
Health and Wellbeing Benefits from Nature Experiences in Tropical Settings Depend on Strength of Connection to Nature

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
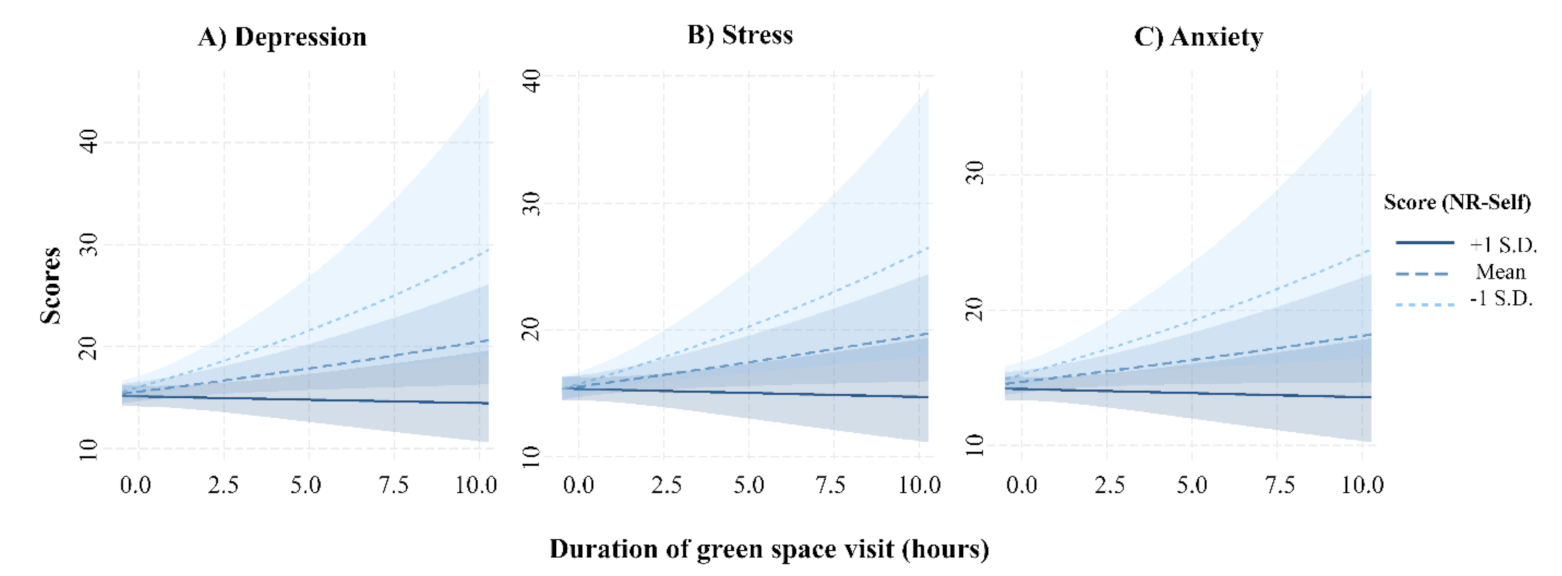
3.1. Mental Wellbeing Outcomes
3.2. Physical Health Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moore, M.; Gould, P.; Keary, B.S. Global Urbanization and Impact on Health. Int. J. Hyg. Environ. Health 2003, 206, 269–278. [Google Scholar] [CrossRef]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.; Wu, J.; Wang, L.; Remais, J.V. Urbanisation and Health in China. Lancet 2012, 379, 843–852. [Google Scholar] [CrossRef]
- World Health Organization; United Nations; Human Settlements Programme. Hidden Cities: Unmasking and Overcoming Health Inequities in Urban Settings; WHO Press: Geneva, Switzerland, 2010; p. 145. [Google Scholar]
- Berry, H.L. “Crowded Suburbs” and “Killer Cities”: A Brief Review of the Relationship between Urban Environments and Mental Health. NSW Public Health Bull. 2007, 18, 222. [Google Scholar] [CrossRef] [PubMed]
- Dye, C. Health and Urban Living. Science 2008, 319, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.B.; Mortensen, P.B. Evidence of a Dose-Response Relationship Between Urbanicity During Upbringing and Schizophrenia Risk. Arch. Gen. Psychiatry 2001, 58, 1039–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krabbendam, L.; van Os, J. Schizophrenia and Urbanicity: A Major Environmental Influence—Conditional on Genetic Risk. Schizophr. Bull. 2005, 31, 795–799. [Google Scholar] [CrossRef]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The Current Status of Urban-Rural Differences in Psychiatric Disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Gruebner, O.A.; Rapp, M.; Adli, M.; Kluge, U.; Galea, S.; Heinz, A. Cities and Mental Health. Dtsch Arztebl Int. 2017, 114, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Costa, D.G.; Peixoto, J.P.J. COVID-19 Pandemic: A Review of Smart Cities Initiatives to Face New Outbreaks. IET Smart Cities 2020, 2, 64–73. [Google Scholar] [CrossRef]
- Galea, S.; Vlahov, D. URBAN HEALTH: Evidence, Challenges, and Directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [Green Version]
- Dean, J.; van Dooren, K.; Weinstein, P. Does Biodiversity Improve Mental Health in Urban Settings? Med. Hypotheses 2011, 76, 877–880. [Google Scholar] [CrossRef]
- Carpenter, M. From ‘Healthful Exercise’ to ‘Nature on Prescription’: The Politics of Urban Green Spaces and Walking for Health. Landsc. Urban. Plan. 2013, 118, 120–127. [Google Scholar] [CrossRef]
- Johnson, M.; Wood, A. Green Prescription Patient Survey 2015 Report; Ministry of Health: Singapore, 2015; p. 195.
