
A New Interprofessional Community-Service Learning Program, HATS (Health Ambassador Teams for Seniors) to Improve Older Adults Attitudes about Telehealth and Functionality

Abstract
1. Introduction
1.1. Community-Based Service Learning
1.2. Project Rationale
2. Methods
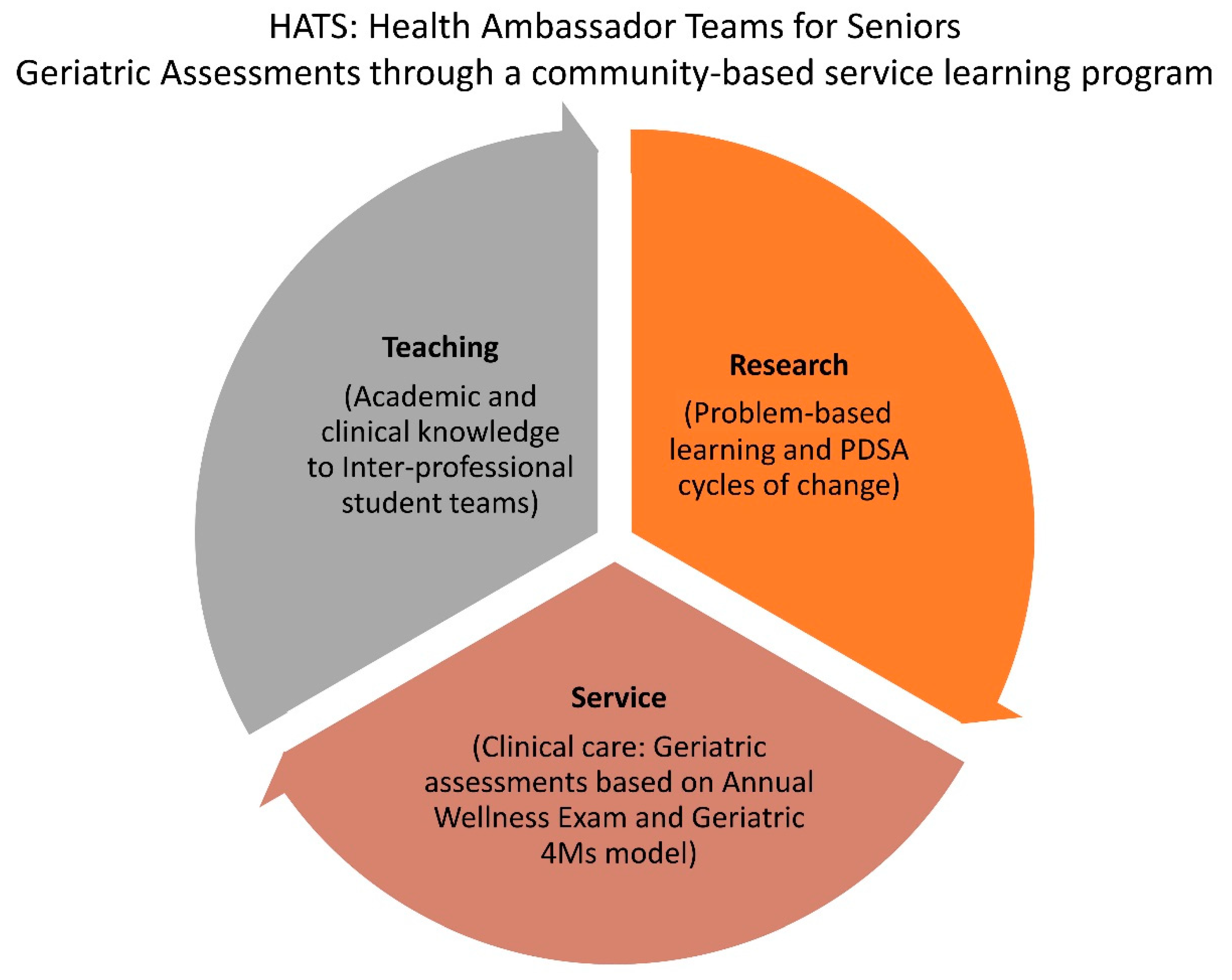
2.1. HATS Protocol
2.2. Structured Patient Visits and Instruction
