
Air Pollutant Particles, PM2.5, Exposure and Glaucoma in Patients with Diabetes: A National Population-Based Nested Case–Control Study

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Comorbidities
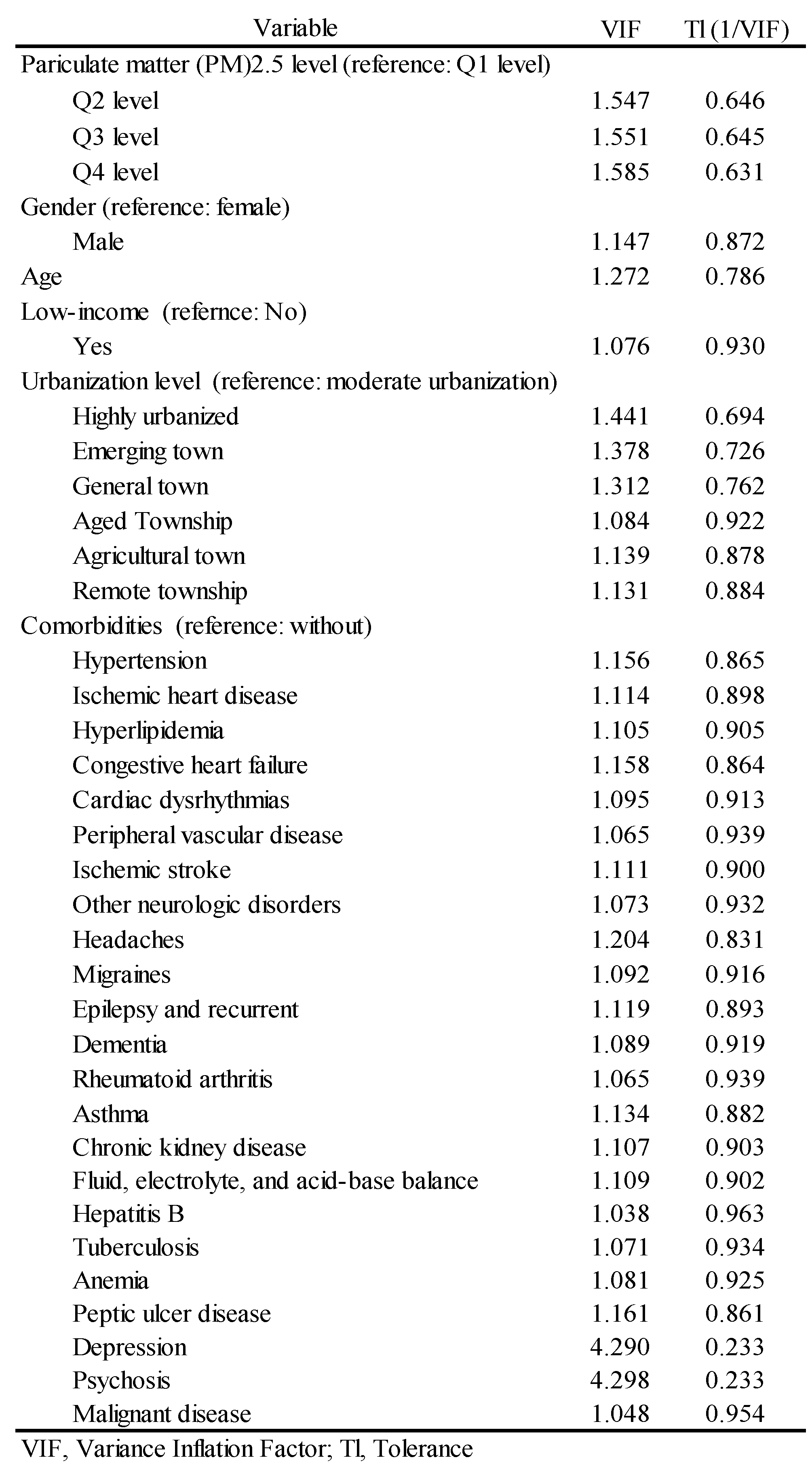
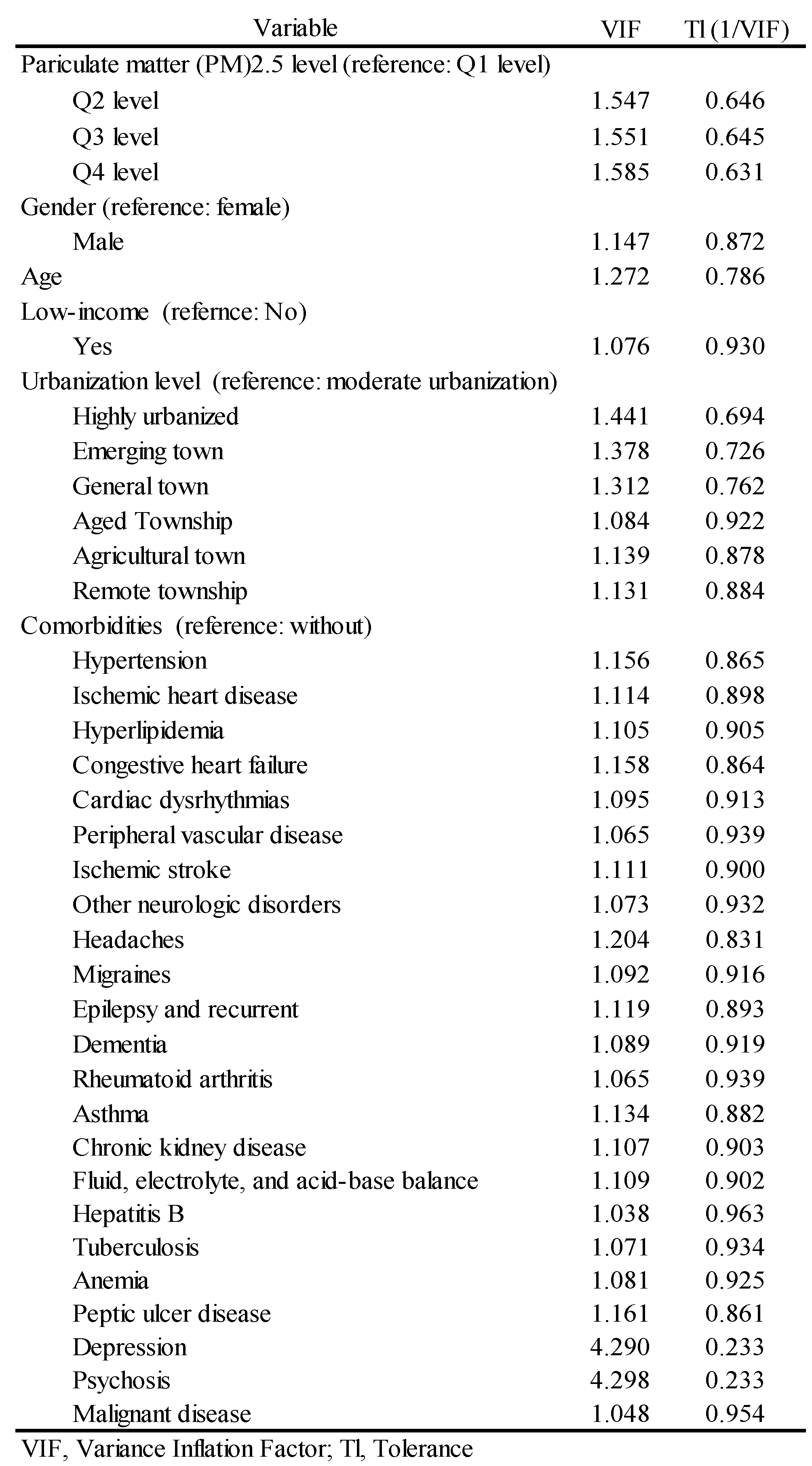
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
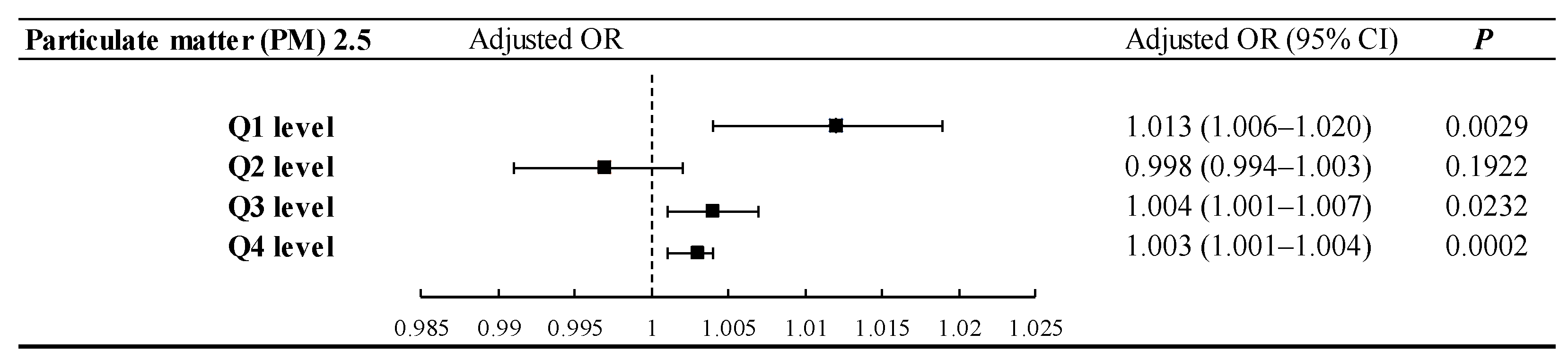
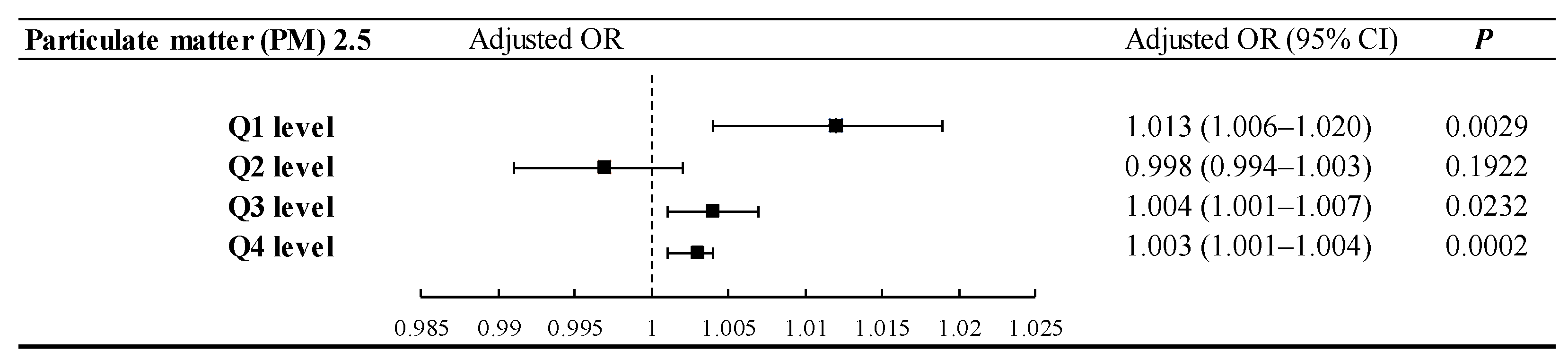
3.2. PM2.5 Exposure Level and Glaucoma Risk
3.3. Independent Risk Factors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pradeepa, R.; Mohan, V. Prevalence of type 2 diabetes and its complications in India and economic costs to the nation. Eur. J. Clin. Nutr. 2017, 71, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balakumar, P.; Maung, U.K.; Jagadeesh, G. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharmacol. Res. 2016, 113, 600–609. [Google Scholar] [CrossRef]
- Zhao, Y.X.; Chen, X.W. Diabetes and risk of glaucoma: Systematic review and a Meta-analysis of prospective cohort studies. Int. J. Ophthalmol. 2017, 10, 1430–1435. [Google Scholar] [PubMed]
