
The Association of Mobile Health Applications with Self-Management Behaviors among Adults with Chronic Conditions in the United States



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
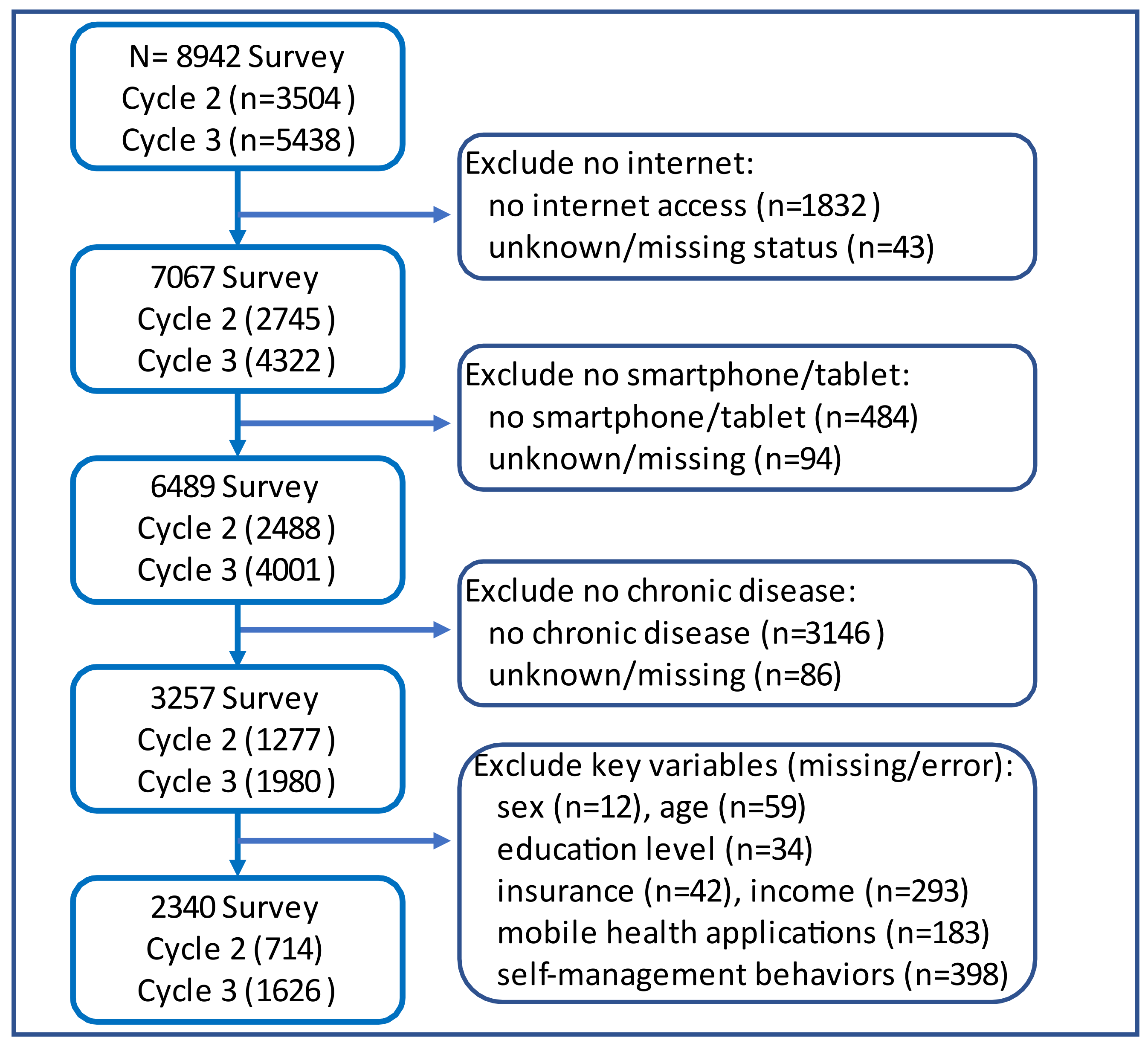
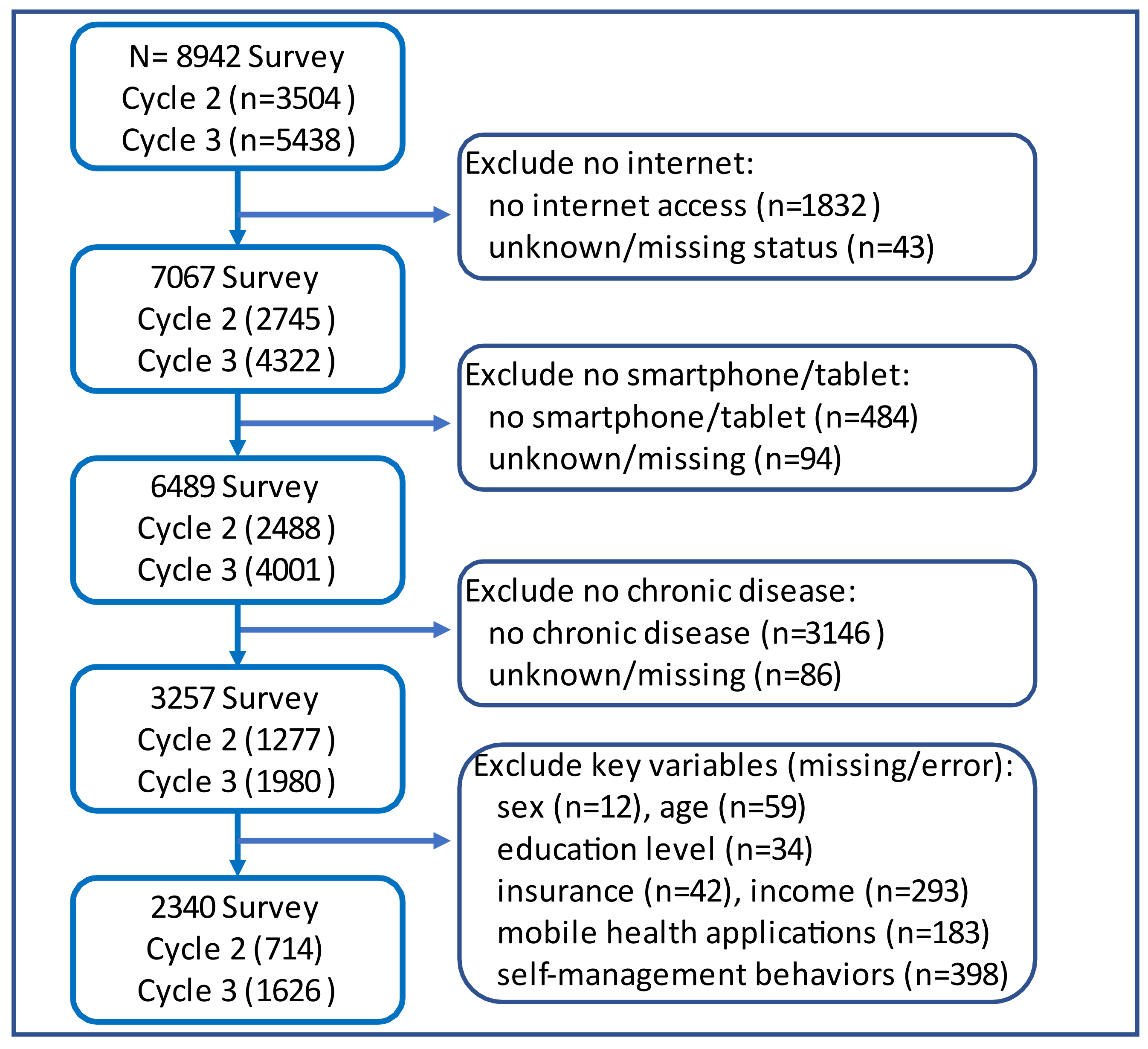
2.2. Study Participants
