
Evidence-Based Status of Forest Healing Program in South Korea




Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Methods
2.2. Effectiveness of Forest Healing Program through SR and Meta-Analyses
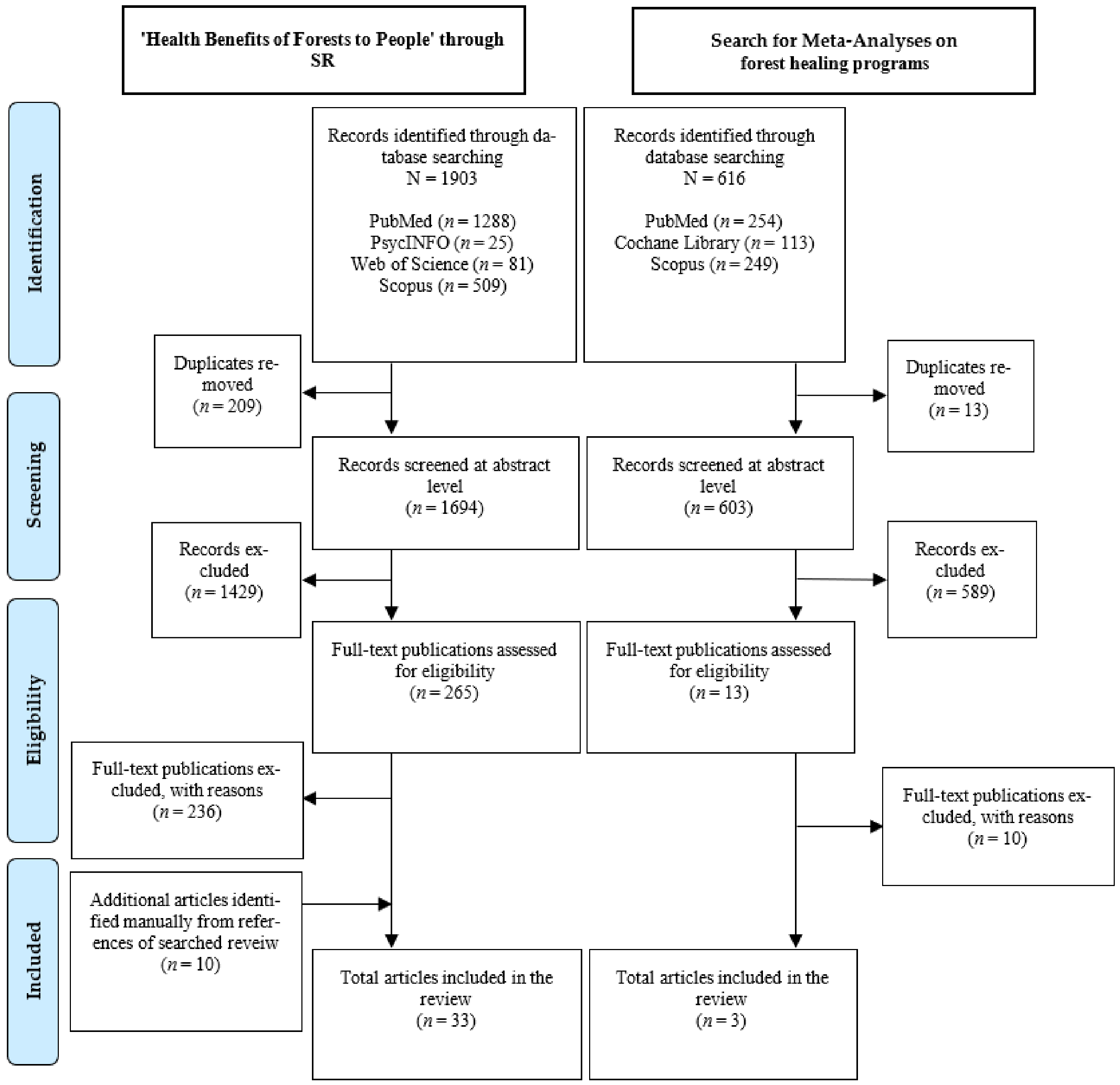
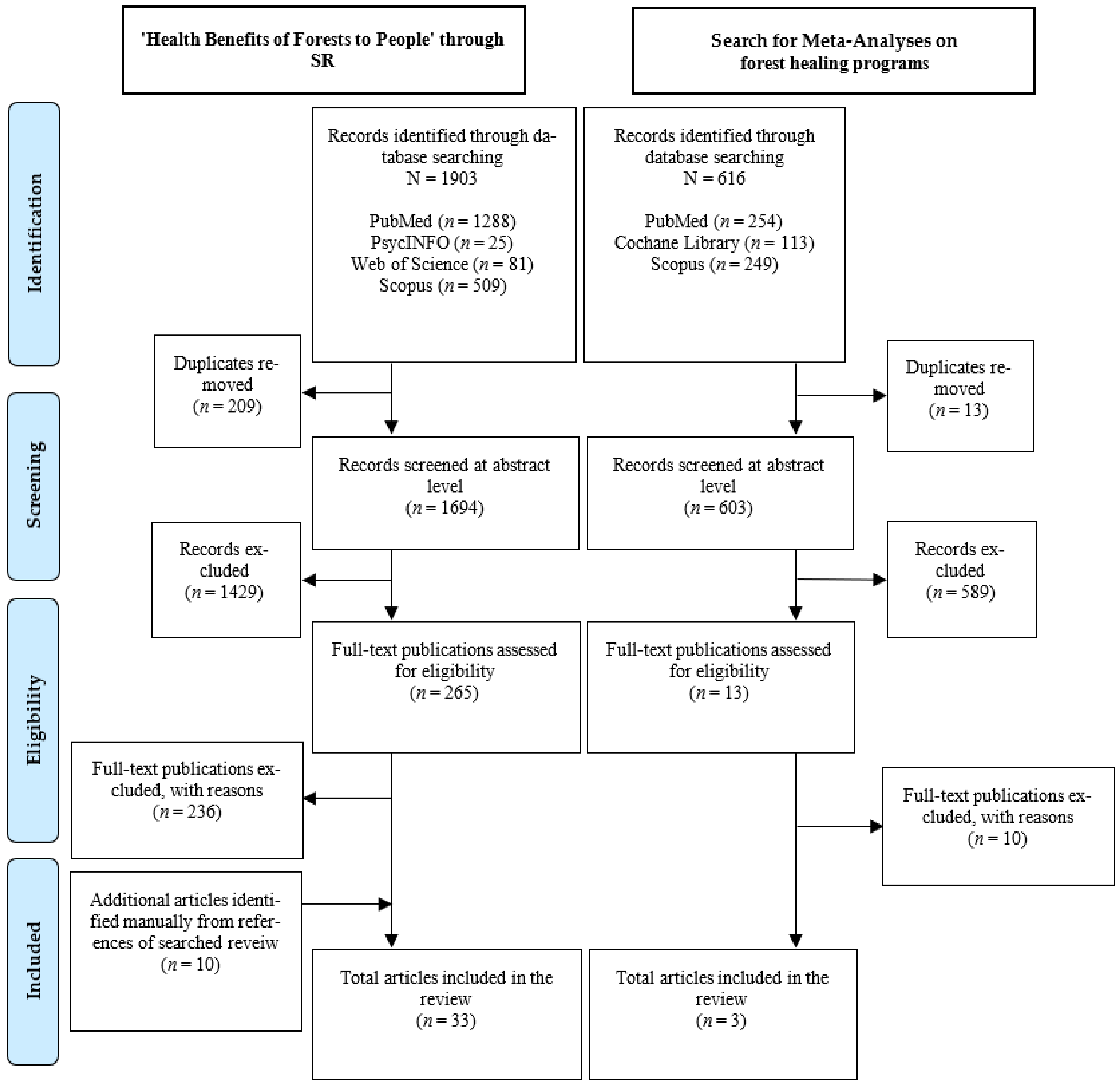
2.2.1. ‘Health Benefits of Forests to People’ through SR