- Danylkova, N.O.; Pomeranz, H.D.; Alcala, S.R.; McLoon, L.K. Histological and morphometric evaluation of transient retinal and optic nerve ischemia in rat. Brain Res. 2006, 1096, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Tezel, G.; Wax, M.B. Hypoxia-inducible factor 1alpha in the glaucomatous retina and optic nerve head. Arch. Ophthalmol. 2004, 122, 1348–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, N.; Nakanishi-Toda, M. Nitric oxide: Ocular blood flow, glaucoma, and diabetic retinopathy. Prog. Retin. Eye Res. 2007, 26, 205–238. [Google Scholar] [CrossRef]
- Myers, J.S.; Fudemberg, S.J.; Lee, D. Evolution of optic nerve photography for glaucoma screening: A review. Clin. Exp. Ophthalmol. 2018, 46, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortune, B. Optical coherence tomography evaluation of the optic nerve head neuro-retinal rim in glaucoma. Clin. Exp. Optom. 2019, 102, 286–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanito, M.; Sugihara, K.; Hara, K.; Takai, Y. Different glaucoma types and glaucoma surgeries among different age groups. Graefes. Arch. Clin. Exp. Ophthalmol. 2018, 256, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.Y.L.; Khawaja, A.P.; Morgan, J.; Strouthidis, N.; Reisman, C.; Dick, A.D.; Khaw, P.T.; Patel, P.J.; Foster, P.J. The Relationship Between Ambient Atmospheric Fine Particulate Matter (PM2.5) and Glaucoma in a Large Community Cohort. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4915–4923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; He, M.; Li, Z.; Huang, W. Epidemiological variations and trends in health burden of glaucoma worldwide. Acta Ophthalmol. 2019, 97, e349–e355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, R.; Emslie-Smith, A.M.; Gardner, I.D.; Morris, A.D. ABC of arterial and venous disease: Vascular complications of diabetes. BMJ 2000, 320, 1062–1066. [Google Scholar] [CrossRef] [PubMed]
- Sjølie, A.K.; Stephenson, J.; Aldington, S.; Kohner, E.; Janka, H.; Stevens, L.; Fuller, J. Retinopathy and vision loss in insulin-dependent diabetes in Europe: The EURODIAB IDDM Complications Study. Ophthalmology 1997, 104, 252–260. [Google Scholar] [CrossRef]
