
Improving Healthy Aging by Monitoring Patients’ Lifestyle through a Wearable Device: Results of a Feasibility Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. Study Design
2.3. Technology Acceptance and Interaction Assessment
2.4. Statistical Analysis
3. Results
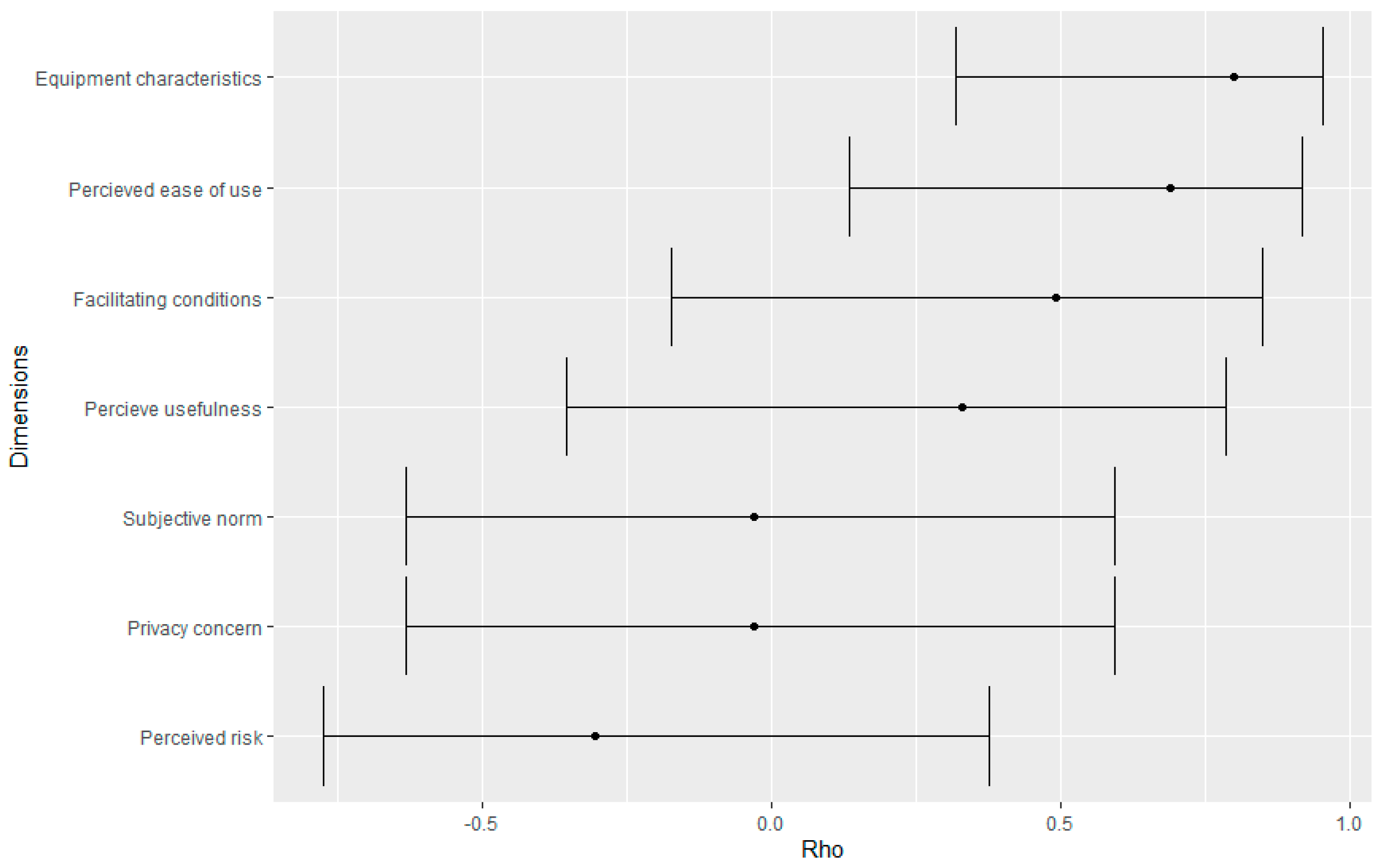
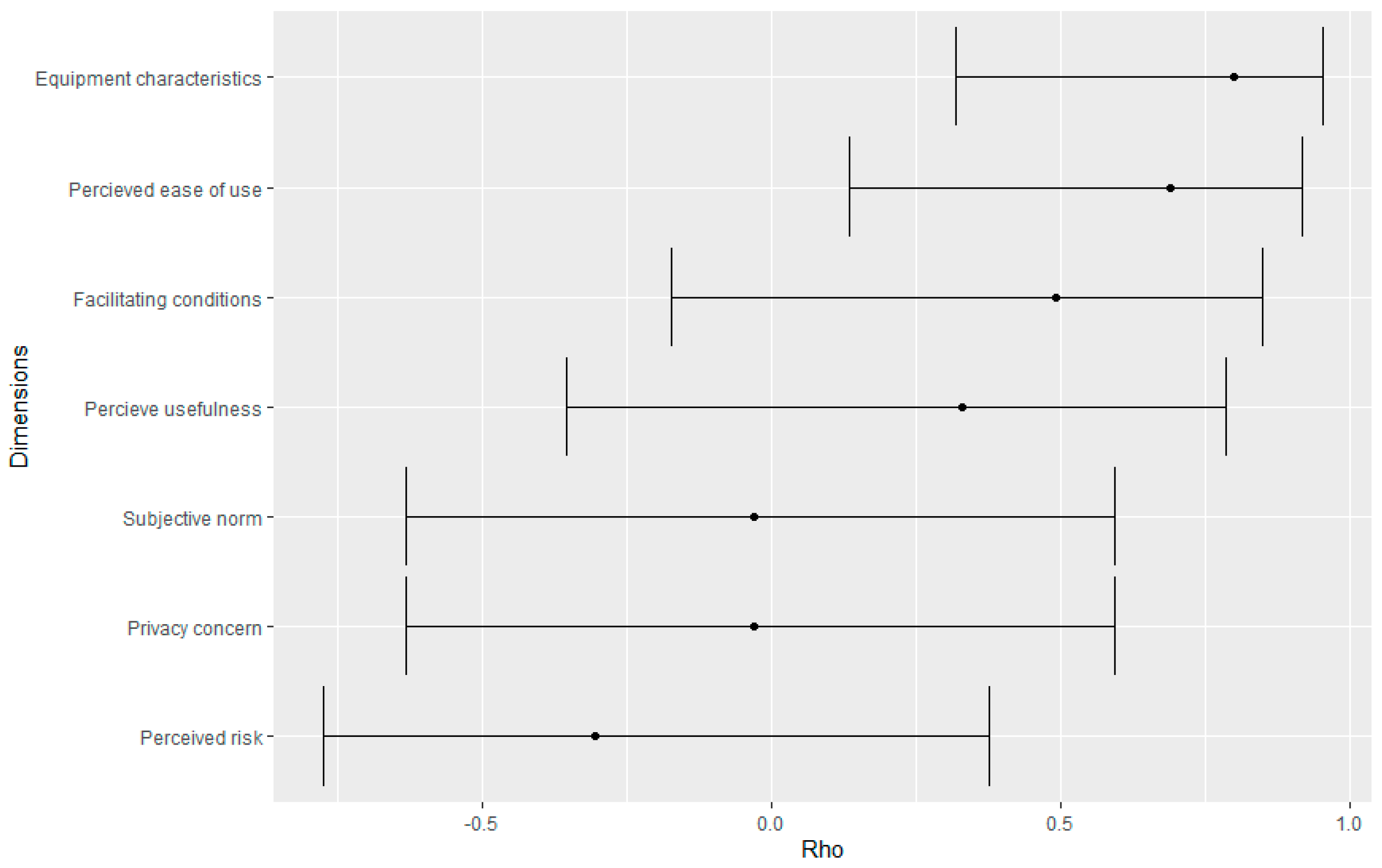
3.1. Technology Acceptance Questionnaire (Patients)
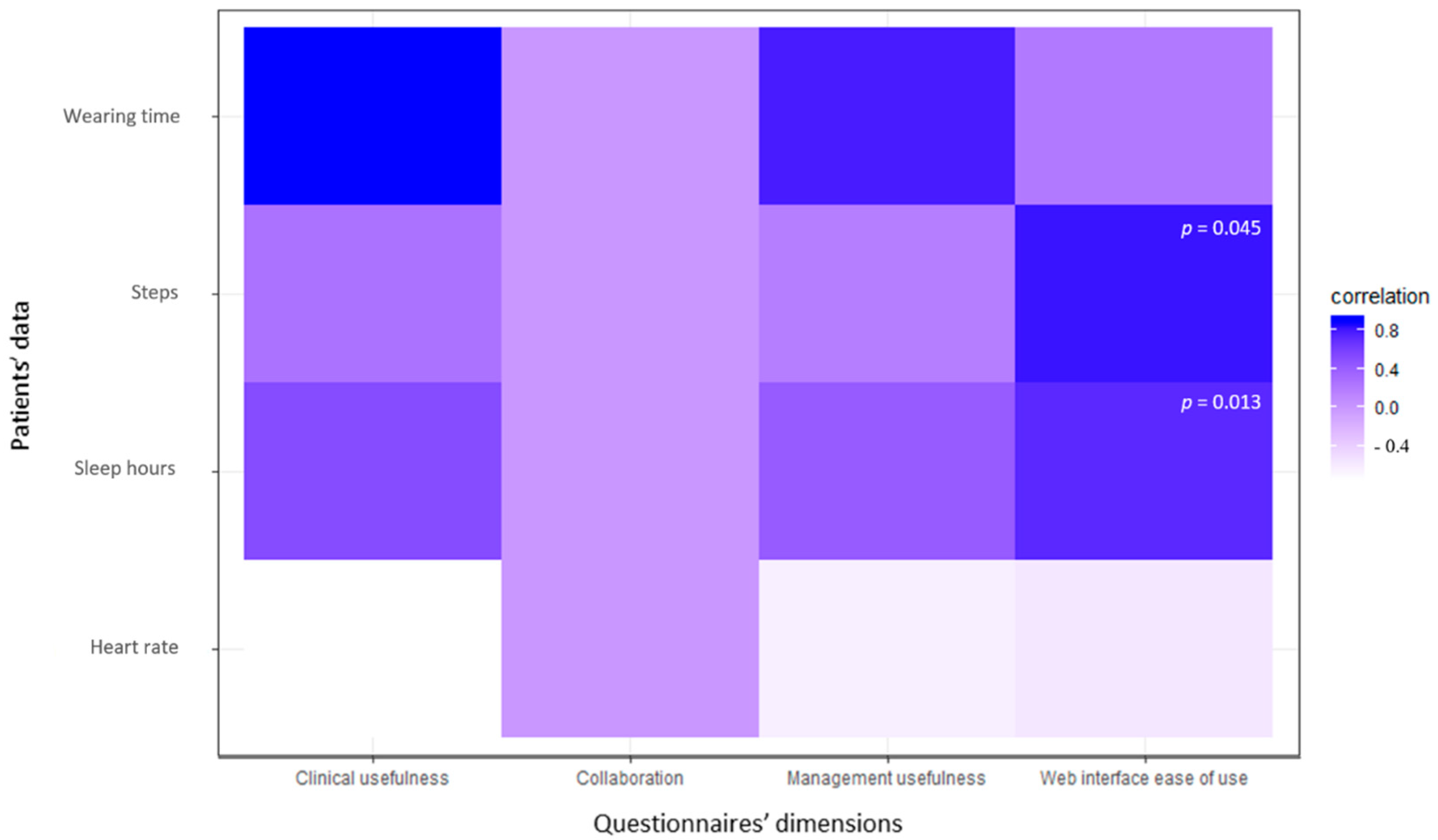
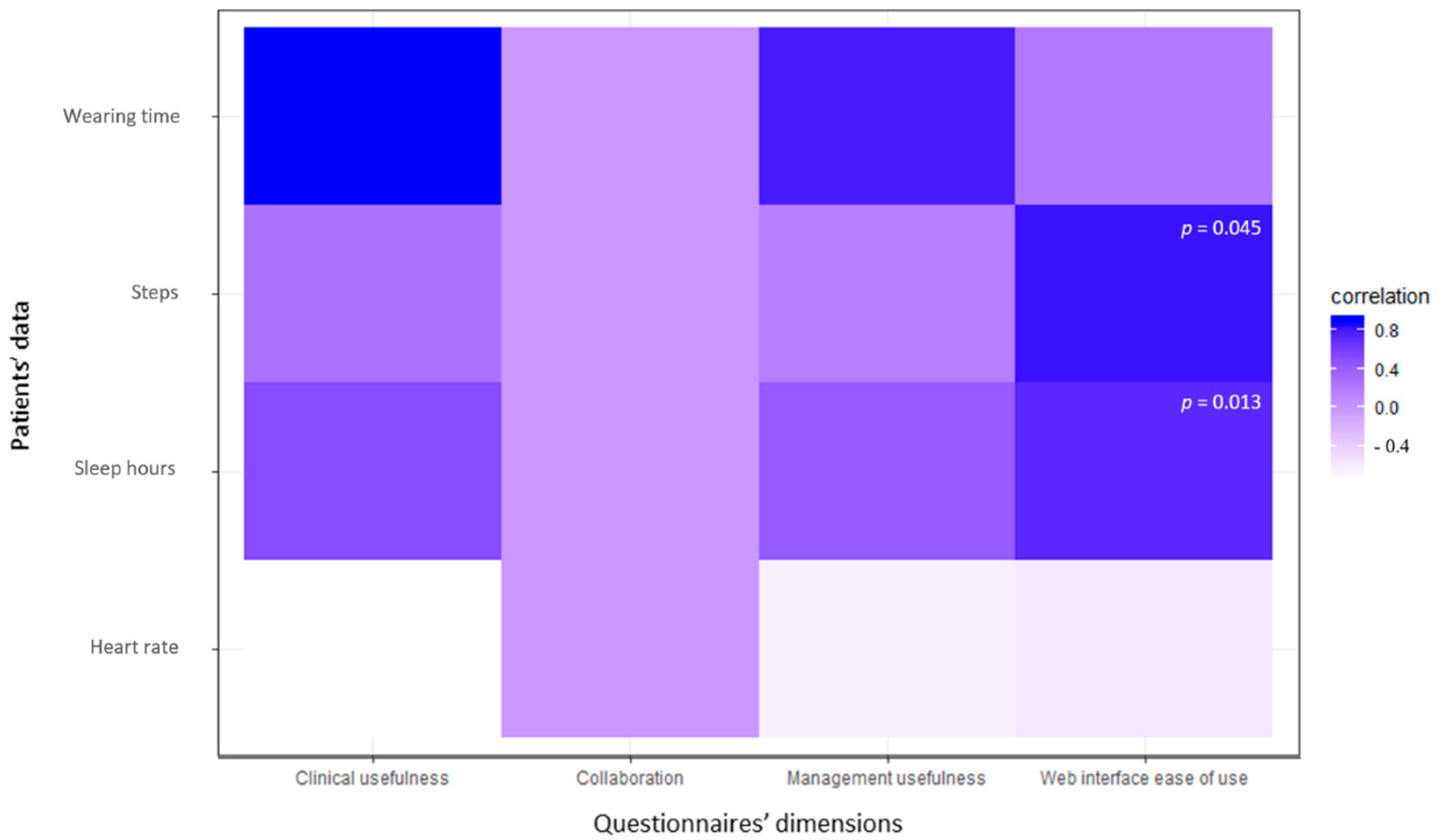
3.2. Technology Interaction Questionnaire (Professionals)
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Istat. Istat.it. Available online: http://www4.istat.it/it/anziani (accessed on 1 June 2021).