2.2.2. Search for Meta-Analyses on Forest Healing Programs
3. Results
3.1. Classification of Forest Healing Program
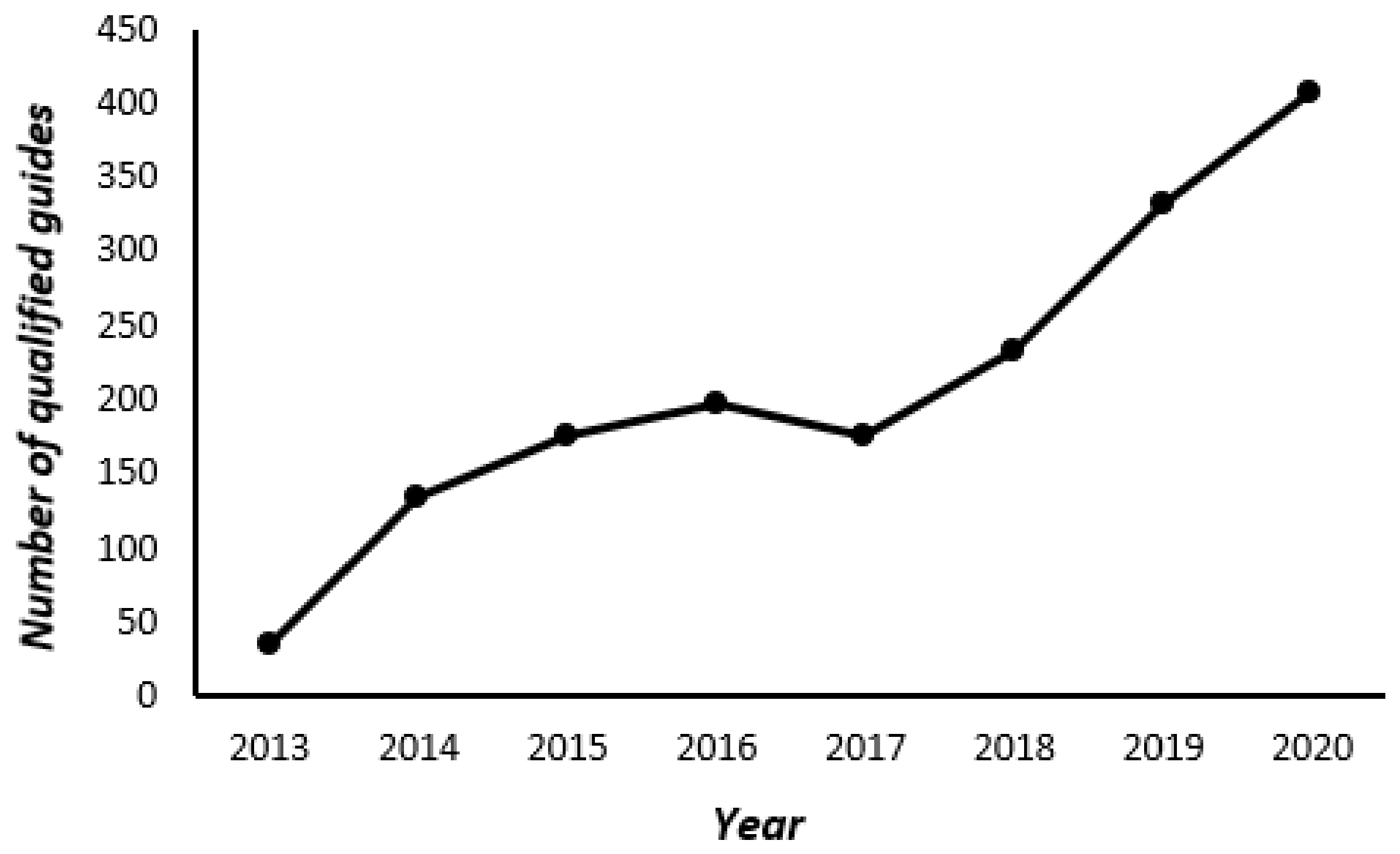
3.1.1. Target Groups for Forest Healing Program Development
3.1.2. Healing Factors and Activity Evaluation
3.1.3. Season and Training Time
3.1.4. Location for Forest Healing Programs, Type of Activities, Number of Educations, Participation Fee
