
The Abbreviated Overall Anxiety Severity and Impairment Scale (OASIS) and the Abbreviated Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation of the Czech Versions

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. The Overall Anxiety Severity and Impairment Scale (OASIS)
2.2.2. The Overall Depression Severity and Impairment Scale (ODSIS)
2.2.3. Big Five Inventory, Neuroticism (BFI-N)
2.2.4. Rosenberg Self-Esteem Scale (RSES)
2.2.5. The Positive and Negative Affect Schedule (PANAS)
2.2.6. General Anxiety Disorder-7 (GAD-7)
2.2.7. Patient Health Questionnaire-9 (PHQ-9)
2.3. Statistical Analyses
3. Results
3.1. Sociodemographic Results
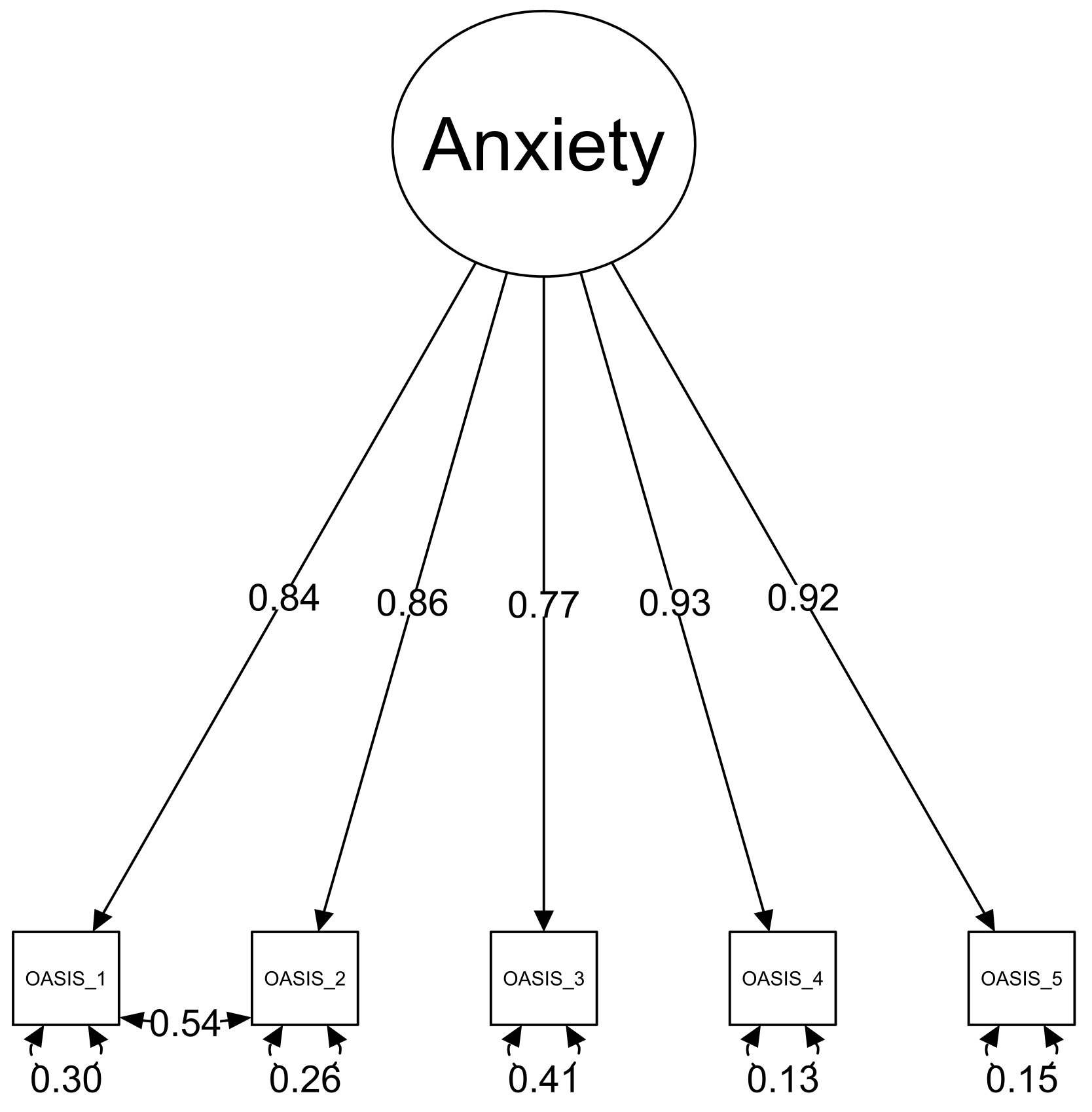
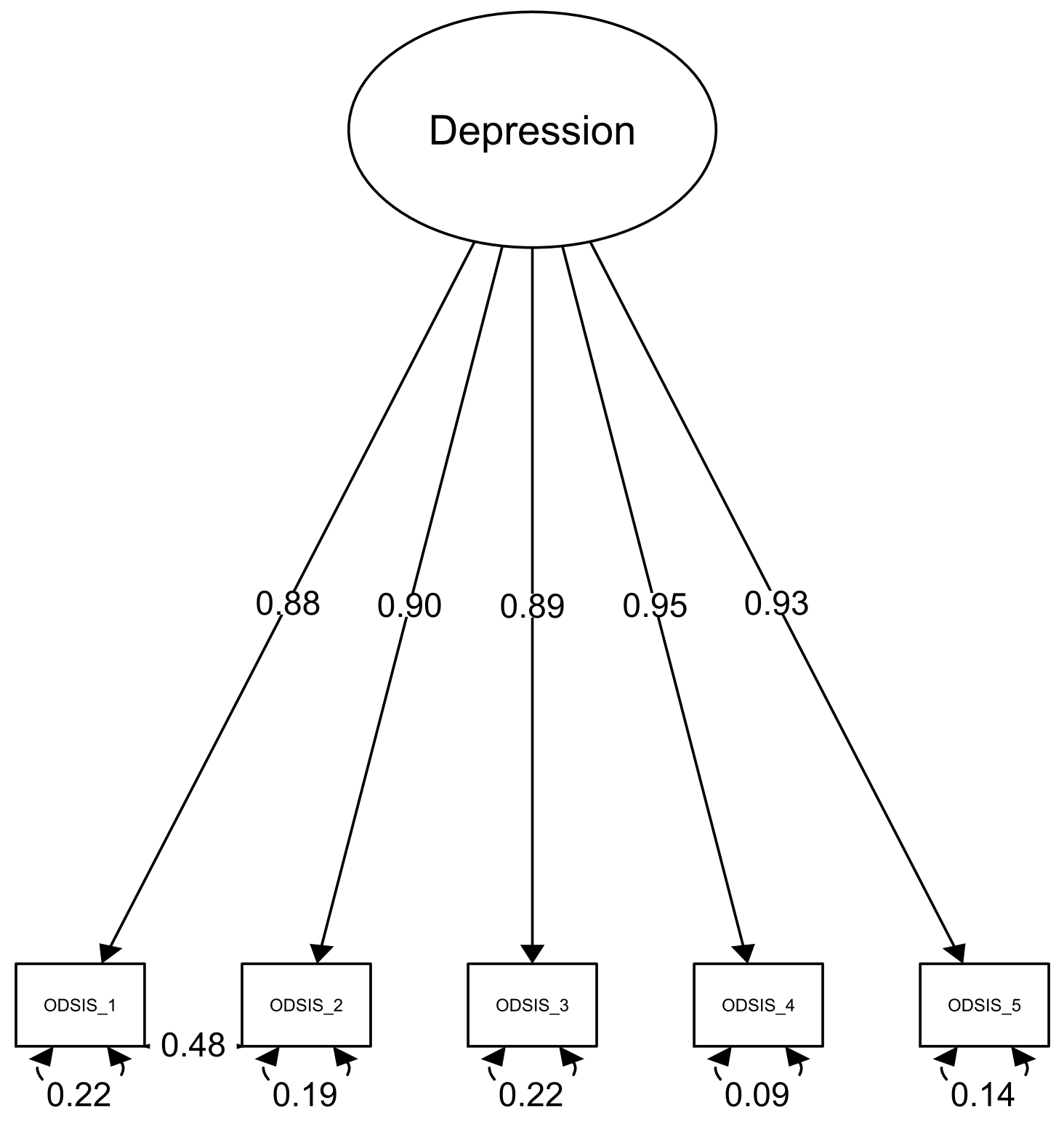
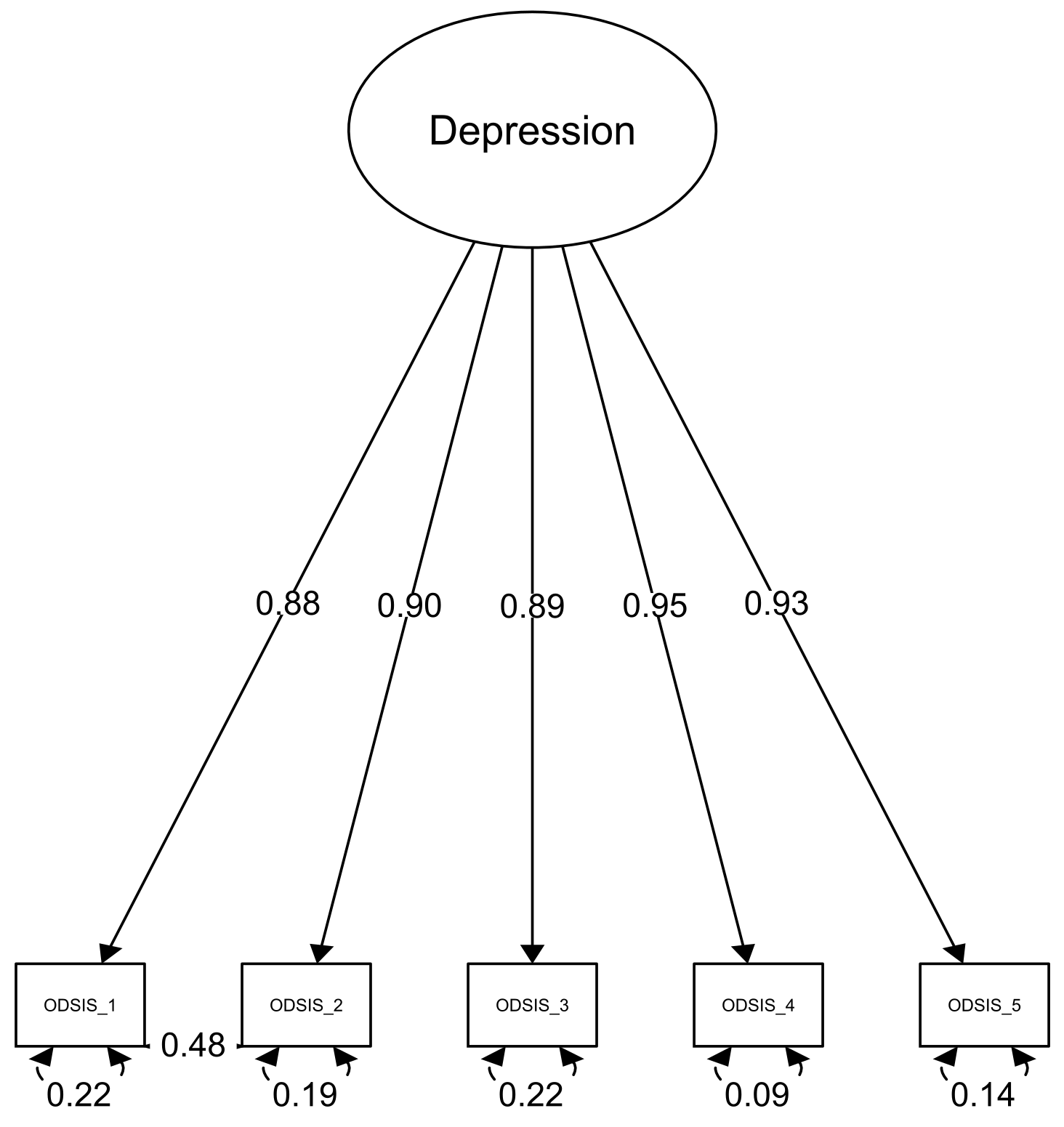
3.2. Confirmatory Factor Analysis Results
3.3. Invariance Testing and Factor Loadings
3.4. Internal Consistency and Test–Retest Reliability
3.5. Convergent Validity
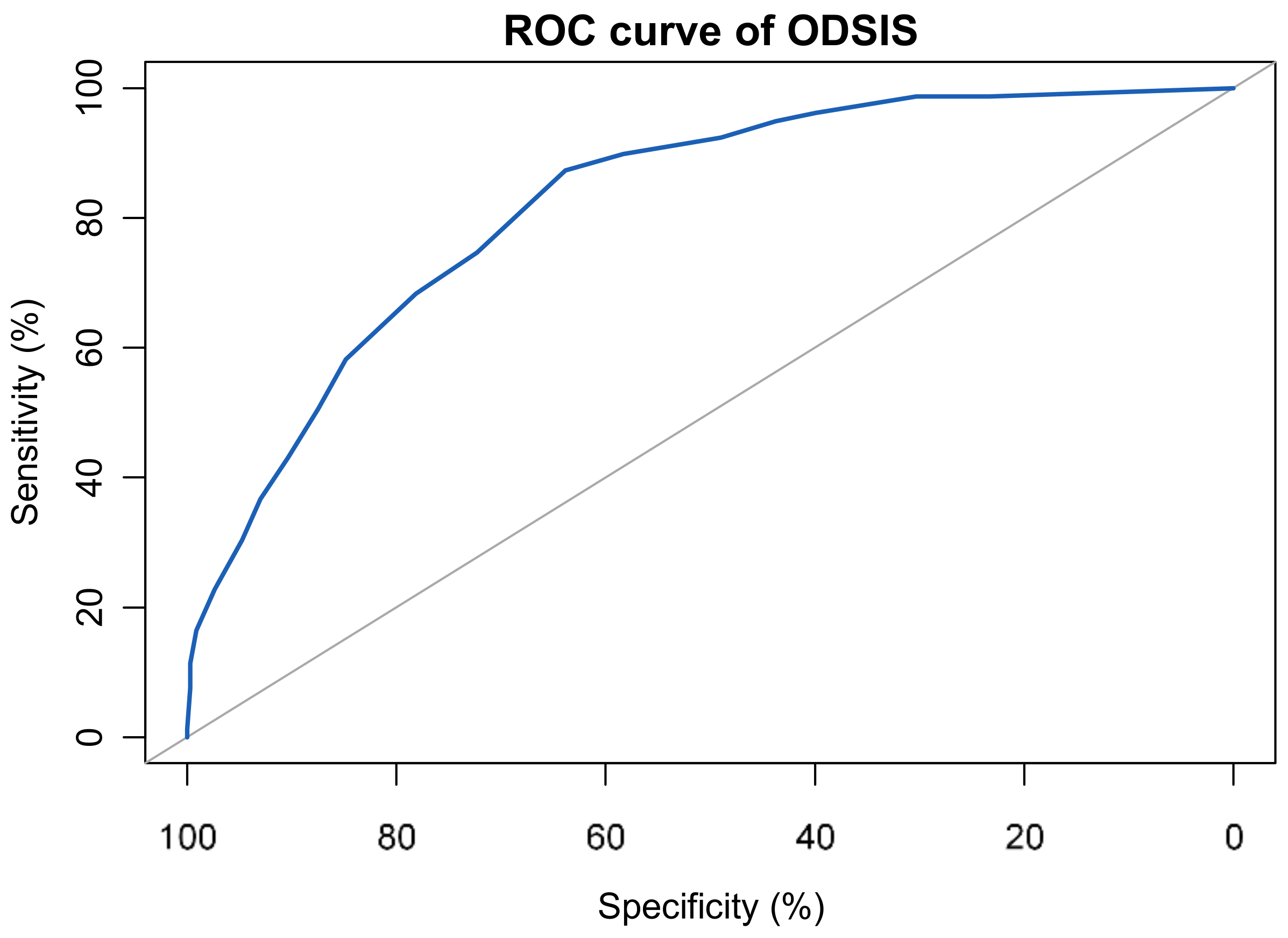
3.6. Sensitivity, Specifity and Cut-Off
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weems, C.F.; Russell, J.D.; Neill, E.L.; Berman, S.L.; Scott, B.G. Existential anxiety among adolescents exposed to disaster: Linkages among level of exposure, PTSD, and depression symptoms. J. Trauma Stress 2016, 29, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Furr, J.M.; Corner, J.S.; Edmunds, J.M.; Kendall, P.C. Disasters and youth: A meta-analytic examination of posttraumatic stress. J. Consult. Clin. Psychol. 