2. Materials and Methods
This research, carried out between 2019 and 2020, collected twenty cases in four charity centers distributed throughout Spain (Castelló, Madrid, Albacete, and Catalonia), as well as contextual data and numerous testimonies from volunteers and social workers (in-depth interviews with six technicians and four volunteers).
2.1. Mixed-Methods Approach
The research adopted a mixed-methods approach drawing on primary sociodemographic data, ethnography, and two kinds of interviews: first, semi-structured interviews aimed to collect sociodemographic data, life histories, and introspective insights about the experience of poverty and exclusion; and second, computer-assisted personal interviews (CAPI) were used to obtain egocentric or personal network data, thus complementing the qualitative methods with structured network data [
35].
The ethnographic perspective allowed us to document the interactions between the various actors involved in the social fabric (users, volunteers, social workers) and to analyze the context of social interactions (social shelters, soup kitchens, medical centers, etc.) through multi-sited fieldwork [
36]. The semi-structured interview, which usually took around two hours, consisted of three parts. In the first part, individual data (place of birth, age, marital status, number of children, level of studies, employment situation, informal income, incoming social benefits, etc.) were asked for. The second part explored the individual’s life history and his/her economic, labor, health, and family situation. Finally, the third part explored the subjective and emotional aspects of the experience of poverty. The interviews were recorded and transcribed with the explicit permission of the interviewees and later analyzed through coding and contextual analysis.
For the personal network analysis, we used Egonet, which is a software package that integrates questionnaires, analysis, and the visualization of personal networks. The approach consists of analyzing the social relationships that an individual (i.e., ego) maintains with the other network members, i.e., his or her alters. We used several name generators to capture alters who provided different types of support (material, emotional, etc.). Furthermore, we collected data on the characteristics of the alters themselves. For the purposes of our study, we selected the following characteristics: sex, type of relationship with ego (father, mother, friend, professional worker, etc.), perceived degree of proximity (I feel close, very close…, etc.), interaction frequency (I meet/communicate very often, often, rarely, etc.) and duration (less than 1 year, between 1 and 5 years, more than 5 years, a lifetime), perceived financial situation from ego’s point of view (better than me, like me, worse than me) and occupational background (high, medium, or low professional skills). Finally, to visualize each network’s structure, we gathered information on the relationship among the alters (“Does Y1 know Y2, Y3, …, Yn?”). Thus, the analysis of personal networks makes it possible to analyze empirically the relational dimension of poverty through the characteristics of the users’ networks and the volume and type of support that flows through them.
The phase of preparing, collecting, processing, and storing personal data follows basic rules, such as anonymizing the data or removing names or other direct identifiers. The names used in this paper are pseudonyms, including that of the charity, and we have removed all sensitive information. All participants were adequately informed of the study’s objectives and procedures, of the voluntary nature of their participation in the study, and of their right to end the interview at any time. The researcher also requested the interviewee’s explicit consent to the interview being recorded before the interview started.
2.2. Sampling
The sample was intentional, aiming at maximizing the diversity of cases and situations in order to acquire a broad vision of the phenomenon. In the present paper, we focus specifically on the cases of users who have suffered severe exclusion and homelessness (i.e., MEH): we found twelve individuals with this profile, nine men and three women, who displayed certain regularities in their personal networks, exclusion processes, and sociodemographic factors. The mean age of informants was 52.2 years in a range from 41 to 65 years (and a median of 51 years). Significantly, in this subsample, all the individuals were single, divorced, or had no known stable partner, except for three individuals who had a temporary relationship with other users of the charitable institution (a couple from the sample and a man with another user). Regarding origins, eleven were born in Spain and one was born abroad. At the time of the interviews, only three were working, the remainder counting as long-term unemployed, although in the past, most of them had had different kinds of temporary employment, e.g., as a cook, artist, factory worker, or hairdresser). Eight out of the twelve had only a basic educational background; two had achieved intermediate educational levels (baccalaureate or professional training), while the remaining two lacked any academic background. In the past, they had all had some problems with substance abuse in the form of alcohol or drugs, and a couple of them were still dependent on it. They were all suffering from different health problems, particularly psychological disorders. At some point in their lives, most had lived on the street for varying lengths of time, from a few months to several years. At the time of the interview, most were renting a room, had been given accommodation by a relative, or were staying in a social shelter under the charity’s supervision.
3. Results
This section presents the life backgrounds, support networks, and impact of charities on users’ personal networks. We first describe Laureano’s case, which exemplifies those who have to resort to charity sporadically because of episodic financial shortages. Due to their relatively wide social links, they usually manage to overcome the impasse despite their financial vulnerability. Next, we will present the specific cases of people experiencing MEH whom the charitable institution deals with at different points in the caring process.
3.1. Temporary Need and Specific Assistance for Poor People
From 2008 onwards, Humancare experienced a dramatic increase in assistance for people needing specific material resources, such as food, clothing, and the timely payment of bills, or information support regarding job training, legal aid for mortgage payments, evictions, etc. New users generally go through a period of socioeconomic vulnerability caused by unemployment, the accumulation of debts, and a temporary lack of economic resources. In these cases, contact with the institution is limited to a specific aid provision that prevents claimants from falling into a more difficult situation of exclusion, but the institution’s casual contacts rarely establish lasting social ties. In most cases, even though their close contacts (family and friends) can barely provide them with enough material resources, they still retain a broad social network.
Laureano’s case provides a good example of this sort of charity client. In 2012, at 62 years old, he was diagnosed with several diseases (fibromyalgia, chronic fatigue, and Crohn’s syndrome). After a brief period of medical leave on top of 25 years working in the IT sector, he was fired. The flexible labor laws enforced by the right-wing government during nearly a decade in power substantially reduced the costs of layoffs. Accordingly, Laureano received a tiny, insufficient pension. As the sole breadwinner in a family also including a wife and two teenage children, the debts began to accumulate. Initially, he asked family members for help. After a while, he felt ashamed and turned to charities instead, which provided him with food and covered some overdue bills.