3.2. Effects of Forest Healing Program
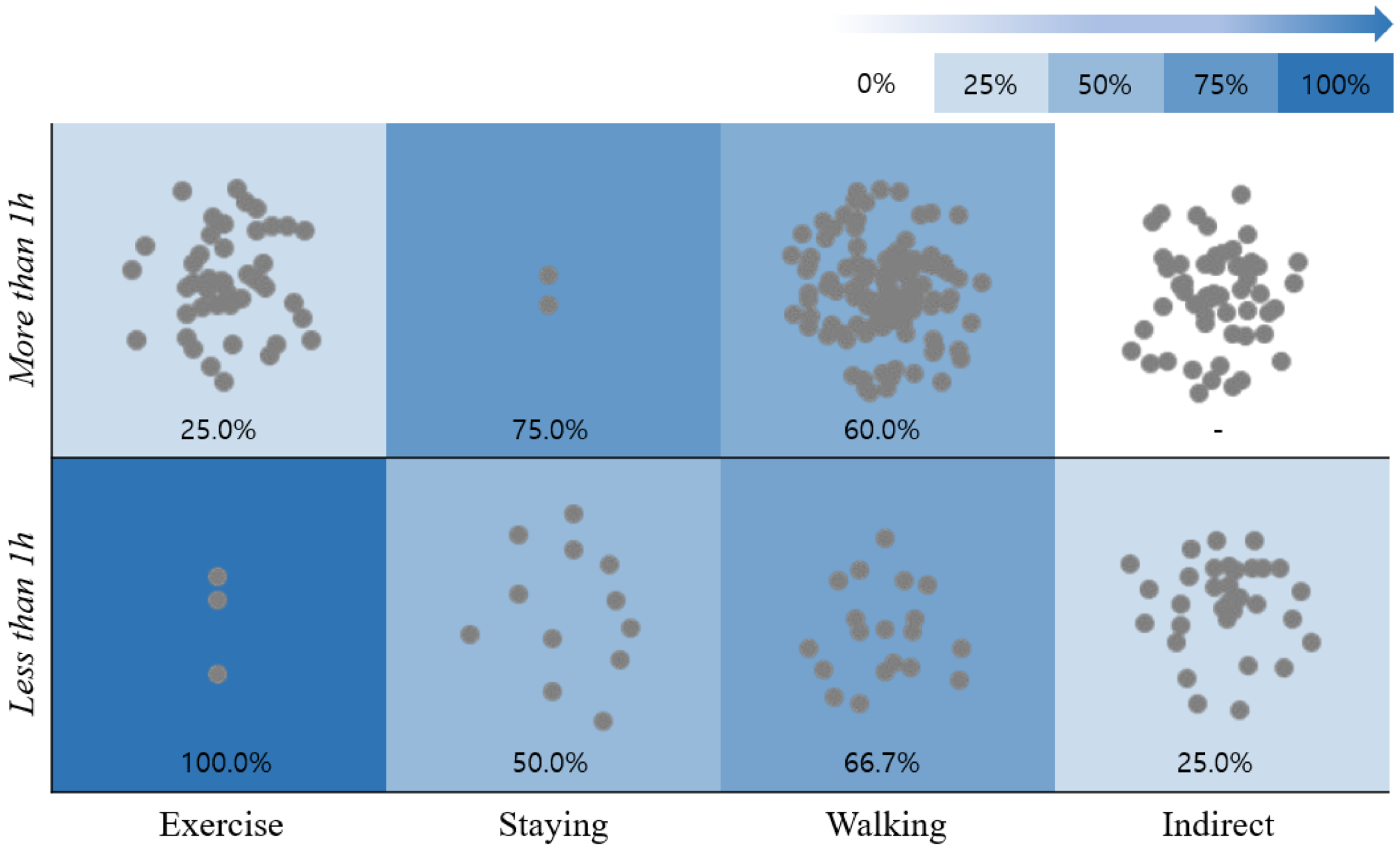
3.2.1. Effectiveness of forest healing programs on Activities and Time
3.2.2. Evidence for Effectiveness of Forest Healing Programs
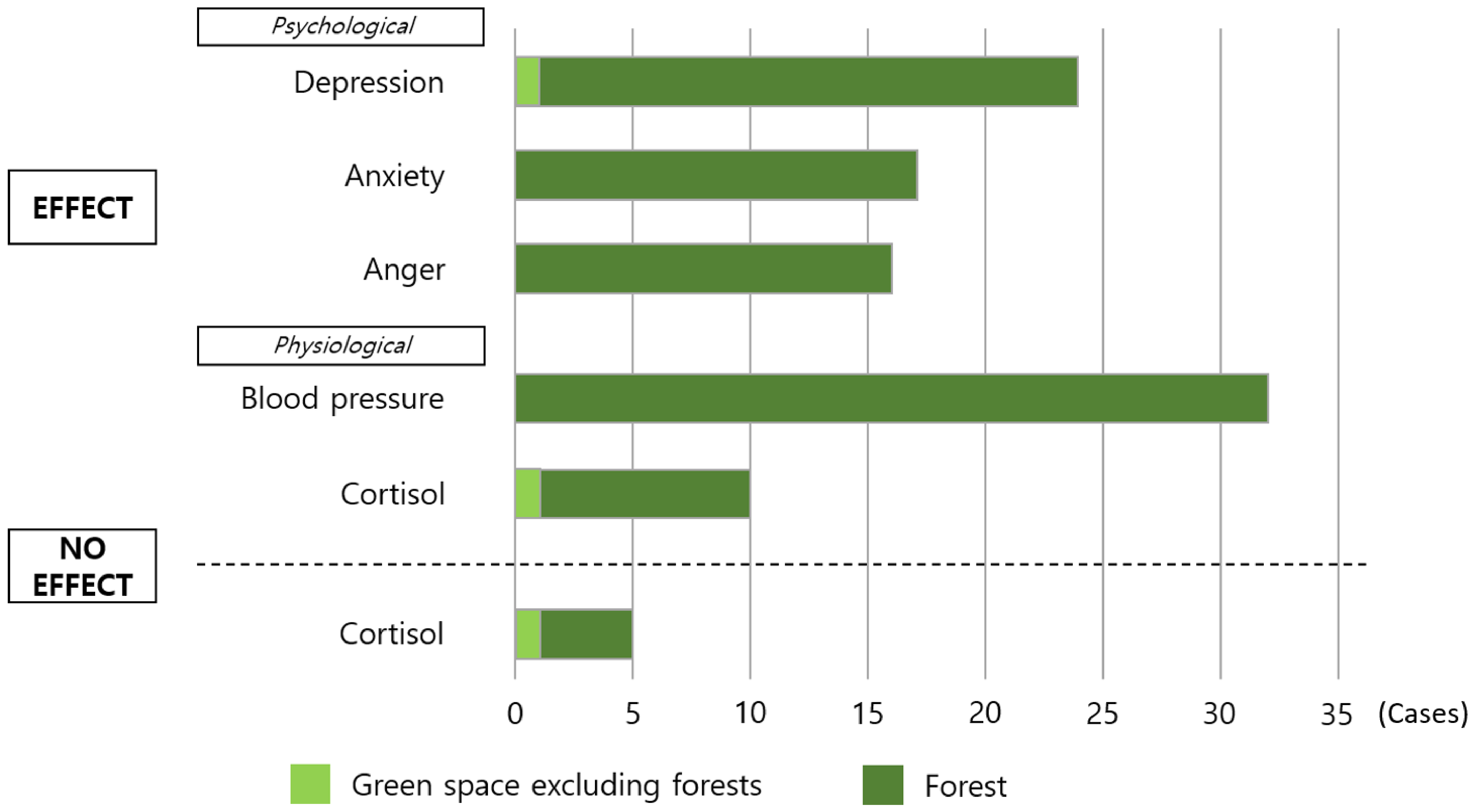
3.2.3. Psychological and Physiological Effects of Forest Healing Programs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Korea Legislation Research Institute. Forestry Culture and Recreation act of Republic of Korea. 2018. Available online: https://elaw.klri.re.kr/kor_service/lawView.do?hseq=46871&lang=ENG (accessed on 31 March 2021).
- Kim, M. A Forest that Gives Generously, the Public Value of our Forest 221 Trillion Won. In Korea Forest Service. 2020. Available online: https://huyang.forest.go.kr/kfsweb/cop/bbs/selectBoardArticle.do?nttId=3143940&bbsId=BBSMSTR_1036&pageUnit=10&pageIndex=11&searchtitle=title&searchcont=&searchkey=&searchwriter=&searchWrd=&ctgryLrcls=CTGRY150&ctgryMdcls=&ctgrySmcls=&ntcStartDt=&ntcEndDt=&mn=UKFR_03_03&orgId=kfri (accessed on 31 March 2021).
