
Analysis of Factors Affecting Employment Status of Kidney Transplant Recipients in Selected European Union Member States

 , ,
, ,
Abstract
:1. Introduction
Objectives
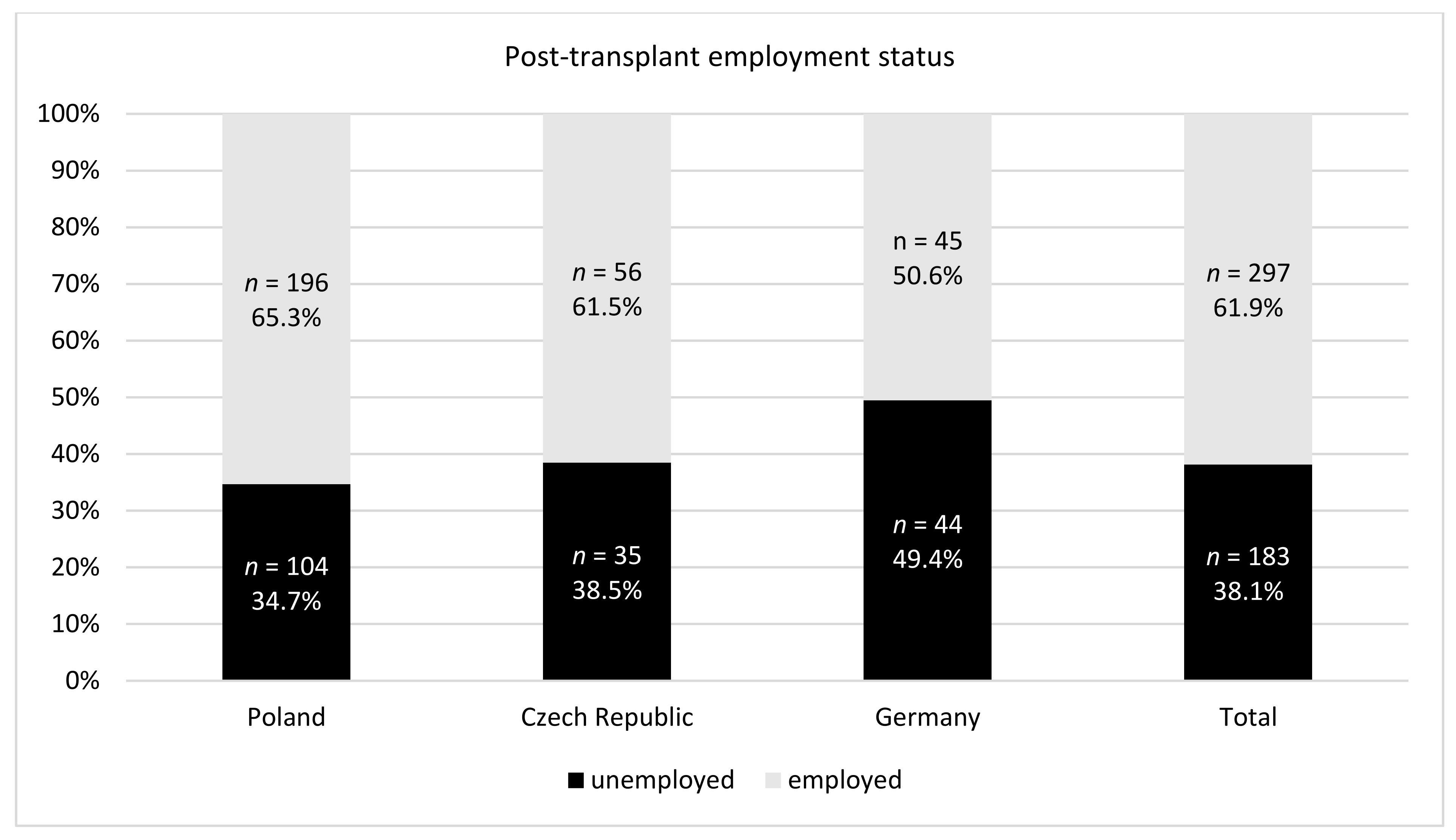
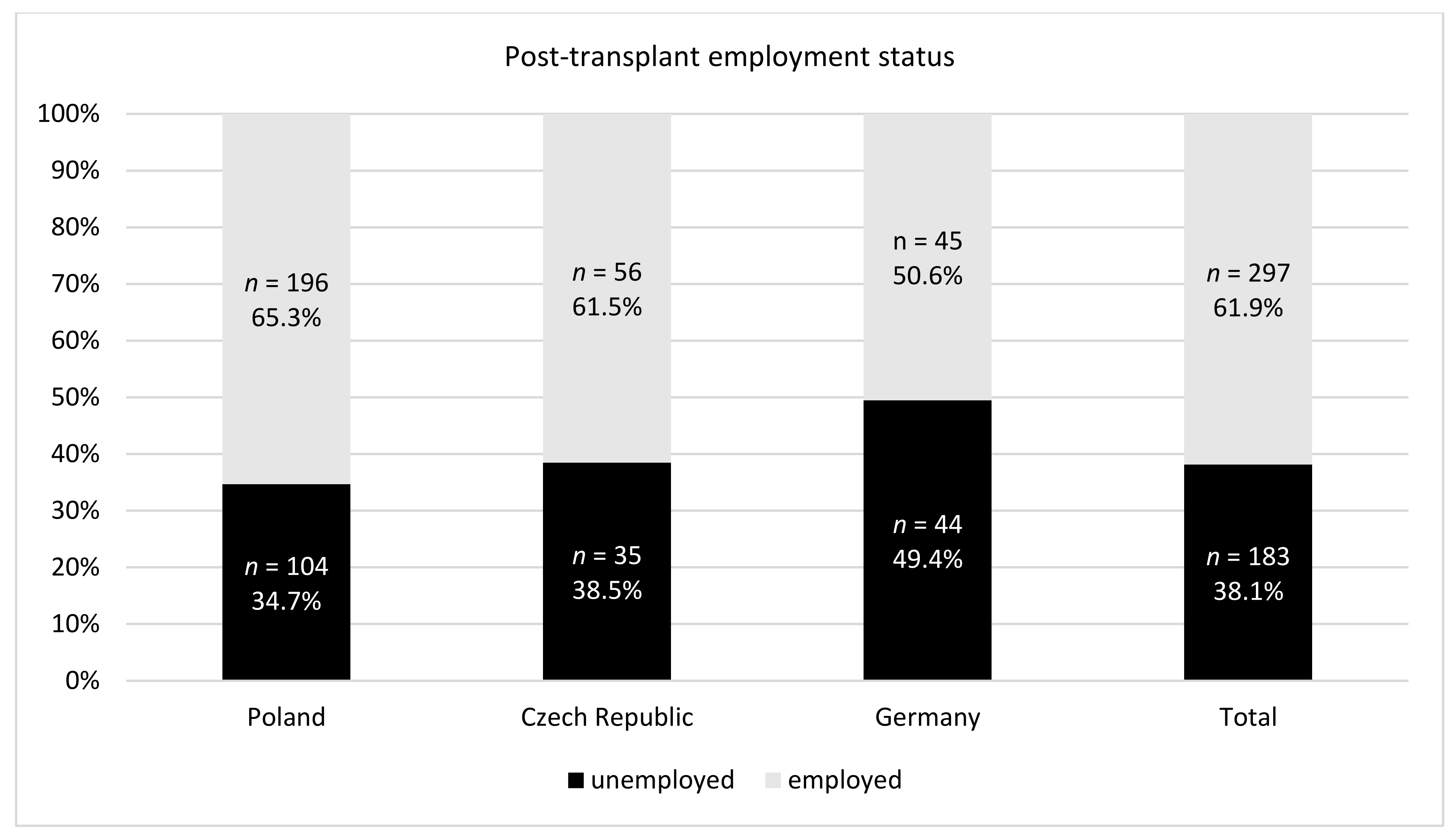
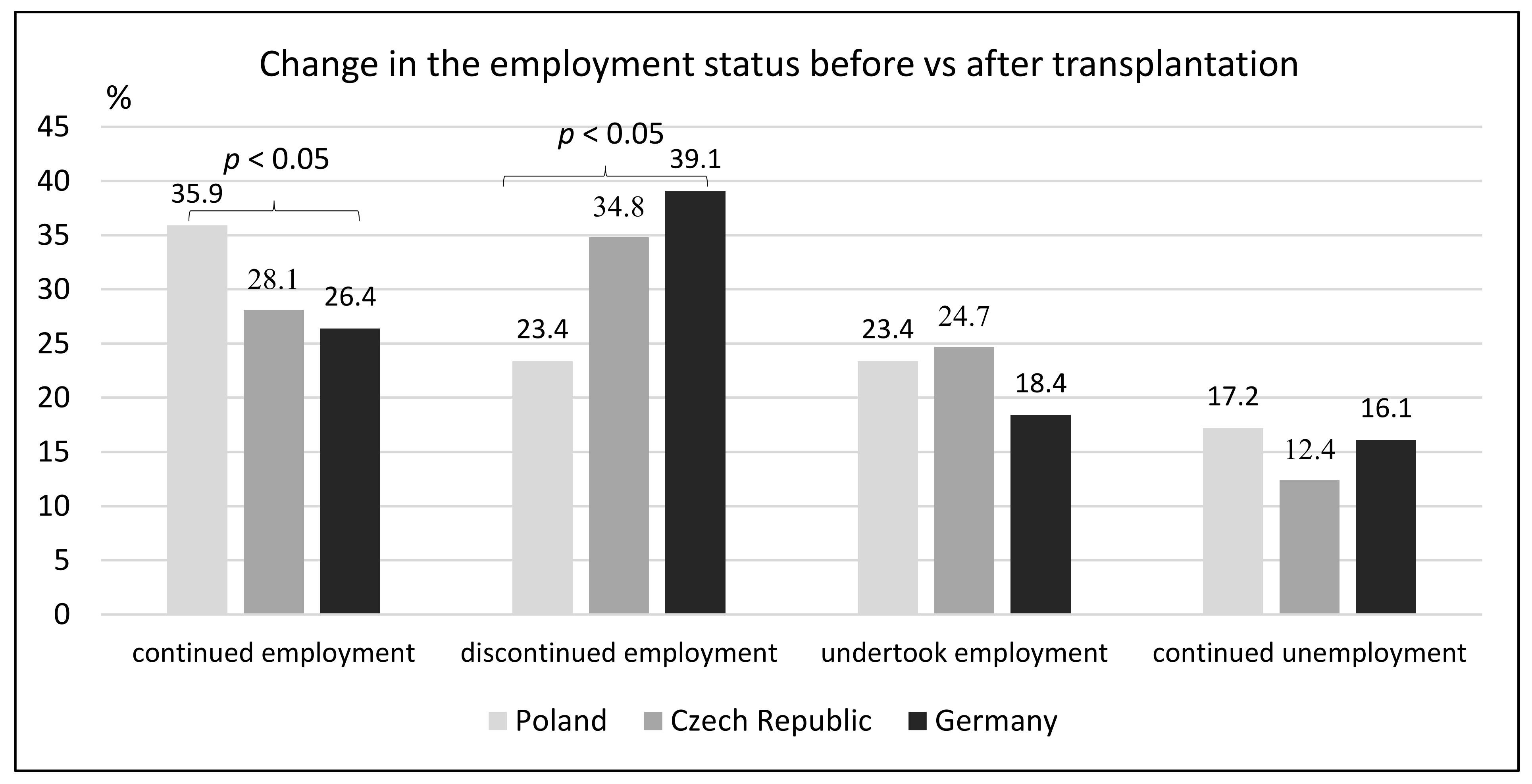
- To assess the re-employment rate after kidney transplantation in selected EU member states
- To identify the factors determining the rate of occupational inactivity after kidney transplantation
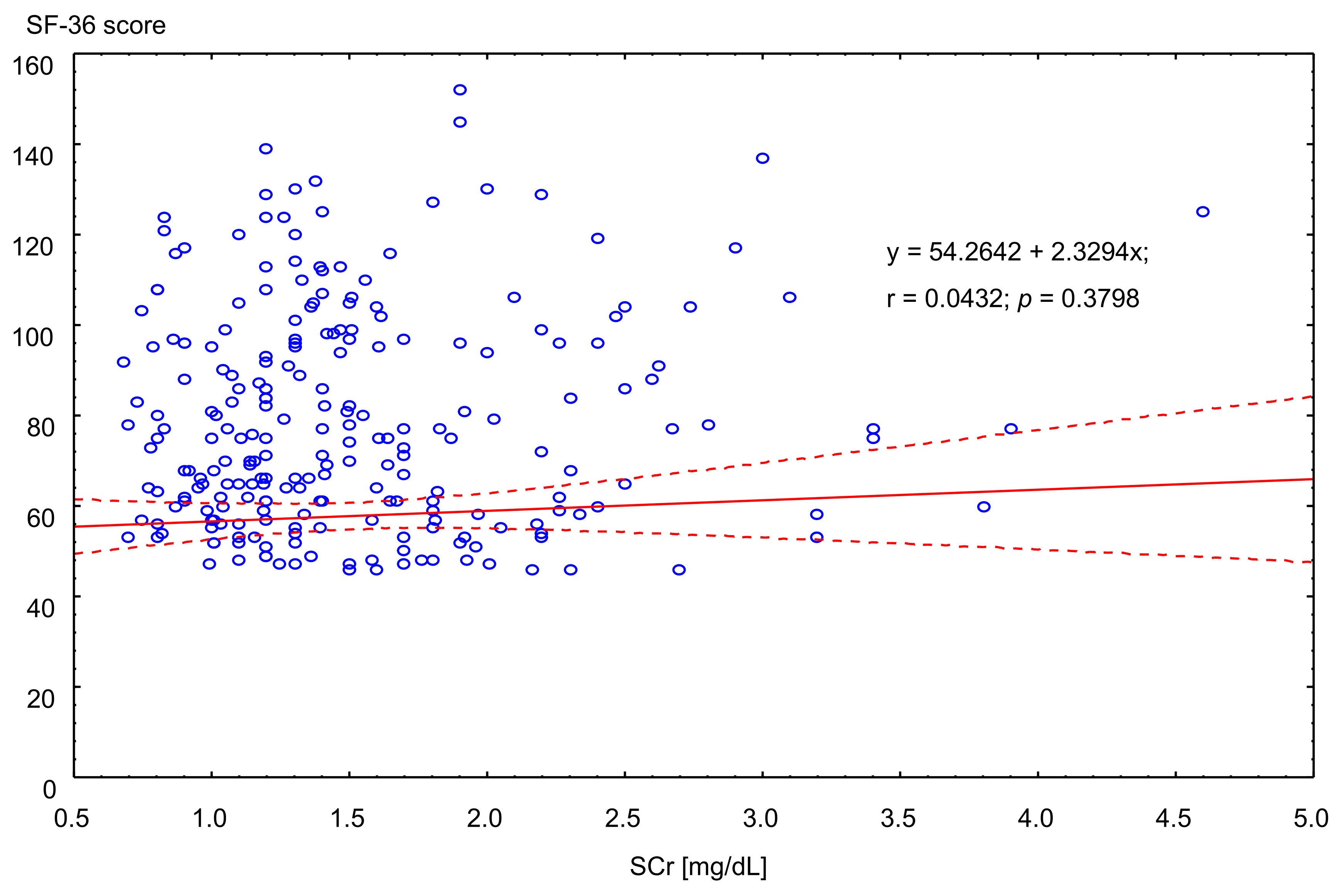
