
The Association between Diabetes Mellitus and Keratoplasty in Poland in the Years 2013–2017



Abstract
:1. Introduction
2. Material and methods
2.1. Data Sources, Disease Codes, and Definitions
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indication | Indication ICD-10 |
|---|---|
| Ocular surface diseases | H18.8 |
| Bullous keratopathy | H18.1 |
| Infectious keratitis and corneal ulcers | H16.0, H16.2, H16.3, H16.8, H16.9 |
| Keratoconus | H18.6 |
| Leucoma and corneal scars | H17.8, H17.9, H17.1 |
| Corneal pigmentations and deposits | H18.0 |
| Corneal dystrophies incl. Fuchs’s dystrophy | H18.5 |
| Band keratopathy | H18.4 |
| Other | - |
Appendix B
| Comorbidity Variable | Comorbidity Group (ICD-10 Codes) | |
|---|---|---|
| 1 | AIDS/HIV | B20, B21, B22, B24 |
| 2 | Alcohol abuse | F10, E52, G62.1, I42.6, K29.2, K70.0, K70.3, K70.9, T51, Z50.2, Z71.4, Z72.1 |
| 3 | Blood loss anemia | D50.0 |
| 4 | Arrhythmias | I44.1, I44.2, I44.3, I45.6, I45.9, I47–I49, R00.0, R00.1, R00.8, T82.1, Z45.0, Z95.0 |
| 5 | Chronic pulmonary disease | I27.8, I27.9, J40–J47, J60–J67, J68.4, J70.1, J70.3 |
| 6 | Coagulopathy | D65, D66, D67, D68, D69.1, D69.3, D69.4, D69.5, D69.6 |
| 7 | Congestive heart failure | I09.9, I11.0, I13.0, I13.2, I25.5, I42.0, I42.5, I42.6, I42.7, I42.8, I42.9, I43, I50, P29.0 |
| 8 | Deficiency anemia | D50.8, D50.9, D51, D52, D53 |
| 9 | Depression | F20.4, F31.3, F31.4, F31.5, F32, F33, F34.1, F41.2, F43.2 |
| 10 | Diabetes, Type 1 | E10 confirmed with purchased medications |
| 11 | Diabetes, Type 2 | E11 confirmed with purchased medications |
| 12 | Drug abuse | F11, F12, F13, F14, F15, F16, F18, F19, Z71.5, Z72.2 |
| 13 | Fluid and electrolyte disorders | E22.2, E86, E87 |
| 14 | Hypertension | I10, I11, I12, I13, I15 |
| 15 | Hypothyroidism | E00, E01, E02, E03, E89.0 |
| 16 | Liver disease | B18, I85, I86.4, I98.2, K70, K71.1, K71.3–K71.5, K71.7, K72–K74, K76.0, K76.2–K76.9, Z94.4 |
| 17 | Lymphoma | C81, C82, C83, C84, C85, C88, C96, C90.0, C90.2 |
| 18 | Metastatic cancer | C77, C78, C79, C80 |
| 19 | Obesity | E66 |
| 20 | Other neurological disorders | G10–G13, G20–G22, G25.4, G25.5, G31.2, G31.8, G31.9, G32, G35–G37, G40, G41, G93.1, G93.4, R47.0, R56 |
| 21 | Paralysis | G04.1, G11.4, G80.1, G80.2, G81, G82, G83.0, G83.1, G83.2, G83.3, G83.4, G83.9 |
| 22 | Peptic ulcer disease excluding bleeding | K25.7, K25.9, K26.7, K26.9, K27.7, K27.9, K28.7, K28.9 |
| 23 | Peripheral vascular disorders | I70, I71, I73.1, I73.8, I73.9, I77.1, I79.0, I79.2, K55.1, K55.8, K55.9, K95.8, Z95.9 |
| 24 | Psychoses | F20, F22, F23, F24, F25, F28, F29, F30.2, F31.2, F31.5 |
| 25 | Pulmonary circulation disorders | I26, I27, I28.0, I28.8, I28.9 |
| 26 | Renal failure | I12.0, I13.1, N18, N19, N25.0, Z49.0, Z49.1, Z49.2, Z94.0, Z99.2 |
| 27 | Rheumatoid arthritis/collagen vascular diseases | L94.0, L94.1, L94.3, M05, M06, M08, M12.0, M12.3, M30, M31.0–M31.3, M32–M35, M45, M46.1, M46.8, M46.9 |
| 28 | Solid tumor without metastasis | C00–C26, C30–C34, C37–C41, C43, C45–C58, C60–C76, C97 |
| 29 | Valvular disease | A52.0, I05–I08, I09.1, I09.8, I34–I39, Q23.0–Q23.3, Z95.2, Z95.3, Z95.4 |
| 30 | Weight loss | E40–E46, R63.4, R64 |
References
- Resnikoff, S.; Pascolini, D.; Etya’Ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar] [PubMed]