2.3. Measures
2.3.1. Self-Management Behaviors
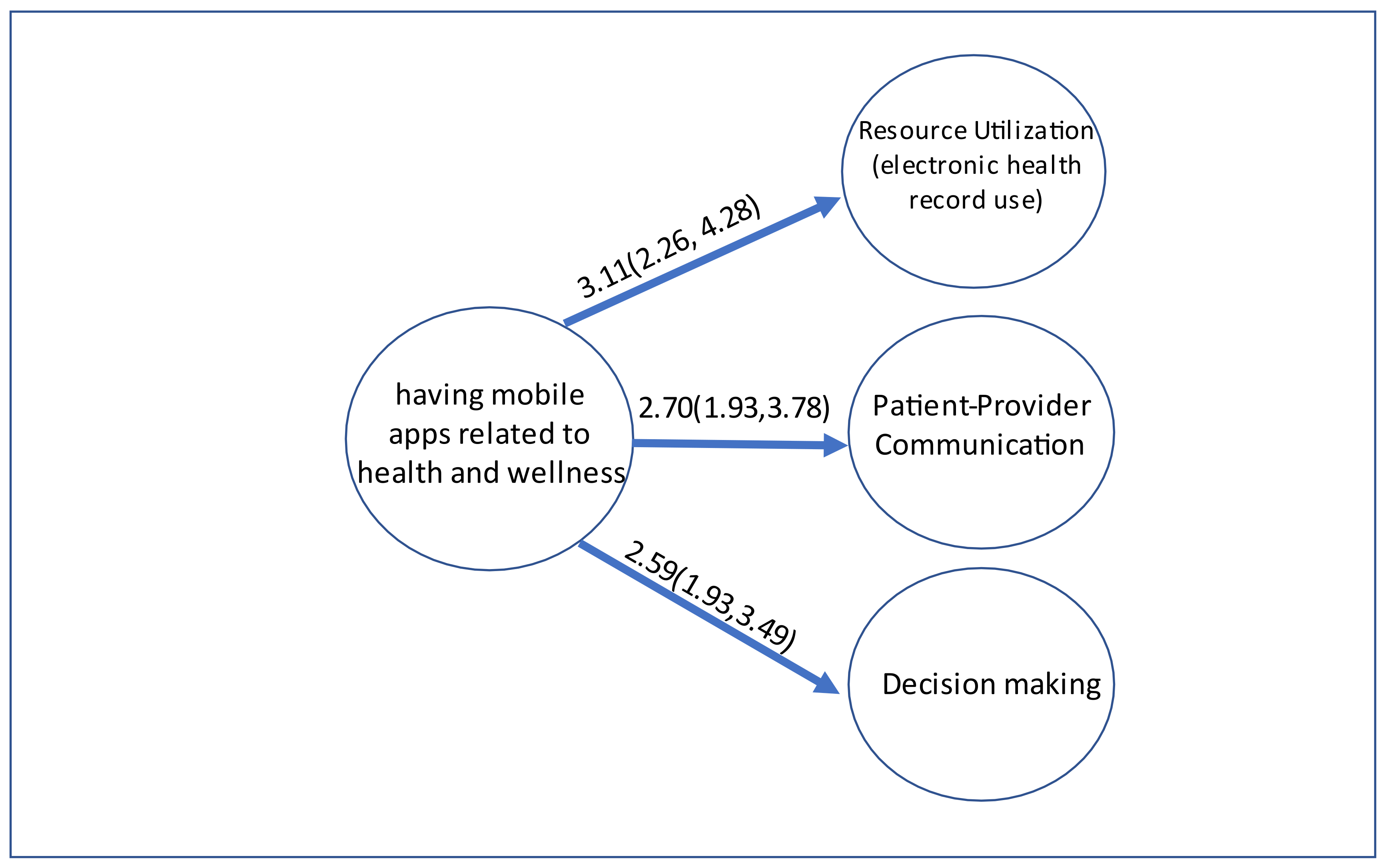
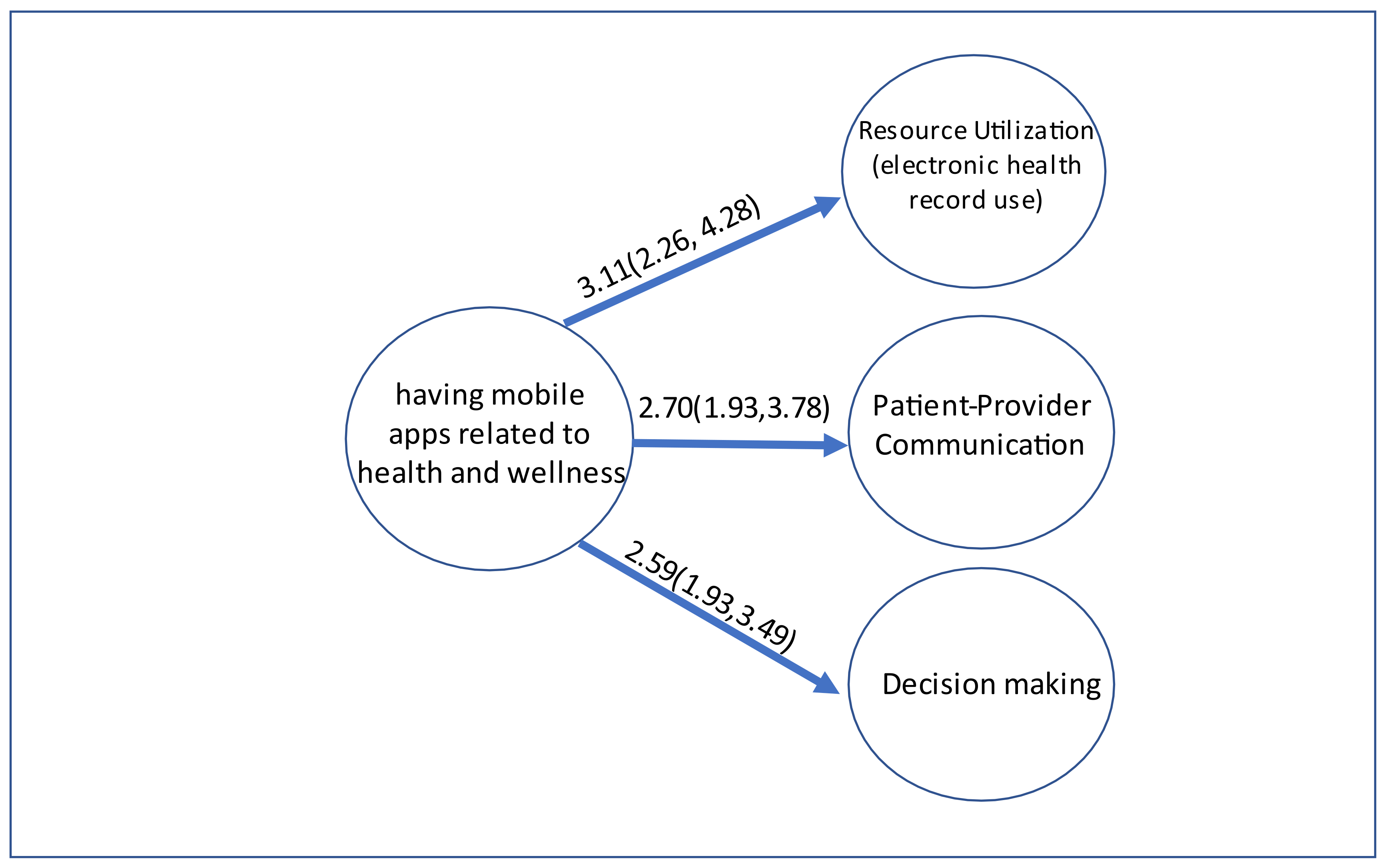
- Patient–provider communication. This was assessed with the yes/no response to the question: “Has your tablet or smartphone helped you in discussions with your health care provider?” [22].
- Resource utilization. This was assessed with a yes/no dichotomy of the personal health record use question: “How many times did you access your online medical record in the last 12 months?” [22]. If the respondents answered “none”, then they were considered as non-using resources. Individuals who accessed their online medical records at least once were considered to have utilized resources.
- Decision-making. This was assessed with the yes/no response to the question: “Has your tablet or smartphone helped you make a decision about how to treat an illness or condition?” [22].