- To evaluate the correlation between the kidney function (as an objective factor) and quality of life (as a subjective factor) and the post-transplant employment status
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
- Gender, low level of education, and rural residency correlates with post-transplant occupational inactivity
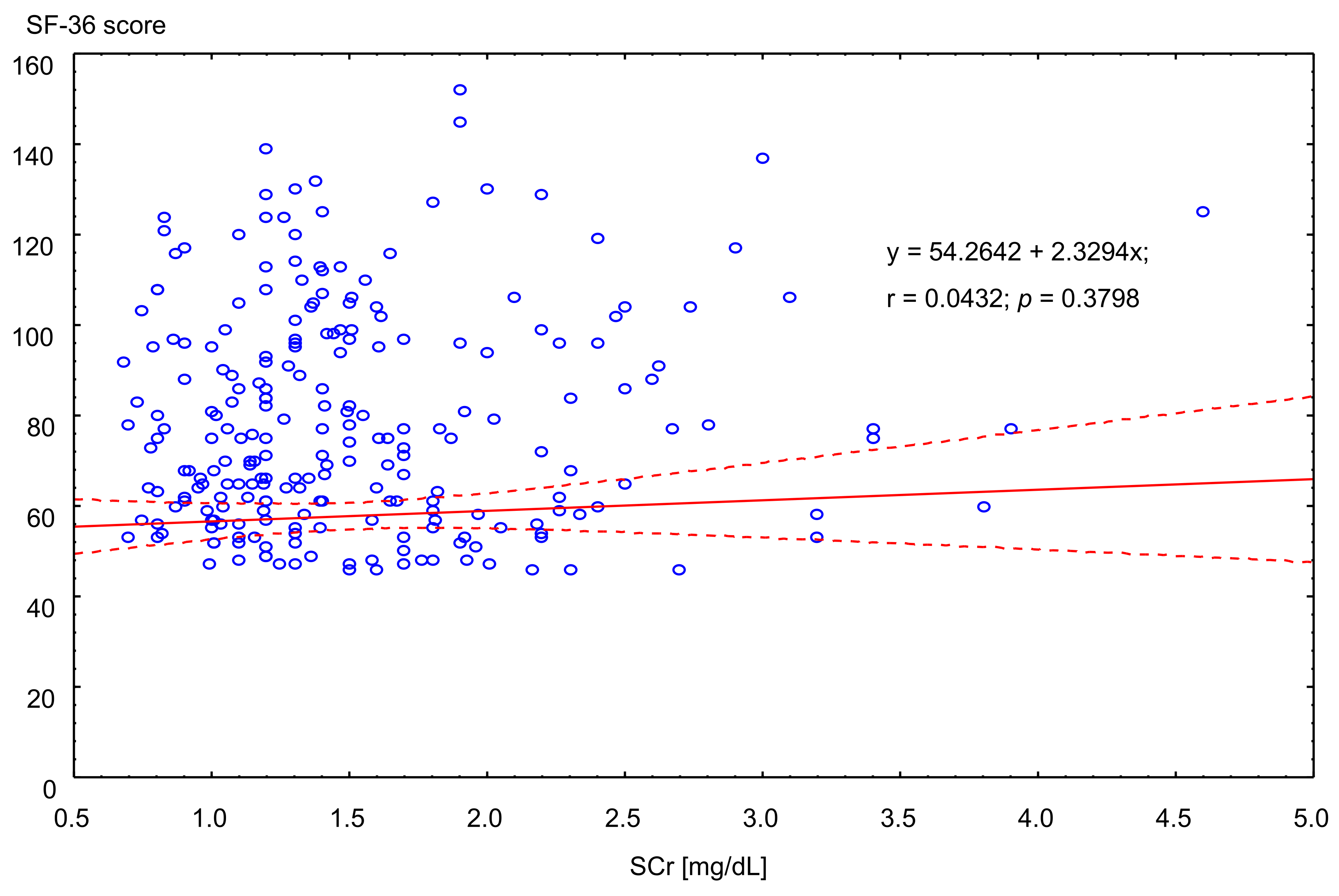
- Unemployed kidney recipients present with lower quality of life, but it is not linked with kidney function