- World Health Organization. Global Initiative for the Elimination of Avoidable Blindness; Unpublished Document WHO/PBL/97.61/Rev 1; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Schwartz, E.C.; Huss, R.; Hopkins, A.; Dadjim, B.; Madjitoloum, P.; Henault, C.; Klauss, V. Blindness and visual impairment in a region endemic for onchocerciasis in the Central African Republic. Br. J. Ophthalmol. 1997, 81, 443–447. [Google Scholar] [CrossRef]
- Pascolini, D.; Mariotti, S.P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 2011, 96, 614–618. [Google Scholar] [CrossRef] [Green Version]
- Gain, P.; Jullienne, R.; He, Z.; Aldossary, M.; Acquart, S.; Cognasse, F.; Thuret, G. Global Survey of Corneal Transplantation and Eye Banking. JAMA Ophthalmol. 2016, 134, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Grzybowski, A.; Patryn, R. Current state of corneal transplants in Poland. Acta Ophthalmol. 2017, 96, e93–e94. [Google Scholar] [CrossRef] [Green Version]
- Zacharias, T.; Ferreira, N. Nutritional risk screening 2002 and ASA score predict mortality after elective liver resection for malignancy. Arch. Med. Sci. 2017, 13, 361–369. [Google Scholar] [CrossRef] [Green Version]
- Budzyński, J.; Tojek, K.; Wustrau, B.; Czerniak, B.; Winiarski, P.; Korzycka-Wilińska, W.; Banaszkiewicz, Z. The “cholesterol paradox” among inpatients–retrospective analysis of medical documentation. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, e46–e57. [Google Scholar] [CrossRef]
- Chlebicki, A.; Kozioł, M. Homogeneous Group approach to Elixhauser comorbidity for hospital death using administrative data. Arch. Med. Sci. 2020, 16, 321–336. [Google Scholar] [CrossRef]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 1, 8–27. [Google Scholar] [CrossRef]
- Ing, J.J.; Ing, H.H.; Nelson, L.R.; Hodge, D.O.; Bourne, W.M. Ten-year postoperative results of penetrating keratoplasty. Ophthalmology 1998, 105, 1855–1865. [Google Scholar] [CrossRef]
- Wang, J.; Chen, K.; Li, X.; Jin, X.; An, P.; Fang, Y.; Mu, Y. Postoperative adverse events in patients with diabetes undergoing orthopedic and general surgery. Medicine 2019, 98, e15089. [Google Scholar] [CrossRef]
- Świrska, J.; Czuczwar, P.; Zwolak, A.; Matyjaszek-Matuszek, B. Perioperative complications of gynecologic surgery in diabetic patients. Ginekol. Polska 2016, 87, 194–199. [Google Scholar] [CrossRef]
- Huang, P.-Y.; Lin, M.-Z.; Wen, J.-P.; Li, X.-J.; Shi, X.-L.; Zhang, H.-J.; Chen, N.; Li, X.-Y.; Yang, S.-Y.; Chen, G. Correlation of early postoperative blood glucose levels with postoperative complications, hospital costs, and length of hospital stay in patients with gastrointestinal malignancies. Endocrine 2014, 48, 187–194. [Google Scholar] [CrossRef]
- Nowak, M.S.; Grabska-Liberek, I.; Michalska-Małecka, K.; Grzybowski, A.; Kozioł, M.; Niemczyk, W.; Więckowska, B.; Szaflik, J.P. Incidence and Characteristics of Cataract Surgery in Poland, during 2010–2015. Int. J. Environ. Res. Public Health 2018, 15, 435. [Google Scholar] [CrossRef] [Green Version]
- Nowak, M.S.; Grzybowski, A.; Michalska-Małecka, K.; Szaflik, J.P.; Kozioł, M.; Niemczyk, W.; Grabska-Liberek, I. Incidence and Characteristics of Endophthalmitis after Cataract Surgery in Poland, during 2010–2015. Int. J. Environ. Res. Public Health 2019, 16, 2188. [Google Scholar] [CrossRef] [Green Version]
- Kozioł, M.; Nowak, M.S.; Udziela, M.; Piątkiewicz, P.; Grabska-Liberek, I.; Szaflik, J.P. First nation-wide study of diabetic retinopathy in Poland in the years 2013–2017. Acta Diabetol. 2020, 57, 1255–1264. [Google Scholar] [CrossRef]
- National Health Fund Data. Available online: http://www.nfz.gov.pl (accessed on 10 August 2020).