- Perneger, T.V.; Brancati, F.L.; Whelton, P.K.; Klag, M.J. End-stage renal disease attributable to diabetes mellitus. Ann. Intern. Med. 1994, 121, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Li, C.Y.; Wu, C.D.; Pan, W.C.; Chen, Y.C.; Su, H.J. Association Between Long-Term Exposure to PM2.5 and Incidence of Type 2 Diabetes in Taiwan: A National Retrospective Cohort Study. Epidemiology 2019, 30 (Suppl. 1), S67–S75. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.Y.; Luo, C.W.; Chiang, Y.W.; Yeh, K.L.; Li, Y.C.; Ho, Y.C.; Lee, S.S.; Chen, W.Y.; Chen, C.J.; Kuan, Y.H. Association Between PM2.5 Exposure Level and Primary Open-Angle Glaucoma in Taiwanese Adults: A Nested Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 1714. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Hernandez, A.M.; Ruiz de Porras, G.D.; Marko, D.; Whitworth, K.W. The Association Between PM2.5 and Ozone and the Prevalence of Diabetes Mellitus in the United States, 2002 to 2008. J. Occup. Environ. Med. 2018, 60, 594–602. [Google Scholar] [CrossRef]
- Taiwan Air Quality Monitoring Network. TAQMN Site. 2019. Available online: http://taqm.epa.gov.tw/taqm/en/b0101.aspx (accessed on 11 August 2019).