3. Results
3.1. Proof of Concept
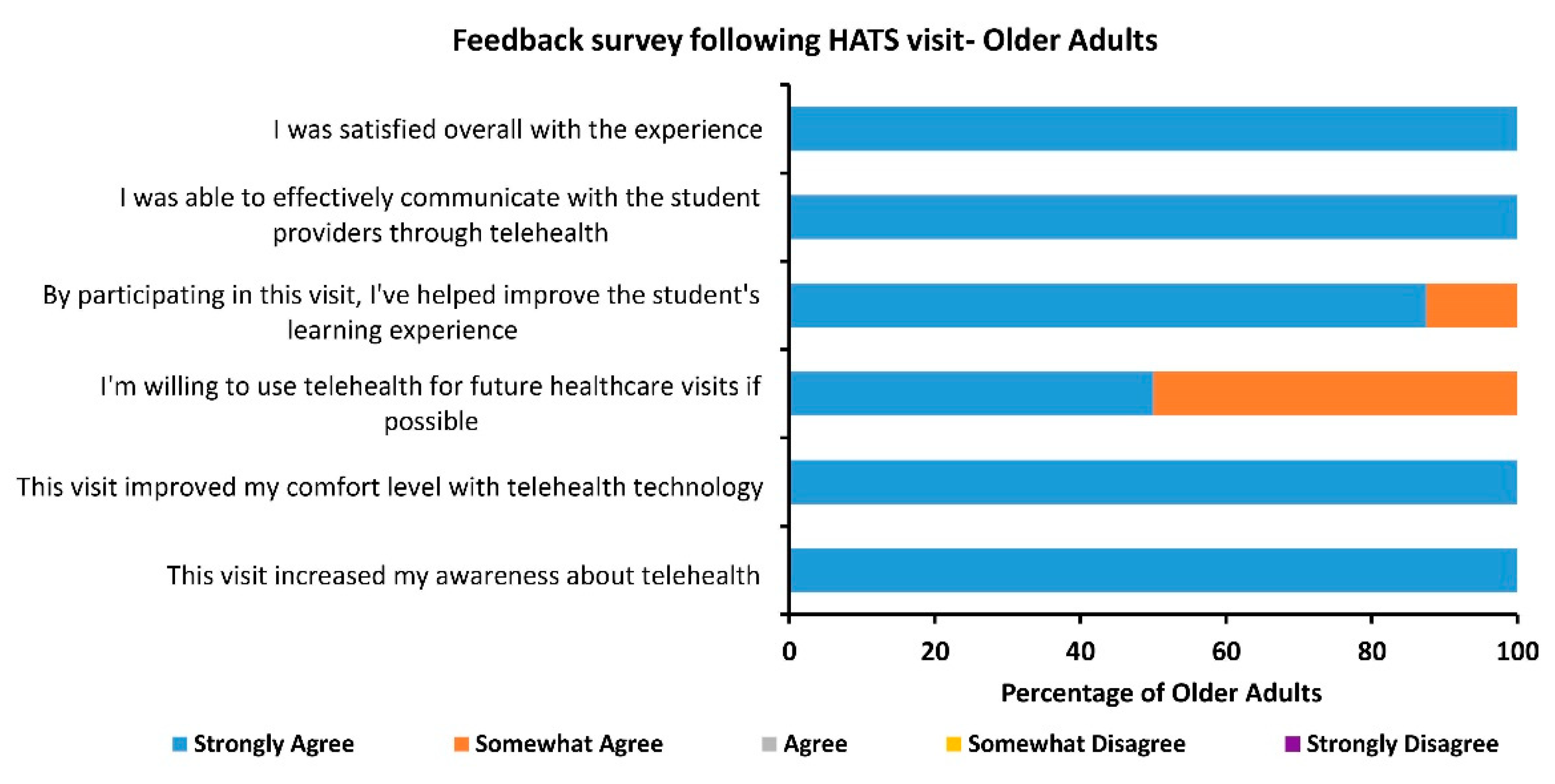
3.2. Feedback Surveys for Older Adults Were Well Received
3.3. Strengths and Weakness of the HATS Program
4. Discussion
4.1. HATS Assessment Protocol
4.2. IPE Competencies
- Work with individuals of other professions to maintain a climate of mutual respect and shared values.
