
The Expert Caregiver Intervention Targeting Former Caregivers in Finland: A Co-Design and Feasibility Study Using Mixed Methods



Abstract
:1. Introduction
- To co-design and implement the Finnish Expert Caregiver intervention with special attention to the impact of the COVID-19 pandemic;
- To assess demand in terms of actual use and perceived demand;
- To assess practicality in terms of the participants’ ability to carry out volunteering activities and the effects on the participants.
2. Materials and Methods
2.1. Research Design
2.2. Setting of the Intervention
2.3. Intervention
2.4. Study Population
2.5. Measures
2.6. Analysis
2.7. Ethical Considerations
3. Results
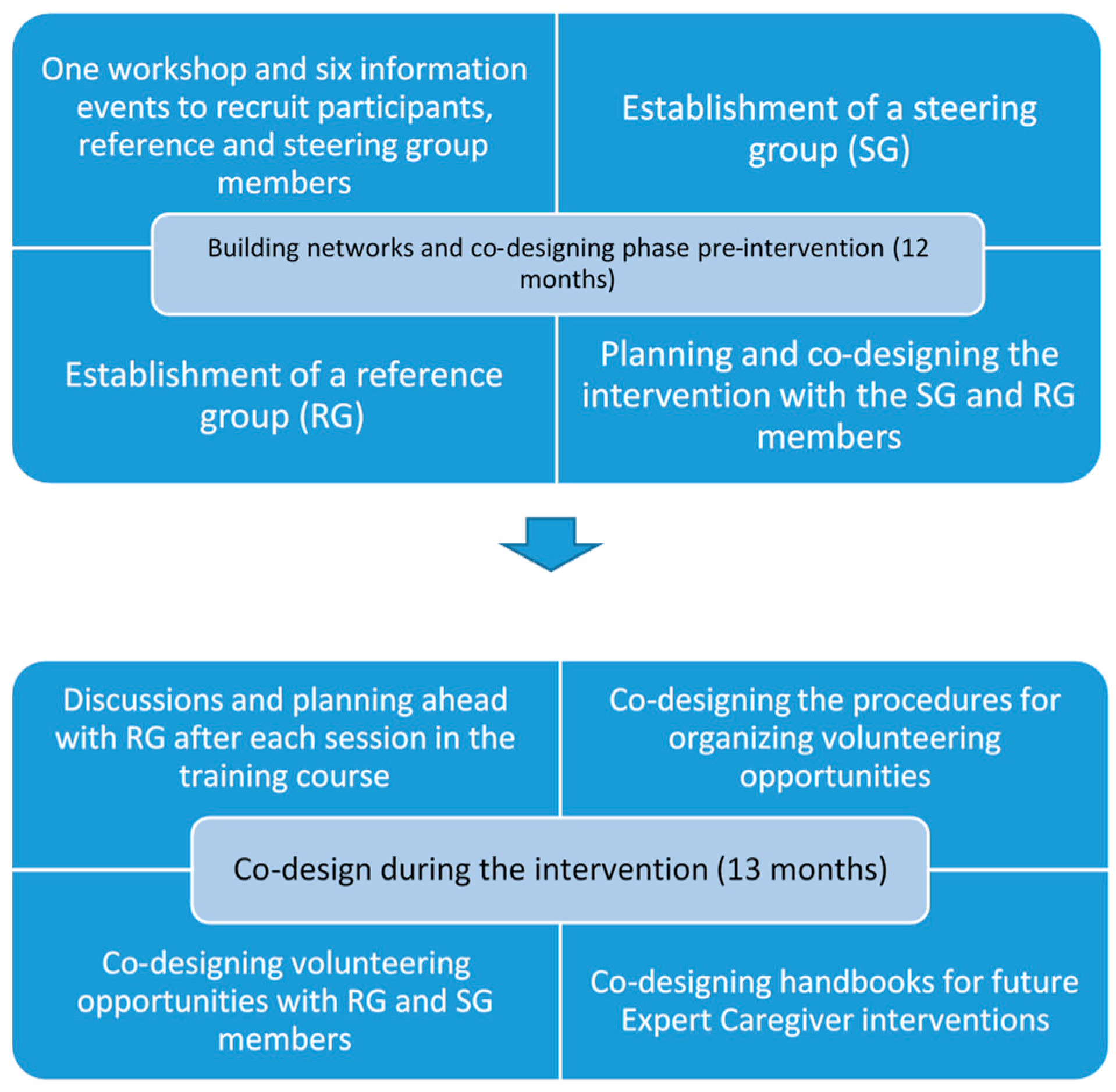
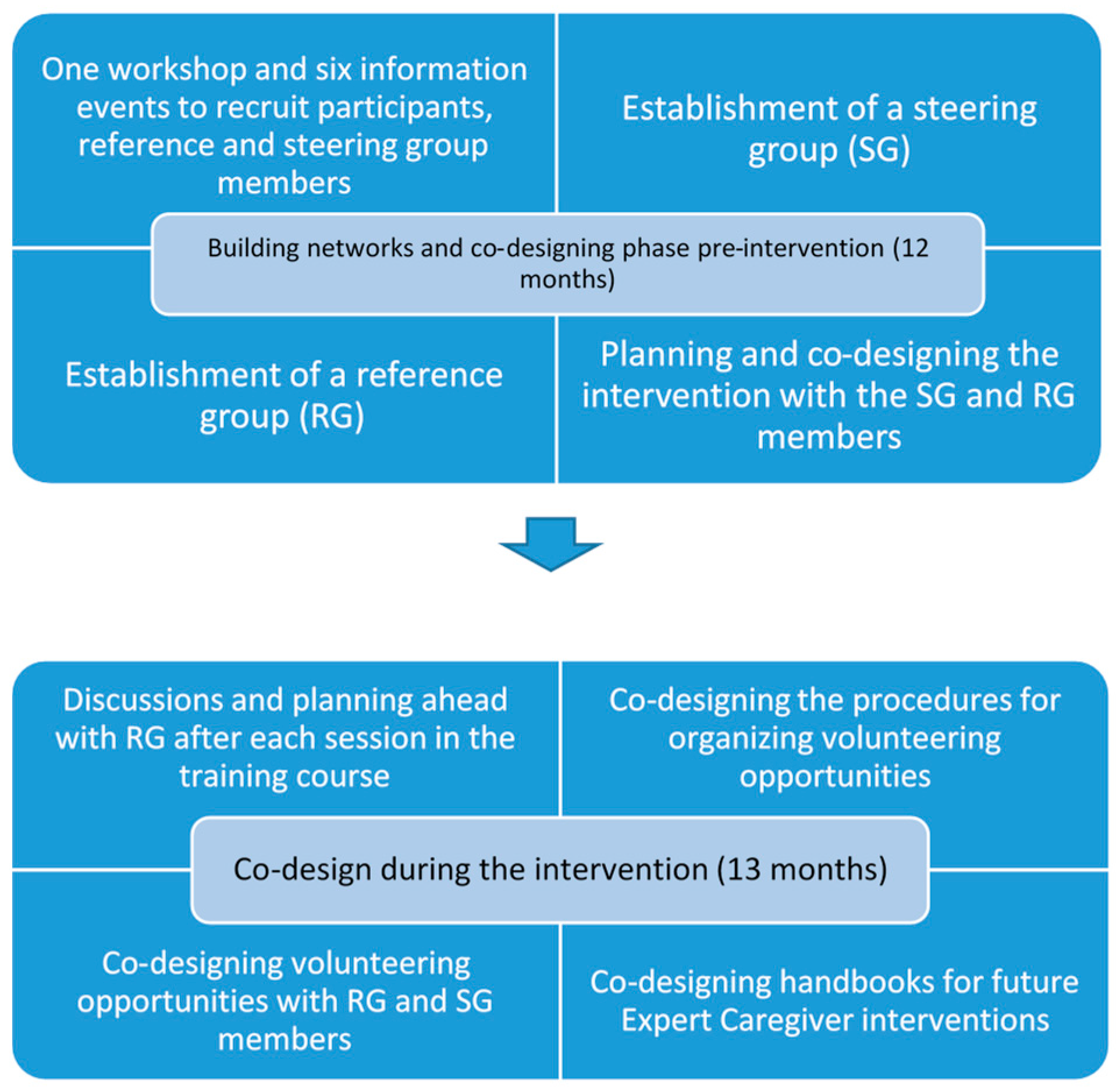
3.1. Co-Design and Implementation
3.2. Demand
3.3. Practicality: Ability to Carry Out Intervention Activities
3.3.1. Individual Barriers and Facilitators to Becoming an Expert Caregiver
Enough Distance to One’s Own Caregiving Experience
“It (the care recipient passing away) was about 2–3 years ago for me so I think I have the distance that is needed. As a recent widower I would not have been able to take on this assignment.”Male participant
“It’s the same for me, it was about 2 years ago that, that I experienced… I would not have been ready before that. Then I was so tired and… I think I needed to work through the grief and move on and find myself, who am I in this? Because one has lived, my husband was ill for 10 years, I lived through him for 10 years. /…/ When you are by yourself and it all runs off you, what do you do? Building, getting a new structure on everyday life… It takes time.”Female participant
Current Life Circumstances
“Well I had thirteen years of experience of providing care to my husband, but then I had to have surgery… I informed them (intervention facilitators) that I maybe could volunteer in the future but not at that time.”Female participant
“Somehow I ended up in a situation where I was an informal caregiver again, unpaid, and she… It was quite hard because she got very ill for a while and was in a hospital ward here in the X (municipality) and then I was in contact with the care staff daily, so I just went into that role completely. /…/ so I was not an Expert Caregiver, I was an informal caregiver.”Female participant