2010, 78, 765–780. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Pan, R.Y.; Wan, X.Y.; Tan, Y.L.; Xu, L.K.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- WHO. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Xiong, J.Q.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Antony, M.M.; Orsillo, S.M.; Roemer, L. Practitioner’s Guide to Empirically Based Measures of Anxiety; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2001. [Google Scholar] [CrossRef]
- Beck, A.T.; Brown, G.; Epstein, N.; Steer, R.A. An inventory for measuring clinical anxiety—psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect—the PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Bandelow, B. Assessing the efficacy of treatments for panic disorder and agoraphobia. The panic and agoraphobia scale. Int. Clin. Psychopharmacol. 1995, 10, 73–81. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9—Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Norman, S.B.; Cissell, S.H.; Means-Christensen, A.J.; Stein, M.B. Development and validation of an Overall Anxiety Severity and Impairment Scale (OASIS). Depress. Anxiety 2006, 23, 245–249. [Google Scholar] [CrossRef]
- Norman, S.B.; Campbell-Sills, L.; Hitchcock, C.A.; Sullivan, S.; Rochlin, A.; Wilkins, K.C.; Stein, M.B. Psychometrics of a brief measure of anxiety to detect severity and impairment: The overall anxiety severity and impairment scale (OASIS). J. Psychiatr. Res. 2011, 45, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Robles, A.; Mira, A.; Miguel, C.; Molinari, G.; Diaz-Garcia, A.; Garcia-Palacios, A.; Breton-Lopez, J.M.; Quero, S.; Banos, R.M.; Botella, C. A brief online transdiagnostic measure: Psychometric properties of the Overall Anxiety Severity and Impairment Scale (OASIS) among Spanish patients with emotional disorders. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Osma, J.; Quilez-Orden, A.; Suso-Ribera, C.; Peris-Baquero, O.; Norman, S.B.; Bentley, K.H.; Sauer-Zavala, S. Psychometric properties and validation of the Spanish versions of the overall anxiety and depression severity and impairment scales. J. Affect. Disord. 2019, 252, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermans, M.; Korrelboom, K.; Visser, S. A Dutch version of the Overall Anxiety Severity and Impairment Scale (OASIS): Psychometric properties and validation. J. Affect. Disord. 2015, 172, 127–132. [Google Scholar] [CrossRef]
- Ito, M.; Oe, Y.; Kato, N.; Nakajima, S.; Fujisato, H.; Miyamae, M.; Kanie, A.; Horikoshi, M.; Norman, S.B. Validity and clinical interpretability of Overall Anxiety Severity And Impairment Scale (OASIS). J. Affect. Disord. 2015, 170, 217–224. [Google Scholar] [CrossRef]