2.3.2. Key Independent Variable: Use of mHealth Apps
2.3.3. Other Explanatory Variables
2.3.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient self-management of chronic disease in primary care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef]
- Grady, P.A.; Gough, L.L. Self-management: A comprehensive approach to management of chronic conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Lorig, K.R.; Holman, H. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef]
- Ha Dinh, T.T.; Bonner, A.; Clark, R.; Ramsbotham, J.; Hines, S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 210–247. [Google Scholar] [CrossRef] [Green Version]
- Allegrante, J.P. Advancing the Science of Behavioral Self-Management of Chronic Disease: The Arc of a Research Trajectory. Health Educ. Behav. 2018, 45, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Allegrante, J.P.; Wells, M.T.; Peterson, J.C. Interventions to Support Behavioral Self-Management of Chronic Diseases. Annu. Rev. Public Health 2019, 40, 127–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.S.; Pisano, M.M.; Boone, A.L.; Baker, G.; Pers, Y.-M.; Pilotto, A.; Valsecchi, V.; Zora, S.; Zhang, X.; Fierloos, I.; et al. Evaluation Design of EFFICHRONIC: The Chronic Disease Self-Management Programme (CDSMP) Intervention for Citizens with a Low Socioeconomic Position. Int. J. Environ. Res. Public Health 2019, 16, 1883. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Self-Management Education: Learn More Feel Better. Available online: www.cdc.gov/learnmorefeelbetter/index.htm. (accessed on 26 November 2018).
- Anderson, K.; Burford, O.; Emmerton, L. Mobile Health Apps to Facilitate Self-Care: A Qualitative Study of User Experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alessa, T.; Hawley, M.S.; Hock, E.S.; de Witte, L. Smartphone Apps to Support Self-Management of Hypertension: Review and Content Analysis. JMIR Mhealth Uhealth 2019, 7, e13645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Whitehead, L.; Seaton, P. The Effectiveness of Self-Management Mobile Phone and Tablet Apps in Long-term Condition Management: A Systematic Review. J. Med. Internet Res. 2016, 18, e97. [Google Scholar] [CrossRef]
- Devan, H.; Farmery, D.; Peebles, L.; Grainger, R. Evaluation of Self-Management Support Functions in Apps for People with Persistent Pain: Systematic Review. JMIR Mhealth Uhealth 2019, 7, e13080. [Google Scholar] [CrossRef]
- Serlachius, A.; Schache, K.; Kieser, A.; Arroll, B.; Petrie, K.; Dalbeth, N. Association Between User Engagement of a Mobile Health App for Gout and Improvements in Self-Care Behaviors: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e15021. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Yu, W. A Mobile App for Diabetes Management: Impact on Self-Efficacy among Patients with Type 2 Diabetes at a Community Hospital. Med Sci Monit 2020, 26, e926719. [Google Scholar] [CrossRef]
- Chen, J.; Lieffers, J.; Bauman, A.; Hanning, R.; Allman-Farinelli, M. The use of smartphone health apps and other mobile health (mHealth) technologies in dietetic practice: A three country study. J. Hum. Nutr. Diet. 2017, 30, 439–452. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, B.; Taylor, C.B.; O’Neil, A.; Cocker, F.; Cameron, L.D. Using new technologies to improve the prevention and management of chronic conditions in populations. Annu. Rev. Public Health 2015, 36, 483–505. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.L.; Laurent, D.D.; Plant, K. Internet-based chronic disease self-management: A randomized trial. Med. Care 2006, 44, 964–971. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, M.M.; Merry, K.J.; Locke, S.R.; Jung, M.E. Effects of Mobile Health Prompts on Self-Monitoring and Exercise Behaviors Following a Diabetes Prevention Program: Secondary Analysis From a Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e12956. [Google Scholar] [CrossRef]