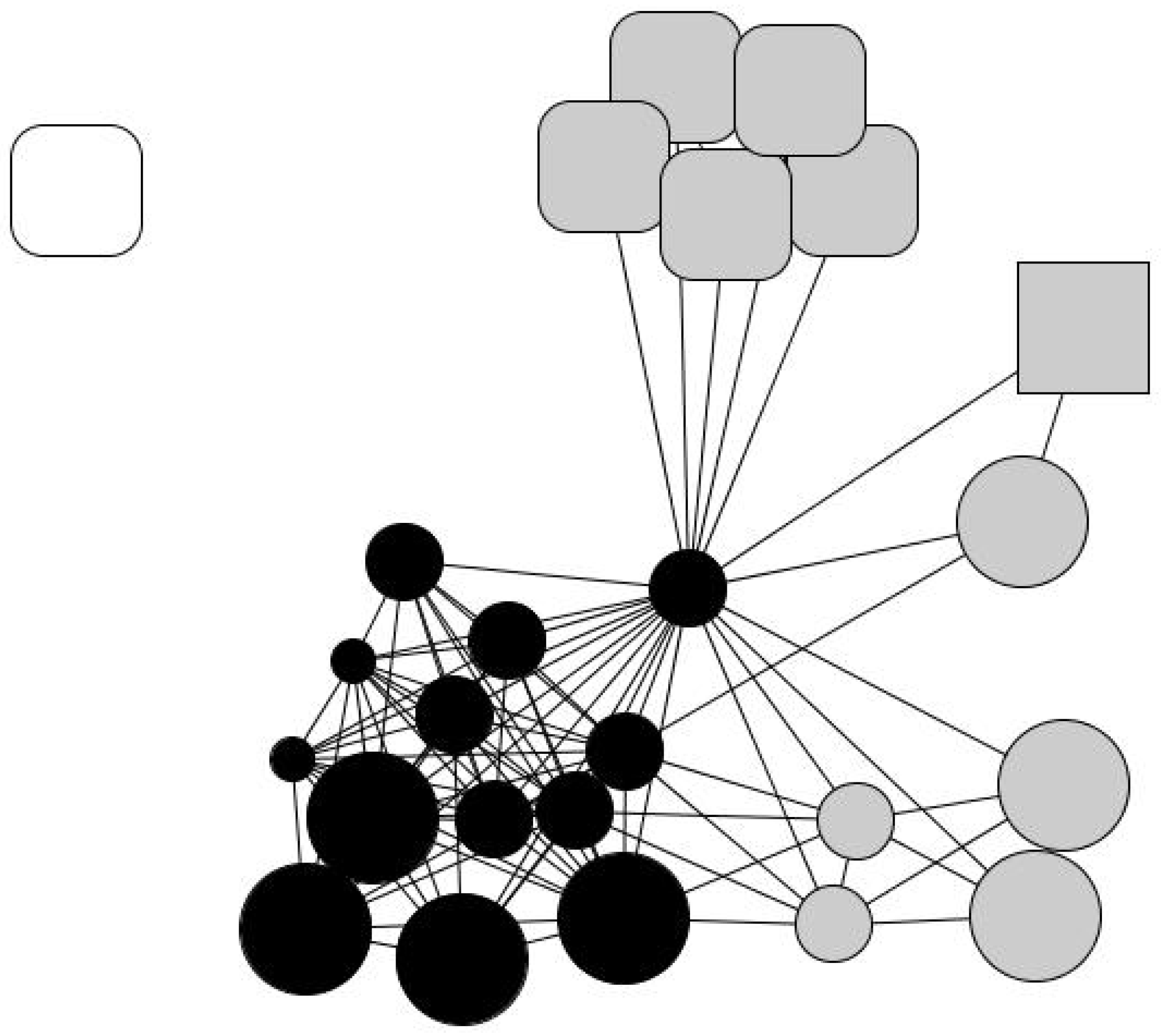
Laureano’s personal network is relatively large, at 25 members: 44% are friends and over 50% are family members. He maintains regular contact with 60% of his old friends and feels “very close” to 88% of his contacts. He believes that 52% of his contacts enjoy a better socioeconomic situation than himself and that the same percentage have had above-average educations. In his network, his wife and children are very central, as they connect different social spheres, namely relatives from both sides of the family and friends from different contexts. His family and close friends may not provide substantial material resources, but they help him with minor services, favors, and gifts, as expressed in the qualitative data. Although he has had to cut down on consumption expenses, he is not living in conditions of severe exclusion. His subsistence and vital necessities, such as medical expenses, his mortgage, and basic material needs, are covered. His personal network has a significant number of strong ties consisting of long-term relationships in different social contexts and with a comfortable socioeconomic status that provides him with socio-emotional support. In other words, his personal network retains some features of the typical Spanish middle-class person. His contact with the charity is depicted in his drawing of his personal network (
Figure 1) with Humancare’s social worker placed in the upper left corner, completely disconnected from any of Laureano’s other contacts.
3.2. Cases of Persons Experiencing MEH
People subject to MEH present several associated problems beyond economic want (
Figure 2). In comparison with Laureano’s case, their personal networks are smaller, and they have little social capital.
Dora, for instance, is a 47-year-old Brazilian transgender person. Some years ago, she arrived in Spain, fleeing the world of prostitution and drugs in her natal favela. In Spain, she married a man who mistreated her, and in running away from him, she ended up on the street without any other social support. She slept in ATM lobbies and collected leftovers from restaurants. Then, she started to “hear voices” inside her head caused by incipient schizophrenia, which prompted her to try and take her own life on several occasions. Once, she swallowed sodium hydroxide, burning her larynx and tongue. She suffered multiple forms of stigma and abuse on the street against her ethnic origin, her gender identity, her economic condition, and her mental distress. On one occasion, someone tried to burn her alive at night, although she managed to get away.
When Dora went to the charity, she was physically impaired, lacking mobility and suffering from atrophy from sleeping on the floor, as well as presenting with memory loss and a lack of communication and social skills alongside severe material needs. She also lost her only suitcase with her phone containing all her contacts.
As in other cases we observed, Dora alternated life on the street with periods in shelters in different cities (staying in shelters is limited to a few weeks). Her nomadism made it challenging to carry out a proper medical diagnosis and follow-up. She was only diagnosed with schizophrenia after the police rescued her from the street after an anonymous call reported her suffering from confusion and hallucinations. Later, she was referred to a psychiatric hospital, where she stayed for several years until she left and ended up at Humancare. Eventually, the charity offered her a single social apartment.
Mutatis mutandis, Dora’s case bears close similarities with those of Kike, Gregor, Inma, and Monroy. They all had small and unstructured social networks and were expelled or had run away from their homes. “(My family) threw me out with my clothes on the street, like shit (…) my children don’t even look at my face”, says Gregor. In these cases, the relationship with family members has deteriorated so much that, as one worker put it: “When we get in touch with their family members, they usually hung up on us or sent us to hell. They don’t want to know anything. At that time that person has no family, he has burned them, there is no turning back, and they must recognize it”.
Nevertheless, although informants’ contacts with their families could be irregular and conflictual, some contact with close friends and family by telephone or via social media platforms such as Facebook was not entirely unusual. Thus, Dora, Inma, and Gregor telephoned their families from time to time. Gregor resumed contact with some of his brothers when their mother fell sick. Monroy called his mother once a week and had engaged in Facebook exchanges with old friends. Inma and Sara stayed in contact with their children, who had been adopted or were in foster homes.
All of them also suffered from severe psychological distress. The frequency of confessed suicide attempts found in the sample is alarming: “My life has no meaning. I’d rather get out of the way”, said Inma, a woman in her forties paired with Gregor. Similar feelings were expressed by Kike, Sara (a woman also in her forties who begged on the street), Monroy and, as already mentioned, Dora.
These informants were all exposed to stigma and structural violence as well. While we were interviewing Monroy on the terrace of a bar, the owner suddenly appeared shouting: “I don’t want this kind of people in my bar!”, and we had to leave. Dora told us that she was not even allowed to look at the women’s clothing through shop windows from the outside because, according to the sellers, she “scared off the clientele”. She missed just “having a coffee on a terrace while chatting with someone”, which is an indication of how isolated she felt. The same situations were reported by Kike, who was often asked to leave public spaces when living on the street, and Eduardo, who, when entering a supermarket, was often followed by shop assistants for fear he would steal alcoholic drinks. According to Sara, homelessness means that “You live in a different world. You are out of society.”
3.3. MEH and Long-Term Attention
The transition from the street to the care institution involves a fragile process. In all cases, individuals showed great distrust when resorting to charity aid, and even after doing so, they showed resistance to being treated, which was probably caused by the addiction and pathologies and by the sustained structural violence they had suffered during their lives. As one social worker observed:
The lives of these people are disjointed, and the soup kitchen is a place where many go, eat, and leave. At the beginning, the objective of the care is rather than rescue the person to undertake work to restore basic patterns and routines.
Severely excluded users usually require prolonged and in-depth social and health care, but in the initial stages, there is a high risk of recidivism (particularly in the case of addictions) because their personal networks become even weaker. On the one hand, they must move away from the harmful situations of the past, while on the other hand, they are encouraged to create new relationships in healthy environments (free from temptations in case of previous addictions).