- Superior post-transplant social provisions may create the conditions for occupational idleness.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Markussen, S.; Roed, K. The Impacts of Vocational Rehabilitation. Labour Econ. 2014, 31, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tzvetanow, I.; D’Amico, G.; Walczak, D.; Jeon, H.; Garcia-Roca, R.; Oberholzer, J.; Benedetti, E. High rate of unemployment after kidney transplantation: Analysis of the United Network for Organ Sharing Database. Transplant Proc. 2014, 46, 1290–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, E.; Baird, B.C.; Barenbaum, L.L.; Leviatov, A.; Koford, J.K.; Shihab, F.; Goldfarb-Rumyantzev, A.S. The impact of employment status on recipient and renal allograft survival. Clin. Transpl. 2008, 22, 428–438. [Google Scholar] [CrossRef] [PubMed]
- De Baere, C.; Delva, D.; Kloeck, A.; Kathleen, R.; Yves, V.; Geert, V.; Johan, V.; Frederik, N.; Fabienne, D. Return to work and social participation: Does type of organ transplantation matter? Transplantation 2010, 89, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Callahan, M.B.; Paris, W. Kidney patient employment and its relationship to physical impairment. J. Nephrol. Soc. Work. 2009, 30, 9–15. [Google Scholar]
- Tylka, J.; Piotrowicz, R. Quality of life questionnaire SF-36—Polish version. Kardiol. Pol. 2009, 67, 1166–1169. [Google Scholar] [PubMed]
- Björnberg, A. Health Consumer Powerhouse Euro Health Consumer Index 2017 Report, Health Consumer Powerhouse. 2018. Available online: https://healthpowerhouse.com/2018-01-29 (accessed on 19 February 2020).