- Response for Nature. Response for Nature: England. 2015. Available online: http://ww2.rspb.org.uk/Images/responsefornature_england_tcm9–407740.pdf (accessed on 2 November 2020).
- Nutsford, D.; Pearson, A.L.; Kingham, S. An Ecological Study Investigating the Association between Access to Urban Green Space and Mental Health. Public Health 2013, 127, 1005–1011. [Google Scholar] [CrossRef]
- van den Berg, M.; Wendel-Vos, W.; van Poppel, M.; Kemper, H.; van Mechelen, W.; Maas, J. Health Benefits of Green Spaces in the Living Environment: A Systematic Review of Epidemiological Studies. Urban. For. Urban. Green. 2015, 14, 806–816. [Google Scholar] [CrossRef]
- Bodicoat, D.H.; O’Donovan, G.; Dalton, A.M.; Gray, L.J.; Yates, T.; Edwardson, C.; Hill, S.; Webb, D.R.; Khunti, K.; Davies, M.J.; et al. The Association between Neighbourhood Greenspace and Type 2 Diabetes in a Large Cross-Sectional Study. BMJ Open 2014, 4, e006076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, M.J.; Clarke, N.D.; Birch, S.L.; Tallis, J.; Hankey, J.; Bryant, E.; Eyre, E.L.J. The Effect of Green Exercise on Blood Pressure, Heart Rate and Mood State in Primary School Children. Int. J. Environ. Res. Public Health 2014, 11, 3678–3688. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Thiering, E.; Fuertes, E.; Sugiri, D.; Berdel, D.; Koletzko, S.; von Berg, A.; Bauer, C.-P.; Heinrich, J. A Cross-Sectional Analysis of the Effects of Residential Greenness on Blood Pressure in 10-Year Old Children: Results from the GINIplus and LISAplus Studies. BMC Public Health 2014, 14, 477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Mäkelä, M.J.; et al. Environmental Biodiversity, Human Microbiota, and Allergy Are Interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.J.; Paus, T.; Berman, M.G. Neighborhood Greenspace and Health in a Large Urban Center. Sci. Rep. 2015, 5, 11610. [Google Scholar] [CrossRef] [Green Version]
- Seresinhe, C.I.; Preis, T.; Moat, H.S. Quantifying the Impact of Scenic Environments on Health. Sci. Rep. 2015, 5, 16899. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of Forest Bathing (Shinrin-Yoku) on Levels of Cortisol as a Stress Biomarker: A Systematic Review and Meta-Analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What Is the Best Dose of Nature and Green Exercise for Improving Mental Health? A Multi-Study Analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Dallimer, M.; Irvine, K.N.; Skinner, A.M.J.; Davies, Z.G.; Rouquette, J.R.; Maltby, L.L.; Warren, P.H.; Armsworth, P.R.; Gaston, K.J. Biodiversity and the Feel-Good Factor: Understanding Associations between Self-Reported Human Well-Being and Species Richness. BioScience 2012, 62, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Ojala, A.; Korpela, K.; Tyrväinen, L.; Tiittanen, P.; Lanki, T. Restorative Effects of Urban Green Environments and the Role of Urban-Nature Orientedness and Noise Sensitivity: A Field Experiment. Health Place 2019, 55, 59–70. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of Exposure to Natural Environment on Health Inequalities: An Observational Population Study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 28551. [Google Scholar] [CrossRef] [Green Version]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. Int. J. Environ. Res. Public Health 2017, 14, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renalds, A.; Smith, T.H.; Hale, P.J. A Systematic Review of Built Environment and Health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Bentley, R.; Blakely, T.; Kavanagh, A.; Aitken, Z.; King, T.; McElwee, P.; Giles-Corti, B.; Turrell, G. A Longitudinal Study Examining Changes in Street Connectivity, Land Use, and Density of Dwellings and Walking for Transport in Brisbane, Australia. Environ. Health Perspect 2018, 126, 57003. [Google Scholar] [CrossRef] [PubMed]