- Central Statistical Office of Poland Data. Available online: http://www.stat.gov.pl (accessed on 10 August 2020).
- Yu, A.; Schaumberger, M.; Kaiser, M.; Messmer, E.; Kook, D.; Welge-Lussen, U. Perioperative and postoperative risk factors for corneal graft failure. Clin. Ophthalmol. 2014, 8, 1641–1647. [Google Scholar] [CrossRef] [Green Version]
- Dandona, L.; Naduvilath, T.; Janarthanan, M.; Ragu, K.; Rao, G.N. Survival analysis and visual outcome in a large series of corneal transplants in India. Br. J. Ophthalmol. 1997, 81, 726–731. [Google Scholar] [CrossRef]
- Flockerzi, E.; Maier, P.; Böhringer, D.; Reinshagen, H.; Kruse, F.; Cursiefen, C.; Reinhard, T.; Geerling, G.; Torun, N.; Seitz, B. Trends in Corneal Transplantation from 2001 to 2016 in Germany: A Report of the DOG–Section Cornea and its Keratoplasty Registry. Am. J. Ophthalmol. 2018, 188, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Zeschau, A.; Balestrin, I.G.; Stock, R.A.; Bonamigo, E.L. Indications of keratoplasty: A retrospective study in a University Hospital. Rev. Bras. Oftalmol. 2013, 72, 316–320. [Google Scholar] [CrossRef] [Green Version]
- Al-Yousuf, N.; Mavrikakis, I.; Daya, S.M. Penetrating keratoplasty: Indications over a 10 year period. Br. J. Ophthalmol. 2004, 88, 998–1001. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.Q.; Rubenstein, D.; Price, A.J.; Côté, E.; Levitt, M.; Sharpen, L.; Slomovic, A. Evolving surgical techniques of and indications for corneal transplantation in Ontario: 2000–2012. Can. J. Ophthalmol. 2013, 48, 153–159. [Google Scholar] [CrossRef]
- Ljubimov, A.V. Diabetic complications in the cornea. Vis. Res. 2017, 139, 138–152. [Google Scholar] [CrossRef]
- Didenko, T.N.; Smoliakova, G.P.; Sorokin, E.L.; Egorov, V.V. Clinical and pathogenetic features of neurotrophic corneal disorders in diabetes. Vestn. Oftalmol. 2000, 115, 7–11. [Google Scholar]
