2. Materials and Methods
The study material consists of data on cases of use of an automated external defibrillator in adults (over 18 years of age) in the period from 1 January 2008 to 31 December 2018 in Poland. Only cases of use of AEDs in a public place, other than a medical facility, were analyzed, along with the exclusion of emergency services, i.e., the State Fire Service and Volunteer Fire Service, which have AEDs as part of their emergency equipment.
The study was approved by the Independent Bioethics Committee for Scientific Research at the Medical University of Gdansk No. NKBBN/52/2018 dated 12 February 2018. The data analyzed represent 120 cases of use of an automated external defibrillator placed in public spaces between 2008 and 2018. In addition, the research material were responses from a diagnostic survey questionnaire. The author’s questionnaire was sent to units where AEDs are located. The respondents’ answers to the questions recorded in the questionnaire were consistent with their consent to participate in the voluntary and free survey. The questionnaires were sent electronically. The questionnaire included the following questions:
Have any of the AED devices placed been used (years 2008–2018)?
By whom was the AED device used?
Under what circumstances was the AED device used? Please briefly characterize.
Was the AED distributor/manufacturer informed of the device’s use?
Did the AED distributor/manufacturer assist you in any way?
The next sources of data were AED manufacturers and distributors in the country, viz: Cardiac Science, Max Harter, Medline, Paramedica Polska, AEDMAX, Stryker, HS Medical, Medtronic, PHYSIO-CONTROL POLAND, Philips, DefiMed, Emtel, HeartSine, DefibTech, IPad, Primedic, Anatom. The respondents’ answers to the questions written in the questionnaire were consistent with their consent to participate in the voluntary and free study. The questionnaires were sent electronically. In case of no response, another e-mail was sent after one month. The questionnaire sent to manufacturers and distributors of AEDs in Poland contained the following questions:
Do you have knowledge about the use of AED device (years 2008–2018)?
Under what circumstances has the AED device been used? Please briefly characterize.
Did the device manager inform you of the use?
Did the AED manager require any assistance from you?
Another source of data analyzed were the responses from the author’s questionnaire sent to foundations involved in promoting first aid and healthy living principles such as: Great Orchestra of Christmas Charity Foundation, Polish Red Cross, World to Children Foundation, ORLEN “Gift of the Heart” Foundation, Department of Bioinformatics and Telemedicine of Collegium Medium UJ in Krakow. The questionnaire contained the following questions:
A retrospective analysis of selected medical records was also conducted. Data were obtained from the reports of the emergency notification center (medical dispatch center), cards of medical rescue activities—after obtaining permission from the dispatcher of the state medical rescue system—and the medical dispatch center. The data obtained were anonymized using only the date and time of the event, age, gender, implemented procedure. We analyzed data generated from a specific “type” of patients, from a specific unit in a given period (giving dates, months, or years), retrospectively in relation to the years 2008–2018.
The research material was collected in Microsoft Office Excel spreadsheet for Windows systems. Statistical analyses were performed using R 3.5.3 software (R version 3.5.3 (Great Truth) of 2019). Data testing was performed according to Poissone tests with a significance level of α = 0.05.
4. Discussion
The aim of the study was to analyze the way and correctness of using public external defibrillators in Poland, taking into account the 10-year period between 2008 and 2018.