- Farrahi, H.; Gharraee, B.; Oghabian, M.A.; Pirmoradi, M.R.; Najibi, S.M.; Batouli, S.A.H. Psychometric Properties of the Persian Version of the Overall Anxiety Severity and Impairment Scale (OASIS). Iran. J. Psychiatry Behav. Sci. 2020, 14. [Google Scholar] [CrossRef]
- Bentley, K.H.; Gallagher, M.W.; Carl, J.R.; Barlow, D.H. Development and Validation of the Overall Depression Severity and Impairment Scale. Psychol. Assess. 2014, 26, 815–830. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Bentley, K.H.; Oe, Y.; Nakajima, S.; Fujisato, H.; Kato, N.; Miyamae, M.; Kanie, A.; Horikoshi, M.; Barlow, D.H. Assessing Depression Related Severity and Functional Impairment: The Overall Depression Severity and Impairment Scale (ODSIS). PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Mira, A.; Gonzalez-Robles, A.; Molinari, G.; Miguel, C.; Diaz-Garcia, A.; Breton-Lopez, J.; Garcia-Palacios, A.; Quero, S.; Banos, R.; Botella, C. Capturing the Severity and Impairment Associated With Depression: The Overall Depression Severity and Impairment Scale (ODSIS) Validation in a Spanish Clinical Sample. Front. Psychiatry 2019, 10, 180. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Norman, S.B.; Craske, M.G.; Sullivan, G.; Lang, A.J.; Chavira, D.A.; Bystritsky, A.; Sherbourne, C.; Roy-Byrne, P.; Stein, M.B. Validation of a brief measure of anxiety-related severity and impairment: The Overall Anxiety Severity and Impairment Scale (OASIS). J. Affect. Disord. 