- Use the knowledge of one’s own role and those of other professions to appropriately assess and address the health care needs of patients and to promote and advance the health of populations.
- Communicate with patients, families, communities, and professionals in health and other fields in a responsive and responsible manner that supports a team approach to the promotion and maintenance of health and the prevention and treatment of disease.
- Apply relationship-building values and the principles of team dynamics to perform effectively in different team roles to plan, deliver and evaluate patient/population-centered care and population health programs and policies that are safe, timely, efficient, effective, and equitable.
4.3. Health Disparities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Averill, N.J.; Sallee, J.M.; Robinson, J.T.; McFarlin, J.M.; Montgomery, A.A.; Burkhardt, G.A.; Schulz-Burton, M.D.; Elam, C.L. A First-Year Community-Based Service Learning Elective: Design, Implementation, and Reflection. Teach. Learn. Med. 2007, 19, 47–54. [Google Scholar] [CrossRef]
- Buckner, A.V.; Ndjakani, Y.D.; Banks, B.; Blumenthal, D.S. Using Service-Learning to Teach Community Health: The Morehouse School of Medicine Community Health Course. Acad. Med. 2010, 85, 1645–1651. [Google Scholar] [CrossRef] [PubMed]
- Elam, C.L.; Musick, D.W.; Sauer, M.J.; Skelton, J. How we implemented a service-learning elective. Med. Teach. 2002, 24, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.B.; Bonham, C.; Jones, L. Understanding the Goals of Service Learning and Community-Based Medical Education: A Systematic Review. Acad. Med. 2011, 86, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, A.L.; Cantwell, N.G.; Byerly, L.K.; Morhardt, D. Medical student education program in Alzheimer’s disease: The PAIRS Program. BMC Med. Educ. 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.; Blinkhorn, L.M.; Schumann, S.-A.; Reddy, S.T. Promoting Sustainable Community Service in the 4th Year of Medical School: A Longitudinal Service-Learning Elective. Teach. Learn. Med. 2014, 26, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Long, J.A.; Lee, R.S.; Federico, S.; Battaglia, C.; Wong, S.; Earnest, M. Developing leadership and advocacy skills in medical students through service learning. J. Public Health Manag. Pract. 2011, 17, 369–372. [Google Scholar] [CrossRef]
- Stearns, J.A.; Stearns, M.A.; Glasser, M.; Londo, R.A. Illinois RMED: A comprehensive program to improve the supply of rural family physicians. Fam. Med. 2000, 32, 5. [Google Scholar]
- Felten, P.; Clayton, P.H. Service-learning. New Dir. Teach. Learn. 2011, 2011, 75–84. [Google Scholar] [CrossRef]
- Stewart, T.; Wubbena, Z. An overview of infusing service-learning in medical education. Int. J. Med. Educ. 2014, 5, 147–156. [Google Scholar] [CrossRef]
- Bickerton, L.; Siegart, N.; Marquez, C. Medical Students Screen for Social Determinants of Health: A Service Learning Model to Improve Health Equity. Primer 2020, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- De Los Santos, M.; McFarlin, C.D.; Martin, L. Interprofessional education and service learning: A model for the future of health professions education. J. Interprof Care 2014, 28, 374–375. [Google Scholar] [CrossRef]