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments—An intervention study. Urban For. Urban Green. 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Park, B.-J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of shinrin-yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Sonntag-Öström, E.; Stenlund, T.; Nordin, M.; Lundell, Y.; Ahlgren, C.; Fjellman-Wiklund, A.; Järvholm, L.S.; Dolling, A. “Nature’s effect on my mind”–Patients’ qualitative experiences of a forest-based rehabilitation programme. Urban For. Urban Green. 2015, 14, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Jing, Y.A.N. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, M.H.; Chang, M.C.; Lee, S.-J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.Y.; Kawada, T. Effect of Forest Environments on Psychological Response Evaluated by the Poms Test; Nova Science Publisher: New York, NY, USA, 2013; pp. 137–146. [Google Scholar]
- Tsunetsugu, Y.; Park, B.-J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S.; Kim, J.J. The influence of interaction with forest on cognitive function. Scand. J. For. Res. 2011, 26, 595–598. [Google Scholar] [CrossRef]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [Green Version]
- Choe, G.-H.; An, D.-S. A Study on the Analysis of Forest Healing Effects-Focusing on the Elderly. Master’s Thesis, Chonbuk National University Graduate School, Jeollabuk-do, Korea, 2013. [Google Scholar]
- Choe, G.-H.; An, D.-S. The Effect of Forest Healing Programs in Urban Forests on the Resilience of the Elderly. Master’s Thesis, Chungbuk National University, Chungju City, Korea, 2019. Unpublished. [Google Scholar]
- Kim, I.D.; Koo, C.D. A study on the effects of walking, scenery appreciation, and forest healing programs using scent on the prevention of dementia in the elderly living alone. Korean J. Environ. Ecol. 2019, 33, 107–115. [Google Scholar] [CrossRef]
- Choi, J.; Kim, H. The effect of 12-week forest walking on functional fitness and body image in the elderly women. J. Korean Inst. For. Recreat. 2017, 21, 47–56. [Google Scholar] [CrossRef]
- Furuyashiki, A.; Tabuchi, K.; Norikoshi, K.; Kobayashi, T.; Oriyama, S. A comparative study of the physiological and psychological effects of forest bathing (Shinrin-yoku) on working age people with and without depressive tendencies. Environ. Health Prev. Med. 2019, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsunetsugu, Y.; Park, B.-J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Psychological relaxation effect of forest therapy: Results of field experiments in 19 forests in Japan involving 228 participants. Jpn. J. Hyg. 2011, 66, 670–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, G.-X.; Cao, Y.-B.; Lan, X.-G.; He, Z.-H.; Chen, Z.-M.; Wang, Y.-Z.; Hu, X.-L.; Lv, Y.-D.; Wang, G.-F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.-P.S.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Aziz, N.A.A. Developing an effective forest therapy program to manage academic stress in conservative societies: A multi-disciplinary approach. Urban For. Urban Green. 2019, 43, 126353. [Google Scholar] [CrossRef]
- Lyu, B.; Zeng, C.; Xie, S.; Li, D.; Lin, W.; Li, N.; Jiang, M.; Liu, S.; Chen, Q. Benefits of a three-day bamboo forest therapy session on the psychophysiology and immune system responses of male college students. Int. J. Environ. Res. Public Health 2019, 16, 4991. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary approach. Tour. Manag. 2017, 62, 322–334. [Google Scholar] [CrossRef]
- Yoo, S. Forestry Statistical Yearbook. In Korea Forest Service: Korea Forest Service Administrative Information; Korea Forest Service: Seo-gu, Daejeon, Korea, 2020; Volume 50. [Google Scholar]
- Korea Forest Service. Available online: https://www.forest.go.kr/kfsweb/kfs/idx/Index.do (accessed on 31 March 2021).
- Kim, G.W. A study on conceptual method for forest trail planning. J. Korean Inst. Forest Recreat. 2009, 13, 11–24. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kang, E.N. A Study on the effects of health promotion of the elderly employment promotion projects for the elderly: By using propensity score matching. Korean J. Local Gov. Adm. Stud. 2011, 25, 419–435. [Google Scholar]