2009, 112, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, S.A.; Welch, S.S.; Michonski, J.; Poquiz, J.; Osborne, T.L.; Sayrs, J.; Spanos, A. Psychometric evaluation of the Overall Anxiety Severity And Impairment Scale (OASIS) in individuals seeking outpatient specialty treatment for anxiety-related disorders. J. Affect. Disord. 2015, 175, 463–470. [Google Scholar] [CrossRef]
- Bragdon, L.B.; Diefenbach, G.J.; Hannan, S.; Tolin, D.F. Psychometric properties of the Overall Anxiety Severity and Impairment Scale (OASIS) among psychiatric outpatients. J. Affect. Disord. 2016, 201, 112–115. [Google Scholar] [CrossRef] [PubMed]
- McCrae, R.R.; Costa, P.T. Validation of the 5-factor model of personality across instruments and observers. J. Personal. Soc. Psychol. 1987, 52, 81–90. [Google Scholar] [CrossRef]
- Svoboda, M. Psychologická Diagnostika Dospělých; Portal: Praha, Czech Republic, 1999. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Lowe, B. A brief measure for assessing generalized anxiety disorder—The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargha, A.; Delaney, H.D. A critique and improvement of the CL common language effect size statistics of McGraw and Wong. J. Educ. Behav. Stat. 2000, 25, 101–132. [Google Scholar] [CrossRef]
- Novák, L.; Malinakova, K.; Tavel, P.; Sandora, J. Czech Version of the short Overall Anxiety Severity and Impairment Scale (OASIS) and the Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation. Available online: osf.io/r483d (accessed on 30 May 2021).
