
The Role of Social Context in Physiological and Psychological Restoration in a Forest: Case Study of a Guided Forest Therapy Program in Taiwan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Experimental Design
2.3. Participants
2.4. Physiological Measures
2.5. Psychological Measures
2.6. Statistical Analyses
3. Results
3.1. Demographic Information
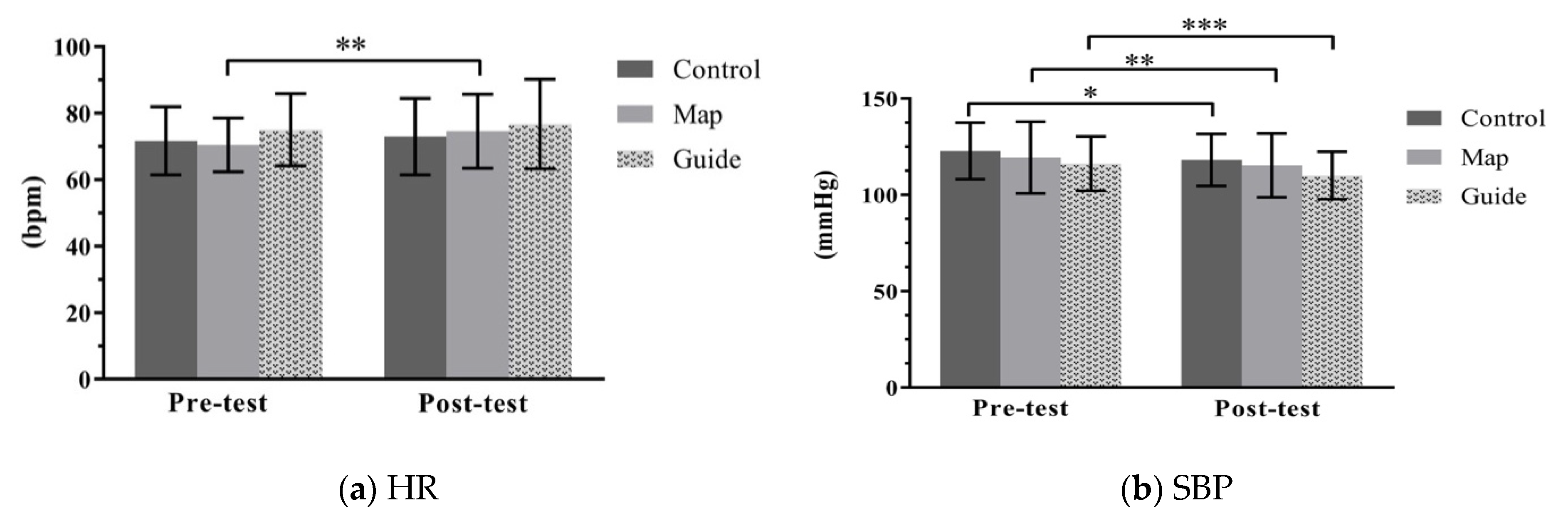
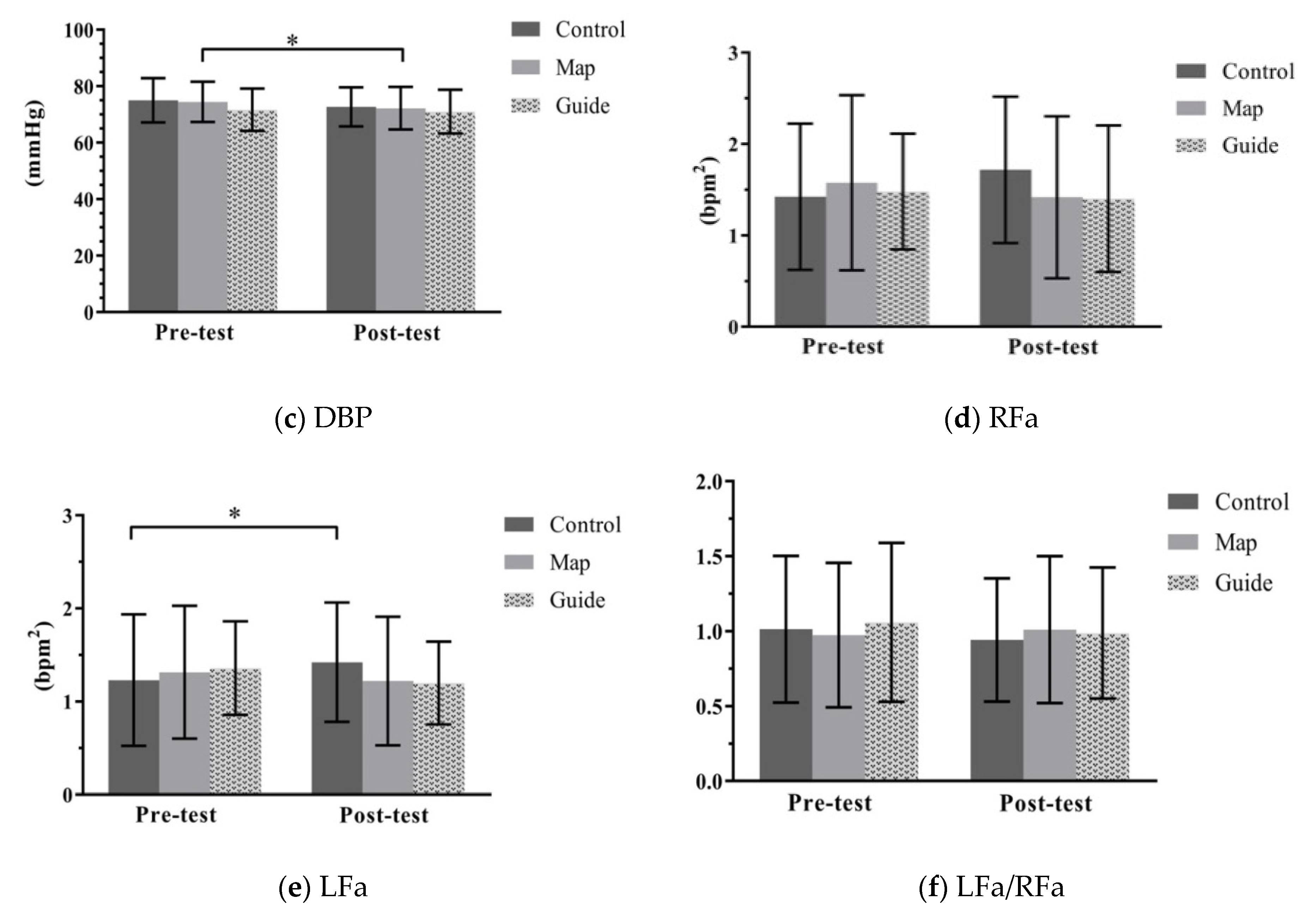
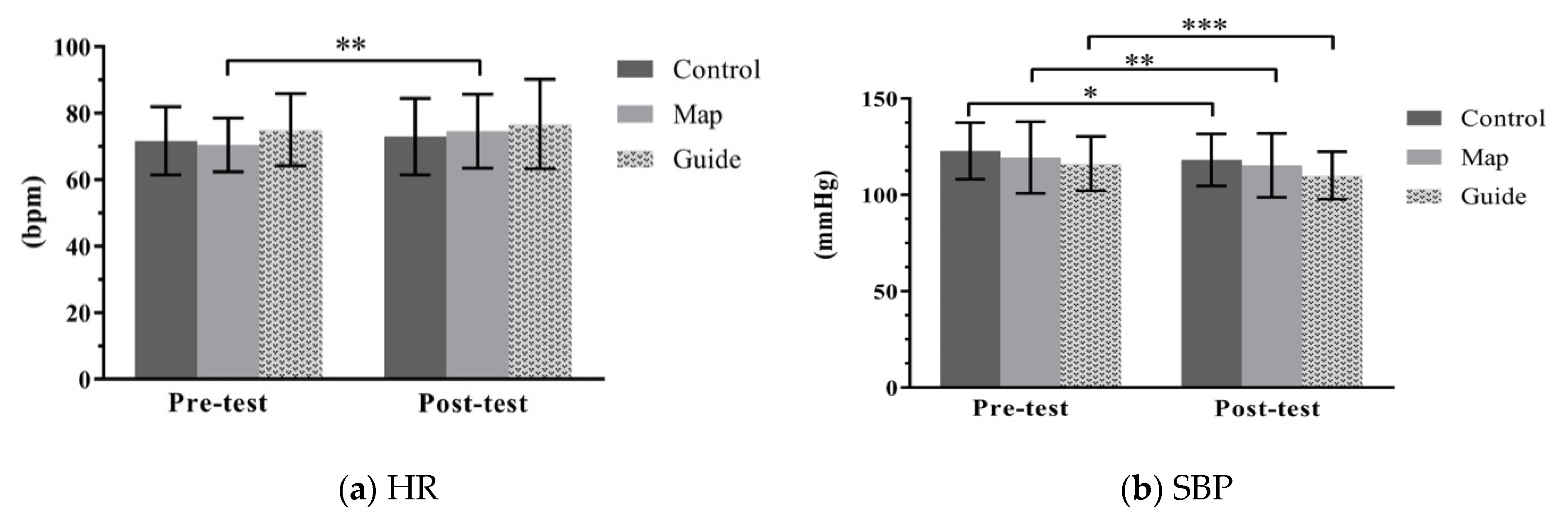
3.2. Influence of Programs on Physiological Responses
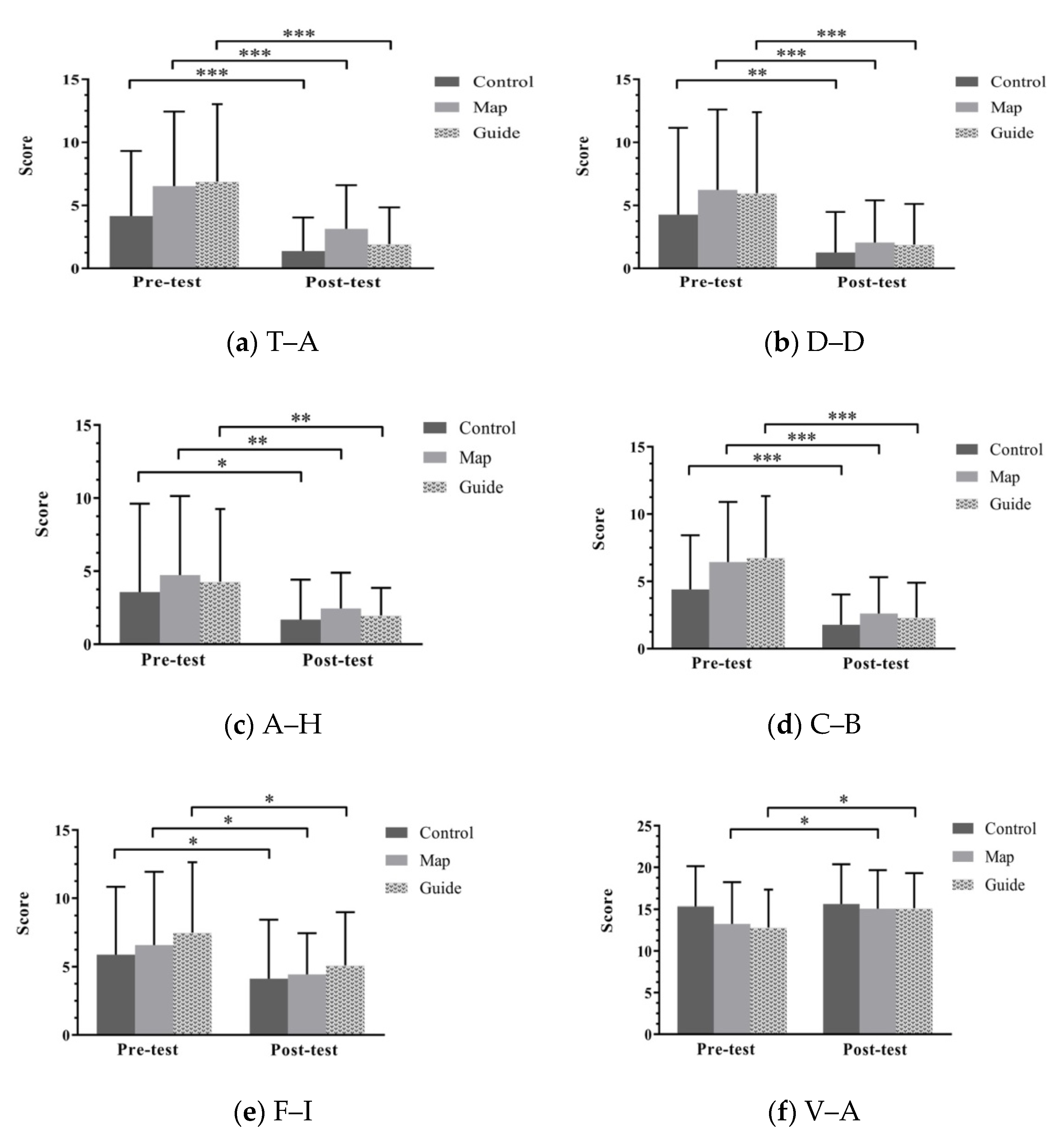
3.3. Influence of Programs on Psychological Response
4. Discussion
4.1. Influences of the Three Forest Therapy Programs on Physiological Responses
4.2. Influences of the Three Forest Therapy Programs on Psychological Responses
4.3. Comparisons of Changes in Physiological Responses and Mood States among the Three Programs
4.4. Limitations of the Study and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-analysis. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.-S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef]
- Ewert, A.; Chang, Y. Levels of Nature and Stress Response. Behav. Sci. 2018, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.-X.; Cao, Y.-B.; Lan, X.-G.; He, Z.-H.; Chen, Z.-M.; Wang, Y.-Z.; Hu, X.-L.; Lv, Y.-D.; Wang, G.-F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondo, M.C.; Jacoby, S.F.; South, E.C. Does spending time outdoors reduce stress? A review of real-time stress response to outdoor environments. Health Place 2018, 51, 136–150. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and Psychological Effects of a Forest Therapy Program on Middle-Aged Females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyazaki, Y.; Song, C.; Ikei, H. Preventive medical effects of nature therapy and their individual differences. Jpn. J. Physiol. Anthropol. 2015, 20, 19–32. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [Green Version]
- Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Yu, C.-P.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Lee, J.; Li, Q.; Tyrvinen, L.; Tsunetsugu, Y.; Park, B.-J.; Kagawa, T.; Miyazaki, Y. Nature Therapy and Preventive Medicine. In Public Health—Social and Behavioral Health; InTech Open Ltd.: London, UK, 2012. [Google Scholar]