- Panter, J.; Mytton, O.; Sharp, S.; Brage, S.; Cummins, S.; Laverty, A.A.; Wijndaele, K.; Ogilvie, D. Using Alternatives to the Car and Risk of All-Cause, Cardiovascular and Cancer Mortality. Heart 2018, 104, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Chandrabose, M.; Owen, N.; Giles-Corti, B.; Turrell, G.; Carver, A.; Sugiyama, T. Urban Densification and 12-Year Changes in Cardiovascular Risk Markers. J. Am. Heart Assoc. 2019, 8. [Google Scholar] [CrossRef]
- Chandrabose, M.; Rachele, J.N.; Gunn, L.; Kavanagh, A.; Owen, N.; Turrell, G.; Giles-Corti, B.; Sugiyama, T. Built Environment and Cardio-Metabolic Health: Systematic Review and Meta-Analysis of Longitudinal Studies. Obes. Rev. 2019, 20, 41–54. [Google Scholar] [CrossRef] [Green Version]
- Glazier, R.H.; Creatore, M.I.; Weyman, J.T.; Fazli, G.; Matheson, F.I.; Gozdyra, P.; Moineddin, R.; Shriqui, V.K.; Booth, G.L. Density, Destinations or Both? A Comparison of Measures of Walkability in Relation to Transportation Behaviors, Obesity and Diabetes in Toronto, Canada. PLoS ONE 2014, 9, e85295. [Google Scholar] [CrossRef] [Green Version]
- Rundle, A.; Roux, A.V.D.; Freeman, L.M.; Miller, D.; Neckerman, K.M.; Weiss, C.C. The Urban Built Environment and Obesity in New York City: A Multilevel Analysis. Am. J. Health Promot 2007, 21, 326–334. [Google Scholar] [CrossRef] [PubMed]
- March, D.; Hatch, S.L.; Morgan, C.; Kirkbride, J.B.; Bresnahan, M.; Fearon, P.; Susser, E. Psychosis and Place. Epidemiol. Rev. 2008, 30, 84–100. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.R.; Passy, P.; Oh, R.R.Y. Impacts of Population Density and Wealth on the Quantity and Structure of Urban Green Space in Tropical Southeast Asia. Landsc. Urban. Plan. 2017, 157, 553–560. [Google Scholar] [CrossRef]
- Fan, P.; Wan, G.; Xu, L.; Park, H.; Xie, Y.; Liu, Y.; Yue, W.; Chen, J. Walkability in Urban Landscapes: A Comparative Study of Four Large Cities in China. Landsc. Ecol. 2018, 33, 323–340. [Google Scholar] [CrossRef]
- Kottek, M.; Grieser, J.; Beck, C.; Rudolf, B.; Rubel, F. World Map of the Köppen-Geiger Climate Classification Updated. Meteorologische Zeitschrift 2006, 15, 259–263. [Google Scholar] [CrossRef]
- Data Europa EU GHS-POP R2015A-GHS Population Grid, Derived from GPW4, Multitemporal (1975, 1990, 2000, 2015)-Data Europa EU 2015. Available online: https://data.europa.eu/data/datasets/jrc-ghsl-ghs_pop_gpw4_globe_r2015a?locale=en (accessed on 17 August 2021).
- Abdul Aziz, N.A.; Konijnendijk van den Bosch, C.; Nilsson, K. Recreational Use of Urban Green Space in Malaysian Cities. Int. J. Bus. Soc. 2018, 19, 1–16. [Google Scholar]
- Priego, C.; Breuste, J.; Rojas, J. Perception and Value of Nature in Urban Landscapes: A Comparative Analysis of Cities in Germany, Chile and Spain. Landsc. Online 2008, 7, 1–22. [Google Scholar] [CrossRef]
- Tam, K.-P. Concepts and Measures Related to Connection to Nature: Similarities and Differences. J. Environ. Psychol. 2013, 34, 64–78. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Fuller, R.A.; Bush, R.; Lin, B.B.; Gaston, K.J. The Health Benefits of Urban Nature: How Much Do We Need? BioScience 2015, 65, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Kuo, M. How Might Contact with Nature Promote Human Health? Promising Mechanisms and a Possible Central Pathway. Front. Psychol. 2015, 6, 1093. [Google Scholar] [CrossRef] [PubMed]
- Government of Singapore Total Land Area of Singapore. Available online: https://data.gov.sg/dataset/total-land-area-of-singapore (accessed on 31 August 2021).
- Singapore Department of Statistics. Population and Population Structure-Latest Data; Singapore Department of Statistics: Singapore, 2019.