Gabino, 57 years old, consumed heroin for more than fifteen years, although he tried to hide it until his whole social world collapsed: he was fired, broke with his family and friends, and his partner left him. After some time on the streets, he turned to the Addictive Behaviour Unit, which is a service provided by Humancare. When we interviewed him, he was “clean” (he had overcome his addiction more than a decade ago) and had started a part-time job in a public library. However, he had not managed to mend his social ties: stigma and a fear of rejection prevented him from talking about his life openly, so he avoided close relationships with his new co-workers. His parents had passed away, and the only stable relationships he maintained were with a friend, a social worker, and his younger brother. So, even years later, his network was still minimal and fragile.
Kike’s case has some close similarities with Gabino’s, although he explains his experience as a “success”. Raised in a large working-class family, he started to consume heroin, committing minor crimes to sustain his addiction. Over a decade, he broke with his family, lived on the streets, went to prison several times, was infected by HIV, and made several suicide attempts. By chance, he met an altruistic lawyer committed to prisoners’ reintegration who put him in touch with a small Jesuit congregation that took care of him and directed him toward Humancare. At the charity, he went through rehabilitation and found crucial emotional support. Later, the charity offered him a job as a receptionist, and he started to recover his contacts with family members and made new close contacts with social workers, professionals, and therapists. Kike, today fifty years