3.3.2. Competency as an Expert Caregiver
Using New and Old Skills
“I haven’t had any issues talking to people in the past either… So I’m not nervous when we get together.”Male participant
“The issue is that one wants to say: ‘in my case, it was like this’ but you shouldn’t do that (laughs). So it’s a little bit difficult to stay put in one’s place.”Male participant
Relationship between Expert Caregiver and Peer Support Receiver
“It wasn’t quite right /…/ I don’t know the reason why, if it was me or… /…/ If it’s a group in a small village, it can be difficult for the group participants to talk freely when there are others from the village around. I thought of that, that it was something… Something there that I couldn’t see. In the air.”Female participant
“When I became a peer supporter to this person I’m supporting, I was a bit hesitant at first because it’s an old acquaintance of mine. /…/ But it works well. And now I don’t know if it’s because I already knew her, that we can have a natural relationship.”Female participant
“I would like to have a stranger (as a peer support recipient) so that one could… Because trying to be an informal Expert Caregiver to old acquaintances is on another level.”Female participant
The Role of the Intervention Organizers for Feeling Safe
“I dare to take on that role and they (the caregivers) also feel safe, those that I know. Because we get these peer support recipients automatically, we do not need to have them assigned to us, they are automatically around us. But I feel safer having you in the background, someone to talk to, I can dial X (intervention organizer) for example and discuss if there is something I’m thinking about. For the peer support recipient’s sake as well.”Female participant
“As long as you don’t get a person who ‘takes the whole hand’. Then you have to be quite good at setting boundaries, but it can be difficult.”Female participant
“It can be difficult, but we have X’s (intervention organizer) support there.”Male participant
“But it’s not certain that it helps.”Female participant
3.3.3. Volunteering during COVID-19