The largest number of AEDs is located in the Mazovia Province (area—35,558 km
2; population—5,403,412; provincial city—Warsaw) and in the Małopolska Province (area—15,183 km
2; population—3,400,577; provincial city—Kraków) [
6]. Comparing the data with those published on the “Rescue with Heart” website [
7] the data are similar. According to the coordinators of the project, in 2017 there was the highest number of active AEDs in the Mazowieckie Province. Silesian province recorded a similar rate. The second place was taken by the Małopolska province. When analyzing the provinces with the highest number of stationary AEDs, the order was identical. There are no other data available to compare the presented results with. Taking into account the cities with the highest number of AEDs the order was as follows: Warsaw, Kraków, Katowice, Bydgoszcz, and Łódź. The result is not accidental and incomprehensible, as the presented cities are the seats of province offices. They cover a large area and are inhabited by a significant number of people. Additionally, they have significantly developed industry, education, and administration. Based on the study by Ślęzak [
8] and coordinators of the project “Save with Heart” [
9] the results are identical. Scientific reports on the location of AEDs in Polish cities were published by Cacko et al. [
10] in Warsaw, Żuratyński et al. [
11] in Bydgoszcz and Pogorzelczyk et al. [
12] in Tricity (Gdańsk, Gdynia, Sopot). Detailed localization data can be found in widely available phone applications or websites i.e., “Save with Heart”,—AED Map (
http://www.ratujzsercem.pl/; accessed on 2 October 2020) [
13]; AEDMAP (
https://www.stayingalive.org/; accessed on 2 October 2020) [
14]; AED + You = Life Campaign (
https://www.aedplusty.pl/; accessed on 2 October 2020) [
15]; AED Project (
https://projektaed.pl/; accessed on 2 October 2020) [
16]. Due to formal and legal considerations, specific models of AEDs located in public places will not be presented, only their most important technical parameters. A total 63% of the surveyed units answered which company produced the localized AED, and 37% stated only that it was an automatic device. Based on the review of literature and registers of AEDs as well as own observations, semi-automatic devices using biphasic discharge impulse dominate. They may differ only in the waveform, e.g., ascending biphasic SCOPE (optimized biphasic waveform adjusts the energy, slope, and impulse of the discharge to the patient’s impedance); straight biphasic, low energy. The device is certified safe for defibrillation on wet and metal surfaces and resistant to external factors such as drop, water, dust, pressure. This is very important because it can be used in such conditions many times. In terms of size and weight of the device, the dominant devices are up to 2 kg in weight and reach dimensions of 18 cm × 22 cm × 6 cm. The most common AED performs defibrillation in an adult with an energy of 150 J at 32 A, while in children with an energy of 50 J at 19 A. Adult defibrillation: nominal current of 32 amps. This is in accordance with ERC and AHA guidelines. Other technical data are not significant.
The surveyed entities confirmed that AEDs were used 65 times, in 60 locations, during the surveyed period 2008–2018. In 55 cases, the rescue was performed by a unit employee (84.62%), while only 10 were performed by a bystander (15.38%). Only 23 units described the circumstances of AED use.