- Paolisso, G.; Boccardi, V. L’invecchiamento della popolazione: I dati dell’Osservatorio ARNO. J. Gerontol. 2014, 62, 60–63. [Google Scholar]
- Mazzola, P.; Rimoldi, S.M.L.; Rossi, P.; Noale, M.; Rea, F.; Facchini, C.; Maggi, S.; Corrao, G.; Annoni, G. Aging in Italy: The Need for New Welfare Strategies in an Old Country. Gerontologist 2015, 56, 383–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tedesco, S.; Barton, J.; O’Flynn, B. A Review of Activity Trackers for Senior Citizens: Research Perspectives, Commercial Landscape and the Role of the Insurance Industry. Sensors 2017, 17, 1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor-Locke, C.E.; Myers, A.M. Challenges and Opportunities for Measuring Physical Activity in Sedentary Adults. Sports Med. 2001, 31, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Appelboom, G.; Camacho, E.; E Abraham, M.; Bruce, S.S.; Dumont, E.L.; E Zacharia, B.; D’Amico, R.; Slomian, J.; Reginster, J.Y.; Bruyère, O.; et al. Smart wearable body sensors for patient self-assessment and monitoring. Arch. Public Health 2014, 72, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henriksen, A.; Mikalsen, M.H.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef] [PubMed]
- Ocagli, H.; Lorenzoni, G.; Lanera, C.; Schiavo, A.; D’Angelo, L.; Liberti, A.D.; Besola, L.; Cibin, G.; Martinato, M.; Azzolina, D.; et al. Monitoring Patients Reported Outcomes after Valve Replacement Using Wearable Devices: Insights on Feasibility and Capability Study: Feasibility Results. Int. J. Environ. Res. Public Health 2021, 18, 7171. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Stull, K.R.; Fantigrassi, M.; Motel, I. The efficacy of wearable activity tracking technology as part of a weight loss program: A systematic review. J. Sports Med. Phys. Fit. 2018, 58, 534–548. [Google Scholar] [CrossRef]
- Martinato, M.; Lorenzoni, G.; Zanchi, T.; Bergamin, A.; Buratin, A.; Azzolina, D.; Gregori, D. Usability and Accuracy of a Smartwatch for the Assessment of Physical Activity in the Elderly Population: Observational Study. JMIR mHealth uHealth 2021, 9, e20966. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Sanità e Salute. Available online: https://www.istat.it/it/files/2018/12/C04.pdf (accessed on 1 June 2021).