- Li, R.L.; Ho, Y.C.; Luo, C.W.; Lee, S.S.; Kuan, Y.H. Influence of PM2.5 Exposure Level on the Association between Alzheimer’s Disease and Allergic Rhinitis: A National Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 3357. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.C.; Chien, C.W.; Hu, C.C.; Ho, J.D. Comparison of comorbid conditions between open-angle glaucoma patients and a control cohort: A case-control study. Ophthalmology 2010, 117, 2088–2095. [Google Scholar] [CrossRef]
- Chen, H.Y.; Lin, C.L. Comparison of medical comorbidity between patients with primary angle-closure glaucoma and a control cohort: A population-based study from Taiwan. BMJ Open 2019, 9, e024209. [Google Scholar] [CrossRef] [Green Version]
- Vélez-Gómez, M.C.; Vásquez-Trespalacios, E.M. Adherence to topical treatment of glaucoma, risk and protective factors: A review. Arch. Soc. Esp. Oftalmol. 2018, 93, 87–92. [Google Scholar] [CrossRef]
- Lee, C.T.; Hsiao, C.Y.; Lee, J.F.; Chen, Y.C.; Nfor, O.N.; Huang, J.Y.; Wang, L.; Ho, C.C.; Liaw, Y.P. Relationship between Schizophrenia and Low-Income Based on Age and Sex: Results from a Nation-wide Population-Based Longitudinal Study. Neuropsychiatry 2018, 8, 1000–1006. [Google Scholar]
- Lin, Y.J.; Tian, W.H.; Chen, C.C. Urbanization and the utilization of outpatient services under National Health Insurance in Taiwan. Health Policy 2011, 103, 236–343. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Ezzati, M.; Dockery, D.W. Fine particulate air pollution and life expectancies in the United States: The role of influential observations. J. Air Waste Manag. Assoc. 2014, 63, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weichenthal, S.; Villeneuve, P.J.; Burnett, R.T.; van Donkelaar, A.; Martin, R.V.; Jones, R.R.; DellaValle, C.T.; Sandler, D.P.; Ward, M.H.; Hoppin, J.A. Long-term exposure to fine particulate matter: Association with nonaccidental and cardiovascular mortalityin the Agricultural Health Study Cohort. Environ. Health Perspect. 2014, 112, 609–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanobetti, A.; Dominici, F.; Wang, Y.; Schwartz, J.D. A national case-crossover analysis of the short-time effect of PM2.5 on hospitalizations and mortality in subjects with diabetes and neurological disorders. Environ. Health 2014, 13, 2778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.W.; Wang, W.; Huang, W.B.; Zhang, X.L. Diabetes Mellitus as a Risk Factor for Open-Angle Glaucoma: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e102972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, A.M.; Datta, M.; Kumpatla, S.; Selvaraj, P.; Viswanthan, V. Prevalence of Diabetes Mellitus and Exposure to Suspended Particulate Matter. J. Health Pollut. 2019, 9, 190608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, C.; Sengupta, S.; Banerjee, S.; Choudhury, S. Angle closure glaucoma in rural and urban populations in eastern India—The Hooghly River Glaucoma Study. Indian J. Ophthalmol. 2018, 66, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.J.; Lu, P.; Zhang, W.F.; Lu, J.H. High myopia as a risk factor in primary open angle glaucoma. Int. J. Ophthalmol. 2012, 5, 750–753. [Google Scholar] [PubMed]
- Bialasiewicz, A.A. Genetics of myopia. Oman J. Ophthalmol. 2011, 4, 49. [Google Scholar] [CrossRef] [PubMed]