- Mayers, L.S.; Gamst, G.; Guarino, A.J. Applied Multivariate Research: Design and Interpretation, 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–59. [Google Scholar] [CrossRef]
- Civelek, M.E. Essentials of Structural Equation Modeling; Zea Books: Lincoln, NE, USA, 2018. [Google Scholar]
- Hoe, S.L. Issues and Procedures in Adopting Structural Equation Modelling Technique. J. Appl. Quant. Methods 2008, 3, 76–83. [Google Scholar]
- Vandenberg, R.J.; Lance, C.E. A Review and Synthesis of the Measurement Invariance Literature: Suggestions, Practices, and Recommendations for Organizational Research. Organ. Res. Methods 2000, 3, 4–70. [Google Scholar] [CrossRef]
- Jackson, D.L.; Gillaspy, J.A.; Purc-Stephenson, R. Reporting Practices in Confirmatory Factor Analysis: An Overview and Some Recommendations. Psychol. Methods 2009, 14, 6–23. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Eisinga, R.; te Grotenhuis, M.; Pelzer, B. The reliability of a two-item scale: Pearson, Cronbach, or Spearman-Brown? Int. J. Public Health 2013, 58, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Aust, F.; Barth, M. Papaja: Create APA Manuscripts with R Markdown; R Package Version: Vienna, Austria, 2020. [Google Scholar]
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Northwestern University: Evanston, IL, USA, 2020. [Google Scholar]
- Peters, G.-J.Y. ufs: Quantitative Analysis Made Accessible; R Package Version: Vienna, Austria, 2018. [Google Scholar]
- Rathbone, A.; Shaw, S.; Kumbhare, D. ICC.Sample.Size: Calculation of Sample Size and Power for ICC; R Package Version: Vienna, Austria, 2015. [Google Scholar]
- Ahmed, M.; Hamid, R.; Hussain, G.; Bux, M.; Ahmed, N.; Kumar, M. Anxiety and depression in medical students of Sindh province during the Covid-19 pandemic. Rawal Med. J. 2020, 45, 947–950. [Google Scholar]
- Fawaz, M.; Samaha, A. E-learning: Depression, anxiety, and stress symptomatology among Lebanese university students during COVID-19 quarantine. Nurs. Forum 2021, 56, 52–57. [Google Scholar] [CrossRef]
- Faisal, R.A.; Jobe, M.C.; Ahmed, O.; Sharker, T. Mental Health Status, Anxiety, and Depression Levels of Bangladeshi University Students During the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2021. [Google Scholar] [CrossRef]
- Odriozola-Gonzalez, P.; Planchuelo-Gomez, A.; Irurtia, M.J.; de Luis-Garcia, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290. [Google Scholar] [CrossRef] [PubMed]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- Dlugosz, P. Factors influencing mental health among American youth in the time of the Covid-19 pandemic. Personal. Individ. Differ. 2021, 175, 110711. [Google Scholar] [CrossRef]
- Shreve-Neiger, A.K.; Edelstein, B.A. Religion and anxiety: A critical review of the literature. Clin. Psychol. Rev. 2004, 24, 379–397. [Google Scholar] [CrossRef]
- AbdAleati, N.S.; Zaharim, N.M.; Mydin, Y.O. Religiousness and Mental Health: Systematic Review Study. J. Relig. Health 2016, 55, 1929–1937. [Google Scholar] [CrossRef]
- Ellis, L.; Wahab, E.A. Religiosity and Fear of Death: A Theory-Oriented Review of the Empirical Literature. Rev. Relig. Res. 2013, 55, 149–189. [Google Scholar] [CrossRef]