“In the beginning it was difficult with the technique, but gradually it worked out and one became used to it. /…/ So it’s sort of fun, and enables connection with others.”Male participant
“It’s been, what should I say, alright but… You haven’t really been able to have the contact you meant to have, but we have been keeping in touch via telephone. It has worked well.”Female participant
“Well the telephone works of course, but it’s not the same (as meeting face to face).Male participant
“I lived in isolation but had daily social contact. For me it was a godsend that she (informal care recipient) came into my life and I got this role (as an informal caregiver).”Female participant
3.4. Practicality: Perceived Effects on Well-Being
3.4.1. Perceived Effects on the Participants’ Well-Being and Related Mediators
Expectations Influencing the Experience
“If one starts to demand too much of oneself and think that now I don’t live up to (the caregivers’ expectations), it should be better, I should… If you put too high demands on yourself, then it becomes a torment. That I’m not enough, they must have been disappointed with the meeting, ‘what was that, just sitting and drinking coffee and talking…’. You should have those demands on yourself on a reasonable level.”Female participant
The Needs of Caregivers as a Stressor
“I met someone who was in the same situation that I was in, who had just left her husband (having him admitted to a nursing home), and I felt so bad the entire evening when she told me, because I went back to how it had been for me. I thought about her all night after she told me.”Female participant
“The only negative thing is that more people should take advantage of peer support, that you would really get it out there to those needing it, because the needs are actually extensive.”Female participant
“There are a lot of people in X (municipality) who should get in touch with us, but they don’t.”Male participant
Volunteering as a Therapeutic, Meaningful, and Joyful Activity
“I feel that these Expert Caregiver conversations have rewarded me in that I have had to prepare myself, I haven’t dared to go unprepared to those conversations, but I have had to look through my life a bit in advance and try to formulate the questions that need to be ventilated. That has given me something to do… and been like therapy for myself as well.”Male participant