- Crnic, M.; Kondo, M.C. Nature RX: Reemergence of pediatric nature-based therapeutic programs from the late 19th and early 20th centuries. Am. J. Public Health 2019, 109, 1371–1378. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.-J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Complement. Altern. Med. 2014, 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Park, B.-J.; Furuya, K.; Kasetani, T.; Takayama, N.; Kagawa, T.; Miyazaki, Y. Relationship between psychological responses and physical environments in forest settings. Landsc. Urban Plan. 2011, 102, 24–32. [Google Scholar] [CrossRef]
- Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.-J.; Li, Q.; Tyrväinen, L.; Miyazaki, Y.; Kagawa, T. Emotional, Restorative and Vitalizing Effects of Forest and Urban Environments at Four Sites in Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.-J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological effects of forest recreation in a young conifer forest in Hinokage Town, Japan. Silva Fenn. 2009, 43, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Park, B.-J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.; Ikei, H.; Miyazaki, Y. Sustained effects of a forest therapy program on the blood pressure of office workers. Urban For. Urban Green. 2017, 27, 246–252. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Park, B.-J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological Effects of Shinrin-yoku (Taking in the Atmosphere of the Forest) in an Old-Growth Broadleaf Forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsunetsugu, Y.; Lee, J.; Park, B.J.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing urban forest landscapes assessed by multiple measurements. Landsc. Urban Plan. 2013, 113, 90–93. [Google Scholar] [CrossRef]
- Park, B.-J.; Tsunetsugu, Y.; Ishii, H.; Furuhashi, S.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in a mixed forest in Shinano Town, Japan. Scand. J. For. Res. 2008, 23, 278–283. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazaki, Y.; et al. Forest bathing enhances human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2007, 20, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.; Wakayama, Y.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [Google Scholar] [PubMed]
- Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of Short Forest Bathing Program on Autonomic Nervous System Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef]
- Beil, K.; Hanes, D. The Influence of Urban Natural and Built Environments on Physiological and Psychological Measures of Stress—A Pilot Study. Int. J. Environ. Res. Public Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef] [Green Version]
- Komori, T.; Mitsui, M.; Togashi, K.; Matsui, J.; Kato, T.; Uei, D.; Shibayama, A.; Yamato, K.; Okumura, H.; Kinoshita, F. Relaxation Effect of a 2-Hour Walk in Kumano-Kodo Forest. J. Neurol. Neurosci. 2017, 8, 1. [Google Scholar] [CrossRef]
- Chen, H.-T.; Yu, C.-P.; Lee, H.-Y. The Effects of Forest Bathing on Stress Recovery: Evidence from Middle-Aged Females of Taiwan. Forests 2018, 9, 403. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.; Bürger-Arndt, R. How Forests Foster Human Health—Present State of Research-Based Knowledge (in the Field of Forests and Human Health). Int. For. Rev. 2014, 16, 421–446. [Google Scholar] [CrossRef]
- Igawahara, K.; Kagawa, T.; Takayama, N.; Park, B. Research on the Effect which a Guide Brings about in a Forest Walk. J. Jpn. Inst. Landsc. Archit. 2007, 70, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Staats, H.; Hartig, T. Alone or with a friend: A social context for psychological restoration and environmental preferences. J. Environ. Psychol. 2004, 24, 199–211. [Google Scholar] [CrossRef]
- Kaplan, S.; Kaplan, R. Cognition and Environment: Functioning in an Uncertain World; Kaplan, R., Ed.; Praeger: New York, NY, USA, 1982. [Google Scholar]
- Reis, H.T.; O’Keefe, S.D.; Lane, R.D. Fun Is More Fun When Others Are Involved. J. Posit. Psychol. 2017, 12, 547–557. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- College of Bio-Resources and Agriculture, National Taiwan University. The Experimental Forest; Lee, C.J., Wei Chiang, Y.-J.J., Eds.; College of Bio-Resources and Agriculture, National Taiwan University: Taipei, Taiwan, 2018. [Google Scholar]