- Jong, J.; Ross, R.; Philip, T.; Chang, S.H.; Simons, N.; Halberstadt, J. The religious correlates of death anxiety: A systematic review and meta-analysis. Relig. Brain Behav. 2018, 8, 4–20. [Google Scholar] [CrossRef]
- Malinakova, K.; Tavel, P.; Meier, Z.; van Dijk, J.P.; Reijneveld, S.A. Religiosity and Mental Health: A Contribution to Understanding the Heterogeneity of Research Findings. Int. J. Environ. Res. Public Health 2020, 17, 494. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Sample 1 | Sample 2 | Sample 3 | Sample 4 | OASIS Differences | ODSIS Differences |
|---|---|---|---|---|---|---|
| Gender | ||||||
| 1. Male | 702 (50%) | 503 (50%) | 3 (30%) | 85 (17%) | ||
| 2. Female | 691 (50%) | 512 (50%) | 7 (70%) | 409 (83%) | ||
| Family status | ||||||
| 1. No relationship/widowed/divorced | 476 (34%) | 519 (51%) | 2 (20%) | 332 (67%) | ||
| 2. In a relationship/married | 917 (66%) | 496 (49%) | 8 (80%) | 162 (33%) | ||
| Education | ||||||
| 1. Elementary school/vocational school | 749 (54%) | 469 (46%) | 28 (5.7%) | |||
| 2. High school or higher vocational school (HVS) | 467 (34%) | 374 (37%) | 4 (40%) | 221 (45%) | ||
| 3. HSV or University bachelor | 37 (3.7%) | 5 (50%) | 107 (22%) | |||
| 4. University master’s or higher | 132 (13%) | 1 (10%) | 138 (28%) | |||
| 5. University unspecified | 177 (13%) | |||||
| Economic status | ||||||
| 1. Working | 754 (54%) | 551 (54%) | 265 (54%) | |||
| 2. Not working | 124 (8.9%) | 90 (8.9%) | ||||
| 3. Pensioner | 438 (31%) | 318 (31%) | 5 > 4 (p = 0.008, Ȃ = 0.35) | 5 > 4 (p = 0.010, Ȃ = 0.35) | ||
| 4. Student | 77 (5.5%) | 53 (5.2%) | 143 (28%) | 5 > 1 (p = 0.008, Ȃ = 0.36) | 5 > 1 (p = 0.011, Ȃ = 0.36) | |
| 5. Other | 86 (17%) | |||||
| Faith | ||||||
| 1. No, I am a convinced atheist | 179 (13%) | 1 (10%) | 47 (9.6%) | 1 < 4 (p = 0.014; Ȃ = 0.4), 1 < 3 (p = 0.031; Ȃ = 0.57), | ||
| 2. Non-religious | 731 (52%) | 4 (40%) | 182 (37%) | |||
| 3. Yes, but I am not a member of church/religious society | 362 (26%) | 3 (30%) | 199 (41%) | 3 > 2 (p = 0.001, Ȃ = 0.43) | 3 > 2 (p = 0.006, Ȃ = 0.42) | |
| 4. Yes, I am a member of church/religious society | 121(8.7%) | 2 (20%) | 62 (13%) | 5 > 6 (p = 0.002, Ȃ = 0.4) |
| Model | ×2 | df | p-Value | CFI | TLI | RMSEA | RMSEA 90%CI lb | RMSEA 90%CI ub | SRMR |
|---|---|---|---|---|---|---|---|---|---|
| OASIS | |||||||||
| Overall model | 38.276 | 4 | p < 0.001 | 0.999 | 0.997 | 0.078 | 0.057 | 0.102 | 0.027 |
| Male model | 26.276 | 4 | p < 0.001 | 0.999 | 0.997 | 0.089 | 0.059 | 0.123 | 0.031 |
| Female model | 11.251 | 4 | p = 0.024 | 0.999 | 0.999 | 0.051 | 0.017 | 0.088 | 0.022 |
| Configural model | 37.527 | 8 | p < 0.001 | 0.999 | 0.998 | 0.073 | 0.05 | 0.097 | 0.027 |
| Metric model | 40.716 | 12 | p < 0.001 | 0.999 | 0.999 | 0.059 | 0.039 | 0.079 | 0.028 |
| Scalar model | 74.638 | 26 | p < 0.001 | 0.999 | 0.999 | 0.052 | 0.038 | 0.066 | 0.027 |
| Strict model | 74.638 | 26 | p < 0.001 | 0.999 | 0.999 | 0.052 | 0.038 | 0.066 | 0.027 |
| ODSIS | |||||||||