“It does open old wounds somewhat, but on the other hand, I think that the positive dimension outweighs it. After the discussions that I have been part of, I have been left with a good taste.”Male participant
“It’s also rewarding. It gives to someone who has gone through it. It heals you.”Female participant
“I have many times thought that what if this existed when we started off as informal caregivers and one would have received this.”Female participant
“And at times, I felt very important. And that was nice.”Male participant
“We have felt needed when they lived. You had to give 100% and more. You felt needed and now when they are gone you also want to be needed, so now I feel like we have a sense of purpose.”Female participant
“I like these kinds of things, so I don’t mind it. It’s not work, it’s pleasure. If you can say that, perhaps you should not say that. But I really don’t mind it.”Male participant
A Sense of Belonging with the Other Participants
“And the thing is that when you become alone, there is so much where you feel like you don’t fit in, but in this context, we fit in.”Female participant
3.5. Sense of Coherence and Satisfaction with Life Scale
4. Discussion
4.1. Interpretation of Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Zigante, V. Exploring Formalisation, Availability and Quality; European Commission: Luxembourg, 2018. [Google Scholar]
- European Commission. Long-Term Care Report. Trends, Challenges and Opportunities in an Ageing Society; European Commission: Luxembourg, 2021. [Google Scholar]
- Pysklywec, A.; Plante, M.; Auger, C.; Mortenson, W.B.; Eales, J.; Routhier, F.; Demers, L. The positive effects of caring for family carers of older adults: A scoping review. Int. J. Care Caring 2020, 4, 349–375. [Google Scholar] [CrossRef]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef]
- Eurocarers/IRCCS-INRCA. Impact of the COVID-19 Outbreak on Informal Carers Across Europe—Final Report. European Commission: Brussels/Ancona. 2021. Available online: https://eurocarers.org/publications/impact-of-the-covid-19-outbreak-on-informal-carers-across-europe/ (accessed on 20 July 2021).