- Angel, S. Atlas of Urban Expansion: The 2016 Edition, Volume 1: Areas and Densities; New York University: New York, NY, USA, 2016; Volume 1, p. 500. [Google Scholar]
- Schwarz, N.; Oyserman, D. Asking Questions about Behavior: Cognition, Communication, and Questionnaire Construction. Am. J. Eval. 2001, 22, 127–160. [Google Scholar] [CrossRef] [Green Version]
- Fontana, S.; Sattler, T.; Bontadina, F.; Moretti, M. How to Manage the Urban Green to Improve Bird Diversity and Community Structure. Landsc. Urban. Plan. 2011, 101, 278–285. [Google Scholar] [CrossRef]
- Gao, T.; Hedblom, M.; Emilsson, T.; Nielsen, A.B. The Role of Forest Stand Structure as Biodiversity Indicator. For. Ecol. Manag. 2014, 330, 82–93. [Google Scholar] [CrossRef]
- Threlfall, C.G.; Williams, N.S.G.; Hahs, A.K.; Livesley, S.J. Approaches to Urban Vegetation Management and the Impacts on Urban Bird and Bat Assemblages. Landsc. Urban. Plan. 2016, 153, 28–39. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X. Association of Urban Green Space With Mental Health and General Health Among Adults in Australia. Jama Netw. Open 2019, 2, e198209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban Redevelopment Authority. Singapore Master Plan 2019. Available online: https://www.ura.gov.sg/maps/?service=MP (accessed on 31 March 2021).
- Gaw, L.Y.-F.; Yee, A.T.K.; Richards, D.R. A High-Resolution Map of Singapore’s Terrestrial Ecosystems. Data 2019, 4, 116. [Google Scholar] [CrossRef] [Green Version]
- Chong, K.Y.; Teo, S.; Kurukulasuriya, B.; Chung, Y.F.; Rajathurai, S.; Tan, H.T.W. Not All Green Is as Good: Different Effects of the Natural and Cultivated Components of Urban Vegetation on Bird and Butterfly Diversity. Biol. Conserv. 2014, 171, 299–309. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales—DASS21 Response Form; Psychology Foundation: Sydney, Australia, 1996; pp. 335–343. [Google Scholar]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; de Vries, S.; Spreeuwenberg, P. Green Space, Urbanity, and Health: How Strong Is the Relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood Environments and Socioeconomic Inequalities in Mental Well-Being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at Least 120 Minutes a Week in Nature Is Associated with Good Health and Wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, R.Y.R.; Fielding, K.S.; Nghiem, T.P.L.; Chang, C.-C.; Shanahan, D.F.; Gaston, K.J.; Carrasco, R.L.; Fuller, R.A. Factors Influencing Nature Interactions Vary between Cities and Types of Nature Interactions. People Nat. 2021, 3, 405–417. [Google Scholar] [CrossRef]
- Nisbet, E.K.; Zelenski, J.M.; Murphy, S.A. The Nature Relatedness Scale: Linking Individuals’ Connection With Nature to Environmental Concern and Behavior. Environ. Behav. 2009, 41, 715–740. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Christensen, R.H.B. Cumulative Link Models for Ordinal Regression with the R Package Ordinal. J. Stat. Softw. 2018, 40. submitted. [Google Scholar]
- Christensen, R.H.B. A Tutorial on FItting Cumulative Link Mixed Models with Clmm2 from the Ordinal Package. Available online: https://cran.r-project.org/web/packages/ordinal/vignettes/clmm2_tutorial.pdf (accessed on 7 August 2020).
- John, F.; Sanford, W.; Brad, P. Package ‘Car’ 2021. Available online: https://cran.r-project.org/web/packages/car/car.pdf (accessed on 9 July 2021).
- Ripley, B.; Venables, B.; Bates, D.M.; Hornik, K.; Gebhardt, A.; Firth, D.; Ripley, M.B. Package ‘Mass’; Version 7.3. 2013. Available online: http://www2.uaem.mx/r-mirror/web/packages/MASS/ (accessed on 12 October 2020).
- Singapore Strategy. Group Population In Brief; 2018. Available online: https://www.strategygroup.gov.sg/media–centre/publications/population–in–brief (accessed on 31 March 2021).