After each use of the AED, the device should be serviced, the battery and adhesive electrodes replaced. For 34 locations where an AED was used, the unit reported the fact to the distributor/manufacturer of the device (56.67%). Every unit that reported AED use received any assistance from the AED distributor/manufacturer. The assistance consisted of replacing the leads, servicing the device, and reading out the record of the resuscitation action. Contrasting these data with those obtained from manufacturers and distributors of AEDs in Poland, AED managers are not obliged to report AED use. According to the distributors, buying new electrodes or replacing batteries does not indicate that the AED has been used, but may be a result of the elements becoming obsolete. Reiterating the most common reasons for not reporting use, distributors noted that entities do not want to publicize incidents as they may have a bad reputation for accidents at work.
Sudden cardiac arrest is more common among men. This is supported by many studies. The male gender is at risk for all heart diseases [
1,
3,
17,
18,
19,
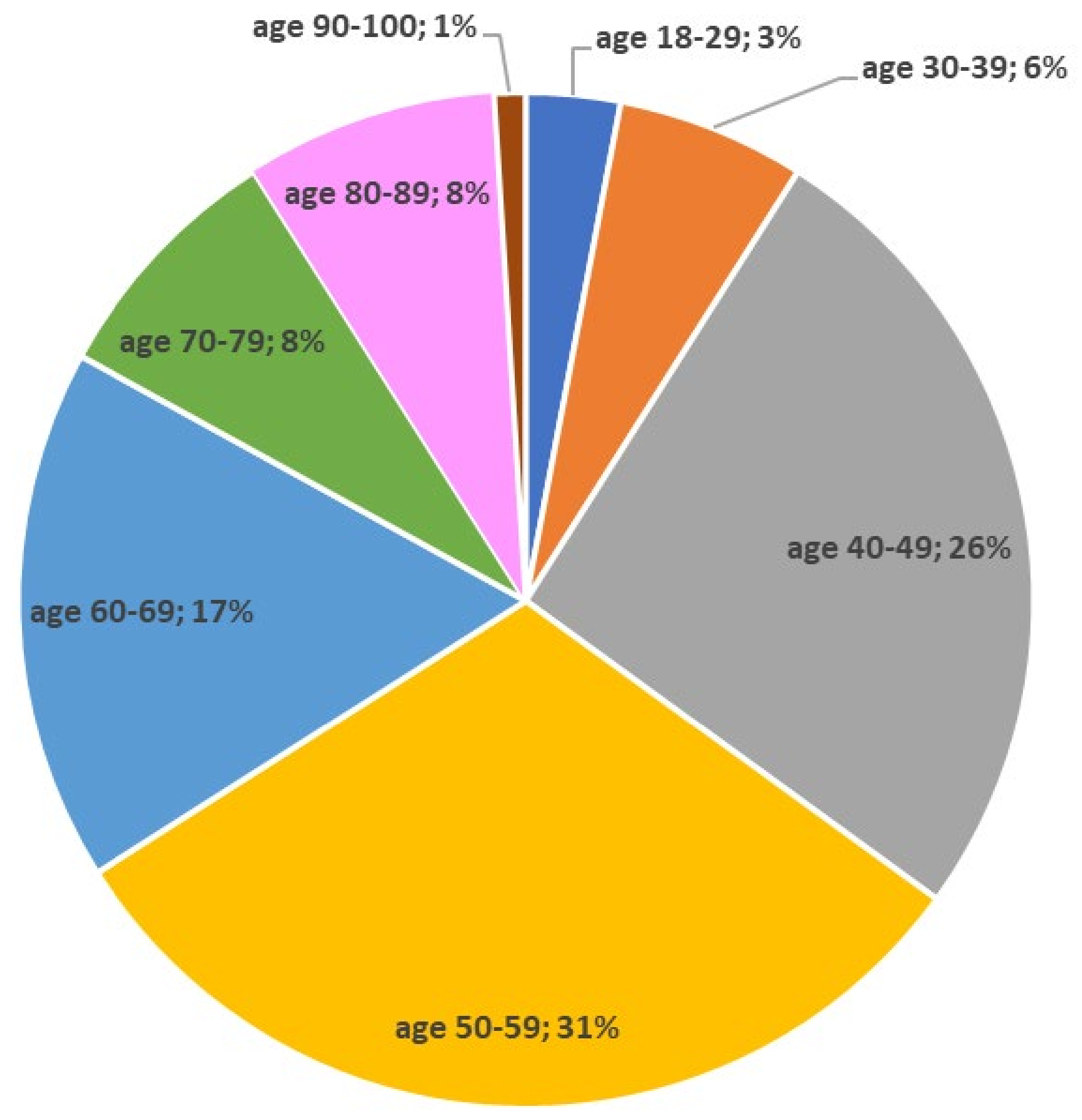
20]. In the material presented here, there is no deviation from global trends. A total 87.5% of AED interventions involved males. When analyzing the age group, it was observed that the highest rate of AED use occurred in the age group of 50–60 years (31%), which is included in the mean (57.27 years) and median (56.5 years). Again, this result can be correlated with the risk group and epidemiological data of SCA [
1,
3,
17,
18,
19,
20].
The largest group who experienced OHCA with AED intervention were travelers by various modes of transportation (30%). This is a result of high availability of defibrillators in the buildings of air, railroad, bus, or other public transport infrastructure. This group includes cases of AED use on board trains, in airports, and at railroad stations. According to the guidelines of ERC or AHA these are the places with the highest risk of OHCA, so the aim should be to have min. Therefore, there should be at least 1 automated defibrillator. This was confirmed by Caffrey et al. [
21], O’Rourke et al. [
22], Page et al. [
23] and Weaver et al. [
24], who published studies on AED use at airports and on board aircraft. Another group consisted of customers of retail, banking, or office establishments (23.33%) and employees (22.5%). These data can be compared with the profile of the place of defibrillator use. Most cases were on public transport infrastructure (n = 41; 34.17%), followed by places of work ( n =21; 17.5%) and places of public service (n = 20; 16.67%). Again, this is supported by the ERC and AHA guidelines as high-risk places.
The first person on the scene is of major importance in reducing OHCA mortality. The implementation of resuscitation depends on this person. Apart from notifying the emergency services and initiating resuscitation, it is important to provide and correctly use the AED. In the study group, it was most often an employee (80%) of one of the places. Security personnel were predominant. Besides them there were policemen, medical staff, hotel staff, streetcar drivers, and swimming pool attendants. Most of them were people who were responsible for AED in a given moment, had training in its use and were obliged to use it in a given moment. In one of the cases of AED use in Kraków, which took place in a library, the defibrillator was used thanks to the efficiency and self-control of the security guard. Only 20% were casual witnesses. Most often they were paramedics, medical students, and qualified first aid workers. A thorough comparison of the results with the literature is lacking, as only “first responders” or “witnesses” appear (witness), without a detailed characterization of that person.