- Verbakel, E. How to understand informal caregiving patterns in Europe? The role of formal long-term care provisions and family care norms. Scand J. Public Health 2018, 46, 436–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corey, K.L.; McCurry, M.K.; Sethares, K.A.; Bourbonniere, M.; Hirschman, K.B.; Meghani, S.H. Predictors of psychological distress and sleep quality in former family caregivers of people with dementia. Aging Ment. Health 2020, 24, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.C.; Wen, F.H.; Chen, J.S.; Chou, W.C.; Shen, W.C.; Tang, S.T. Preloss Psychosocial Resources Predict Depressive Symptom Trajectories Among Terminally Ill Cancer Patients’ Caregivers in Their First Two Years of Bereavement. J. Pain Symptom Manag. 2019, 58, 29–38. [Google Scholar] [CrossRef]
- Tsai, W.-I.; Prigerson, H.G.; Li, C.-Y.; Chou, W.-C.; Kuo, S.-C.; Tang, S.T. Longitudinal changes and predictors of prolonged grief for bereaved family caregivers over the first 2 years after the terminally ill cancer patient’s death. Palliat. Med. 2016, 30, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Larkin, M. Life after Caring: The Post-Caring Experiences of Former Carers. Br. J. Soc. Work 2009, 39, 1026–1042. [Google Scholar] [CrossRef]
- Currow, D.C.; Burns, C.; Agar, M.; Phillips, J.; McCaffrey, N.; Abernethy, A.P. Palliative Caregivers Who Would Not Take on the Caring Role Again. J. Pain Symptom Manag. 2011, 41, 661–672. [Google Scholar] [CrossRef]
- Erikson, E. Childhood and Society, 2nd ed.; Norton: New York, NY, USA, 1993. [Google Scholar]
- von Bonsdorff, M.B.; Rantanen, T. Benefits of formal voluntary work among older people. A review. Aging Clin. Exp. Res. 2011, 23, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.D.; Damianakis, T.; Kröger, E.; Wagner, L.M.; Dawson, D.R.; Binns, M.A.; Bernstein, S.; Caspi, E.; Cook, S.L. The benefits associated with volunteering among seniors: A critical review and recommendations for future research. Psychol. Bull. 2014, 140, 1505–1533. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, D.; Rosato, M.; Moriarty, J.; Leavey, G. Volunteering and mortality risk: A partner-controlled quasi-experimental design. Int. J. Epidemiol. 2017, 46, 1295–1302. [Google Scholar] [CrossRef] [Green Version]
- Musick, M.A.; Herzog, A.R.; House, J.S. Volunteering and Mortality Among Older Adults: Findings from a National Sample. J. Gerontol. Ser. B 1999, 54, S173–S180. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing: Healthy Ageing and Functional Ability. Available online: https://www.who.int/news-room/q-a-detail/ageing-healthy-ageing-and-functional-ability (accessed on 30 May 2021).
- Carter, G.; Monaghan, C.; Santin, O. What is known from the existing literature about peer support interventions for carers of individuals living with dementia: A scoping review. Heal. Soc. Care Community 2020, 28, 1134–1151. [Google Scholar] [CrossRef]
- Charlesworth, G.; Sinclair, J.B.; Brooks, A.; Sullivan, T.; Ahmad, S.; Poland, F. The impact of volunteering on the volunteer: Findings from a peer support programme for family carers of people with dementia. Heal. Soc. Care Community 2016, 25, 548–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, A.; Farquharson, L.; Burnell, K.; Charlesworth, G. A Narrative Enquiry of Experienced Family Carers of People with Dementia Volunteering in a Carer Supporter Programme. J. Community Appl. Soc. Psychol. 2014, 24, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Halvorsrud, L.; Bye, A.; Brekke, L.A.; Bergland, A. Being a trained volunteer Peer Supporter for carers of people living with dementia in Norway: Reciprocal benefits and challenges. Health Soc. Care Community 2020, 28, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Population Structure and Ageing. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 22 June 2021).
- Social Welfare Act 710/1982. Available online: http://finlex.fi/en/laki/kaannokset/1982/en19820710_20140491.pdf (accessed on 29 July 2021).
- Act on Informal Care Allowance 2.12.937/2005. Available online: https://www.finlex.fi/fi/laki/ajantasa/2012/20120980 (accessed on 29 July 2021).
- Ministry of Social Affairs and Health. Development of Informal Care and Family Care in 2015–2018. Conclusions and Recommendations for Further Measures. Available online: http://urn.fi/URN:ISBN:978-952-00-4022-2 (accessed on 29 July 2021).
- Omaisena Edelleen. Omaisena Edelleen. (Still Next of Kin). Available online: https://omaisenaedelleen.fi/ (accessed on 16 June 2021).
- Polli. Omaishoidon Kokemusasiantuntijat. Experts by Experience in Informal Care. Available online: https://www.polli.fi/kokemusasiantuntijat/ (accessed on 21 June 2021).
- Agency for Health Quality and Assessment of Catalonia. Caregiving Firsthand. Available online: https://blog.aquas.cat/2017/11/02/expert-caregiver/?lang=en (accessed on 23 June 2021).