- Ratcliffe, E. Toward a Better Understanding of Pleasant Sounds and Soundscapes in Urban Settings. Cities Health 2021, 5, 82–85. [Google Scholar] [CrossRef]
- Soga, M.; Gaston, K.J. The Ecology of Human–Nature Interactions. Proc. R. Soc. B Biol. Sci. 2020, 287, 20191882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, L.S.; Shanahan, D.F.; Fuller, R.A. A Review of the Benefits of Nature Experiences: More Than Meets the Eye. Int. J. Environ. Res. Public Health 2017, 14, 864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Green Space Is Associated with Walking and Moderate-to-Vigorous Physical Activity (MVPA) in Middle-to-Older-Aged Adults: Findings from 203 883 Australians in the 45 and Up Study. Br. J. Sports Med. 2014, 48, 404–406. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Urban. Green Spaces and Health: A Review of Evidence; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The Mental and Physical Health Outcomes of Green Exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social Contacts as a Possible Mechanism behind the Relation between Green Space and Health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Ward-Smith, C.; Naidoo, T.; Olvitt, L.; Akhurst, J. Perceived Benefits of Nature-Based Experiences as Mediators of Connectedness with Nature: The Case of Mystic Mountain. South. Afr. J. Psychol. 2020, 50, 553–564. [Google Scholar] [CrossRef]
- Bowler, D. The Importance of Nature for Health: Is There a Specific Benefit of Contact with Green Space? Syst. Rev. Collab. Environ. Evid. 2010, 40, 1–57. [Google Scholar]
- Martyn, P.; Brymer, E. The Relationship between Nature Relatedness and Anxiety. J. Health Psychol. 2016, 21, 1436–1445. [Google Scholar] [CrossRef]
- Capaldi, C.A.; Dopko, R.L.; Zelenski, J.M. The Relationship between Nature Connectedness and Happiness: A Meta-Analysis. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelenski, J.M.; Nisbet, E.K. Happiness and Feeling Connected: The Distinct Role of Nature Relatedness. Environ. Behav. 2014, 46, 3–23. [Google Scholar] [CrossRef] [Green Version]
- Mayer, F.S.; Frantz, C.M.; Bruehlman-Senecal, E.; Dolliver, K. Why Is Nature Beneficial?: The Role of Connectedness to Nature. Environ. Behav. 2009, 41, 607–643. [Google Scholar] [CrossRef]
- Bang, M.; Medin, D.L.; Atran, S. Cultural Mosaics and Mental Models of Nature. Proc. Natl. Acad. Sci. USA 2007, 104, 13868–13874. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.L.; Phoenix, C.; Lovell, R.; Wheeler, B.W. Green Space, Health and Wellbeing: Making Space for Individual Agency. Health Place 2014, 30, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Beatley, T. Singapore: How to Grow a High-Rise City in a Garden. SiteLINES J. Place 2012, 8, 14–17. [Google Scholar]
- Tan, P.Y.; Wang, J.; Sia, A. Perspectives on Five Decades of the Urban Greening of Singapore. Cities 2013, 32, 24–32. [Google Scholar] [CrossRef]
- Lawton, E.; Brymer, E.; Clough, P.; Denovan, A. The Relationship between the Physical Activity Environment, Nature Relatedness, Anxiety, and the Psychological Well-Being Benefits of Regular Exercisers. Front. Psychol. 2017, 8, 1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bixler, R.D.; Floyd, M.F. Nature Is Scary, Disgusting, and Uncomfortable. Environ. Behav. 1997, 29, 443–467. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Sinha, R. The Effects of Stress on Physical Activity and Exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef] [PubMed]
- Difrancesco, S.; Lamers, F.; Riese, H.; Merikangas, K.R.; Beekman, A.T.F.; van Hemert, A.M.; Schoevers, R.A.; Penninx, B.W.J.H. Sleep, Circadian Rhythm, and Physical Activity Patterns in Depressive and Anxiety Disorders: A 2-Week Ambulatory Assessment Study. Depress. Anxiety 2019, 36, 975–986. [Google Scholar] [CrossRef] [Green Version]
- de Vries, S.; van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape Greenery and Health: Stress, Social Cohesion and Physical Activity as Mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Wolf, L.J.; Ermgassen, S.Z.; Balmford, A.; White, M.; Weinstein, N. Is Variety the Spice of Life? An Experimental Investigation into the Effects of Species Richness on Self-Reported Mental Well-Being. PLoS ONE 2017, 12, e0170225. [Google Scholar] [CrossRef] [Green Version]
- Marselle, M.R.; Martens, D.; Dallimer, M.; Irvine, K.N. Review of the Mental Health and Well-being Benefits of Biodiversity. In Biodiversity and Health in the Face of Climate Change; Marselle, M.R., Stadler, J., Korn, H., Irvine, K.N., Bonn, A., Eds.; Springer International Publishing: Cham, Germany, 2019; pp. 175–211. ISBN 978-3-030-02318-8. [Google Scholar]
- Fuller, R.A.; Irvine, K.N.; Devine-Wright, P.; Warren, P.H.; Gaston, K.J. Psychological Benefits of Greenspace Increase with Biodiversity. Biol. Lett. 2007, 3, 390–394. [Google Scholar] [CrossRef]
- Luck, G.W.; Davidson, P.; Boxall, D.; Smallbone, L. Relations between Urban Bird and Plant Communities and Human Well-Being and Connection to Nature. Conserv. Biol. 2011, 25, 816–826. [Google Scholar] [CrossRef]