- Lee, E.T.; Park, S.J.; Yu, R.H.; Hong, S.J. Analysis on the activity contents of forest healing programs in Korea. J. Korean Inst. Forest Recreat. 2011, 15, 101–109. [Google Scholar]
- Kim, Y.H.; Jeong, D.W.; Park, B.J. A study on analyze contents of forest based therapeutic programs in Korea. J. Korean Inst. Forest Recreat. 2019, 23, 43–58. [Google Scholar]
- Hong, J.Y.; Lee, J.H. Analysis on activities of forest healing program in healing forests. J. Korean Inst. Forest Recreat. 2018, 22, 1–9. [Google Scholar] [CrossRef]
- Mygind, L.; Kjeldsted, E.; Hartmeyer, R.D.; Mygind, E.; Bølling, M.; Bentsen, P. Immersive nature-experiences as health promotion interventions for healthy, vulnerable, and sick populations? A systematic review and appraisal of controlled studies. Front. Psychol. 2019, 10, 943. [Google Scholar] [CrossRef]
- Pless, I.B.; Douglas, J.W.B. Chronic illness in childhood: Part I. Epidemiological and clinical characteristics. Pediatrics 1971, 47, 405–414. [Google Scholar] [PubMed]
- Jo, Y.M. A Meta-Analysis on Effects of Forest Therapy Program. Ph.D. Thesis, Chungbuk National University, Chungju City, Korea, 2019. Unpublished. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Korea Forest Service | Ministry of Gender Equality and Family | Ministry of Environment |
|---|---|---|---|
| Certification System | Forest Education Program | Adolescent Training Activity | Selection of Outstanding Environmental Education Program |
| Purpose | Providing opportunities to understand the necessity and role of forests and the value of forest environment system. | Providing superior programs to help adolescents to participate by choosing beneficial and safe activities | Providing the environmental education programs that are eco-friendly, high-quality, and safe |
| Criteria | Total 5 index, 9 items Education program: Composition, Management, Evaluation, Faculty members, Education environment (place and equipment, safety control, hygienics), Activity records, Accommodations | Common Criteria, 6 items Individual Criteria: 3 items with accommodation, 5 without accommodation. Special Criteria: 2 items for high risk, 1 for accommodation as groups, and 3 for non-face-to-face (real-time, contents, task performance) | Total 3 index, 5 items Program (quality, management, evaluation), instructors (certification and arrangement), education activity environment (safety control) |
| Process | Documentation review Field survey and evaluation report of consulting examination of item and review Consideration and decision Issue of certification | Verification consulting Applying for verification Verification examination Consideration to verify Issue of verification | Pre-consulting (optional) Appointed application Appointed examination Appointed consideration Selection as outstanding program |
| Classification Criteria | Classification | Detailed Items |
|---|---|---|
| Participants | Disease State | Normal, Chronic, Addictive, Environmental |
| Target Group | Infant, Adolescent, Aged, Pregnant, Health-Impaired | |
| The Six Methods | Plant Therapy, Water Therapy, Diet, Psychotherapy, Climate Therapy, Exercise | |
| Season | four seasons, Spring, Summer, Fall, Winter | |
| Sensory Activities | Visual, Olfactory, Auditory, Tactile, Palate | |
| Activities | Dynamic activities, Static activities, Both | |
| Locations | Indoor, Indoor/Outdoor, Outdoor |
| Keywords | ‘Health Benefits of Forests to People’ through SR | Search for Meta-Analyses on Forest Healing Programs |
|---|---|---|
| P | (people OR volunteers OR participants OR subjects OR individuals) | (people OR infant OR adolescent OR adult OR elderly OR pregnant women OR disabled) |
| I | (“natural environment” OR “green space” OR “nature space” OR “green nature” OR “forest”) | (“green space” OR “forest”) |
| AND | AND | |
| (intervention OR program OR programme OR exposure OR therapy OR recreation OR “physical activity” OR exercise OR activities OR walking OR meditation OR staying) | (healing OR therapy OR program) | |
| C | - | |
| O | “health” OR “well being” OR “well-being” OR “health promotion” OR “physiological” OR “psychological” OR “mental health” OR “physical health” OR therapeutic | |