- Tsai, M.J.; Yang, C.K.; Wu, T.Y.; Chen, W.L.; Lin, L.C. The healing forest—The new mission of the NTU Experimental Forest. For. Res. Newsl. 2016, 23, 16–19. [Google Scholar]
- Malliani, A.; Pagani, M.; Montano, N.; Mela, G.S. Sympathovagal balance: A reappraisal. Circulation 1998, 98, 2640–2643. [Google Scholar] [CrossRef] [Green Version]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Barger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef]
- Aysin, B.; Aysin, E. Effect of respiration in heart rate variability (HRV) analysis. In Proceedings of the 28th Annual International Conference of the IEEE Engineering in Medicine and Biology, New York, NY, USA, 30 August–3 September 2006; pp. 1776–1779. [Google Scholar]
- Colombo, J.; Arora, R.; DePace, N.L.; Vinik, A.I. Clinical Autonomic Dysfunction: Measurement, Indications, Therapies, and Outcomes; Springer International Publishing: New York, NY, USA, 2014; ISBN 9783319073712. [Google Scholar]
- Goldstein, D.S.; Bentho, O.; Park, M.-Y.; Sharabi, Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart rate variability and pain: Associations of two interrelated homeostatic processes. Biol. Psychol. 2008, 77, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Colombo, J.; Shoemaker, W.C.; Belzberg, H.; Hatzakis, G.; Fathizadeh, P.; Demetriades, D. Noninvasive Monitoring of the Autonomic Nervous System and Hemodynamics of Patients With Blunt and Penetrating Trauma. J. Trauma Inj. Infect. Crit. Care 2008, 65, 1364–1373. [Google Scholar] [CrossRef] [PubMed]
- Shacham, S. A Shortened Version of the Profile of Mood States. J. Pers. Assess. 1983, 47, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, D.M.; Rumrill, P.D. Pretest-Posttest Designs and Measurement of Change; IOS Press: Amsterdam, The Netherlands, 2003; Volume 20. [Google Scholar]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Does perceived restorativeness mediate the effects of perceived biodiversity and perceived naturalness on emotional well-being following group walks in nature? J. Environ. Psychol. 2016, 46, 217–232. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Programs | References |
|---|---|
| Alone (participants walking and/or watching in a forest individually) | Beil and Hanes [32]; Komori et al. [33]; Lee et al. [16]; Lee et al. [18]; Mao et al. [5]; Park et al. [20]; Park et al. [27]; Park et al. [10]; Park et al. [22]; Song et al. [8]; Takayama et al. [21]. |