- Yu, A.L.; Kaiser, M.; Schaumberger, M.; Messmer, E.; Kook, D.; Welge-Lussen, U. Donor-Related Risk Factors and Preoperative Recipient-Related Risk Factors for Graft Failure. Cornea 2014, 33, 1149–1156. [Google Scholar] [CrossRef] [Green Version]
- Watson, S.; Ramsay, A.; Dart, J.K.; Bunce, C.; Craig, E. Comparison of deep lamellar keratoplasty and penetrating keratoplasty in patients with keratoconus. Ophthalmology 2004, 111, 1676–1682. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2019. Available online: http://vizhub.healthdata.org/gbd-compare/ (accessed on 7 April 2021).

| 2013 | 2014 | 2015 | 2016 | 2017 | All (Average) | |
|---|---|---|---|---|---|---|
| Age 0–18 | 7,431,731 | 7,367,066 | 7,309,001 | 7,286,480 | 7,299,996 | 7,338,855 |
| DM in the subgroup, % | 0.18% | 0.19% | 0.20% | 0.21% | 0.22% | 0.20% |
| No. of corneal grafts | 27 | 33 | 17 | 35 | 18 | 130 |
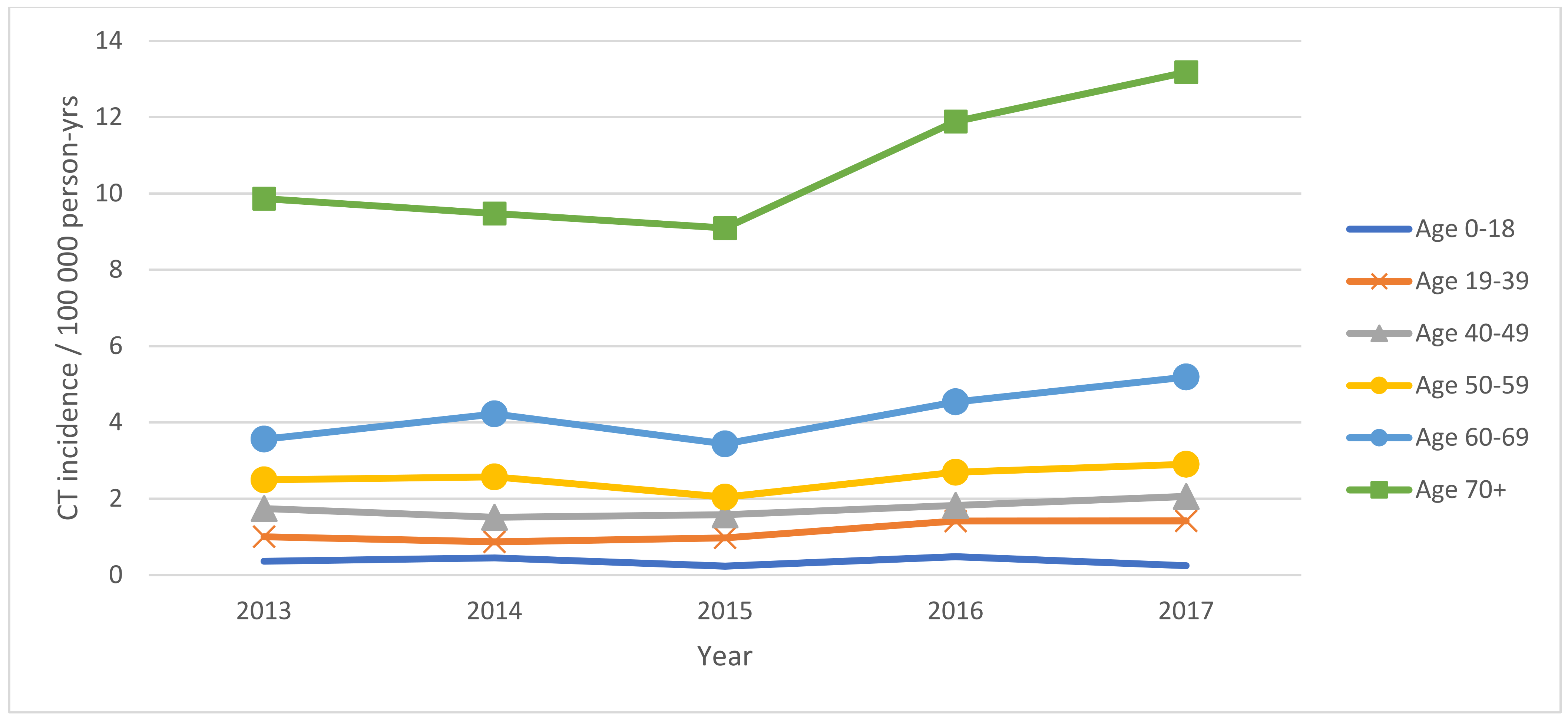
| Incidence/100,000 person-yrs | 0.36 | 0.45 | 0.23 | 0.48 | 0.25 | 0.35 |
| DM, % | 0.00% | 0.00% | 0.00% | 2.86% | 0.00% | 0.57% |
| Age 19–39 | 12,355,235 | 12,201,430 | 12,015,345 | 11,799,562 | 11,570,164 | 11,988,347 |
| DM in the subgroup, % | 0.58% | 0.68% | 0.79% | 0.90% | 1.01% | 0.79% |
| fNo. of corneal grafts | 124 | 106 | 117 | 167 | 164 | 678 |
| Incidence/100,000 person-yrs | 1.00 | 0.87 | 0.97 | 1.42 | 1.42 | 1.14 |
| DM, % | 4.03% | 4.72% | 1.71% | 1.20% | 1.83% | 2.70% |
| Age 40–49 | 4,879,816 | 4,956,005 | 5,064,587 | 5,202,444 | 5,341,530 | 5,088,876 |
| DM in the subgroup, % | 2.14% | 2.30% | 2.45% | 2.59% | 2.70% | 2.44% |
| No. of corneal grafts | 85 | 75 | 80 | 95 | 110 | 445 |
| Incidence/100,000 person-yrs | 1.74 | 1.51 | 1.58 | 1.83 | 2.06 | 1.74 |
| DM, % | 10.59% | 8.00% | 7.50% | 16.84% | 7.27% | 10.04% |
| Age 50–59 | 5,536,118 | 5,406,320 | 5,245,352 | 5,089,290 | 4,928,276 | 5,241,071 |