- Nghiem, L.T.P.; Zhang, Y.; Oh, R.R.Y.; Chang, C.; Tan, C.L.Y.; Shannahan, D.F.; Lin, B.B.; Gaston, K.J.; Fuller, R.A.; Carrasco, L.R. Equity in Green and Blue Spaces Availability in Singapore. Landsc. Urban. Plan. 2021, 210, 104083. [Google Scholar] [CrossRef]
- Ode, Å.; Hagerhall, C.M.; Sang, N. Analysing Visual Landscape Complexity: Theory and Application. Landsc. Res. 2010, 35, 111–131. [Google Scholar] [CrossRef]
- de Vries, S.; Snep, R. Biodiversity in the Context of ‘Biodiversity–Mental Health’ Research. In Biodiversity and Health in the Face of Climate Change; Marselle, M.R., Stadler, J., Korn, H., Irvine, K.N., Bonn, A., Eds.; Springer International Publishing: Cham, Germany, 2019; pp. 159–173. ISBN 978-3-030-02318-8. [Google Scholar]
- Austen, G.E.; Dallimer, M.; Irvine, K.N.; Maund, P.R.; Fish, R.D.; Davies, Z.G. Exploring Shared Public Perspectives on Biodiversity Attributes. People Nat. 2021, 3, 901–913. [Google Scholar] [CrossRef]
- Doherty, S.T.; Lemieux, C.J.; Canally, C. Tracking Human Activity and Well-Being in Natural Environments Using Wearable Sensors and Experience Sampling. Soc. Sci. Med. 2014, 106, 83–92. [Google Scholar] [CrossRef]
- Cooper, A.R.; Page, A.S.; Wheeler, B.W.; Hillsdon, M.; Griew, P.; Jago, R. Patterns of GPS Measured Time Outdoors after School and Objective Physical Activity in English Children: The PEACH Project. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening Is Beneficial for Health: A Meta-Analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef]
- Hu, F.B. Globalization of Diabetes: The Role of Diet, Lifestyle, and Genes. Diabetes Care 2011, 34, 1249–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B.; Solomon, C.G. Diet, Lifestyle, and the Risk of Type 2 Diabetes Mellitus in Women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colagiuri, S.; Vita, P.; Cardona-Morrell, M.; Singh, M.F.; Farrell, L.; Milat, A.; Haas, M.; Bauman, A. The Sydney Diabetes Prevention Program: A Community-Based Translational Study. BMC Public Health 2010, 10, 328. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing Walking. Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Mental Health Benefits of Neighbourhood Green Space Are Stronger among Physically Active Adults in Middle-to-Older Age: Evidence from 260,061 Australians. Prev. Med. 2013, 57, 601–606. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Greener Neighborhoods, Slimmer People? Evidence from 246 920 Australians. Int. J. Obes 2014, 38, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Is Neighborhood Green Space Associated With a Lower Risk of Type 2 Diabetes? Evidence From 267,072 Australians. Diabetes Care 2014, 37, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.S.; Teede, H.; Aroni, R. Spicing up Your Advice for South Asian and Anglo-Australians with Type 2 Diabetes and CVD: Do Cultural Constructions of Diet Matter? Appetite 2018, 120, 679–697. [Google Scholar] [CrossRef]
- Brown, C.D.; Higgins, M.; Donato, K.A.; Rohde, F.C.; Garrison, R.; Obarzanek, E.; Ernst, N.D.; Horan, M. Body Mass Index and the Prevalence of Hypertension and Dyslipidemia. Obes. Res. 2000, 8, 605–619. [Google Scholar] [CrossRef] [Green Version]
- Drøyvold, W.B.; Midthjell, K.; Nilsen, T.I.L.; Holmen, J. Change in Body Mass Index and Its Impact on Blood Pressure: A Prospective Population Study. Int. J. Obes 2005, 29, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Flores-Huerta, S.; Klünder-Klünder, M.; Reyes de la Cruz, L.; Santos, J.I. Increase in Body Mass Index and Waist Circumference Is Associated with High Blood Pressure in Children and Adolescents in Mexico City. Arch. Med. Res. 2009, 40, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Tebar, W.R.; Ritti-Dias, R.M.; Farah, B.Q.; Zanuto, E.F.; Vanderlei, L.C.M.; Christofaro, D.G.D. High Blood Pressure and Its Relationship to Adiposity in a School-Aged Population: Body Mass Index vs Waist Circumference. Hypertens Res. 2018, 41, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Tsunetsugu, Y.; Lee, J.; Park, B.-J.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and Psychological Effects of Viewing Urban Forest Landscapes Assessed by Multiple Measurements. Landsc. Urban. Plan. 2013, 113, 90–93. [Google Scholar] [CrossRef]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.-J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of Forest Therapy on Cardiovascular Relaxation in Young Adults. Evid. Based Complementary Altern. Med. 2014, 2014, e834360. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Igarashi, M.; Miwa, M.; Takagaki, M.; Miyazaki, Y. Physiological and Psychological Responses of Young Males during Spring-Time Walks in Urban Parks. J. Physiol. Anthropol. 2014, 33, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global Estimates of Undiagnosed Diabetes in Adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Tatiana, N.; Sug (Sarah) Yoon, S.; Vicki, B.; Qiuping, G. Hypertension Among Adults in the United States: National Health and Nutrition Examination Survey, 2011–2012; U.S. Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Health Statistics: Hyattsville, MA, USA, 2013.