- Hornbeak, D.M.; Young, T.L. Myopia genetics: A review of current research and emerging trends. Curr. Opin. Ophthalmol. 2009, 20, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, W.; Shimada, N.; Hayashi, K.; Moriyama, M.; Yoshida, T.; Tokoro, T.; Ohno-Matsui, K. Retinal vessels and high myopia. Ophthalmology 2011, 118, 791–791.e2. [Google Scholar] [CrossRef] [PubMed]
- Ip, J.M.; Rose, K.A.; Morgan, I.G.; Burlutsky, G.; Mitchell, P. Myopia and the urban environment: Findings in a sample of 12-year-old Australian school children. Invest. Ophthalmol. Vis. Sci. 2008, 49, 3858–3863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, H.D.; Chinh, D.D.; Tan, P.V.; Duong, N.V.; Anh, N.Q.; Le, N.H.; Tuan, H.X.; Anh, N.T.; Duong, N.T.T.; Kien, V.D. The Prevalence of Myopia and Factors Associated with it among Secondary School Children in Rural Vietnam. Clin. Ophthalmol. 2020, 14, 1079–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.Y.; Lo, C.T.; Sheu, S.J.; Yin, L.T. Risk factors for and progression of myopia in young Taiwanese men. Ophthalmic. Epidemiol. 2015, 22, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Gramer, G.; Weber, B.H.; Gramer, E. Migraine and vasospasm in glaucoma: Age-related evaluation of 2027 patients with glaucoma or ocular hypertension. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7999–8007. [Google Scholar] [CrossRef] [Green Version]
- Flammer, J.; Orgul, S.; Costa, V.P.; Orzalesi, N.; Krieglstein, G.K.; Serra, L.M.; Renard, J.P.; Stefánsson, E. The impact of ocular blood flow in glaucoma. Prog. Retin. Eye Res. 2002, 21, 359–393. [Google Scholar] [CrossRef]
- Plange, N.; Remky, A.; Arend, O. Colour Doppler imaging and fluorescein filling defects of the optic disc in normal tension glaucoma. Br. J. Ophthalmol. 2003, 87, 731–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. Pain 2013, 154, S44–S53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stovner, L.J.; Hagen, K.; Jensen, R.; Katsarava, Z.; Lipton, R.B.; Scher, A.I.; Steiner, T.J.; Zwart, J.A. The global burden of headache: A documentation of headache prevalence and disability worldwide. Cephalalgia 2007, 27, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Tsai, S.S.; Yang, C.Y. Association between Fine Particulate Air Pollution and Daily Clinic Visits for Migraine in a Subtropical City: Taipei, Taiwan. Int. J. Environ. Res. Public Health 2015, 12, 4697–4708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.Y.; Lin, C.L.; Kao, C.H. Does Migraine Increase the Risk of Glaucoma: A Population-Based Cohort Study. Medicine 2016, 95, e3670. [Google Scholar] [CrossRef]
- Xu, C.; Li, J.; Li, Z.; Mao, X. Migraine as a risk factor for primary open angle glaucoma: A systematic review and meta-analysis. Medicine 2018, 97, e11377. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Su, C.C.; Wang, T.H.; Tsai, I.J. Migraine and increased risk of developing open angle glaucoma: A population-based cohort study. BMC Ophthalmol. 2019, 19, 50. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Degoumois, A.; Miocque, S.; Denion, E. Central retinal artery occlusion without underlying chronic ocular ischemic syndrome may lead to neovascular glaucoma. J. Fr. Ophtalmol. 2017, 40, 758–762. [Google Scholar] [CrossRef]
- Naghavi, M.; Makela, S.; Foreman, K.; O’Brien, J.; Pourmalek, F.; Lozano, R. Algorithms for enhancing public health utility of national causes-of-death data. Popul. Health Metr. 2010, 10, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Control | Glaucoma | p-Value | |||