| Overall model | 36.538 | 4 | p < 0.001 | 0.999 | 0.999 | 0.076 | 0.055 | 0.1 | 0.021 |
| Male model | 28.207 | 4 | p < 0.001 | 0.999 | 0.998 | 0.093 | 0.062 | 0.127 | 0.026 |
| Female model | 10.107 | 4 | p = 0.039 | 1 | 1 | 0.047 | 0.01 | 0.084 | 0.016 |
| Configural model | 38.314 | 8 | p < 0.001 | 0.999 | 0.999 | 0.074 | 0.051 | 0.098 | 0.021 |
| Metric model | 49.469 | 12 | p < 0.001 | 0.999 | 0.999 | 0.067 | 0.048 | 0.087 | 0.023 |
| Scalar model | 52.548 | 26 | p = 0.002 | 1 | 1 | 0.038 | 0.023 | 0.053 | 0.022 |
| Strict model | 52.548 | 26 | p = 0.002 | 1 | 1 | 0.038 | 0.023 | 0.053 | 0.022 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | M | SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. OASIS | - | 9.50 | 4.25 | ||||||||
| 2. ODSIS | 0.83 *** | - | 8.73 | 4.34 | |||||||
| 3. Gender | 0.17 *** | 0.09 *** | - | 1.50 | 0.50 | ||||||
| 4. BFI_N | 0.54 *** | 0.51 *** | 0.09 ** | - | 2.76 | 0.73 | |||||
| 5. RSES | −0.40 *** | −0.42 *** | −0.05 | −0.53 *** | - | 28.89 | 4.69 | ||||
| 6. PANAS-P | 0.23 *** | 0.20 *** | −0.02 | 0.07 ** | 0.03 | - | 28.83 | 9.77 | |||
| 7. PANAS-N | 0.56 *** | 0.53 *** | 0.06 * | 0.45 *** | −0.30 *** | 0.61 *** | - | 18.27 | 7.58 | ||
| 8. Age | −0.11 *** | −0.16 *** | 0.08 ** | −0.22 *** | 0.21 *** | −0.16 *** | −0.17 *** | - | 48.29 | 16.42 | |
| 9. Education | 0.01 | −0.03 | 0.20 *** | −0.01 | 0.07 * | 0.08 ** | 0.06 * | −0.07 ** | - | 2.51 | 0.82 |
| 10. Faith | 0.09 *** | 0.08 ** | 0.05 | 0.02 | −0.01 | 0.04 | 0.01 | 0.04 | 0.09 ** | 1.78 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandora, J.; Novak, L.; Brnka, R.; van Dijk, J.P.; Tavel, P.; Malinakova, K. The Abbreviated Overall Anxiety Severity and Impairment Scale (OASIS) and the Abbreviated Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation of the Czech Versions. Int. J. Environ. Res. Public Health 2021, 18, 10337. https://doi.org/10.3390/ijerph181910337
Sandora J, Novak L, Brnka R, van Dijk JP, Tavel P, Malinakova K. The Abbreviated Overall Anxiety Severity and Impairment Scale (OASIS) and the Abbreviated Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation of the Czech Versions. International Journal of Environmental Research and Public Health. 2021; 18(19):10337. https://doi.org/10.3390/ijerph181910337
Chicago/Turabian StyleSandora, Jan, Lukas Novak, Robert Brnka, Jitse P. van Dijk, Peter Tavel, and Klara Malinakova. 2021. "The Abbreviated Overall Anxiety Severity and Impairment Scale (OASIS) and the Abbreviated Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation of the Czech Versions" International Journal of Environmental Research and Public Health 18, no. 19: 10337. https://doi.org/10.3390/ijerph181910337
APA StyleSandora, J., Novak, L., Brnka, R., van Dijk, J. P., Tavel, P., & Malinakova, K. (2021). The Abbreviated Overall Anxiety Severity and Impairment Scale (OASIS) and the Abbreviated Overall Depression Severity and Impairment Scale (ODSIS): Psychometric Properties and Evaluation of the Czech Versions. International Journal of Environmental Research and Public Health, 18(19), 10337. https://doi.org/10.3390/ijerph181910337