| Guided (participants interacting with a guide) | Chen, Yu and Lee [34]; Ochiai et al. [7]; Ochiai et al. [11]; Song et al. [24]; Yu et al. [31]. |
| Locations | Activities | Senses | Time (min) |
|---|---|---|---|
| 1 | Warm-up and departing the aromatherapy room for Location 2 | 5 | |
| 2 | Starting point: explaining the sensory activities in the forest therapy program (visual, auditory, olfactory, and tactile) | 5 | |
| 3 | Strolling in a bamboo forest | Visual and tactile | 10 |
| 4 | Admiring forests, listening to a river, and exploring sounds from insects and birds | Visual and auditory | 10 |
| 5 | Cooling down with stream water; breathing and stretching exercises | Tactile and olfactory | 15 |
| Break | 10 | ||
| 6 | Walking on a Japanese cedar path and experiencing the forest’s density and serenity | Visual and auditory | 10 |
| 7 | Embracing trees and enjoying the forest air | Tactile and olfactory | 10 |
| 8 | Listening to nature in the quiet forest and sharing sounds with other participants | Auditory | 10 |
| 9 | Wrap-up | 5 |
| Demographics | N (%) | |
|---|---|---|
| Gender | Female | 40 (40.4) |
| Male | 59 (59.6) | |
| Age | 21–30 | 38 (38.4) |
| 31–50 | 14 (14.1) | |
| 51–65 | 41 (41.4) | |
| ≥66 | 6 (6.1) | |
| Education | Graduate school | 17 (17.2) |
| College | 58 (58.6) | |
| High school | 17 (17.2) | |
| Middle school and below | 7 (7.1) | |
| Living area | Urban | 45 (45.5) |
| Suburban | 42 (42.4) | |
| Rural | 9 (9.1) | |
| Others | 3 (3.0) | |
| Last time to visit nature | Within 1 week | 38 (38.4) |
| Between 1 week and half month | 30 (13.5) | |
| Between half month to 1 month | 8 (8.1) | |
| Over 1 month | 23 (23.3) |
| Indicators | N | Walk Alone Group (Control, C) | N | Self-Guided Group/Map (M) | N | Guided Group (G) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||||
| Physiological | HR (bpm) | 25 a | 71.7 ± 10.3 | 73.0 ± 11.5 | 33 b | 70.5 ± 8.1 | 74.1 ± 11.4 | 28 | 75.1 ± 10.8 | 76.8 ± 13.4 |
| SBP (mmHg) | 25 a | 123.0 ± 14.7 | 118.2 ± 13.6 | 33 b | 119.4 ± 18.6 | 115.8 ±16.4 | 28 | 116.3 ± 14.1 | 110.1 ± 12.3 | |