|---|---|---|---|---|---|
| (n = 788) | (n = 197) | ||||
| Gender | |||||
| Female | 384 | (48.73%) | 96 | (48.73%) | 1.0000 |
| Male | 404 | (51.27%) | 101 | (51.27%) | |
| Age | |||||
| Mean ± SD | 57.35 ± 10.42 | 57.29 ± 10.34 | 0.9628 | ||
| Low income | |||||
| Yes | 366 | (46.45%) | 103 | (52.28%) | 0.1423 |
| No | 422 | (53.55%) | 94 | (47.72%) | |
| Urbanization level | |||||
| Highly urbanized | 210 | (26.65%) | 68 | (34.52%) | 0.0066 |
| Moderate urbanization | 228 | (28.93%) | 65 | (32.99%) | |
| Emerging town | 169 | (21.45%) | 27 | (13.71%) | |
| General town | 106 | (13.45%) | 22 | (11.17%) | |
| Aged Township | 10 | (1.27%) | 5 | (2.54%) | |
| Agricultural town | 40 | (5.08%) | 2 | (1.02%) | |
| Remote township | 25 | (3.17%) | 8 | (4.06%) | |
| Comorbidities | |||||
| Hypertension | 500 | (63.45%) | 136 | (69.04%) | 0.1428 |
| Ischemic heart disease | 83 | (10.53%) | 20 | (10.15%) | 0.5154 |
| Hyperlipidemia | 456 | (57.87%) | 124 | (62.94%) | 0.1953 |
| Congestive heart failure | 38 | (4.82%) | 4 | (2.03%) | 0.0828 |
| Cardiac dysrhythmias | 63 | (7.99%) | 20 | (10.15%) | 0.3296 |
| Peripheral vascular disease | 19 | (2.41%) | 5 | (2.54%) | 0.9177 |
| Ischemic stroke | 13 | (1.65%) | 2 | (1.02%) | 0.8759 |
| Other neurologic disorders | 11 | (1.4%) | 5 | (2.54%) | 0.2567 |
| Headaches | 266 | (33.76%) | 72 | (36.55%) | 0.4604 |
| Migraines | 19 | (2.41%) | 10 | (5.08%) | 0.0478 |
| Epilepsy and recurrent | 11 | (1.4%) | 1 | (0.51%) | 0.3094 |
| Dementia | 16 | (2.03%) | 2 | (1.02%) | 0.3413 |
| Rheumatoid arthritis | 21 | (2.66%) | 4 | (2.03%) | 0.6125 |
| Asthma | 166 | (21.07%) | 31 | (15.74%) | 0.0944 |
| Chronic kidney disease | 28 | (3.55%) | 7 | (3.55%) | 1.0000 |
| Fluid, electrolyte, and acid-base balance | 16 | (2.03%) | 3 | (1.52%) | 0.6431 |
| Hepatitis B | 43 | (5.46%) | 7 | (3.55%) | 0.2763 |
| Tuberculosis | 21 | (2.66%) | 2 | (1.02%) | 0.1702 |
| Anemia | 57 | (7.23%) | 21 | (10.66%) | 0.1112 |
| Peptic ulcer disease | 256 | (32.49%) | 61 | (30.96%) | 0.6824 |
| Depression | 12 | (1.52%) | 4 | (2.03%) | 0.6142 |
| Psychosis | 16 | (2.03%) | 5 | (2.54%) | 0.6591 |
| Malignant disease | 102 | (12.94%) | 26 | (13.20%) | 0.9245 |
| Particulate matter (PM) 2.5 | |||||
| Q1 level (0–561.56 μg/m3) | 208 | (26.40%) | 39 | (19.80%) | 0.0686 |
| Q2 level (561.57–852.26 μg/m3) | 198 | (25.13%) | 46 | (23.35%) | |
| Q3 level ( 852.27–1284.69 μg/m3) | 198 | (25.13%) | 50 | (25.38%) | |
| Q4 level (1284.70–2727.44 μg/m3) | 184 | (23.35%) | 62 | (31.47%) | |
| Glaucoma | ||
|---|---|---|
| Adjusted OR (95%CI) | p | |
| Particulate matter (PM)2.5 level (reference: Q1 level) | ||
| Q2 level | 1.232 (0.757–2.004) | 0.4015 |
| Q3 level | 1.451 (0.895–2.352) | 0.1313 |
| Q4 level | 1.731 (1.084–2.764) | 0.0215 |
| Gender (reference: female) | ||
| Male | 0.835 (0.590–1.182) | 0.3097 |
| Age | 0.999 (0.981–1.016) | 0.8765 |
| Low-income (reference: No) | ||
| Yes | 1.294 (0.927–1.806) | 0.1299 |
| Urbanization level (reference: moderate urbanization) | ||
| Highly urbanized | 1.109 (0.742–1.659) | 0.6131 |
| Emerging town | 0.559 (0.337–0.929) | 0.0247 |
| General town | 0.791 (0.453–1.381) | 0.4104 |
| Aged Township | 1.795 (0.546–5.900) | 0.3353 |
| Agricultural town | 0.197 (0.046–0.853) | 0.0297 |
| Remote township | 1.138 (0.469–2.762) | 0.7755 |
| Comorbidities (reference: without) | ||
| Hypertension | 1.296 (0.898–1.872) | 0.1665 |