{kind=link}
| Variable | Description |
|---|---|
| Age (linear) | Respondents provided their age in years. |
| Personal income (linear) | Respondents selected from 16 income brackets *. For analysis purposes, the mid- point of each income bracket was used and treated as a continuous variable. |
| Gender (categorical) | Female or male. |
| Ethnic group (categorical) | Respondents selected from: Chinese, Malay, Indian, Eurasian, Others. For analysis purposes, these were later aggregated to two categories: ethnic majority (Chinese) and minorities (Malay, Indian, Eurasian, Others). |
| Education (categorical) | Respondents indicated their highest formal education by selecting from 10 catego- ries *. For analysis purposes, these were later aggregated into two categories: No bachelor’s degree and bachelor’s degree and higher. |
| Number of workdays per week (linear) | The number of days the respondent works in an average week. |
| Physical activity (linear) | Number of days in the last week where the respondent engaged in vigorous physi- cal activity. |
| Body mass index (linear) | Respondent’s body mass index (BMI), calculated as: weight in kilograms divided by height in metres squared. |
| Social cohesion (linear) | A measure of a respondent’s perceptions of social cohesion as derived from three questions *, with higher scores representing stronger social cohesion. |
| Ability (or inability) to access green space be- cause of poor health (binary) | Respondents indicated the extent to which poor health prevents them from spend- ing time in outdoor green spaces. Respondents selected from: never; sometimes; of- ten; most of the time. For analysis purposes, these were later aggregated into two categories: unable to access green space because of poor health (responses of “of- ten” and “most of the time”) and able to access green space because of poor health (responses of “never” and “sometimes”). |
| NR-Self (linear) | A measure of a respondent’s ecological identity as derived from the nature related- ness affective sub-scale *, with higher scores representing stronger NR-Self. |
| NR-Experience (linear) | A measure of a respondent’s familiarity with nature as derived from the nature re- latedness experiential sub-scale *, with higher scores representing stronger NR-Ex- perience. |
| Frequency of green space visits (linear) | Self-reported number of visits to public outdoor green spaces in the past year. |
| Duration of green space visits (linear) | Self-reported average number of hour(s) spent during each visit to public outdoor green spaces in the week prior to completing the survey. |
| Nature intensity (linear) | Area of tree canopy within the most vegetated outdoor green space visited by each respondent, and the proportion of that which is human-managed. |
| Predictor Variables | Depression | Stress | Anxiety |
|---|---|---|---|
| Cond. H = 2.6 × 103 | Cond. H = 2.3 × 103 | Cond. H = 8.6 × 101 | |
| Age | −0.45 (0.05) | −0.28 (0.04) | −0.30 (0.03) |
| Personal Income | −0.08 (0.06) | −0.09 (0.05) | −0.04 (0.04) |
| Education (bachelor’s degree) | −0.06 (0.10) | 0.03 (0.08) | −0.07 (0.07) |
| Gender (female) | −0.08 (0.10) | 0.11 (0.08) | 0.04 (0.06) |
| Ethnicity (minorities) | −0.24 (0.11) | −0.20 (0.09) | −0.15 (0.08) |
| Number of work days | −0.01 (0.05) | 0.04 (0.04) | −0.01 (0.03) |
| Body Mass Index | −0.01 (0.05) | −0.03 (0.04) | 0.01 (0.03) |
| Physical activity | 0.03 (0.05) | 0.08 (0.04) | 0.07 (0.03) |
| Duration of green space visit | 1.17 (0.44) | 0.90 (0.35) | 0.06 (0.04) |
| Frequency of green space visits | −0.32 (0.43) | −0.15 (0.34) | −0.10 (0.04) |
| Average tree cover | −0.02 (0.05) | −0.01 (0.04) | −0.01 (0.03) |
| Proportion of tree cover that is managed | 0.03 (0.11) | 0.09 (0.09) | −0.02 (0.08) |