When presenting the actions of a witness to an event with an OHCA victim, it was noted that in 63.33% the mechanism of cardiac arrest was defibrillatory (VT or VF), 30.83% nondefibrillatory or sinus rhythm was recognized. In 5.83%, no data were obtained. Based on scientific data, the most common SCA rhythm is ventricular fibrillation or ventricular tachycardia without a pulse. Each time the European Resuscitation Council or American Heart Association recommends the fastest possible defibrillation, which performed within 3–5 min from cardiac arrest determines the survival rate of 50–70%. It is worth noting that with every minute of delay in implementation of AED, the probability decreases by 10–12% [
25,
26,
27,
28,
29]. As mentioned, the rapid response of the witness to the event is important. On the basis of 33 documented resuscitation actions with the use of AED it can be stated that the average time that elapsed from SCA to the use of AED was 3 min 22 s, which was consistent with the ERC and AHA guidelines. The longest time elapsed from SCA to AED use was 10 min. In this case, the victim was defibrillated 2 times at the scene, then transferred to the emergency medical team, but did not receive ROSC. What reasons might have contributed to some of the delays in providing the AED? These include the witness’s lack of knowledge of the location of the AED, improper signage of the location, or the medical dispatcher’s lack of knowledge of the location. As stated in the 2015 ERC resuscitation guidelines, the medical dispatcher should have knowledge of the current distribution of AEDs in their area. Telec et al. [
27] investigated the assessment of actual AED availability and the assessment of possible sources of defibrillation delays in Poznań, Łódź, and Warsaw. From a selected group of 200 sites, they chose 78 sites and sent volunteers who had no knowledge of the location of AEDs in that site. Based on the OHCA simulation, the volunteers had to respond appropriately including, but not limited to, using the AED. The devices were located within a range of 2–163 m from the scene. The average total device delivery time was 96 s (1 min 36 s) with a maximum of 144 s (2 min 24 s). Delays that may occur in obtaining an AED were also assessed. These included only discussion with the person responsible for the AED (safety officer, staff, etc.) (mean time—16 s, max 49 s). The authors drew their conclusions, i.e., the recommended time for early defibrillation was below 3 min and there were some reasons that could affect the delay of defibrillation, e.g., badly marked places, lack of unrestricted access to AEDs (kept under the care of personnel or in cabinets).
Summing up the resuscitation actions performed, the average total time of AED operation on the scene was 7 min 34 s (+/−3 min 10 s). The minimum time of AED operation was 1 min 11 s, the maximum—15 min 23 s. Analyzing the number of defibrillations performed with AED at the scene, the average was 1.51 and the maximum was 4 defibrillations. Non-defibrillation rhythms were recognized in the total of 8 events (AS – n = 5, 15.15%; PEA – n = 3; 9.09%). The time elapsed from the end of rhythm analysis and defibrillation recommendation to the triggering of the electrical impulse was on average 7 s (SD=1 s), which is confirmed by the device specifications. The time from the end of CPR to readiness for discharge was 8 s [
30].
The goal of resuscitation procedures is to achieve ROSC. As is well known, rapid defibrillation is important in addition to chest compressions and ventilation. On the basis of such a small group, it cannot be concluded whether the return of spontaneous blood circulation is related to AED and public access defibrillation (PAD). In the study group, ROSC at the scene occurred in only 27 cases, with missing data from 58 cases. This is a topic that requires further research. Citing reports by Dwyer and Dennett [
31], the authors concluded that the use of AEDs in patients after cardiac arrest was not associated with improved survival. This study cannot be compared to the results of this paper because Dwyer and Dennett’s inference was for in-hospital cardiac arrest and in-hospital AED use.
Analyzing the time of arrival relative to the call and disposition received from the emergency notification centers, it was noted that the mean time was 564.66 s (9 min 24 s) with SD = 279.98 (4 min 39 s). The fastest EMS arrived after 240 s (4 min) and the latest after 1200 s (20 min). The fastest result indicated the nearest EMS station to the incident site. When analyzing the time of arrival of the first responders relative to the use of the AED, it was noted that the mean time was 469.47 s (7 min 49 s) with SD = 209.13 (3 min 29 s). Relative to the study value, the fastest EMS arrived 131 s (2 min 12 s) after AED use and the latest after 960 s (16 min). The fastest result indicated the closest location of EMS in relation to the incident site. The time of arrival of the first responders to the scene of the accident was within the standards established by the National Medical Rescue Act [
32]. Recalling the study by Zijlstra et al. [
33], the witness to the event used the AED on average 2 min 39 s before the arrival of the emergency medical service and for 10.5% performed the discharge less than 6 min after the call. Hallstrom et al. [
34] noted that the average time from the 911 call to the first rhythm analysis was almost 3 min shorter.
From the collected evidence, 16 OHCAs with AEDs (14.55%) had a patient survival of more than 30 days. A review of the literature showed a median overall survival of 40% in OHCA patients treated with PAD [
35].


 ,
, 




{kind=link}