeKalb, GA | 19/20 | A, B, C, D | 58 (2) | >22,500 | 24 |
| Viant [28] | Grand Rapids, MI | 18/19 | A, B, C, D | 20 (12) | ~80–1520 | 24 |
| Background [28] | Grand Rapids, MI | 19 | A | 4 (4) | >2100 | 24 |
| Terumo [29] | Lakewood, CO | 18 | B, C | 84 (8) | ~40–1570 | 24 |
| Background [29] | Denver, CO area | 18 | C | 18 (4) | >4500 | 24 |
| Percentile | HEVunadj 1 | Total Eq. 2 | HEVadj 3 | Endog. Eq. 4 |
|---|---|---|---|---|
| pmol/g Hb | ppb | pmol/g Hb | ppb | |
| P5 | 13.4 | 1.3 | 11.2 | 1.0 |
| P10 | 16.0 | 1.5 | 13.8 | 1.3 |
| P25 | 20.8 | 1.9 | 18.6 | 1.7 |
| P50 | 27.0 | 2.5 | 24.8 | 2.3 |
| P75 | 35.1 | 3.2 | 32.9 | 3.0 |
| P90 | 47.5 | 4.4 | 45.3 | 4.2 |
| P95 | 60.1 | 5.5 | 57.9 | 5.3 |
| Facility (Controls 1) | Mean ± SD | P50 2 | P90 3 |
|---|---|---|---|
| Medline (pre) | 0.31 ± 0.74 | 0.11 | 0.86 |
| Medline (post) | 0.17 ± 0.12 | 0.13 | 0.43 |
| Vantage | 0.17 ± 0.40 | 0.09 | 0.43 |
| Background | 0.10 ± 0.11 | 0.07 | 0.26 |
| Sterigenics 4 | 0.70 ± 1.72 | 0.22 | 1.92 |
| Background | 0.15 ± 0.11 | 0.13 | 0.31 |
| Sterigenics 5 | 0.26 ± 0.21 | 0.19 | 0.77 |
| Becton Dickinson | 0.28 ± 0.50 | 0.20 | 0.73 |
| Sterilization Services | 0.58 ± 0.42 | 0.46 | 1.45 |
| Background | 0.19 ± 0.16 | 0.13 | 0.56 |
| Viant | 0.22 ± 0.26 | 0.15 | 0.57 |
| Background | 0.11 ± 0.01 | 0.11 | 0.12 |
| Terumo (pre) | 1.14 ± 0.87 | 0.87 | 3.10 |
| Terumo (post) | 0.29 ± 0.21 | 0.21 | 0.89 |
| Background | 0.15 ± 0.15 | 0.10 | 0.44 |
| NATTS / UAT Background | Facility Background | ||
|---|---|---|---|
| Location | ppb | Location | ppb 1 |
| Phoenix, AZ | 0.22 | Denver, CO area | 0.18 |
| Phoenix, AZ | 0.12 | Denver, CO area | 0.07 |
| Grand Junction, CO | 0.17 | Denver, CO area | 0.25 |
| Pinellas Park, FL | 0.08 | Denver, CO area | 0.08 |
| St. Petersburg, FL | 0.08 | General Coffee, GA | 0.20 |
| Valrico, FL | 0.08 | South DeKalb, GA | 0.19 |
| Northbrook, IL | 0.15 | South DeKalb, GA | 0.15 |
| Schiller Park, IL | 0.19 | Chicago, IL area | 0.18 |
| Ashland, KY | 0.16 | Chicago, IL area | 0.15 |
| Calvert City, KY | 0.16 | Chicago, IL area | 0.09 |
| Grayson, KY | 0.14 | Chicago, IL area | 0.14 |
| Smithland, KY | 0.17 | Chicago, IL area | 0.17 |
| Albany, NY | 0.10 | Chicago, IL area | 0.10 |
| Bronx, NY | 0.09 | Chicago, IL area | 0.11 |
| Bronx, NY | 0.08 | Chicago, IL area | 0.10 |
| Camden, NJ | 0.19 | Chicago, IL area | 0.10 |
| Chester, NJ | 0.19 | Chicago, IL area | 0.10 |
| E. Brunswick, NJ | 0.17 | Chicago, IL area | 0.49 |
| Elizabeth, NJ | 0.16 | Chicago, IL area | 0.15 |
| Pinnacle, NY | 0.10 | Chicago, IL area | 0.27 |
| Queens, NY | 0.08 | Chicago, IL area | 0.11 |
| Rochester, NY | 0.10 | Gurnee, IL | 0.11 |
| Dearborn, MI | 0.13 | Gurnee, IL | 0.09 |
| St. Louis, MO | 0.15 | Grand Rapids, MI | 0.10 |
| Bountiful, UT | 0.14 | Grand Rapids, MI | 0.10 |
| Lacey, WA | 0.11 | Grand Rapids, MI | 0.12 |
| Seattle, WA | 0.09 | Grand Rapids, MI | 0.10 |
| Overall mean ± SD | 0.13 ± 0.04 | Overall mean ± SD | 0.14 ± 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheehan, P.J.; Lewis, R.C.; Kirman, C.R.; Watson, H.N.; Winegar, E.D.; Bus, J.S. Ethylene Oxide Exposure in U.S. Populations Residing Near Sterilization and Other Industrial Facilities: Context Based on Endogenous and Total Equivalent Concentration Exposures. Int. J. Environ. Res. Public Health 2021, 18, 607. https://doi.org/10.3390/ijerph18020607
Sheehan PJ, Lewis RC, Kirman CR, Watson HN, Winegar ED, Bus JS. Ethylene Oxide Exposure in U.S. Populations Residing Near Sterilization and Other Industrial Facilities: Context Based on Endogenous and Total Equivalent Concentration Exposures. International Journal of Environmental Research and Public Health. 2021; 18(2):607. https://doi.org/10.3390/ijerph18020607
Chicago/Turabian StyleSheehan, Patrick J., Ryan C. Lewis, Christopher R. Kirman, Heather N. Watson, Eric D. Winegar, and James S. Bus. 2021. "Ethylene Oxide Exposure in U.S. Populations Residing Near Sterilization and Other Industrial Facilities: Context Based on Endogenous and Total Equivalent Concentration Exposures" International Journal of Environmental Research and Public Health 18, no. 2: 607. https://doi.org/10.3390/ijerph18020607
APA StyleSheehan, P. J., Lewis, R. C., Kirman, C. R., Watson, H. N., Winegar, E. D., & Bus, J. S. (2021). Ethylene Oxide Exposure in U.S. Populations Residing Near Sterilization and Other Industrial Facilities: Context Based on Endogenous and Total Equivalent Concentration Exposures. International Journal of Environmental Research and Public Health, 18(2), 607. https://doi.org/10.3390/ijerph18020607