| DM in the subgroup, % | 6.87% | 7.16% | 7.38% | 7.57% | 7.68% | 7.33% |
| No. of corneal grafts | 138 | 139 | 107 | 137 | 143 | 664 |
| Incidence/100,000 person-yrs | 2.49 | 2.57 | 2.04 | 2.69 | 2.90 | 2.54 |
| DM, % | 15.22% | 15.83% | 10.28% | 10.22% | 9.79% | 12.27% |
| Age 60–69 | 4,409,809 | 4,642,821 | 4,888,294 | 5,024,702 | 5,127,315 | 4,818,588 |
| DM in the subgroup, % | 15.53% | 16.20% | 16.76% | 17.15% | 17.34% | 16.60% |
| No. of corneal grafts | 157 | 196 | 168 | 228 | 266 | 1015 |
| Incidence/100,000 person-yrs | 3.56 | 4.22 | 3.44 | 4.54 | 5.19 | 4.19 |
| DM, % | 35.67% | 26.02% | 36.31% | 25.88% | 24.06% | 29.59% |
| Age 70+ | 3,882,950 | 3,904,960 | 3,914,660 | 4,030,514 | 4,166,277 | 3,979,872 |
| DM in the subgroup, % | 21.41% | 22.88% | 24.15% | 25.27% | 26.17% | 23.98% |
| No. of corneal grafts | 383 | 370 | 356 | 479 | 549 | 2137 |
| Incidence/100,000 person-yrs | 9.86 | 9.48 | 9.09 | 11.88 | 13.18 | 10.70 |
| DM, % | 31.85% | 32.16% | 35.39% | 33.19% | 30.24% | 32.57% |
| All | 38,495,659 | 38,478,602 | 38,437,239 | 38,432,992 | 38,433,558 | 38,455,610 |
| DM in the subgroup, % | 5.42% | 5.83% | 6.20% | 6.56% | 6.86% | 6.17% |
| No. of corneal grafts | 914 | 919 | 845 | 1141 | 1250 | 5069 |
| Incidence/100,000 person-yrs | 2.37 | 2.39 | 2.20 | 2.97 | 3.25 | 2.64 |
| DM, % | 23.30% | 22.09% | 24.38% | 22.00% | 20.40% | 22.43% |
| 2013 | 2014 | 2015 | 2016 | 2017 | All | |
|---|---|---|---|---|---|---|
| Mean age ± SE | 60.99 ± 19.45 | 61 ± 18.8 | 61.25 ± 19.32 | 61.29 ± 20.04 | 63.15 ± 18.4 | 61.63 ± 19.2 |
| Women (%) | 426 (49.71%) | 412 (47.96%) | 388 (49.87%) | 554 (52.31%) | 615 (53.15%) | 2395 (50.85%) |
| Men (%) | 431 (50.29%) | 447 (52.04%) | 390 (50.13%) | 505 (47.69%) | 542 (46.85%) | 2315 (49.15%) |
| Urban residence (%) | 612 (71.41%) | 600 (69.85%) | 550 (70.69%) | 740 (69.88%) | 792 (68.45%) | 3294 (69.94%) |