- Terada, I.; Hyde, C. The SF-36: An instrument for measuring quality of life in ESRD patients. TNA/ERCA J. 2002, XXVIII, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.; Gould, D.; Wainwright, S.; Fallon, M. Quality of life after renal transplantation. J. Clin. Nurs. 1998, 7, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Evers, A. The new Long-Term Care Insurance Program in Germany. J. Aging Soc. Policy 1998, 10, 77–98. [Google Scholar] [CrossRef] [PubMed]
- Health–Nutrition–Prevention–Insurance. Available online: https://www.krankenkassenzentrale.de (accessed on 28 June 2021).
- Danuser, B.; Simcox, A.; Studer, R.; Koller, M.; Wild, P. Employment 12 months after kidney transplantation: An in-depth bio-psycho-social analysis of the Swiss Transplant Cohort. PLoS ONE 2017, 12, e0175161. [Google Scholar] [CrossRef] [PubMed]
- Nour, N.; Heck, K.S.; Ross, H. Factors related to participation in paid work after organ transplantation: Perceptions of kidney transplant recipients. J. Occup. Rehabil. 2015, 25, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Van der Mei, S.F.; Krol, B.; van Son, W.J.; de Jong, P.E.; Groothoff, J.W.; van den Heuvel, W.J.A. Social participation and employment status after kidney transplantation: A systematic review. Qual. Life Res. 2006, 15, 979–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raiz, L. The transplant trap: The impact of health policy on employment status following renal transplantation. Health Soc. Policy 1997, 8, 67–87. [Google Scholar] [CrossRef] [PubMed]
- Matas, A.J.; Lawson, W.; McHugh, L.; Gillingham, K.; Payne, W.D.; Dunn, D.L.; Gruessner, R.W.G.; Sutherland, D.E.R.; Najarian, J.S. Employment patterns after successful kidney transplantation. Transplantation 1996, 61, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Markell, M.S.; DiBendetto, A.; Maursky, V.; Sumrani, N.; Hong, J.H.; Distant, D.A.; Miles, A.M.; Sommer, B.G.; Friedman, E.A. Unemployment in inner-city renal recipients: Predictive and sociodemographic factors. Am. J. Kidney Dis. 1997, 29, 881–887. [Google Scholar] [CrossRef]
- Callahan, M.B.; Paris, W.; Moncrief, M. Kidney Transplant Patient employment: Vocational Training and intervention by use of an impairment rather than disability Model—The job club. J. Nephrol. Soc. Work. 2010, 34, 52–60. [Google Scholar]
- Kelly, E.L.; Dobbin, F. Civil Rights Law at Work: Sex Discrimination and the Rise of Maternity Leave Policies. Am. J. Sociol. 1999, 105, 455–492. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Poland | Czech Republic | Germany | p | |
|---|---|---|---|---|
| Female | N = 176 (59.5%) | N = 59 (64.8%) | N = 45 (50.6%) | ns |
| Male | N = 120 (40.55%) | N = 32 (35.2%) | N = 44 (49.4%) | ns |
| Age (years) | ||||
| 20–20 | N = 22 (7.4%) | N = 5 (5.5%) | N = 10 (11.2%) | ns |
| 30–39 | N = 68 (23.0%) | N = 9 (9.9%) | N = 8 (9.0%) | 0.001 |
| 40–49 | N = 75 (25.3%) | N = 19 (20.9%) | N = 24 (27.0%) | ns |
| 50–65 | N = 131 (44.3%) | N = 58 (63.7%) | N = 46 (51.7%) | ns |
| Education | ||||
| Basic | N = 19 (6.4%) | N = 7 (7.7%) | N = 8 (9.0%) | ns |
| Professional | N = 82 (27.7%) | N = 37 (40.7%) | N = 41 (46.1%) | 0.0424 |
| Secondary | N = 127 (42.9%) | N = 34 (37.4%) | N = 21 (23.6%) | 0.011 |
| University | N = 68 (23.0%) | N = 13 (14.3%) | N = 19 (21.4%) | ns |
| Place of residency | ||||