old, overcame his addiction 25 years ago, but HIV had caused a deterioration in his physical appearance, and he cannot avoid stigma: “Facing society is more difficult than giving up drugs,” he says. He lives with his younger brother, and today, his personal network is broad and integrated, but mainly “institutional”.
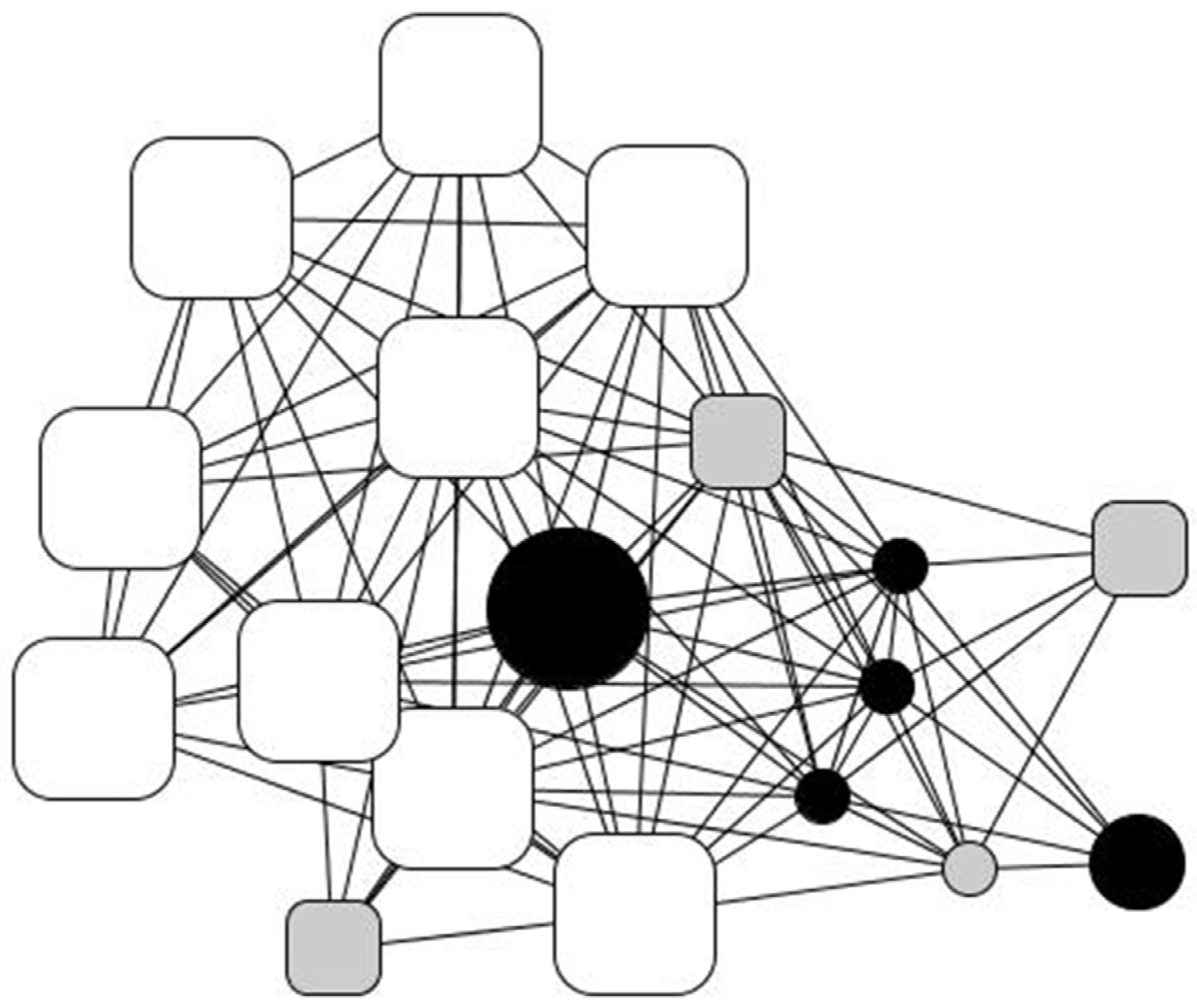
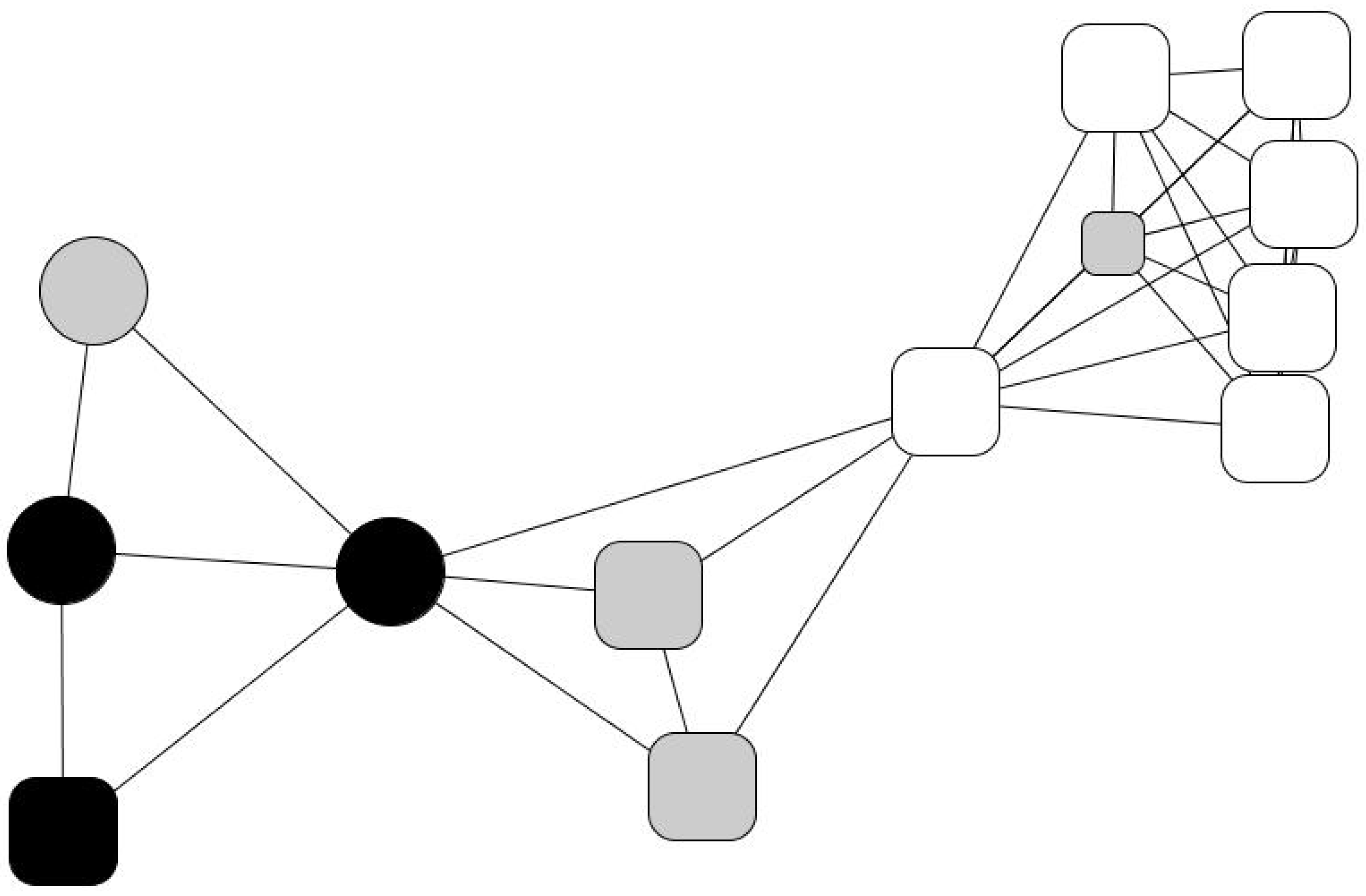
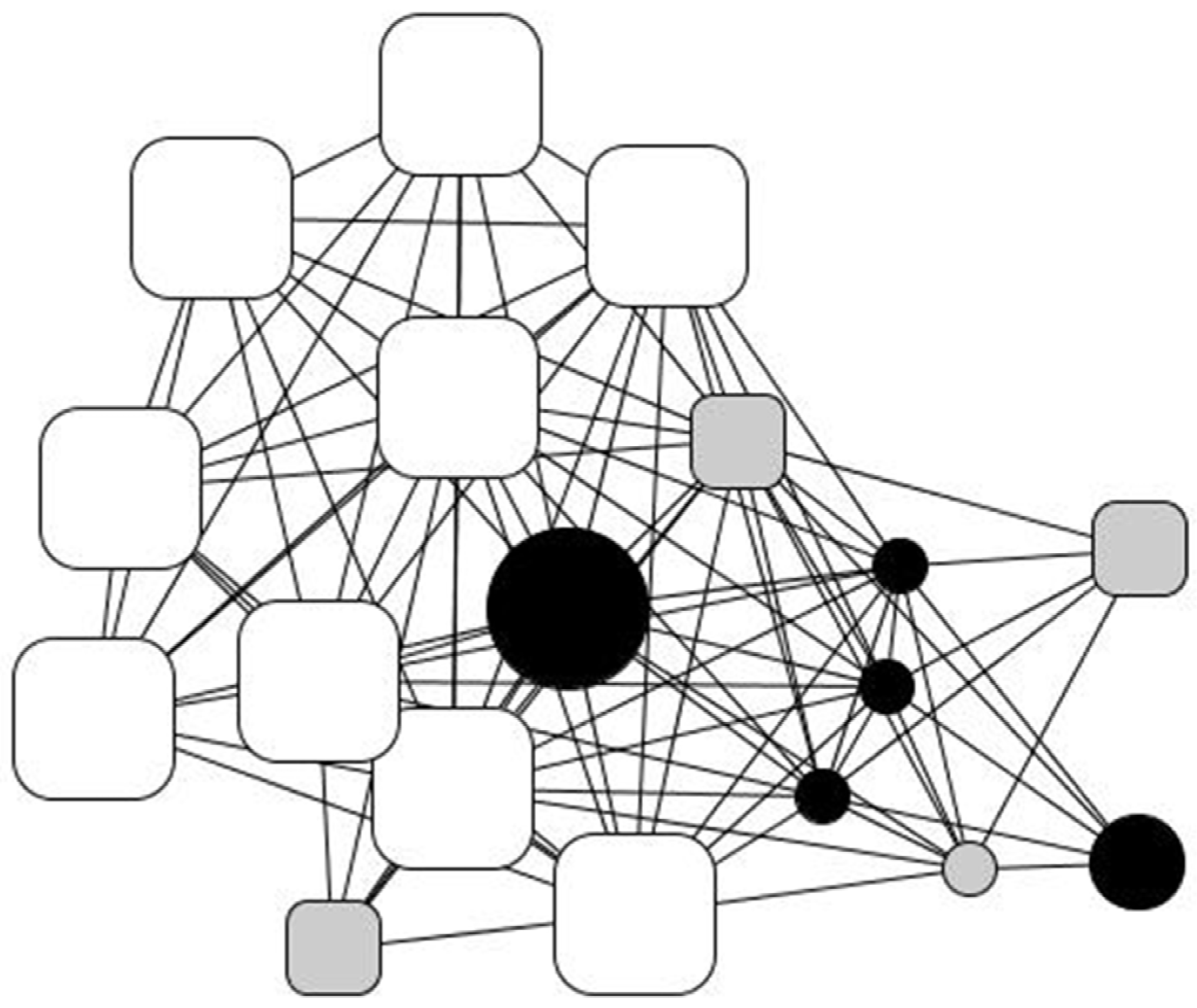
His personal network (
Figure 3) consists of eighteen people to whom he feels “very close”. Roughly half of them are strong ties: family members (22%), with the notable centrality of his older brother, who supports him in several ways, his younger brother, his sister, and his two nieces, who in turn often resort to him, as well as old friends from humble backgrounds (25%). The rest comprise professionals from the social institution that Kike refers to as “my other family”: a cohesive and well-to-do group of people who provide high social and emotional support. Therefore, his network is broad and cohesive, very heterogeneous, and offers Kike chances to reciprocate (e.g., they constantly ask him for small and material help, involvement, advice, support, and company) that, as he puts it, “helped me to recover my self-esteem”.
Julio and Andrés, both in their fifties and long-term Humancare users, share a social apartment in Castelló, where they are starting to reconstitute their lives from the ruptures left by long periods of alcohol addiction. In the past, they exhausted all their financial resources, unsuccessfully stayed in several detoxification centers, and broke off relationships with their relatives and friends: “I’ve lost twenty years of my life, from twenty to forty,” says Julio.