- Meili, R.; Fuller, D.; Lydiate, J. Teaching social accountability by making the links: Qualitative evaluation of student experiences in a service-learning project. Med. Teach. 2011, 33, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Cashman, S.B.; Seifer, S.D. Service-learning: An integral part of undergraduate public health. Am. J. Prev. Med. 2008, 35, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Mayne, L.; Glascoff, M. Service Learning: Preparing a Healthcare Workforce for the Next Century. Nurse Educ. 2002, 27, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Seifer, S.D. Service-learning: Community-campus partnerships for health professions education. Acad. Med. 1998, 73, 273–277. [Google Scholar] [CrossRef]
- Doucet, S.; Lauckner, H.; Wells, S. Patients’ Messages as Educators in an Interprofessional Health Education Program. J. Res. Interprofessional Pract. Educ. 2013, 3. [Google Scholar] [CrossRef]
- Eleazer, G.P.; Stewart, T.J.; Wieland, G.D.; Anderson, M.B.; Simpson, D.; Steering Committee of the National Evaluation of Senior Mentor Programs. The national evaluation of senior mentor programs: Older adults in medical education. J. Am. Geriatr. Soc. 2009, 57, 321–326. [Google Scholar] [CrossRef]
- Lucas, B.; Pearson, D. Patient perceptions of their role in undergraduate medical education within a primary care teaching practice. Educ. Prim. Care 2012, 23, 277–285. [Google Scholar] [CrossRef]
- Towle, A.; Bainbridge, L.; Godolphin, W.; Katz, A.; Kline, C.; Lown, B.; Madularu, I.; Solomon, P.; Thistlethwaite, J. Active patient involvement in the education of health professionals: Active patient involvement in education. Med. Educ. 2010, 44, 64–74. [Google Scholar] [CrossRef]
- 2017 National Population Projections Tables: Main Series; The United States Census Bureau: Suitland, Suitland-Silver Hill, MD, USA, 2017.
- Reilly, J.M.; Halle, A.; Resnik, C.; Teoh, J.; Williams, B.; Harris, P.; Segal-Gidan, F. Qualitative Analysis of an Inter-Professional, In-Home, Community Geriatric Educational Training Program. Gerontol. Geriatr. Med. 2021, 7, 2333721421997203. [Google Scholar] [CrossRef]
- Kuzuya, M. Era of geriatric medical challenges: Multimorbidity among older patients. Geriatr. Gerontol. Int. 2019, 19, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Lester, P.E.; Dharmarajan, T.S.; Weinstein, E. The Looming Geriatrician Shortage: Ramifications and Solutions. J. Aging Health 2020, 32, 1052–1062. [Google Scholar] [CrossRef]
- American Geriatrics Society. Geriatrics Workforce by the Numbers. 2018. Available online: https://www.americangeriatrics.org/geriatrics-profession/about-geriatrics/geriatrics-workforce-numbers (accessed on 23 September 2021).
- Lee, W.-C.; Sumaya, C.V. Geriatric Workforce Capacity: A Pending Crisis for Nursing Home Residents. Front. Public Health 2013, 1, 24. [Google Scholar] [CrossRef] [PubMed]
- Callahan, K.E.; Tumosa, N.; Leipzig, R.M. Big ‘G’ and Little ‘g’ Geriatrics Education for Physicians. J. Am. Geriatr. Soc. 2017, 65, 2313–2317. [Google Scholar] [CrossRef]
- Institute for Healthcare Improvement. Age-Friendly Health Systems: Guide to Using the 4Ms in the Care of Older Adults. 2020. Available online: http://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Documents/IHIAgeFriendlyHealthSystems_GuidetoUsing4MsCare.pdf (accessed on 23 September 2021).