- Bjögvinsson, E.; Ehn, P.; Hillgren, P.-A. Design Things and Design Thinking: Contemporary Participatory Design Challenges. Des. Issues 2012, 28, 101–116. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How We Design Feasibility Studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Macdonald, H.; Johnston, M.; Lamb, S.E.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348. [Google Scholar] [CrossRef] [Green Version]
- Official Statistics of Finland. Appendix Table 2. Household-Dwelling Units by Housing Density on 31 Decemember 2018, by Region. Available online: https://www.stat.fi/til/asas/2018/01/asas_2018_01_2019-10-10_tau_002_en.html (accessed on 13 June 2021).
- Sotkanet Indicator Bank. Demographic Dependency Ratio. Life Expectancy at Birth. Available online: https://sotkanet.fi/sotkanet/en/taulukko/?indicator=s04Ks_b3BwA=®ion=szYPtDYqAQA=&year=sy5ztDbS0zUEAA==&gender=t&abs=f&color=f&buildVersion=3.0-SNAPSHOT&buildTimestamp=202103120740 (accessed on 22 June 2021).
- Reini, K.; Saarela, J. Life Expectancy of the Ethnically Mixed: Register-Based Evidence from Native Finns. Int. J. Environ. Res. Public Heal. 2021, 18, 3415. [Google Scholar] [CrossRef] [PubMed]
- Nyqvist, F.; Nygård, M.; Snellman, F. Active ageing: Results from Western Finland. Finn. J. Soc. Res. 2019, 12, 55–66. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; SAGE Publications: San Fransisco, CA, USA, 2012; pp. 127–139. [Google Scholar]
- Diener, E. Understanding Scores on the Satisfaction with Life Scale Ed Diener. Available online: http://labs.psychology.illinois.edu/~ediener/Documents/Understanding%20SWLS%20Scores.pdf (accessed on 29 June 2021).
- Smith, J.A.; Osborn, M. Interpretive phenomenological analysis. In Qualitative Psychology: A Practical Guide to Research Methods; Sage: London, UK, 2003; pp. 51–80. [Google Scholar]
- Noble, H.; Smith, J. Issues of validity and reliability in qualitative research. Evid. Based Nurs. 2015, 18, 34–35. [Google Scholar] [CrossRef] [Green Version]
- Finnish National Board on Research Integrity Tenk. Responsible Conduct of Research and Procedures for Handling Allegations of Misconduct in Finland. Available online: https://tenk.fi/en/advice-and-materials/guidelines-ethical-review-human-sciences (accessed on 22 June 2021).
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Heal. Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Waldrop, D.P.; McGinley, J.M. “I want to go home”: How location at death influences caregiver well-being in bereavement. Palliat. Support. Care 2020, 18, 691–698. [Google Scholar] [CrossRef]
- LaManna, J.B.; Unruh, L.; Chisholm, L.; Pericles, P.; Fotovvat, H. Perceptions of health and well-being among older adult caregivers: Comparisons of current caregivers with former and never caregivers. Geriatr. Nurs. 2020, 41, 429–435. [Google Scholar] [CrossRef]
- Corey, M.K.L.; McCurry, M.K. When Caregiving Ends: The Experiences of Former Family Caregivers of People with Dementia. Gerontologist 2017, 58, e87–e96. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef]

{kind=link}
| Session | Components |
|---|---|
| Training course session 1/3 August 2019 Theme: Me as an informal caregiver then and now (4 h) |
|
| |
| Training course session 2/3 October 2019 Theme: The everyday puzzle of an informal caregiver (camp, 5 h + 8 h) |
|
| October 2019–September 2020 11 months long period of optional volunteering opportunities coordinated by the intervention providers |
|
| Training course session 3/3 December 2019 Theme: Me as an Expert Caregiver—the journey so far and what next? (5 h) |