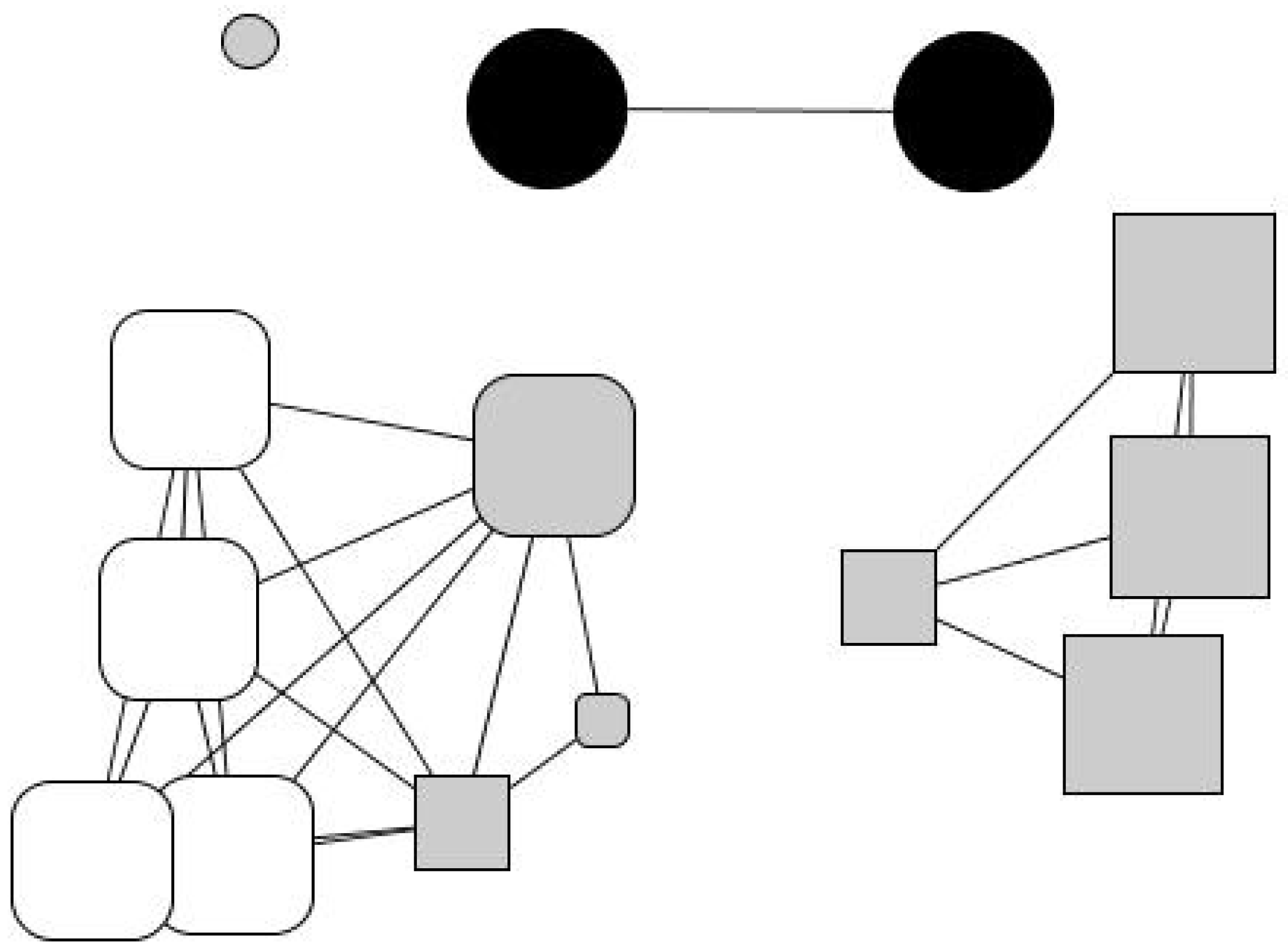
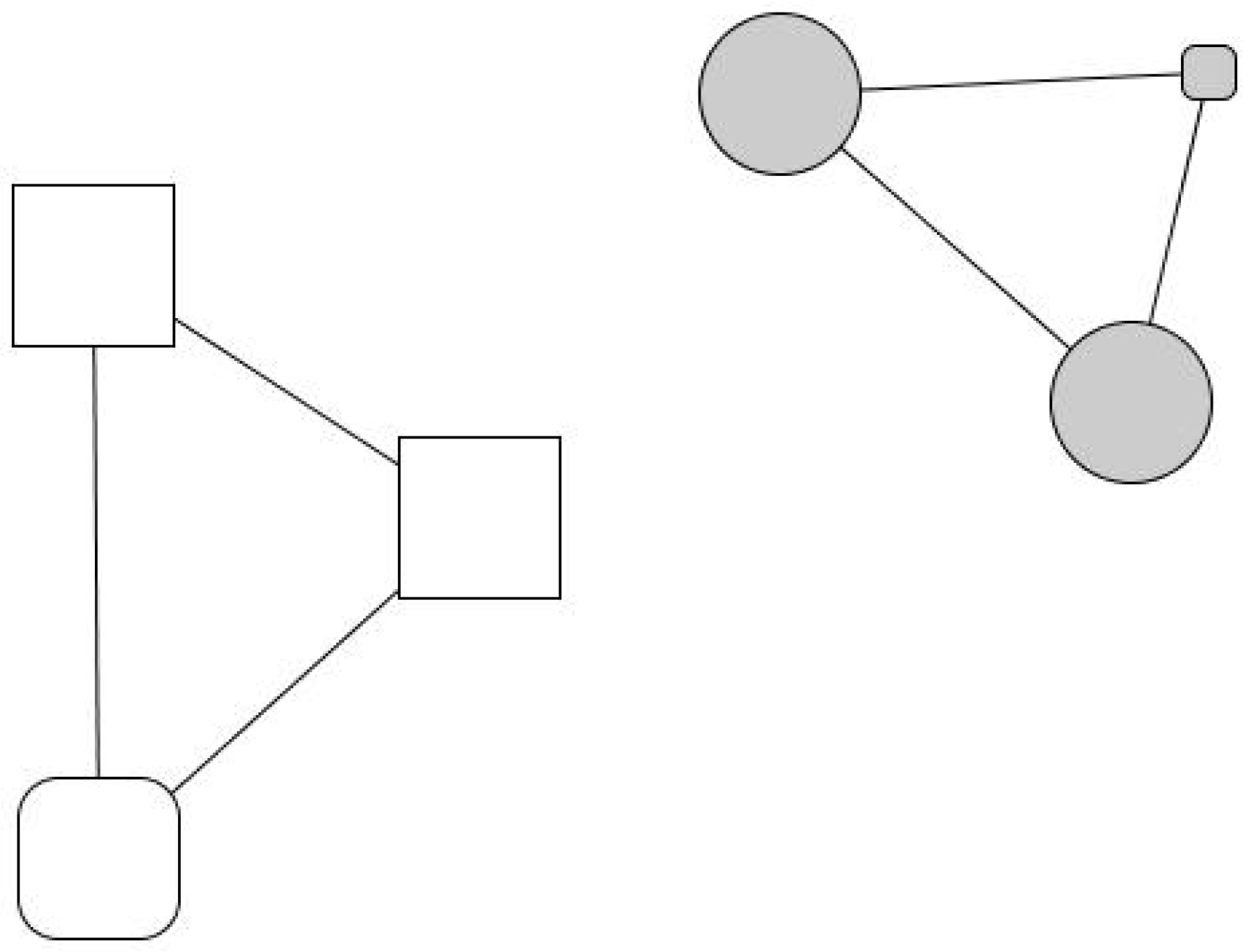
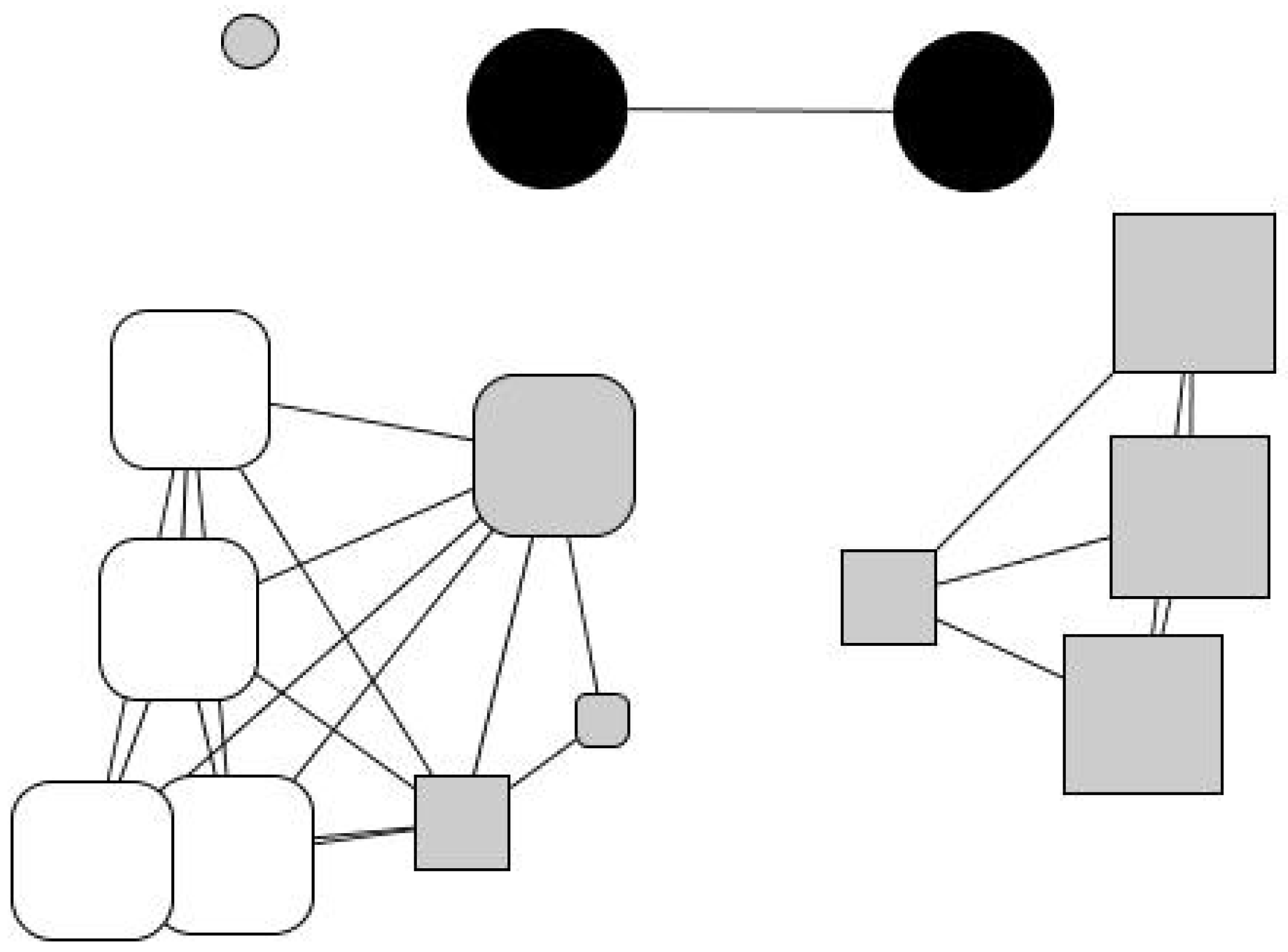
Julio went through a period living on the streets until he accessed a social shelter. He particularly valued the supervision it provided him with, which helped him establish routines and habits, prioritize needs, and have some control over savings. He also appreciated the material aid: the charity paid some of his debts, provided him with a temporary job, and covered his medical treatment. The charity also assigned him a social worker, Mariluz, who established an emotionally intense and dependent relationship with him. As Julio explains, this relationship has acquired a maternal dimension: “I respect Mariluz like a mother. What I like the most is her confidence. We are not friends, we are something else… And I’m going to tell you what we are: a family”. In his personal network (
Figure 4), now considerably wide, fourteen people are distributed into four subgroups: an isolated friend (in the upper-left corner), two distant relatives (his aunt and cousin, upper side), a group of new friends (right-hand margin), and a group of users and professionals from institutional contexts (left-hand side). In his network, 79% of his contacts are recent (last five years), indicating the creation of a new social fabric away from the context of