| NR_Self | −0.21 (0.10) | −0.07 (0.08) | −0.08 (0.04) |
| NR_Experience | −0.08 (0.06) | −0.07 (0.05) | −0.06 (0.04) |
| Social Cohesion | −0.18 (0.05) | −0.07 (0.04) | 0.01 (0.03) |
| Ability to access green space | −0.69 (0.13) | −0.61 (0.11) | −0.56 (0.09) |
| Duration of green space visits * NR_Self | −0.30 (0.12) | −0.23 (0.10) | −0.10 (0.04) |
| Frequency of green space visits * NR_Self | 0.06 (0.12) | 0.01 (0.10) | 0.02 (0.05) |
| Duration of green space visits * NR_ Experience | 0.08 (0.07) | 0.06 (0.06) | 0.08 (0.05) |
| Frequency of green space visits * NR_ Experience | 0.04 (0.06) | 0.06 (0.05) | −0.01 (0.04) |
| Predictor Variables | High Blood Pressure | Diabetes |
|---|---|---|
| Pseudo R2 = 0.35 | Pseudo R2 = 0.21 | |
| Age | 1.35 (0.13) | 0.91 (0.16) |
| Personal Income | 0.17 (0.12) | −0.06 (0.18) |
| Education (bachelor’s degree) | −0.35 (0.22) | −0.59 (0.33) |
| Gender (female) | −0.19 (0.21) | −0.54 (0.30) |
| Ethnicity (minorities) | −0.53 (0.28) | −0.24 (0.38) |
| Number of work days | 0.01 (0.11) | −0.11 (0.14) |
| Body Mass Index | 0.77 (0.10) | 0.49 (0.13) |
| Physical activity | 0.10 (0.10) | −0.37 (0.19) |
| Duration of green space visit | −0.03 (0.10) | −0.07 (0.18) |
| Frequency of green space visits | 0.02 (0.11) | −0.22 (0.22) |
| Average tree cover | 0.05 (0.10) | 0.15 (0.13) |
| Proportion of tree cover that is managed | −0.27 (0.25) | −0.17 (0.35) |
| NR_Self | −0.21 (0.13) | −0.12 (0.18) |
| NR_Experience | 0.09 (0.13) | 0.02 (0.19) |
| Social Cohesion | 0.13 (0.11) | 0.36 (0.17) |
| Ability to access green space | −0.80 (0.26) | −0.32 (0.37) |
| Duration of green space visits * NR_Self | 0.06 (0.15) | 0.14 (0.21) |
| Frequency of green space visits * NR_Self | −0.06 (0.13) | 0.04 (0.24) |
| Duration of green space visits * NR_Experience | −0.01 (0.16) | −0.16 (0.25) |
| Frequency of green space visits * NR_Experience | −0.04 (0.13) | 0.05 (0.23) |
| Predictor Variables | Estimated Coefficient (Standard Error) |
|---|---|
| Pseudo R2 = 0.01 | |
| Age | 0.20 (0.08) |
| Personal Income | 0.01 (0.09) |
| Education (Bachelor’s degree) | −0.04 (0.17) |
| Gender (Female) | −0.04 (0.15) |
| Ethnicity (Minorities) | −0.26 (0.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, R.R.Y.; Fielding, K.S.; Chang, C.-C.; Nghiem, L.T.P.; Tan, C.L.Y.; Quazi, S.A.; Shanahan, D.F.; Gaston, K.J.; Carrasco, R.L.; Fuller, R.A. Health and Wellbeing Benefits from Nature Experiences in Tropical Settings Depend on Strength of Connection to Nature. Int. J. Environ. Res. Public Health 2021, 18, 10149. https://doi.org/10.3390/ijerph181910149
Oh RRY, Fielding KS, Chang C-C, Nghiem LTP, Tan CLY, Quazi SA, Shanahan DF, Gaston KJ, Carrasco RL, Fuller RA. Health and Wellbeing Benefits from Nature Experiences in Tropical Settings Depend on Strength of Connection to Nature. International Journal of Environmental Research and Public Health. 2021; 18(19):10149. https://doi.org/10.3390/ijerph181910149
Chicago/Turabian StyleOh, Rachel R. Y., Kelly S. Fielding, Chia-Chen Chang, Le T. P. Nghiem, Claudia L. Y. Tan, Shimona A. Quazi, Danielle F. Shanahan, Kevin J. Gaston, Roman L. Carrasco, and Richard A. Fuller. 2021. "Health and Wellbeing Benefits from Nature Experiences in Tropical Settings Depend on Strength of Connection to Nature" International Journal of Environmental Research and Public Health 18, no. 19: 10149. https://doi.org/10.3390/ijerph181910149
APA StyleOh, R. R. Y., Fielding, K. S., Chang, C.-C., Nghiem, L. T. P., Tan, C. L. Y., Quazi, S. A., Shanahan, D. F., Gaston, K. J., Carrasco, R. L., & Fuller, R. A. (2021). Health and Wellbeing Benefits from Nature Experiences in Tropical Settings Depend on Strength of Connection to Nature. International Journal of Environmental Research and Public Health, 18(19), 10149. https://doi.org/10.3390/ijerph181910149