| Ischemic heart disease | 0.930 (0.534–1.619) | 0.7966 |
| Hyperlipidemia | 1.061 (0.750–1.500) | 0.7372 |
| Congestive heart failure | 0.415 (0.137–1.258) | 0.1200 |
| Cardiac dysrhythmias | 1.426 (0.803–2.531) | 0.2255 |
| Peripheral vascular disease | 1.130 (0.387–3.306) | 0.8228 |
| Ischemic stroke | 0.586 (0.120–2.855) | 0.5086 |
| Other neurologic disorders | 1.930 (0.614–6.068) | 0.2605 |
| Headaches | 1.232 (0.847–1.791) | 0.2760 |
| Migraines | 2.672 (1.127–6.335) | 0.0257 |
| Epilepsy and recurrent | 0.499 (0.058–4.271) | 0.5258 |
| Dementia | 0.530 (0.112–2.513) | 0.4238 |
| Rheumatoid arthritis | 0.770 (0.248–2.392) | 0.6518 |
| Asthma | 0.665 (0.418–1.056) | 0.0840 |
| Chronic kidney disease | 0.993 (0.397–2.487) | 0.9884 |
| Fluid, electrolyte, and acid-base balance | 0.719 (0.187–2.770) | 0.6321 |
| Hepatitis B | 0.716 (0.308–1.664) | 0.4378 |
| Tuberculosis | 0.407 (0.090–1.839) | 0.2425 |
| Anemia | 1.641 (0.933–2.887) | 0.0855 |
| Peptic ulcer disease | 0.879 (0.605–1.279) | 0.5015 |
| Depression | 2.403 (0.179–32.333) | 0.5086 |
| Psychosis | 0.629 (0.062–6.395) | 0.6955 |
| Malignant disease | 0.971 (0.597–1.580) | 0.9071 |
| Particulate Matter (PM)2.5 Level (Reference: Q1 Level) | p | ||||
|---|---|---|---|---|---|
| Q2 level | Q3 level | Q4 level | |||
| Urbanization level | |||||
| Emerging town groups | |||||
| Yes | (n = 196) | 1.289 (0.320–5.190) | 0.729 (0.168–3.166) | 0.439 (0.080–2.423) | 0.2572 |
| No | (n = 789) | 1.198 (0.695–2.066) | 1.491 (0.871–2.550) | 2.046 (1.229–3.406) | 0.0018 |
| Agricultural town groups | |||||
| Yes | (n = 42) | - | - | - | 0.9729 |
| No | (n = 943) | 1.254 (0.768–2.049) | 1.440 (0.883–2.349) | 1.749 (1.091–2.803) | 0.0117 |
| Comorbidities | |||||
| Migraines groups | |||||
| Yes | (n = 29) | - | - | - | 0.6125 |
| No | (n = 956) | 1.195 (0.721–1.979) | 1.465 (0.893–2.403) | 1.728 (1.074–2.782) | 0.0065 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, Y.-W.; Wu, S.-W.; Luo, C.-W.; Chen, S.-P.; Chen, C.-J.; Chen, W.-Y.; Chang, C.-C.; Chen, C.-M.; Kuan, Y.-H. Air Pollutant Particles, PM2.5, Exposure and Glaucoma in Patients with Diabetes: A National Population-Based Nested Case–Control Study. Int. J. Environ. Res. Public Health 2021, 18, 9939. https://doi.org/10.3390/ijerph18189939
Chiang Y-W, Wu S-W, Luo C-W, Chen S-P, Chen C-J, Chen W-Y, Chang C-C, Chen C-M, Kuan Y-H. Air Pollutant Particles, PM2.5, Exposure and Glaucoma in Patients with Diabetes: A National Population-Based Nested Case–Control Study. International Journal of Environmental Research and Public Health. 2021; 18(18):9939. https://doi.org/10.3390/ijerph18189939
Chicago/Turabian StyleChiang, Yun-Wei, Sheng-Wen Wu, Ci-Wen Luo, Shih-Pin Chen, Chun-Jung Chen, Wen-Ying Chen, Chia-Che Chang, Chuan-Mu Chen, and Yu-Hsiang Kuan. 2021. "Air Pollutant Particles, PM2.5, Exposure and Glaucoma in Patients with Diabetes: A National Population-Based Nested Case–Control Study" International Journal of Environmental Research and Public Health 18, no. 18: 9939. https://doi.org/10.3390/ijerph18189939
APA StyleChiang, Y.-W., Wu, S.-W., Luo, C.-W., Chen, S.-P., Chen, C.-J., Chen, W.-Y., Chang, C.-C., Chen, C.-M., & Kuan, Y.-H. (2021). Air Pollutant Particles, PM2.5, Exposure and Glaucoma in Patients with Diabetes: A National Population-Based Nested Case–Control Study. International Journal of Environmental Research and Public Health, 18(18), 9939. https://doi.org/10.3390/ijerph18189939