addiction. However, the isolated friend is someone Julio wants to avoid because he considers he is a bad influence, and the new groups of friends are a group of young people who work in a gambling house and share high consumption habits.
Julio perceives 71% of his network members as having a “better socioeconomic situation” than his (the professionals, distant relatives, and new friends), while 14% have a “similar situation” and 14% are socioeconomically worse off. According to Julio, most of his contacts (except for 28% of the institution’s professionals) have received only a little (40%) formal education, if any (28%).
Andrés, Julio’s flatmate, started working as a bartender at an early age. His father’s sudden death triggered a depression, so he began to drink. Things went awry when he lost his job and stopped paying his mortgage until he was evicted. Some old friends persuaded him to visit the Addictive Behavior Unit (UCA). From there, after some months of treatment, he lived for a while in a social shelter until he was transferred to a small shared social house and finally settled in the social apartment he shares with Julio. During these last months, he has gone on training courses and worked in a clothing recycling company depending on the charity. Today, he works in a hospital under an interim contract.
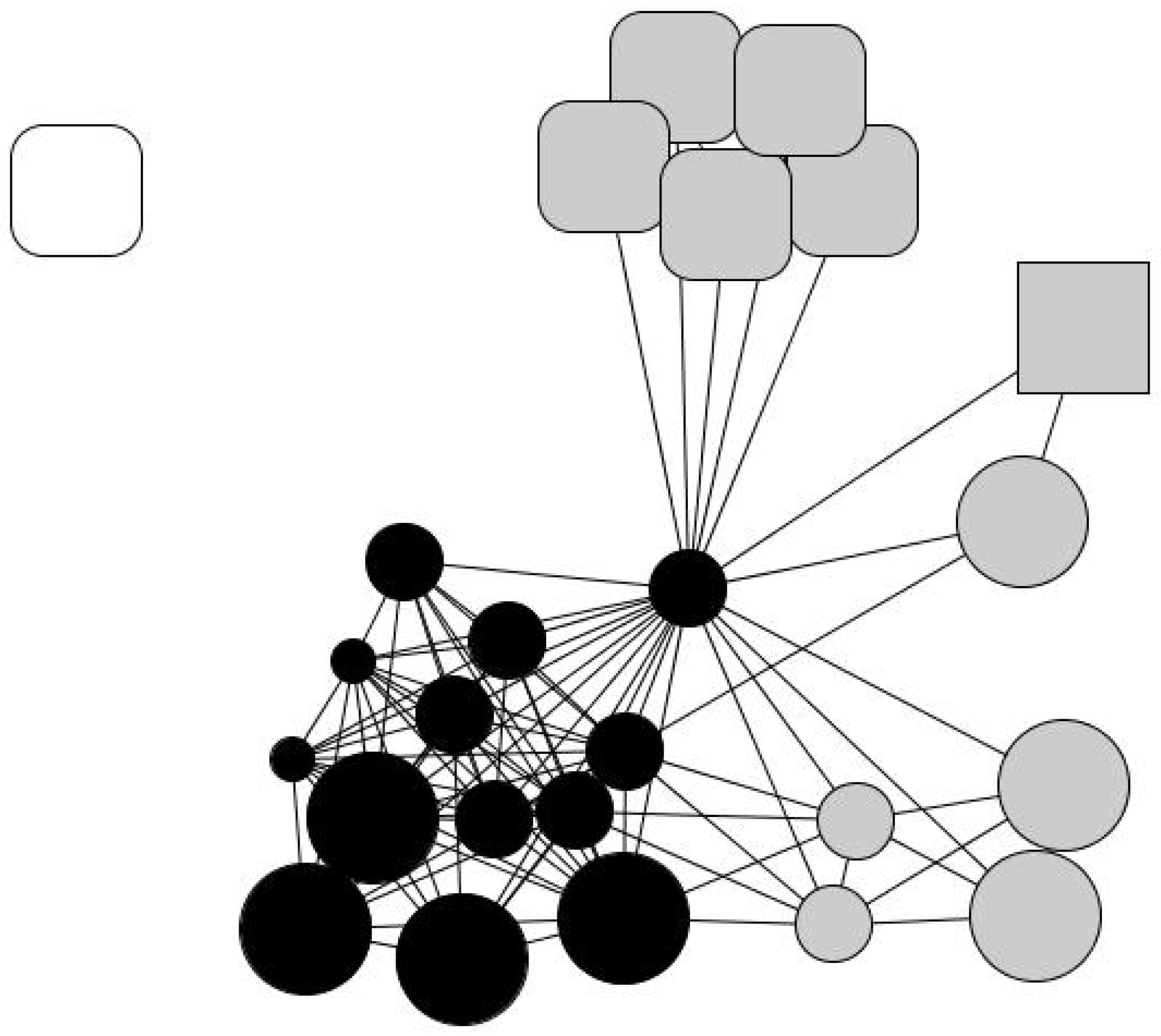