- Bell, S.P.; Vasilevskis, E.; Saraf, A.A.; Ba, J.M.L.J.; Kripalani, S.; Mixon, A.S.; Schnelle, J.F.; Simmons, S.F. Geriatric Syndromes in Hospitalized Older Adults Discharged to Skilled Nursing Facilities. J. Am. Geriatr. Soc. 2016, 64, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric Syndromes: Clinical, Research, and Policy Implications of a Core Geriatric Concept. J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Fried, T. The end of the disease era. Am. J. Med. 2004, 116, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Lucchetti, G.; Granero, A.L. Use of comprehensive geriatric assessment in general practice: Results from the ‘Senta Pua’ project in Brazil. Eur. J. Gen. Pract. 2010, 17, 20–27. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Colburn, J.L.; Nothelle, S. The Medicare Annual Wellness Visit. Clin. Geriatr. Med. 2018, 34, 1–10. [Google Scholar] [CrossRef]
- Katz, S. Assessing Self-maintenance: Activities of Daily Living, Mobility, and Instrumental Activities of Daily Living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [CrossRef]
- Levis, B.; Sun, Y.; He, C.; Wu, Y.; Krishnan, A.; Bhandari, P.M.; Neupane, D.; Imran, M.; Brehaut, E.; Negeri, Z.; et al. Accuracy of the PHQ-2 Alone and in Combination With the PHQ-9 for Screening to Detect Major Depression: Systematic Review and Meta-analysis. JAMA 2020, 323, 2290–2300. [Google Scholar] [CrossRef]
- Borson, S.; Scanlan, J.; Brush, M.; Vitaliano, P.; Dokmak, A. The mini-cog: A cognitive ’vital signs’ measure for dementia screening in multi-lingual elderly. Int. J. Geriatr. Psychiatry 2000, 15, 1021–1027. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Duncan, R.P.; Leddy, A.L.; Earhart, G.M. Five times sit-to-stand test performance in Parkinson’s disease. Arch. Phys. Med. Rehabil. 2011, 92, 1431–1436. [Google Scholar] [CrossRef]
- Rossiter-Fornoff, J.E.; Wolf, S.L.; Wolfson, L.I.; Buchner, D.M. A Cross-sectional Validation Study of the FICSIT Common Data Base Static Balance Measures. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 1995, 50, M291–M297. [Google Scholar] [CrossRef] [PubMed]
- Knipscheer, J.W.; Sleijpen, M.; Mooren, T.; Ter Heide, F.J.; van der Aa, N. Trauma exposure and refugee status as predictors of mental health outcomes in treatment-seeking refugees. BJPsych Bull. 2015, 39, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Levin, P.F.; Cary, A.H.; Kulbok, P.; Leffers, J.; Molle, M.; Polivka, B.J. Graduate Education for Advanced Practice Public Health Nursing: At the Crossroads. Public Health Nurs. 2008, 25, 176–193. [Google Scholar] [CrossRef]
- Drawz, P.E.; Pajewski, N.M.; Bates, J.T.; Bello, N.A.; Cushman, W.C.; Dwyer, J.P.; Fine, L.J.; Goff Jr, D.C.; Haley, W.E.; Krousel-Wood, M.; et al. Effect of Intensive Versus Standard Clinic-Based Hypertension Management on Ambulatory Blood Pressure: Results From the SPRINT (Systolic Blood Pressure Intervention Trial) Ambulatory Blood Pressure Study. Hypertension 2017, 69, 2–50. [Google Scholar] [CrossRef]
- Clemson, L.; Cumming, R.G.; Kendig, H.; Swann, M.; Heard, R.; Taylor, K. The Effectiveness of a Community-Based Program for Reducing the Incidence of Falls in the Elderly: A Randomized Trial: Effectiveness of a Falls Prevention Program. J. Am. Geriatr. Soc. 2004, 52, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Larkey, L.K.; Day, S.H.; Houtkooper, L.; Renger, R. Osteoporosis prevention: Knowledge and behavior in a southwestern community. J. Community Health 2003, 28, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Crump, J.R. Learning by Doing: Implementing Community Service-based Learning. J. Geogr. 2002, 101, 144–152. [Google Scholar] [CrossRef]
- Interprofessional Education Collaborative. Core Competencies for Interprofessional Collaborative Practice: 2016 Update; Interprofessional Education Collaborative: Washington, DC, USA, 2016; Available online: https://ipec.memberclicks.net/assets/2016-Update.pdf (accessed on 23 September 2021).