|
| Follow-up session September 2020 Theme: Coping as an Expert Caregiver (3 h) |
|
| Variable | n | % | Mean | Range | SD |
|---|---|---|---|---|---|
| Age | 72.52 | 57–82 | 6.93 | ||
| Gender | |||||
| Female | 18 | 78.3 | |||
| Male | 5 | 21.7 | |||
| Education | |||||
| Lower secondary | 7 | 30.4 | |||
| Upper secondary | 16 | 69.6 | |||
| Household | |||||
| Alone | 19 | 82.6 | |||
| With someone | 4 | 17.3 | |||
| Relationship to main CR | |||||
| Spouse | 18 | 78.3 | |||
| Parent | 5 | 21.7 | |||
| Years since main caregiving ended | 21 | 2.48 | 0–16 | 4.06 | |
| Years of caregiving to main CR | 8.13 | 0–37 | 7.43 | ||
| Age of former CR at death | 21 | 78.29 | 62–101 | 10.15 | |
| Diagnosis of main CR | |||||
| Cognitive disorder | 9 | 39.1 | |||
| Other | 14 | 60.9 |
| Research Focus | Main Theme | Subthemes |
|---|---|---|
| 3.3. Practicality: Ability of participants to carry out activities | 3.3.1. Individual barriers and facilitators to becoming an Expert Caregiver | Enough distance to one’s own caregiving experienceCurrent life circumstances |
| 3.3.2. Competency as an Expert Caregiver | Using new and old skills Relationship between Expert Caregiver and peer support recipient The role of the intervention organizers for feeling safe | |
| 3.3.3. Volunteering during COVID-19 | ||
| 3.4. Practicality: Perceived effects on well-being | 3.4.1. Perceived effects on the participants’ well-being and related Mediators | Expectations influencing the experience The needs of caregivers as a stressor Volunteering as a therapeutic, meaningful or joyful activity A sense of belonging with the other participants |
| Variable | T1 (n = 25) | T2 (n = 24) | T3 (n = 23) |
|---|---|---|---|
| SOC | 67.60, 8.20, 51–82, 69 | 68.96, 7.79, 48–86, 69.5 | 68.52, 8.63, 50–81, 70 |
| Comprehensability | 24.64, 4.20, 14–32, 25 | 25.67, 3.63, 19–33, 26 | 25.43, 3.57, 17–31, 26 |
| Manageability | 20.24, 2.85, 14–25, 21 | 20.75, 2.97, 13–26, 21 | 20.52, 3.93, 9–25, 22 |
| Meaningfulness | 22.72, 3.08, 18–28, 23 | 22.54, 2.99, 16–27, 22.5 | 22.57, 3.30, 14–26, 23 |
| SLWS | 25.92, 5.24, 12–33, 26 | 26.38, 5.77, 15–34, 29 | 26.61, 4.92, 16–34, 28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Åkerman, S.; Nyqvist, F.; Coll-Planas, L.; Wentjärvi, A. The Expert Caregiver Intervention Targeting Former Caregivers in Finland: A Co-Design and Feasibility Study Using Mixed Methods. Int. J. Environ. Res. Public Health 2021, 18, 10133. https://doi.org/10.3390/ijerph181910133
Åkerman S, Nyqvist F, Coll-Planas L, Wentjärvi A. The Expert Caregiver Intervention Targeting Former Caregivers in Finland: A Co-Design and Feasibility Study Using Mixed Methods. International Journal of Environmental Research and Public Health. 2021; 18(19):10133. https://doi.org/10.3390/ijerph181910133
Chicago/Turabian StyleÅkerman, Sarah, Fredrica Nyqvist, Laura Coll-Planas, and Annika Wentjärvi. 2021. "The Expert Caregiver Intervention Targeting Former Caregivers in Finland: A Co-Design and Feasibility Study Using Mixed Methods" International Journal of Environmental Research and Public Health 18, no. 19: 10133. https://doi.org/10.3390/ijerph181910133
APA StyleÅkerman, S., Nyqvist, F., Coll-Planas, L., & Wentjärvi, A. (2021). The Expert Caregiver Intervention Targeting Former Caregivers in Finland: A Co-Design and Feasibility Study Using Mixed Methods. International Journal of Environmental Research and Public Health, 18(19), 10133. https://doi.org/10.3390/ijerph181910133