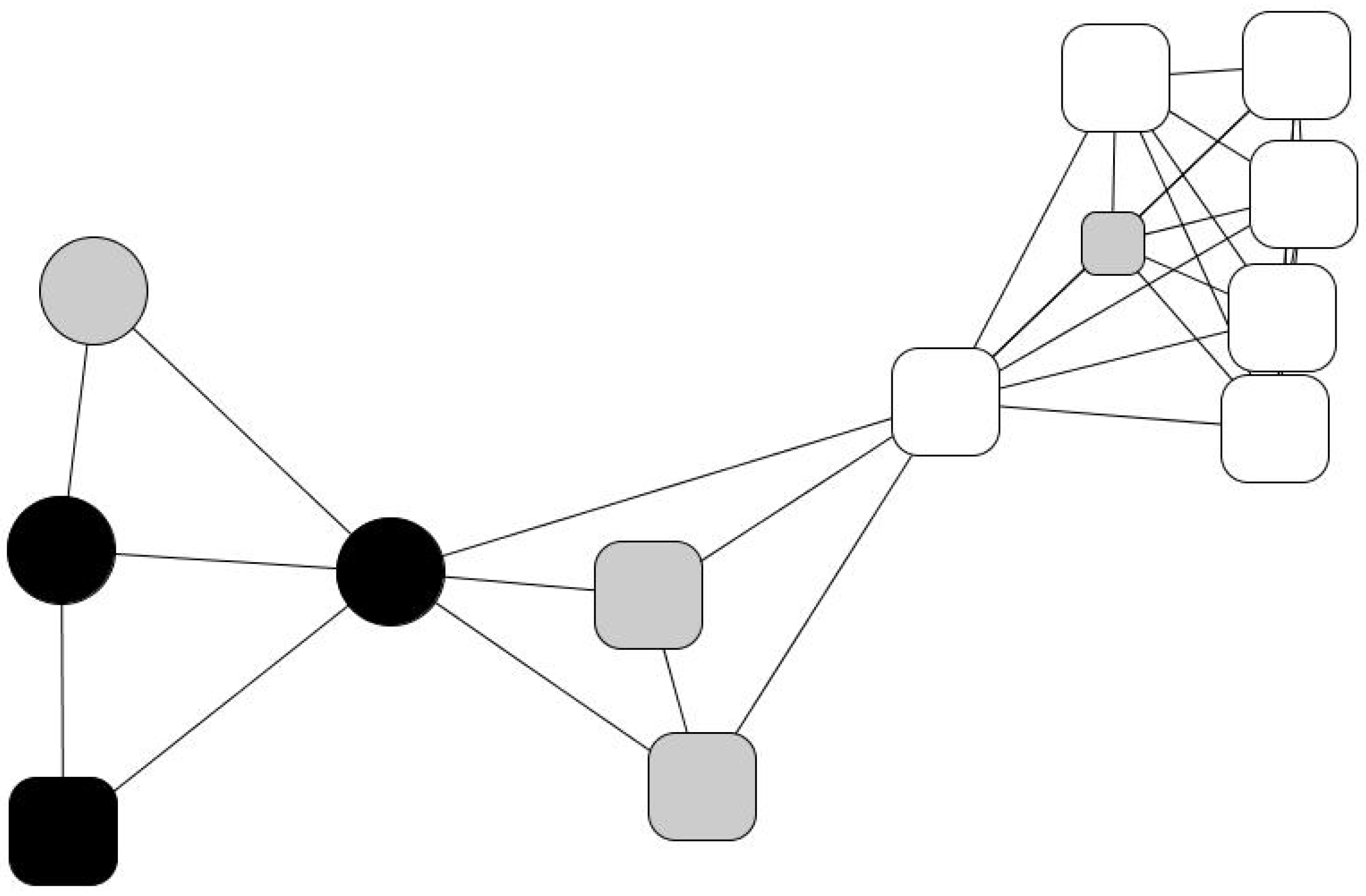
Andrés’ network (
Figure 5), similar to Julio’s, contains a large concentration of professionals (46%). Eulalia, a social worker, with the highest network centrality, mediates between the institution and his personal world (friends, a brother, and a few relatives). Three groups may be identified: one formed by friends (30%), another by social workers (47%), and one-third by relatives (14%). However, he considers he does not have close interactions with anyone apart from 7% of his acquaintances, whom he meets regularly. His network is slightly feminine (61% are women), and he perceives that 92% of his contacts enjoy better socioeconomic situations than him. However, 54% of his contacts (everyone except the professional staff) have barely any formal educational background (30% have no training, 23% have only basic training) nor a comfortable socioeconomic position. Thus, there is an evident socioeconomic divide between his institutional (right-hand side) and personal relationships (left-hand side).
However, social exclusion is not always related to addictions, as the cases of Evaristo and Joaquín show. They both depart from a socially disadvantaged situation, which may partly explain their difficulties in establishing long-term relationships. Alone, after long-term unemployment, they turned to charities.