- Bokolo, A.J. Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic. J. Med. Syst. 2020, 44, 132. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B. Revisiting Health Information Technology Ethical, Legal, And Social Issues And Evaluation: Telehealth/Telemedicine and COVID-19. Int. J. Med. Inform. 2020, 143, 104239. [Google Scholar] [CrossRef]
- National Cancer Institution. Health Information National Trend Survey. Available online: https://hints.cancer.gov (accessed on 27 September 2021).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, A.; Kedia, S.; Wyant, D.K.; Ahn, S.; Bhuyan, S.S. Use of mobile health applications for health-promoting behavior among individuals with chronic medical conditions. Digit Health 2019, 5, 2055207619882181. [Google Scholar] [CrossRef] [PubMed]
- Lyles, C.R.; Nelson, E.C.; Frampton, S.; Dykes, P.C.; Cemballi, A.G.; Sarkar, U. Using Electronic Health Record Portals to Improve Patient Engagement: Research Priorities and Best Practices. Ann. Intern. Med. 2020, 172, S123–S129. [Google Scholar] [CrossRef]
- Irizarry, T.; Shoemake, J.; Nilsen, M.L.; Czaja, S.; Beach, S.; DeVito, D.A. Patient Portals as a Tool for Health Care Engagement: A Mixed-Method Study of Older Adults With Varying Levels of Health Literacy and Prior Patient Portal Use. J. Med. Internet Res. 2017, 19, e99. [Google Scholar] [CrossRef]
- Jenerette, C.M.; Mayer, D.K. Patient-Provider Communication: The Rise of Patient Engagement. Semin. Oncol. Nurs. 2016, 32, 134–143. [Google Scholar] [CrossRef]
- Granados-Santiago, M.; Valenza, M.C.; Lopez-Lopez, L.; Prados-Roman, E.; Rodriguez-Torres, J.; Cabrera-Martos, I. Shared decision-making and patient engagement program during acute exacerbation of COPD hospitalization: A randomized control trial. Patient Educ. Couns. 2020, 103, 702–708. [Google Scholar] [CrossRef]
- Williams, R. Using the margins command to estimate and interpret adjusted predictions and marginal effects. Stata J. 2012, 12, 308–331. [Google Scholar] [CrossRef] [Green Version]
- Finney Rutten, L.J.; Blake, K.D.; Skolnick, V.G.; Davis, T.; Moser, R.P.; Hesse, B.W. Data Resource Profile: The National Cancer Institute’s Health Information National Trends Survey (HINTS). Int. J. Epidemiol. 2020, 49, 17–17j. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Nunn, C.A.; Rotondi, M.; Couperthwaite, A.B.; Reiser, S.; Simone, A.; Katzman, D.K.; Cafazzo, J.A.; Palmert, M.R. A Mobile App for the Self-Management of Type 1 Diabetes among Adolescents: A Randomized Controlled Trial. JMIR Mhealth Uhealth 2017, 5, e82. [Google Scholar] [CrossRef] [PubMed]
- Aji, M.; Gordon, C.; Peters, D.; Bartlett, D.; Calvo, R.A.; Naqshbandi, K.; Glozier, N. Exploring User Needs and Preferences for Mobile Apps for Sleep Disturbance: Mixed Methods Study. JMIR Ment. Health 2019, 6, e13895. [Google Scholar] [CrossRef]
- Gill, P.S.; Kamath, A.; Gill, T.S. Distraction: An assessment of smartphone usage in health care work settings. Risk Manag. Healthc. Policy 2012, 5, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Cui, M.; Wu, X.; Mao, J.; Wang, X.; Nie, M. T2DM Self-Management via Smartphone Applications: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166718. [Google Scholar] [CrossRef]
- Farzandipour, M.; Nabovati, E.; Sharif, R.; Arani, M.H.; Anvari, S. Patient Self-Management of Asthma Using Mobile Health Applications: A Systematic Review of the Functionalities and Effects. Appl. Clin. Inform. 2017, 8, 1068–1081. [Google Scholar] [CrossRef] [PubMed]