| Rural Residence (%) | 245 (28.59%) | 259 (30.15%) | 228 (29.31%) | 319 (30.12%) | 365 (31.55%) | 1416 (30.06%) |
| Indication | No. of Corneal Grafts 2013–2017 (% of all) | No. of Subjects with Corneal Grafts and Type 1 DM (% of All) | No. of Subjects with Corneal Grafts and Type 2 DM (% of All) | No. of Full-Thickness Corneal Grafts 2013–2017 (% of All) | No. of Partial-Corneal Grafts 2013–2017 (% of All) |
|---|---|---|---|---|---|
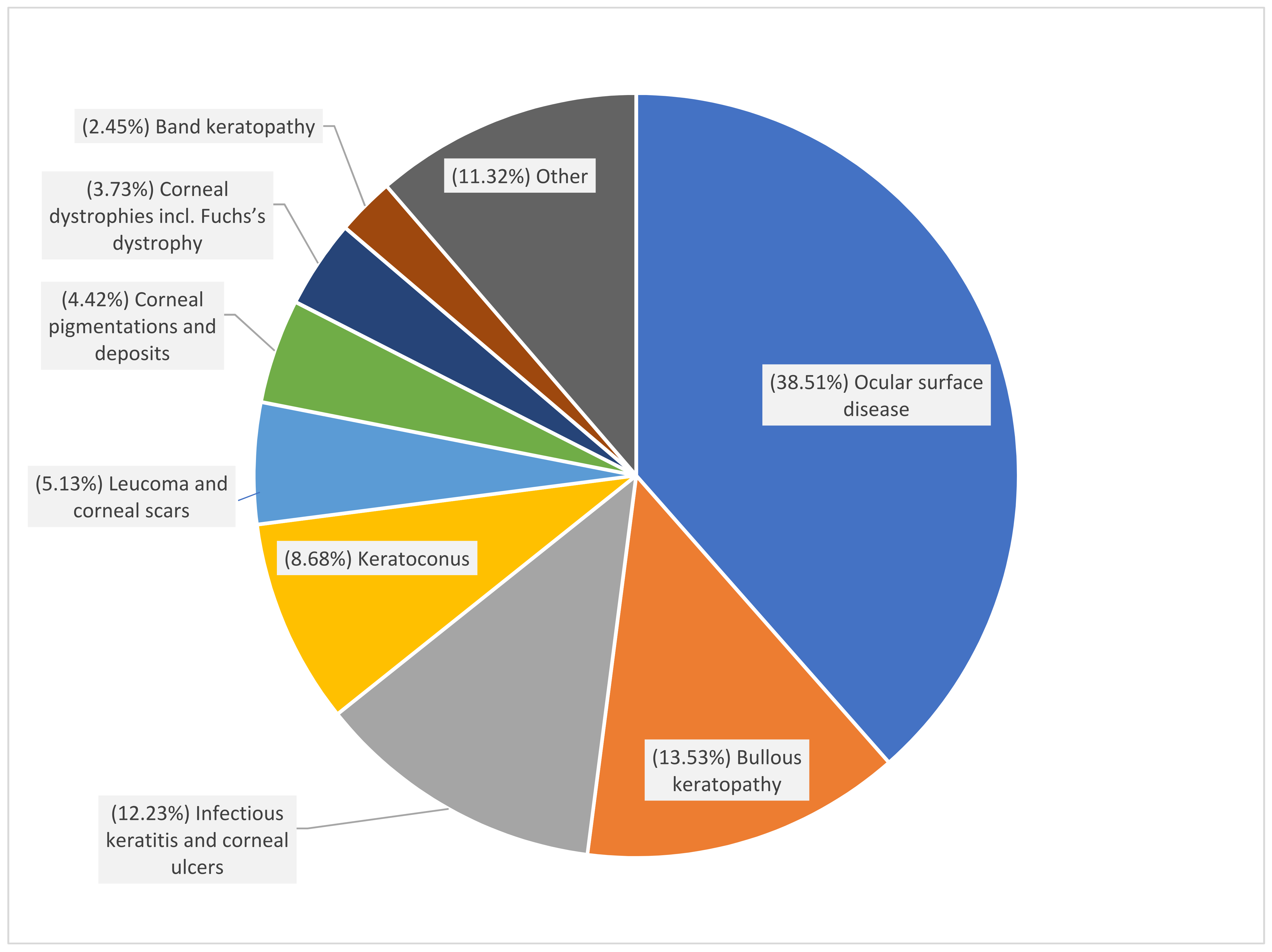
| Ocular surface disease | 1952 (38.51%) | 33 (41.77%) | 411 (39.18%) | 1707 (41.86%) | 245 (24.72%) |
| Bullous keratopathy | 686 (13.53%) | 9 (11.39%) | 182 (17.35%) | 386 (9.47%) | 300 (30.27%) |
| Infectious keratitis and corneal ulcers | 620 (12.23%) | 19 (24.05%) | 131 (12.49%) | 591 (14.49%) | 29 (2.93%) |
| Keratoconus | 440 (8.68%) | 1 (1.27%) | 21 (2.00%) | 386 (9.47%) | 54 (5.45%) |
| Leucoma and corneal scars | 260 (5.13%) | 3 (3.80%) | 53 (5.05%) | 242 (5.93%) | 18 (1.82%) |
| Corneal pigmentations and deposits | 224 (4.42%) | 0 (0.00%) | 59 (5.62%) | 194 (4.76%) | 30 (3.03%) |
| Corneal dystrophies incl. Fuchs’s dystrophy | 189 (3.73%) | 2 (2.53%) | 38 (3.62%) | 39 (0.96%) | 150 (15.14%) |
| Band keratopathy | 124 (2.45%) | 2 (2.53%) | 26 (2.48%) | 80 (1.96%) | 44 (4.44%) |
| Other | 574 (11.32%) | 10 (12.66%) | 128 (12.20%) | 453 (11.11%) | 121 (12.21%) |
| All | 5069 (100%) | 79 (100%) | 1049 (100%) | 991 (100%) | 4078 (100%) |
| 2013 | 2014 | 2015 | 2016 | 2017 | All | |
|---|---|---|---|---|---|---|
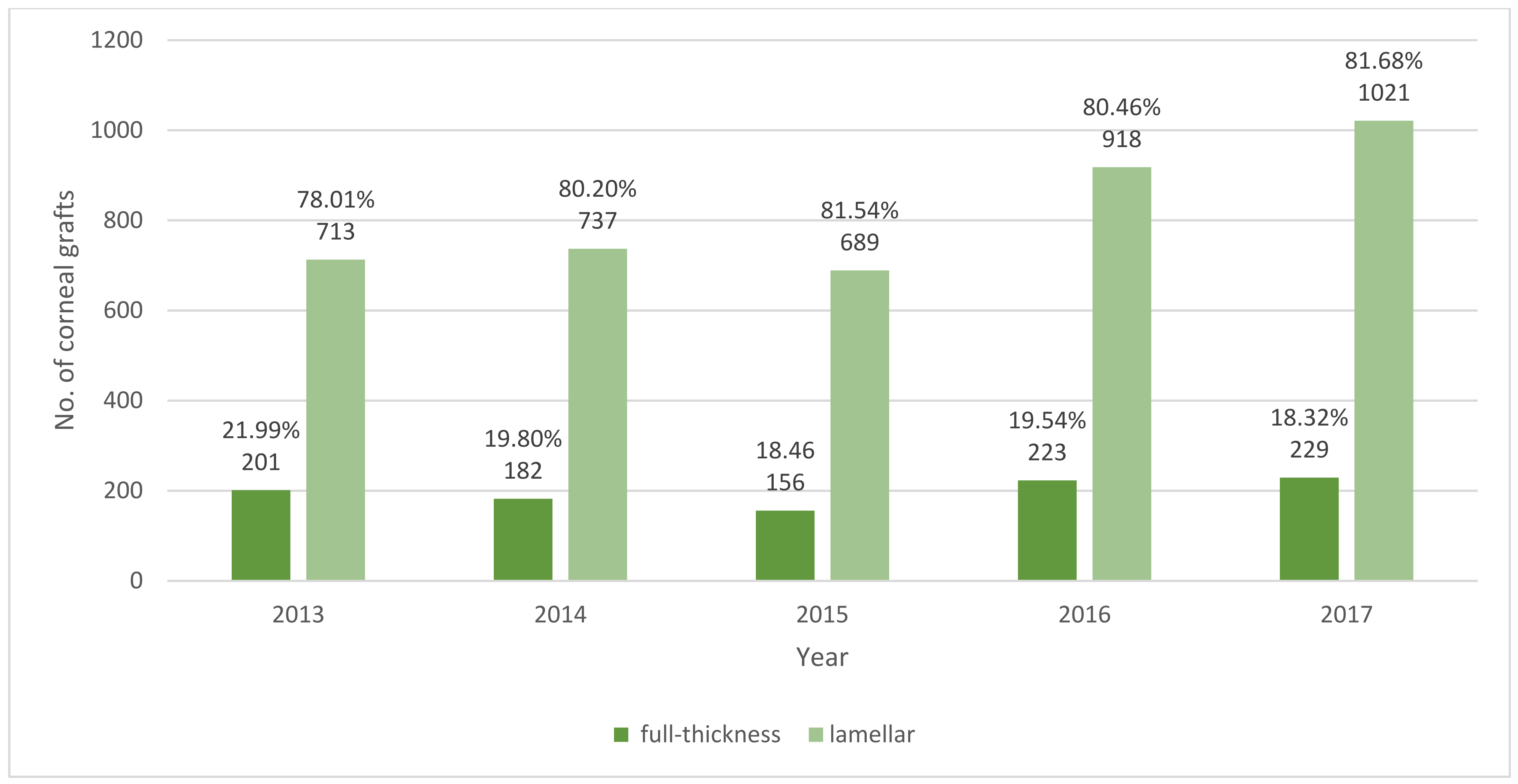
| No. of full-thickness corneal grafts (%) | 201 (21.99%) | 182 (19.8%) | 156 (18.46%) | 223 (19.54%) | 229 (18.32%) | 991 (19.55%) |
| No. of lamellar corneal grafts (%) | 713 (78.01%) | 737 (80.2%) | 689 (81.54%) | 918 (80.46%) | 1021 (81.68%) | 4078 (80.45%) |
| No. of corneal grafts combined with cataract surgery (%) | 187 (20.46%) | 193 (21%) | 160 (18.93%) | 214 (18.76%) | 220 (17.6%) | 997 (19.39%) |