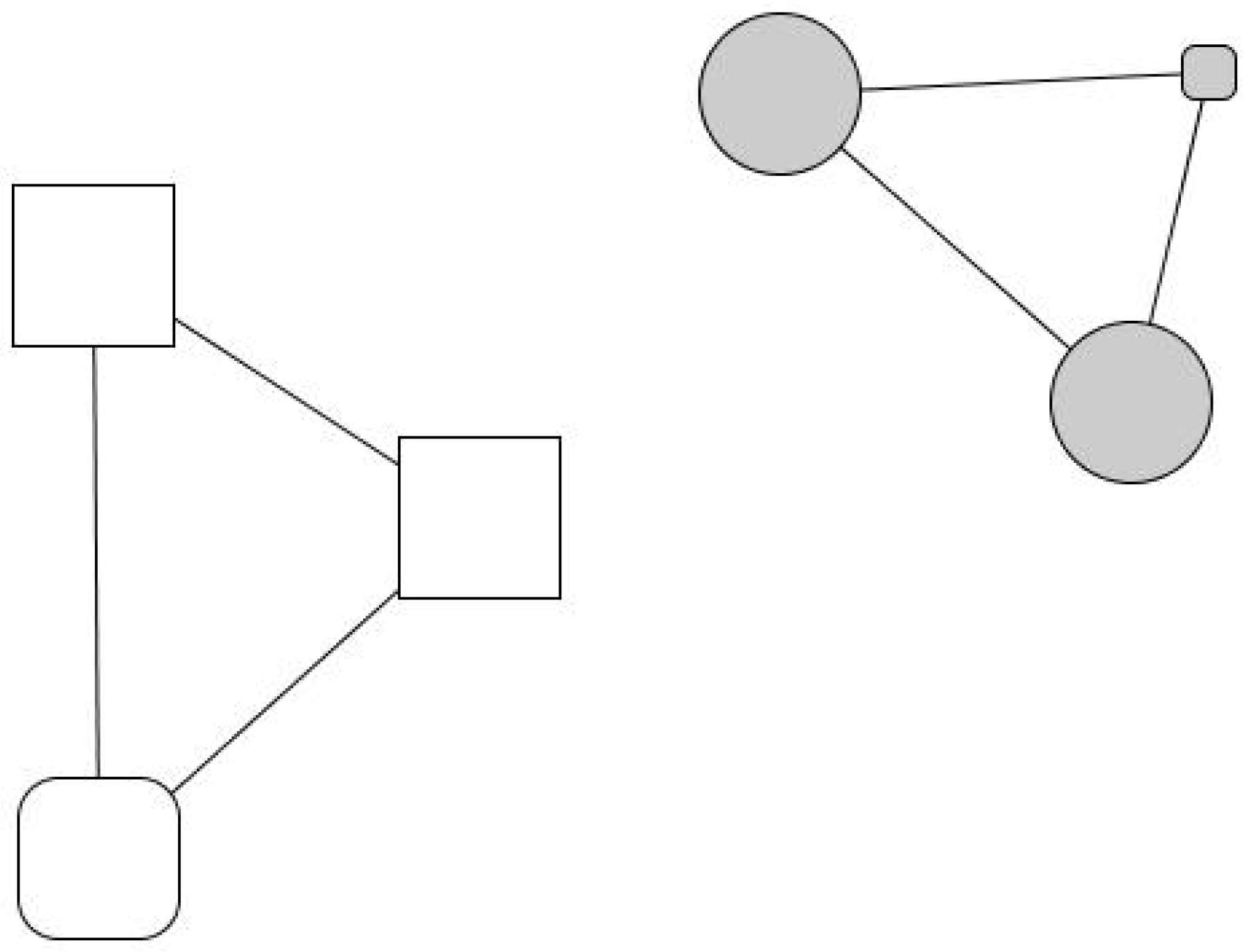
Evaristo, a man in his fifties, had been married three times, had no children, and during his life had worked as a cook in several restaurants. However, he never established lasting labor nor social ties. After his last divorce, aimless, he suffered severe depression, lost his job, and ended up in a social shelter, where he started a relationship with Africa, another charity user whom he was planning to marry and start again from scratch, probably with a small restaurant—i.e., the same story that had been repeated so many times before in his case (see
Figure 6).
Joaquín, a man in his sixties, had been raised in orphanages and, as a teenager, received training as a plasterer and bricklayer. He did not have a happy childhood, frequently being disobedient and suffering bad treatment and punishments. Since leaving the institution, he never managed to establish any stable social relationship. Aged sixty, alone, unemployed, and ill, he resorted to charities. His network has only six active contacts, three women and three men—two recent relationships, the rest being long-term acquaintances with whom he does not feel “very close”. He perceives most of his contacts as having a better socioeconomic situation than himself and, although he thinks these people would help him unconditionally, he recognizes that they “have their own problems”. In his network too, we observe two asymmetric social spheres: one made up of past friends with a similar or worse situation than himself and another made up of professionals, mainly women, with significantly better socioeconomic situations. His minimal personal network reflects an intense relational vulnerability.
3.4. Support Relations among Users, Volunteers, and Professionals
Here, we will summarize some of the interactional recurrences found in our sample. First, there is an evident deficiency of social bonds, both strong ties (family members, close friends, or stable partners) and weak ties (work relationships, neighborhoods, acquaintances). Often, the loss of a loved one, usually a parent, triggers a process of socioemotional decline, as in the cases of Andrés and Kike with their father, Julián with his mother, and Gabino with both parents. When his father died, Andrés explains, “I got into a labyrinth that I didn’t know how to get out of. The only exit was alcohol: you keep drinking and drinking and, in the end, you don’t remember anymore”.
Second, we observe a disproportionate presence of professionals in virtually all networks. These professionals provide care and support and have a crucial role in bridging the relationship between the user and his or her family, showing a commitment that often trespasses on the working day and job position: e.g., they visit their families, answer phone calls at any time, and take their charges to recreational activities such as the theatre. However, the blurring of the boundaries between work and leisure among professionals generates two opposite attitudes, both having reasonable rationales and justifications. On the one hand, some professionals affirm that establishing a strong bond is not a problem, while on the other hand, others believe they must encourage it to promote users’ social inclusion. For instance, one social worker, Roberto, wondered, “Why we don’t we talk and relate with them equally?” Yet others, however, prefer to maintain the boundary as a matter of professionalism. Francisco, the manager of a social shelter, put it this way: “Ethically, I cannot be a friend. It is something I must avoid to maintain an equal position in relation to everyone. Of course, this contradicts the guidelines that we try to give them: empathy, and putting ourselves in their place.” Similarly, Carmen, responsible for the addiction treatment center, said: “Our role is what it is. We have to avoid creating affective bonds that may confuse them”.
Third, gender plays a relevant role in diverse ways. Feminized networks (i.e., networks with a disproportionate number of female contacts) including MEH-affected males are widespread, suggesting a gender bias in the distribution of caregivers (professionals and volunteers) and aid depositaries (users). On the other hand, although severe exclusion often occurs among single adult males with a past of substance abuse and/or mental disorders (nine out of the twelve cases), less frequent female cases also show higher levels of violence and abuse. These findings are congruent with the opinion of mainstream research (see [
20]).
Fourth, we noticed a significant absence: even though a large proportion of Humancare’s tasks rely on volunteering (generally retired women), we have not been able to document the presence of volunteers in any network. Rosa, a 59-year-old volunteer, thinks they should detach themselves emotionally from close interactions with users: “You have to try not to cross [the line]. Otherwise, you take them [the users] home”.
Fifth, although users tend to describe contexts of social care as competitive and insecure spaces where theft, rivalry, or arguments are not uncommon, social and collaborative ties of different types and intensities are also observed. Gregor accompanied another disabled user to solve some administrative problems; Enrique, a disabled homeless man, was cared for by many users at the social shelter; and users used to exchange tobacco, help, and information. Likewise, in long-term care contexts (shelters, social apartments, soup kitchens, etc.), we observed two types of dyadic ties. On the one hand, heterosexual romantic relationships play an essential role and provided mutual support and protection. During the fieldwork, we documented seven cases in our sample, including those of Inma and Gregor, Evaristo and Africa, and Sara and her indigent partner. These couples are often ephemeral because the circumstances are not suitable: they occur in transitional spaces and without privacy. On the other hand, dyadic relations of friendship are also observed, generally between adult males who share care spaces for a sustained period (e.g., Julio and Andrés).
Sixth, outside these protected niches, we find dependency relationships with children or elderly parents that imply high degrees of commitment and responsibility: examples include Inma or Sara and their children, or Gregor and his sick and elderly mother. Conversely, we also find ambivalent toxic links, emotionally loaded, particularly in cases of drug addiction and alcoholism. Julio wanted to get rid of an old friend whom he considered a bad influence. Gregor had a very conflictual relationship with his father, while Inma had one with his mother, and Monroy had one with his entire family. However, even though there was hardly any contact, these relationships were very present in their testimonies.
Finally, despite the traumatic contextual circumstances of the street, most narrate experiences in which they have received help from anonymous people. On one occasion, an old lady gave Eduardo a hot macaroni dish, and another man left him a €50 bill in the cardboard where he slept. Inma and Gregor encountered “good and altruistic people, who offered us alms and conversation (…) especially people with fewer resources: elderly women, teenagers, or poor people from the neighbourhood”. From time to time, Monroy, who is still living on the street, receives free second-hand books from the corner’s bookseller and food from strangers. Kike was supported by a philanthropist lawyer, and Eduardo considered that people, in general, “have treated me very well”.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}