- Kaphle, S.; Chaturvedi, S.; Chaudhuri, I.; Krishnan, R.; Lesh, N. Adoption and Usage of mHealth Technology on Quality and Experience of Care Provided by Frontline Workers: Observations From Rural India. JMIR Mhealth Uhealth 2015, 3, e61. [Google Scholar] [CrossRef]
- Tenforde, M.; Nowacki, A.; Jain, A.; Hickner, J. The association between personal health record use and diabetes quality measures. J. Gen. Intern. Med. 2012, 27, 420–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldwin, J.L.; Singh, H.; Sittig, D.F.; Giardina, T.D. Patient portals and health apps: Pitfalls, promises, and what one might learn from the other. Healthcare 2017, 5, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Wells, S.; Rozenblum, R.; Park, A.; Dunn, M.; Bates, D.W. Personal health records for patients with chronic disease: A major opportunity. Appl. Clin. Inform. 2014, 5, 416–429. [Google Scholar]
- Ammenwerth, E.; Schnell-Inderst, P.; Hoerbst, A. The impact of electronic patient portals on patient care: A systematic review of controlled trials. J. Med. Internet Res. 2012, 14, e162. [Google Scholar] [CrossRef] [PubMed]
- Han, H.R.; Gleason, K.T.; Sun, C.A.; Miller, H.N.; Kang, S.J.; Chow, S.; Anderson, R.; Nagy, R.; Bauer, T. Using Patient Portals to Improve Patient Outcomes: Systematic Review. JMIR Hum. Factors 2019, 6, e15038. [Google Scholar] [CrossRef] [Green Version]
- Holman, H.; Lorig, K. Patients as partners in managing chronic disease. Partnership is a prerequisite for effective and efficient health care. BMJ 2000, 320, 526–527. [Google Scholar] [CrossRef]
- Belasen, A.; Belasen, A.T. Doctor-patient communication: A review and a rationale for using an assessment framework. J. Health Organ. Manag. 2018, 32, 891–907. [Google Scholar] [CrossRef]
- Hincapie, M.A.; Gallego, J.C.; Gempeler, A.; Pineros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. J. Prim. Care Community Health 2020, 11, 2150132720980612. [Google Scholar] [CrossRef] [PubMed]
- Gustin, A.N., Jr. Shared Decision-Making. Anesthesiol. Clin. 2019, 37, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Milky, G.; Thomas, J., III. Shared decision making, satisfaction with care and medication adherence among patients with diabetes. Patient Educ. Couns. 2020, 103, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Holmen, H.; Torbjornsen, A.; Wahl, A.K.; Jenum, A.K.; Småstuen, M.C.; Årsand, E.; Ribu, L. A Mobile Health Intervention for Self-Management and Lifestyle Change for Persons With Type 2 Diabetes, Part 2: One-Year Results From the Norwegian Randomized Controlled Trial RENEWING HEALTH. JMIR Mhealth Uhealth 2014, 2, e57. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.C.; Shardell, M.D.; Terrin, M.L.; Barr, E.A.; Park, D.; Shaikh, F.; Guralnik, J.M.; Gruber-Baldini, A.L. Mobile Diabetes Intervention for Glycemic Control in 45- to 64-Year-Old Persons With Type 2 Diabetes. J. Appl. Gerontol. 2016, 35, 227–243. [Google Scholar] [CrossRef]
- Cameron-Tucker, H.L.; Wood-Baker, R.; Owen, C.; Joseph, L.; Walters, E.H. Chronic disease self-management and exercise in COPD as pulmonary rehabilitation: A randomized controlled trial. Int. J. Chron. Obstr. Pulmon. Dis. 2014, 9, 513–523. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Biological and Socioeconomic Variables | Individual Having mHealth Apps | Individual Not Having mHealth Apps | ||||
|---|---|---|---|---|---|---|
| n | Wt % | n | Wt % | p-Value | ||
| ALL | 1327 | 59.8 | 1013 | 40.3 | ||
| Sex | 0.0695 | |||||
| Female | 760 | 52.0 | 529 | 46.0 | ||
| Male | 567 | 48.0 | 484 | 54.0 | ||
| Age in Years | 0.0027 | |||||
| 18–34 years | 130 | 19.1 | 51 | 11.7 | ||
| 35–49 years | 255 | 25.5 | 128 | 23.1 | ||
| 50–64 years | 525 | 37.8 | 354 | 36.2 | ||
| 65–74 years | 298 | 12.1 | 333 | 20.6 | ||