- Accordo Collettivo Nazionale Medici di Medicina gGenerale-Art. 40. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaArticolo?art.progressivo=0&art.idArticolo=40&art.versione=1&art.codiceRedazionale=000G0320&art.dataPubblicazioneGazzetta=2000-10-02&art.idGruppo=2&art.idSottoArticolo1=10&art.idSottoArticolo=1&art.flagTipoArticolo=1 (accessed on 2 June 2021).
- Puri, A.; Kim, B.; Nguyen, O.; Stolee, P.; Tung, J.; Lee, J. User Acceptance of Wrist-Worn Activity Trackers Among Community-Dwelling Older Adults: Mixed Method Study. JMIR mHealth uHealth 2017, 5, e173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vooijs, M.; Alpay, L.L.; Snoeck-Stroband, J.B.; Beerthuizen, T.; Siemonsma, P.C.; Abbink, J.J.; Sont, J.K.; A Rövekamp, T. Validity and Usability of Low-Cost Accelerometers for Internet-Based Self-Monitoring of Physical Activity in Patients With Chronic Obstructive Pulmonary Disease. Interact. J. Med. Res. 2014, 3, e14. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.K.; Lewis, B.; Oakes, M.; Guan, W.; Wyman, J.F.; Rothman, A.J. Older Adults’ Experiences Using a Commercially Available Monitor to Self-Track Their Physical Activity. JMIR mHealth uHealth 2016, 4, e35. [Google Scholar] [CrossRef] [PubMed]
- Mercer, K.; Giangregorio, L.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of Commercially Available Wearable Activity Trackers Among Adults Aged Over 50 and With Chronic Illness: A Mixed-Methods Evaluation. JMIR mHealth uHealth 2016, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Borup, M.T.; Trusina, A.; Andersson, A.M. Aging mechanism as the “down side” of adaptation: A network approach. J. Theor. Biol. 2008, 250, 66–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, P.E.; Gundersen, T.; Hejlesen, O.; Fensli, R. Sensor Acceptance Model—Measuring Patient Acceptance of Wearable Sensors. Methods Inf. Med. 2008, 47, 89–95. [Google Scholar] [CrossRef] [PubMed]
- R Foundation for Statistical Computing; R Development Core Team R. A Language and Environment for Statistical Computing; R Development Core Team R: Vienna, Austria, 2008; ISBN 3-900051-07-0. [Google Scholar]
- Harrell, F.E. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis, 2nd ed.; Springer: New York, NY, USA, 2015. [Google Scholar]
- Shih, P.C.; Han, K.; Poole, E.S.; Rosson, M.B.; Carroll, J.M. Use and Adoption Challenges of Wearable Activity Trackers; In iConference 2015 Proceedings. Available online: https://www.ideals.illinois.edu/bitstream/handle/2142/73649/164_ready.pdf (accessed on 26 June 2021).