| Rural | N = 112 (37.8%) | N = 31 (34.1%) | N = 22 (24.7%) | ns |
| Suburban | N = 110 (37.5%) | N = 36 (39.6%) | N = 16 (18.0%) | ns |
| Urban | N = 73 (24.7%) | N = 24 (26.4%) | N = 51 (57.3%) | 0.002 |
| Time of pre-transplant dialysis (months: mean, SD) | 27 (±23) | 28 (±25) | 59 (±45) | 0.000 |
| Time since transplantation (months: mean, SD) | 94 (±66) | 90 (±76) | 89 (±65) | 0.777 |
| OR (95% CI) | p | |
|---|---|---|
| Gender M vs. F | 1.9 (1.31–2.75) | 0.0007 |
| Age (years) | ||
| 30–39 vs. 20–30 | 2.69 (1.21–5.98) | 0.0156 |
| 40–49 vs. 20–30 | 2.85 (1.32–6.12) | 0.0074 |
| 50–65 vs. 20–30 | 0.94 (0.47–1.91) | 0.8739 |
| Education | ||
| professional vs. basic | 2.92 (1.2–7.11) | 0.0179 |
| Secondary vs. basic | 5.89 (2.44–14.25) | 0.0001 |
| University vs. basic | 9.78 (3.82–25.02) | 0.0000 |
| Place of residency | ||
| Suburban vs. rural | 1.93 (1.24–2.99) | 0.0034 |
| Urban vs. rural | 1.89 (1.21–2.97) | 0.0054 |
| Employment during pre-transplant period of dialyses (yes vs. no) | 1.68 (1.16–2.43) | 0.0060 |
| Unemployed | Employed | p | |||
|---|---|---|---|---|---|
| n | SF36 Median (Q1–Q3) | n | SF36 Median (Q1–Q3) | ||
| Poland | 103 | 74 (47–99) | 185 | 53 (30–69) | <0.01 |
| Czech Republic | 32 | 70.5 (47–92) | 53 | 44.5 (24–57.5) | <0.05 |
| Germany | 42 | 59.5 (38.5–73.5) | 41 | 37.5 (22–50) | <0.01 |
| All patients | 177 | 69.9 (45.4–81.5) | 279 | 49.1 (25.2–58.6) | <0.05 |
| Unemployed | Employed | p | |||
|---|---|---|---|---|---|
| n | Average SCr (mg/dL) | n | Average SCr (mg/dL) | ||
| Poland | 103 | 1.61 (0.55–4.60) | 185 | 1.52 (0.73–3.90) | ns |
| Czech Republic | 32 | 1.68 (0.59–3.05) | 53 | 1.54 (0.68–4.64) | ns |
| Germany | 42 | 1.78 (0.90–3.40) | 41 | 1.64 (0.86–3.20) | ns |
| All patients | 177 | 1.66 | 279 | 1.54 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wlodarczyk, E.; Viklický, O.; Budde, K.; Kolářová, M.; Bergfeld, L.; Paczek, L.; Mucha, K.; Glyda, M.; Wlodarczyk, Z. Analysis of Factors Affecting Employment Status of Kidney Transplant Recipients in Selected European Union Member States. Int. J. Environ. Res. Public Health 2021, 18, 10284. https://doi.org/10.3390/ijerph181910284
Wlodarczyk E, Viklický O, Budde K, Kolářová M, Bergfeld L, Paczek L, Mucha K, Glyda M, Wlodarczyk Z. Analysis of Factors Affecting Employment Status of Kidney Transplant Recipients in Selected European Union Member States. International Journal of Environmental Research and Public Health. 2021; 18(19):10284. https://doi.org/10.3390/ijerph181910284
Chicago/Turabian StyleWlodarczyk, Elzbieta, Ondřej Viklický, Klemens Budde, Marie Kolářová, Leon Bergfeld, Leszek Paczek, Krzysztof Mucha, Maciej Glyda, and Zbigniew Wlodarczyk. 2021. "Analysis of Factors Affecting Employment Status of Kidney Transplant Recipients in Selected European Union Member States" International Journal of Environmental Research and Public Health 18, no. 19: 10284. https://doi.org/10.3390/ijerph181910284
APA StyleWlodarczyk, E., Viklický, O., Budde, K., Kolářová, M., Bergfeld, L., Paczek, L., Mucha, K., Glyda, M., & Wlodarczyk, Z. (2021). Analysis of Factors Affecting Employment Status of Kidney Transplant Recipients in Selected European Union Member States. International Journal of Environmental Research and Public Health, 18(19), 10284. https://doi.org/10.3390/ijerph181910284