| 75 and older | 119 | 5.5 | 147 | 8.4 | ||
| Race/Ethnicity | 0.5404 | |||||
| Non-Hispanic White | 814 | 66.4 | 676 | 68.4 | ||
| Non-Hispanic Black | 191 | 8.7 | 115 | 8.5 | ||
| Hispanic | 153 | 13.3 | 111 | 14.4 | ||
| Others | 169 | 11.7 | 111 | 8.7 | ||
| Education | 0.0047 | |||||
| Less than High School | 31 | 4.0 | 35 | 4.6 | ||
| High School or equivalent | 229 | 25.0 | 271 | 37.3 | ||
| Some College | 331 | 35.2 | 266 | 31.7 | ||
| College and above | 736 | 35.8 | 441 | 26.4 | ||
| Insurance | 0.5819 | |||||
| Yes | 1286 | 94.6 | 970 | 93.5 | ||
| No | 41 | 5.4 | 43 | 6.5 | ||
| Annual Income | 0.0003 | |||||
| Less than 20k | 140 | 10.3 | 170 | 16.5 | ||
| 20k–<35k | 136 | 9.1 | 136 | 11.8 | ||
| 35k–<50k | 158 | 13.1 | 146 | 14.8 | ||
| 50k–<75k | 255 | 18.1 | 234 | 24.3 | ||
| 75k+ | 638 | 49.4 | 327 | 32.6 | ||
| Chronic diseases | 0.3233 | |||||
| 1 chronic condition | 812 | 65.5 | 596 | 61.5 | ||
| >1 chronic conditions | 515 | 34.5 | 417 | 38.5 | ||
| Self-Management Behaviors | Individuals with mHealth Apps | Individuals without mHealth Apps | |||
|---|---|---|---|---|---|
| n | Wt% | n | Wt% | p Value | |
| Decision Making Yes No | - 725 602 | - 53.9 46.1 | - 314 699 | - 30.9 69.1 | <0.0001 |
| Patient–provider Communication Yes No | - 741 586 | - 53.6 46.4 | - 292 721 | - 28.7 71.4 | <0.0001 |
| Resource Utilization (electronic health record use) Yes No | - 877 450 | - 69.4 30.6 | - 441 572 | - 40.6 59.4 | <0.0001 |
| Proportional Odds Ratios | 95% Confidence Interval | p Value | |
|---|---|---|---|
| Having mHealth apps No Yes | - reference 3.53 | - reference [2.63–4.72] | - - <0.0001 |
| Cutoff | Point | 95% Confidence Interval | p value |
| Cut1 Cut2 Cut3 | 0.28 1.72 2.92 | [−0.44, 0.99] [0.99, 2.44] [2.21, 3.63] | 0.441 <0.0001 <0.0001 |
| Margins of Different Engagement Levels of Self-management | - probability | - 95% Confidence Interval | - p value |
| No engagement Without mHealth apps With mHealth apps | - 0.37 0.15 | - [0.32, 0.42] [0.12, 0.18] | - <0.0001 <0.0001 |
| Low level of engagement Without mHealth apps With mHealth apps | - 0.34 0.27 | - [0.30, 0.37] [0.23, 0.30] | - <0.0001 <0.0001 |
| Moderate level of engagement Without mHealth apps With mHealth apps | - 0.18 0.28 | - [0.15, 0.21] [0.24, 0.32] | - <0.0001 <0.0001 |
| High level of engagement Without mHealth apps With mHealth apps | - 0.11 0.31 | - [0.09, 0.14] [0.27, 0.34] | - <0.0001 <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Ho, A.F.; Wiener, R.C.; Sambamoorthi, U. The Association of Mobile Health Applications with Self-Management Behaviors among Adults with Chronic Conditions in the United States. Int. J. Environ. Res. Public Health 2021, 18, 10351. https://doi.org/10.3390/ijerph181910351
Wang H, Ho AF, Wiener RC, Sambamoorthi U. The Association of Mobile Health Applications with Self-Management Behaviors among Adults with Chronic Conditions in the United States. International Journal of Environmental Research and Public Health. 2021; 18(19):10351. https://doi.org/10.3390/ijerph181910351
Chicago/Turabian StyleWang, Hao, Amy F. Ho, R. Constance Wiener, and Usha Sambamoorthi. 2021. "The Association of Mobile Health Applications with Self-Management Behaviors among Adults with Chronic Conditions in the United States" International Journal of Environmental Research and Public Health 18, no. 19: 10351. https://doi.org/10.3390/ijerph181910351
APA StyleWang, H., Ho, A. F., Wiener, R. C., & Sambamoorthi, U. (2021). The Association of Mobile Health Applications with Self-Management Behaviors among Adults with Chronic Conditions in the United States. International Journal of Environmental Research and Public Health, 18(19), 10351. https://doi.org/10.3390/ijerph181910351