| DBP (mmHg) | 25 a | 75.0 ± 7.9 | 72.7 ± 6.9 | 33 b | 74.5 ± 7.1 | 72.5 ± 7.5 | 28 | 71.7 ± 7.5 | 71.0 ± 7.8 | |
| RFa (bpm2) | 25 a | 1.4 ± 0.8 | 1.7 ± 0.8 | 33 b | 1.6 ± 1.0 | 1.4 ± 0.9 | 28 | 1.5 ± 0.6 | 1.4 ± 0.8 | |
| LFa (bpm2) | 25 a | 1.2 ± 0.7 | 1.4 ±0.6 | 33 b | 1.3 ±0.7 | 1.2 ± 0.7 | 28 | 1.4 ± 0.5 | 1.2 ± 0.4 | |
| LFa/RFa | 25 a | 1.0 ± 0.5 | 0.9 ± 0.4 | 33 b | 1.0 ± 0.5 | 1.0 ± 0.5 | 28 | 1.1 ± 0.5 | 1.0 ± 0.4 | |
| Psychological | T–A | 37 | 4.2 ± 5.2 | 1.4 ± 2.7 | 34 | 6.5 ± 5.9 | 3.2 ± 3.5 | 28 | 6.9 ± 6.1 | 1.9 ± 2.9 |
| D–D | 37 | 4.3 ± 6.9 | 1.3 ± 3.2 | 34 | 6.2 ± 6.4 | 2.1 ± 3.4 | 28 | 6.0 ± 6.4 | 1.9 ± 3.2 | |
| A–H | 37 | 3.6 ± 6.1 | 1.7 ± 2.8 | 34 | 4.7 ± 5.4 | 2.4 ± 2.5 | 28 | 4.3 ± 5.0 | 2.0 ± 1.9 | |
| C–B | 37 | 4.4 ± 4.0 | 1.8 ± 2.3 | 34 | 6.4 ± 4.5 | 2.6 ± 2.7 | 28 | 6.8 ± 4.6 | 2.3 ± 2.6 | |
| F–I | 37 | 5.9 ± 5.0 | 4.1 ± 4.3 | 34 | 6.6 ± 5.4 | 4.4 ± 3.0 | 28 | 7.5 ± 5.2 | 5.1 ± 3.9 | |
| V–A | 37 | 15.4 ± 4.8 | 15.6 ± 4.8 | 34 | 13.3 ± 5.0 | 15.1 ± 4.6 | 28 | 12.8 ± 4.5 | 15.1 ± 4.2 | |
| Group C | Pre | Post | t | p | Change (%) |
| HR (bpm) | 71.7 ± 10.3 | 73.0 ± 11.5 | 0.872 | 0.392 | 1.73 |
| SBP (mmHg) | 122.8 ± 14.7 | 118.2 ± 13.6 | −2.741 | 0.011 * | −3.78 |
| DBP (mmHg) | 75.0 ± 7.9 | 72.7 ± 6.9 | −1.945 | 0.064 | −3.09 |
| RFa (bpm2) | 1.4 ± 0.8 | 1.7 ± 0.8 | 2.021 | 0.055 | 21.13 |
| LFa (bpm2) | 1.2 ± 0.7 | 1.4 ±0.6 | 2.184 | 0.039 * | 15.45 |
| LFa/RFa | 1.0 ± 0.5 | 0.9 ± 0.4 | −0.793 | 0.436 | −6.93 |
| Group M | Pre | Post | |||
| HR (bpm) | 70.5 ± 8.1 | 74.1 ± 11.4 | 3.413 | 0.002 ** | 5.12 |
| SBP (mmHg) | 119.4 ± 18.6 | 115.8 ±16.4 | −2.832 | 0.008 ** | −3.04 |
| DBP (mmHg) | 74.5 ± 7.1 | 72.5 ± 7.5 | −2.502 | 0.018* | −2.70 |
| RFa (bpm2) | 1.6 ± 1.0 | 1.4 ± 0.9 | −1.332 | 0.192 | −10.76 |
| LFa (bpm2) | 1.3 ±0.7 | 1.2 ± 0.7 | −0.933 | 0.358 | –6.87 |
| LFa/RFa | 1.0 ± 0.5 | 1.0 ± 0.5 | 0.373 | 0.711 | 4.12 |
| Group G | Pre | Post | |||
| HR (bpm) | 75.1 ± 10.8 | 76.8 ± 13.4 | 1.334 | 0.193 | 2.24 |
| SBP (mmHg) | 116.3 ± 14.1 | 110.1 ± 12.3 | −4.360 | 0.000 *** | −5.31 |
| DBP (mmHg) | 71.7 ± 7.5 | 71.0 ± 7.8 | −0.0733 | 0.470 | −0.93 |
| RFa (bpm2) | 1.5 ± 0.6 | 1.4 ± 0.8 | −0.0556 | 0.583 | −5.41 |
| LFa (bpm2) | 1.4 ± 0.5 | 1.2 ± 0.4 | −1.850 | 0.075 | −11.76 |