| No. corneal grafts combined with glaucoma surgery (%) | 5 (0.55%) | 9 (0.98%) | 5 (0.59%) | 3 (0.26%) | 5 (0.4%) | 27 (0.52%) |
| No. of corneal grafts combined with PPV (%) | 14 (1.53%) | 10 (1.09%) | 14 (1.66%) | 9 (0.79%) | 27 (2.16%) | 74 (1.44%) |
| No. of corneal grafts in urgent admission (%) | 474 (51.86%) | 553 (60.17%) | 570 (67.46%) | 696 (61.00%) | 739 (59.12%) | 3032 (59.81%) |
| OR | 95% CI | p-Value | |
|---|---|---|---|
| DM type (no) | reference | ||
| Type 1 DM | 1.01 | (0.63; 1.64) | 0.976 |
| Type 2 DM | 1.05 | (0.9; 1.23) | 0.498 |
| Type—partial | reference | ||
| Type—full | 11.54 | (10.08; 18.58) | 0.000 * |
| Age 0–18 | reference | ||
| Age 19–39 | 0.45 | (0.27; 0.72) | 0.001 * |
| Age 40–49 | 0.49 | (0.29; 0.79) | 0.004 * |
| Age 50–59 | 0.49 | (0.3; 0.78) | 0.004 * |
| Age 60–69 | 0.44 | (0.27; 0.69) | 0.001 * |
| Age 70+ | 0.35 | (0.21; 0.54) | 0.000 * |
| Combined (no) | reference | ||
| Combined (yes) | 0.82 | (0.70; 0.96) | 0.011 * |
| Sex (man) | reference | ||
| Sex (woman) | 1 | (0.88; 1.13) | 0.959 |
| Residence (rural) | reference | ||
| Residence (urban) | 0.91 | (0.8; 1.04) | 0.168 |
| Comorbidity Variable | No. of People on the Waiting List | Comorbidity Variable | No. of People on the Waiting List |
|---|---|---|---|
| Age | 62.05 ± 19.00 | Fluid and electrolyte disorders | 176 (2.22%) |
| Sex (women) | 4144 (52.30%) | AIDS/HIV | 0 (0.00%) |
| Urban | 5466 (69.10%) | Hypothyroidism | 809 (10.21%) |
| Alcohol abuse | 206 (2.60%) | Hypertension | 4770 (60.21%) |
| Blood loss anaemia | 21 (0.27%) | Liver disease | 220 (2.78%) |
| Arrhythmias | 1436 (18.13%) | Lymphoma | 42 (0.53%) |
| Solid tumor without metastasis | 654 (8.26%) | Metastatic cancer | 53 (0.67%) |
| Congestive heart failure | 1297 (16.37%) | Other neurological disorders | 352 (4.44%) |