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mynatt, E.; Melenhorst, A.-S.; Fisk, A.-D.; Rogers, W. Aware technologies for aging in place: Understanding user needs and attitudes. IEEE Pervasive Comput. 2004, 3, 36–41. [Google Scholar] [CrossRef]
- Segura Anaya, L.H.; Alsadoon, A.; Costadopoulos, N.; Prasad, P.W.C. Ethical Implications of User Perceptions of Wearable Devices. Sci. Eng. Ethics 2018, 24, 1–28. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | n = 11 |
|---|---|
| Age in years, median (IQR) | 69 (67–72) |
| Sex, n (%) | |
| Male | 10 (91%) |
| Female | 1 (9%) |
| Marital status, n (%) | |
| Married | 10 (91%) |
| Widowed | 1 (9%) |
| Educational level | |
| Primary school | 4 (36%) |
| Secondary school | 7 (64%) |
| BMI, median (IQR) | 28 (27.5–31.0) |
| Panel A | ||||
|---|---|---|---|---|
| Patients’ Educational Level | ||||
| Dimensions (Scale Maximum Score) | Primary School (n = 4) | Secondary School (n = 7) | Combined (n = 11) | p |
| Perceived usefulness (25) | 19.5 (18.0–20.3) | 17.0(13.0–18.0) | 18.0 (14.5–19.5) | 0.165 |
| Perceived ease-of-use (35) | 26.5 (24.5–29.3) | 25.0 (21.0–27.0) | 25.0 (22.5–28.0) | 0.370 |
| Equipment characteristics (30) | 28.6 (27.2–31.0) | 26.0 (24.0–28.5) | 27.2 (25.5–29.5) | 0.279 |
| Privacy concern (15) | 11.00 (10.25–11.25) | 11.0 (7.0–13.0) | 11.0 (7.5–11.5) | 0.719 |
| Perceived risk (15) | 4.5 (3.8–5.5) | 8.0 (8.0–9.0) | 8.0 (4.5–8.0) | 0.033 |
| Facilitating conditions (10) | 4.0 (2.0–7.0) | 7.0 (6.0–8.0) | 6.0 (4.0–8.0) | 0.466 |
| Subjective norm (15) | 10.0 (9.0–11.5) | 9.0 (7.0–12.5) | 9.0 (8.5–12.0) | 0.594 |
| Panel B | ||||
| Professional Type | ||||
| Nurse (n = 3) | Physician (n = 3) | Combined (n = 6) | p | |
| Clinical usefulness (35) | 25.0 (22.5–28.0) | 27.0 (25.0–29.5) | 26.0 (23.5–30.0) | 0.573 |
| Management usefulness (15) | 10.0 (10.0–11.0) | 11.0 (10.0–12.0) | 10.5 (10.0–11.7) | 0.852 |
| Web interface ease-of-use (15) | 11.0 (9.5–11.5) | 10.0 (9.0–11.5) | 10.5 (8.5–11.7) | 1 |
| Collaboration (10) | 8.0 (7.5–9.0) | 7.0 (7.0–7.5) | 7.5 (7.0–8.0) | 0.405 |
| Patients’ Educational Level | ||||
|---|---|---|---|---|
| Patients’ Variables | Acceptability: No (n = 3) | Acceptability: Yes (n = 7) | Combined (n = 10) | p |
| Median steps | 3859 (1929–6170) | 6987 (6075–8138) | 6612 (4384–8302) | 0.23 |
| Median sleep hours | 6.0 (6.0–6.0) | 7.0 (6.5–7.0) | 7.0 (6.0–7.0) | 0.24 |
| Median wearing time (hours) | 17.0 (4.5–20.5) | 24.0 (23.5–24.0) | 24.0 (8.5–24.0) | 0.33 |
| Median heart rate | 69 (67–71) | 53 (51–55) | 53 (52–66) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fioranzato, M.; Comoretto, R.I.; Lanera, C.; Pressato, L.; Palmisano, G.; Barbacane, L.; Gregori, D. Improving Healthy Aging by Monitoring Patients’ Lifestyle through a Wearable Device: Results of a Feasibility Study. Int. J. Environ. Res. Public Health 2021, 18, 9806. https://doi.org/10.3390/ijerph18189806
Fioranzato M, Comoretto RI, Lanera C, Pressato L, Palmisano G, Barbacane L, Gregori D. Improving Healthy Aging by Monitoring Patients’ Lifestyle through a Wearable Device: Results of a Feasibility Study. International Journal of Environmental Research and Public Health. 2021; 18(18):9806. https://doi.org/10.3390/ijerph18189806
Chicago/Turabian StyleFioranzato, Maria, Rosanna Irene Comoretto, Corrado Lanera, Lamberto Pressato, Giuseppe Palmisano, Luca Barbacane, and Dario Gregori. 2021. "Improving Healthy Aging by Monitoring Patients’ Lifestyle through a Wearable Device: Results of a Feasibility Study" International Journal of Environmental Research and Public Health 18, no. 18: 9806. https://doi.org/10.3390/ijerph18189806
APA StyleFioranzato, M., Comoretto, R. I., Lanera, C., Pressato, L., Palmisano, G., Barbacane, L., & Gregori, D. (2021). Improving Healthy Aging by Monitoring Patients’ Lifestyle through a Wearable Device: Results of a Feasibility Study. International Journal of Environmental Research and Public Health, 18(18), 9806. https://doi.org/10.3390/ijerph18189806