| S | “randomized controlled” OR “RCT” | “meta” |
| Section | Subsection | Participation Frequency | Rate (%) |
|---|---|---|---|
| Disease State | Normal | 68 | 90.67 |
| Chronic disease | 2 | 2.67 | |
| Addictive disease | 3 | 4.00 | |
| Environmental disease | 2 | 2.67 | |
| Target Group | Infant | 5 | 6.67% |
| Adolescent | 41 | 54.67% | |
| Adult | 15 | 20.00% | |
| Elderly | 3 | 4.00% | |
| Pregnant women | 1 | 1.33% | |
| Disabled | 3 | 4.00% |
| Categories | Detailed Contents | Frequency (Cnt.) | Ratio (%) | ||
|---|---|---|---|---|---|
| Therapeutic approach | Plant therapy | 188 | 67.63 | ||
| Water therapy | 16 | 5.76 | |||
| Dietary therapy | 2 | 0.72 | |||
| Psychotherapy | 35 | 12.59 | |||
| Climate therapy | 6 | 2.16 | |||
| Exercise | 31 | 11.15 | |||
| Total | 278 | 100.00 | |||
| Sense activities | Visual | 36 | 11.96 | ||
| Olfactory | 74 | 24.58 | |||
| Auditory | 52 | 17.28 | |||
| Tactile | 103 | 34.22 | |||
| Palate | 36 | 11.96 | |||
| Total | 301 | 100.00 | |||
| Type of physical activity | Static activities | 75 | 27.99 | ||
| Dynamic activities | 160 | 59.70 | |||
| Dynamic–Static activities | 33 | 12.31 | |||
| Total | 268 | 100.00 | |||
| Season | Spring | 72 | 96.00 | ||
| Summer | 75 | 100.00 | |||
| Fall | 72 | 96.00 | |||
| Winter | 27 | 36.00 | |||
| Session duration | >60 min | 69 | 25.75 | ||
| <60 min | 199 | 74.25 | |||
| Total | 268 | 100.00 | |||
| Venue | outdoor | 153 | 57.09 | ||
| indoor | 81 | 30.22 | |||
| Outdoor–indoor | 34 | 12.69 | |||
| Total | 268 | 100.00 | |||
| Type of visit | One day visit | 35 | 46.67 | ||
| Days and nights visit | 2 days/1 night | 26 | 34.67 | ||
| 3 days/2 nights | 9 | 12.00 | |||
| Regular visit | 5 | 6.67 | |||
| Total | 75 | 100.00 | |||
| Activities | Mental Health | Physical Health | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | +/ | / | - | % p | % p + m | + | +/ | / | - | % p | % p + m | |
| Staying | ||||||||||||
| <1 h | 6 | 3 | 2 | - | 54.5% | 81.8% | - | 1 | 1 | - | 0.0% | 50.0% |
| >1 h | 3 | 1 | 8 | - | 25.0% | 33.3% | 3 | - | 1 | - | 75.0% | 75.0% |
| Walking | ||||||||||||
| <1 h | 23 | 5 | 5 | 2 | 65.7% | 80.0% | 5 | 3 | 4 | 41.7% | 66.7% | |
| >1 h | 5 | 5 | 1 | - | 45.5% | 90.9% | 27 | - | 18 | - | 60.0% | 60.0% |
| Exercise | ||||||||||||
| <1 h | 2 | 2 | 3 | - | 28.6% | 57.1% | - | 1 | - | - | 0.0% | 100.0% |
| >1 h | - | 2 | 4 | - | 0.0% | 33.3% | - | 1 | 2 | 1 | 0.0% | 25.0% |
| Indirect | ||||||||||||
| <1 h | 3 | 2 | 8 | 1 | 21.4% | 35.7% | 1 | - | 3 | - | 25.0% | 25.0% |
| >1 h | - | - | - | - | - | - | - | - | - | - | - | - |
| Categories | Detailed Contents | Frequency (Cnt.) | Ratio (%) |
|---|---|---|---|
| Activities | Staying | 24 | 8.96 |
| Walking | 124 | 46.27 | |
| Exercise | 41 | 15.30 | |
| Indirect (natural materials, audiovisual materials) | 79 | 29.48 | |
| Total | 268 | 100.00 |
| Activities | Numbers of References | ||
|---|---|---|---|
| Effect | No Effect | ||
| Staying | 31 (10.44%) | 27 | - |
| Walking | 132 (44.44%) | 31 | 5 |
| Exercise | 48 (16.16%) | 1 | - |
| Indirect | 86 (28.96%) | 4 | - |
| Total | 297 (100%) | 63 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Kim, S.; Kim, G.; Choi, Y.; Kim, E.; Paek, D. Evidence-Based Status of Forest Healing Program in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 10368. https://doi.org/10.3390/ijerph181910368
Park S, Kim S, Kim G, Choi Y, Kim E, Paek D. Evidence-Based Status of Forest Healing Program in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(19):10368. https://doi.org/10.3390/ijerph181910368
Chicago/Turabian StylePark, Sujin, Soojin Kim, Geonwoo Kim, Yeji Choi, Eunsoo Kim, and Domyung Paek. 2021. "Evidence-Based Status of Forest Healing Program in South Korea" International Journal of Environmental Research and Public Health 18, no. 19: 10368. https://doi.org/10.3390/ijerph181910368
APA StylePark, S., Kim, S., Kim, G., Choi, Y., Kim, E., & Paek, D. (2021). Evidence-Based Status of Forest Healing Program in South Korea. International Journal of Environmental Research and Public Health, 18(19), 10368. https://doi.org/10.3390/ijerph181910368