| Coagulopathy | 76 (0.96%) | Obesity | 210 (2.65%) |
| Chronic pulmonary disease | 1241 (15.67%) | Paralysis | 69 (0.87%) |
| Deficiency anaemia | 169 (2.13%) | Pulmonary circulation disorders | 81 (1.02%) |
| Type 1 Diabetes | 104 (1.31%) | Psychoses | 91 (1.15%) |
| Type 2 Diabetes | 1555 (19.63%) | Peptic ulcer disease excluding bleeding | 52 (0.66%) |
| Depression | 613 (7.74%) | Peripheral vascular disorders | 1335 (16.85%) |
| Drug abuse | 47 (0.59%) | Renal failure | 422 (5.33%) |
| Fluid and electrolyte disorders | 176 (2.22%) | Rheumatoid arthritis/ collagen vascular diseases | 460 (5.81%) |
| AIDS/HIV | 0 (0.00%) | Valvular disease | 356 (4.49%) |
| Hypothyroidism | 809 (10.21%) | Weight loss | 45 (0.57%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozioł, M.; Nowak, M.S.; Udziela, M.; Szaflik, J.P. The Association between Diabetes Mellitus and Keratoplasty in Poland in the Years 2013–2017. Int. J. Environ. Res. Public Health 2021, 18, 9767. https://doi.org/10.3390/ijerph18189767
Kozioł M, Nowak MS, Udziela M, Szaflik JP. The Association between Diabetes Mellitus and Keratoplasty in Poland in the Years 2013–2017. International Journal of Environmental Research and Public Health. 2021; 18(18):9767. https://doi.org/10.3390/ijerph18189767
Chicago/Turabian StyleKozioł, Milena, Michał Szymon Nowak, Monika Udziela, and Jacek Paweł Szaflik. 2021. "The Association between Diabetes Mellitus and Keratoplasty in Poland in the Years 2013–2017" International Journal of Environmental Research and Public Health 18, no. 18: 9767. https://doi.org/10.3390/ijerph18189767
APA StyleKozioł, M., Nowak, M. S., Udziela, M., & Szaflik, J. P. (2021). The Association between Diabetes Mellitus and Keratoplasty in Poland in the Years 2013–2017. International Journal of Environmental Research and Public Health, 18(18), 9767. https://doi.org/10.3390/ijerph18189767