| LFa/RFa | 1.1 ± 0.5 | 1.0 ± 0.4 | −1.039 | 0.308 | −6.60 |
| Physiological Changes | Group | Mean ± SD | Change (%) | F | p | ηp2 | Post-hoc |
|---|---|---|---|---|---|---|---|
| △HR (bpm) | C | 1.24 ± 7.11 | 1.73 | 1.527 | 0.223 | 0.035 | |
| M | 4.12 ± 6.93 | 5.12 | |||||
| G | 1.67 ± 6.66 | 2.24 | |||||
| △SBP (mmHg) | C | −4.64 ± 8.47 | −3.78 | 0.594 | 0.555 | 0.014 | |
| M | −3.974 ± 8.05 | −3.04 | |||||
| G | −61.81 ± 7.50 | −5.31 | |||||
| △DBP (mmHg) | C | −2.321 ± 5.96 | −3.09 | 0.852 | 0.430 | 0.020 | |
| M | −2.24 ± 5.15 | −2.70 | |||||
| G | −0.68 ± 4.90 | −0.93 | |||||
| △RFa (bpm2) | C | 0.29 ± 0.73 | 21.13 | 3.102 | 0.050 | 0.070 | |
| M | −0.16 ± 0.68 | −10.76 | |||||
| G | −0.08 ± 0.73 | −5.41 | |||||
| △LFa (bpm2) | C | 0.19 ± 0.44 | 15.45 | 3.552 | 0.033 * | 0.079 | C > G |
| M | −0.10 ± 0.60 | −6.87 | |||||
| G | −0.16 ± 0.46 | −11.76 | |||||
| △LFa/RFa | C | −0.07 ± 0.45 | −6.93 | 0.527 | 0.592 | 0.013 | |
| M | 0.04 ± 0.57 | 4.12 | |||||
| G | 0.07 ± 0.47 | −6.60 |
| Group C | Pre | Post | t | p | Change (%) |
| T–A | 4.2 ± 5.2 | 1.38 ± 2.66 | −3.796 | 0.001 ** | −66.83 |
| D–D | 4.3 ± 6.9 | 1.27 ± 3.21 | −3.277 | 0.002 ** | −70.26 |
| A–H | 3.6 ± 6.1 | 1.68 ± 2.75 | −2.054 | 0.047 * | −52.94 |
| C–B | 4.4 ± 4.0 | 1.78 ± 2.25 | −4.401 | 0.000 *** | −59.64 |
| F–I | 5.9 ± 5.0 | 4.14 ± 4.32 | −2.286 | 0.028 * | −29.71 |
| V–A | 15.4 ± 4.8 | 15.62 ± 4.76 | 0.310 | 0.758 | 1.76 |
| Group M | Pre | Post | |||
| T–A | 6.5 ± 5.9 | 3.15 ± 3.46 | −4.307 | 0.000 *** | −51.76 |
| D–D | 6.2 ± 6.4 | 2.06 ± 3.35 | −5.409 | 0.000 *** | −66.99 |
| A–H | 4.7 ± 5.4 | 2.44 ± 2.45 | −3.088 | 0.004 ** | −45.41 |
| C–B | 6.4 ± 4.5 | 2.62 ± 2.70 | −6.760 | 0.000 *** | −59.32 |
| F–I | 6.6 ± 5.4 | 4.44 ± 3.03 | −2.421 | 0.021 * | −32.63 |
| V–A | 13.3 ± 5.0 | 15.09 ± 4.59 | 2.180 | 0.036 * | 13.80 |
| Group G | Pre | Post | |||
| T–A | 6.9 ± 6.1 | 1.9 ± 2.9 | −5.549 | 0.000 *** | −71.99 |
| D–D | 6.0 ± 6.4 | 1.9 ± 3.2 | −5.079 | 0.000 *** | −68.29 |
| A–H | 4.3 ± 5.0 | 2.0 ± 1.9 | −2.982 | 0.006 ** | −54.31 |
| C–B | 6.8 ± 4.6 | 2.3 ± 2.6 | −6.576 | 0.000 *** | −65.63 |
| F–I | 7.5 ± 5.2 | 5.1 ± 3.9 | −2.698 | 0.012 * | −31.87 |
| V–A | 12.8 ± 4.5 | 15.1 ± 4.2 | 2.444 | 0.021 * | 18.10 |