- Hill, C.V.; Pérez-Stable, E.J.; Anderson, N.A.; Bernard, M.A. The National Institute on Aging Health Disparities Research Framework. Ethn. Dis. 2015, 25, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.X.; Luo, M.; Zhang, A.; Li, L.W. Associations of Ageism and Health: A Systematic Review of Quantitative Observational Studies. Res. Aging 2021, 43, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Saif-Ur-Rahman, K.; Mamun, R.; Eriksson, E.; He, Y.; Hirakawa, Y. Discrimination against the elderly in health-care services: A systematic review. Psychogeriatrics 2021, 21, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, I.; Souza, J.; McWilliams, J.M.; Mehrotra, A. Practices Caring For The Underserved Are Less Likely To Adopt Medicare’s Annual Wellness Visit. Health Aff. 2018, 37, 283–291. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Geriatric 4M’s | Tests Utilized in Assessment |
|---|---|
| What Matters | (1) Questions on patient priorities for health and daily activities of living (e.g., “What would you like us to know about you?”, “What matters most to you about your health?”) [28] (2) Functional ability and quality of life through the Katz Activities of Daily Living (ADLs) and Lawton-Brody Instrumental Activities of Daily Living (IADLs) [34] |
| Medications | Medication reconciliation accompanied by cross-screening with Beer’s Criteria for potentially inappropriate medications [35] |
| Mentation | Patient Health Questionnaire (PHQ-2) questionnaire for depression [28,36], Mini-Cog for cognitive impairment [37] |
| Mobility | (1) Timed-Up and Go (TUG) test [38], (2) Five-times sit-to-stand (5xSTS) [39], or (3) Four-stage balance test (FSBT) to measure fall risk [40] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurivich, D.; Schimke, C.; Snustad, D.; Floura, M.; Morton, C.; Waind, M.; Holloway, J.; Janssen, S.; Danks, M.; Semmens, K.; et al. A New Interprofessional Community-Service Learning Program, HATS (Health Ambassador Teams for Seniors) to Improve Older Adults Attitudes about Telehealth and Functionality. Int. J. Environ. Res. Public Health 2021, 18, 10082. https://doi.org/10.3390/ijerph181910082
Jurivich D, Schimke C, Snustad D, Floura M, Morton C, Waind M, Holloway J, Janssen S, Danks M, Semmens K, et al. A New Interprofessional Community-Service Learning Program, HATS (Health Ambassador Teams for Seniors) to Improve Older Adults Attitudes about Telehealth and Functionality. International Journal of Environmental Research and Public Health. 2021; 18(19):10082. https://doi.org/10.3390/ijerph181910082
Chicago/Turabian StyleJurivich, Donald, Carter Schimke, Dakota Snustad, Mitchell Floura, Casey Morton, Marsha Waind, Jeremy Holloway, Sclinda Janssen, Meridee Danks, Karen Semmens, and et al. 2021. "A New Interprofessional Community-Service Learning Program, HATS (Health Ambassador Teams for Seniors) to Improve Older Adults Attitudes about Telehealth and Functionality" International Journal of Environmental Research and Public Health 18, no. 19: 10082. https://doi.org/10.3390/ijerph181910082
APA StyleJurivich, D., Schimke, C., Snustad, D., Floura, M., Morton, C., Waind, M., Holloway, J., Janssen, S., Danks, M., Semmens, K., & Manocha, G. D. (2021). A New Interprofessional Community-Service Learning Program, HATS (Health Ambassador Teams for Seniors) to Improve Older Adults Attitudes about Telehealth and Functionality. International Journal of Environmental Research and Public Health, 18(19), 10082. https://doi.org/10.3390/ijerph181910082