| Physiological Changes | Group | Mean ± SD | Change (%) | F | p | ηp2 | Post Hoc |
|---|---|---|---|---|---|---|---|
| ΔT–A | C | −2.78 ± 4.46 | −66.83 | 1.869 | 0.160 | 0.037 | |
| M | −3.38 ± 4.58 | −51.76 | |||||
| G | −4.96 ± 4.73 | −71.99 | |||||
| ΔD–D | C | −3.00 ± 5.57 | −70.26 | 0.628 | 0.536 | 0.013 | |
| M | −4.18 ± 4.50 | −66.99 | |||||
| G | −4.07 ± 4.24 | −68.29 | |||||
| ΔA–H | C | −2.321 ± 5.96 | −52.94 | 0.087 | 0.917 | 0.002 | |
| M | −2.24 ± 5.15 | −45.41 | |||||
| G | −0.68 ± 4.90 | −54.31 | |||||
| ΔC–B | C | −2.62 ± 3.62 | −59.64 | 2.290 | 0.107 | 0.046 | |
| M | −3.82 ± 3.30 | −59.32 | |||||
| G | −4.43 ± 3.56 | −65.63 | |||||
| ΔF–I | C | −1.76 ± 4.67 | −29.71 | 0.143 | 0.867 | 0.003 | |
| M | −2.15 ± 5.17 | −32.63 | |||||
| G | −2.39 ± 4.69 | −31.87 | |||||
| ΔV–A | C | 0.27 ± 5.31 | 1.76 | 1.491 | 0.230 | 0.030 | |
| M | 1.82 ± 4.88 | 13.80 | |||||
| G | 2.32 ± 5.03 | 18.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.-P.; Chen, H.-T.; Chao, P.-H.; Yin, J.; Tsai, M.-J. The Role of Social Context in Physiological and Psychological Restoration in a Forest: Case Study of a Guided Forest Therapy Program in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 10076. https://doi.org/10.3390/ijerph181910076
Yu C-P, Chen H-T, Chao P-H, Yin J, Tsai M-J. The Role of Social Context in Physiological and Psychological Restoration in a Forest: Case Study of a Guided Forest Therapy Program in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(19):10076. https://doi.org/10.3390/ijerph181910076
Chicago/Turabian StyleYu, Chia-Pin, Heng-Ting Chen, Pei-Hua Chao, Jie Yin, and Ming-Jer Tsai. 2021. "The Role of Social Context in Physiological and Psychological Restoration in a Forest: Case Study of a Guided Forest Therapy Program in Taiwan" International Journal of Environmental Research and Public Health 18, no. 19: 10076. https://doi.org/10.3390/ijerph181910076
APA StyleYu, C.-P., Chen, H.-T., Chao, P.-H., Yin, J., & Tsai, M.-J. (2021). The Role of Social Context in Physiological and Psychological Restoration in a Forest: Case Study of a Guided Forest Therapy Program in Taiwan. International Journal of Environmental Research and Public Health, 18(19), 10076. https://doi.org/10.3390/ijerph181910076