
User Requirements Analysis of an Embodied Conversational Agent for Coaching Older Adults to Choose Active and Healthy Ageing Behaviors during the Transition to Retirement: A Cross-National User Centered Design Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
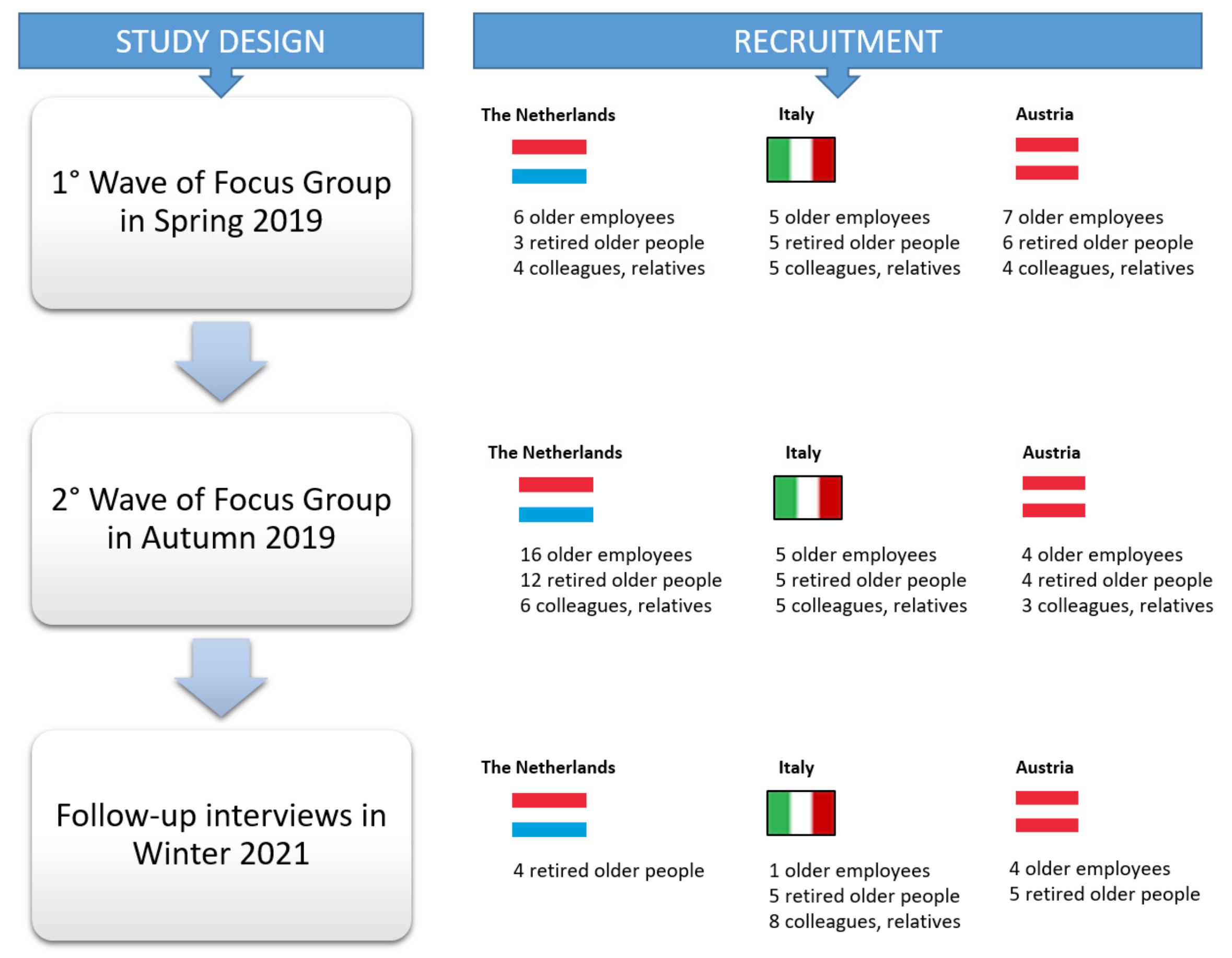
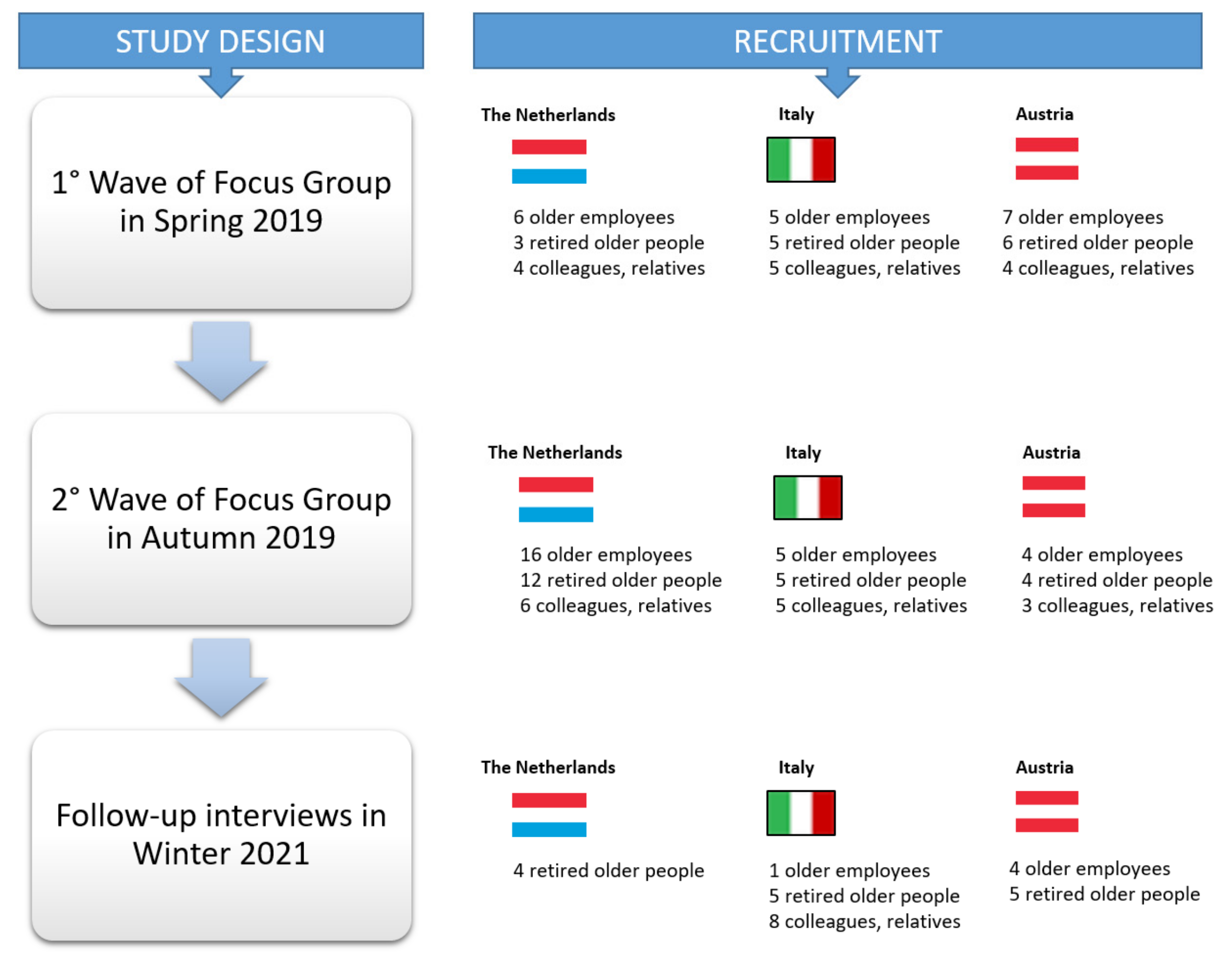
2.1. Study Design
2.2. Participants’ Inclusion Criteria and Recruitment Strategy
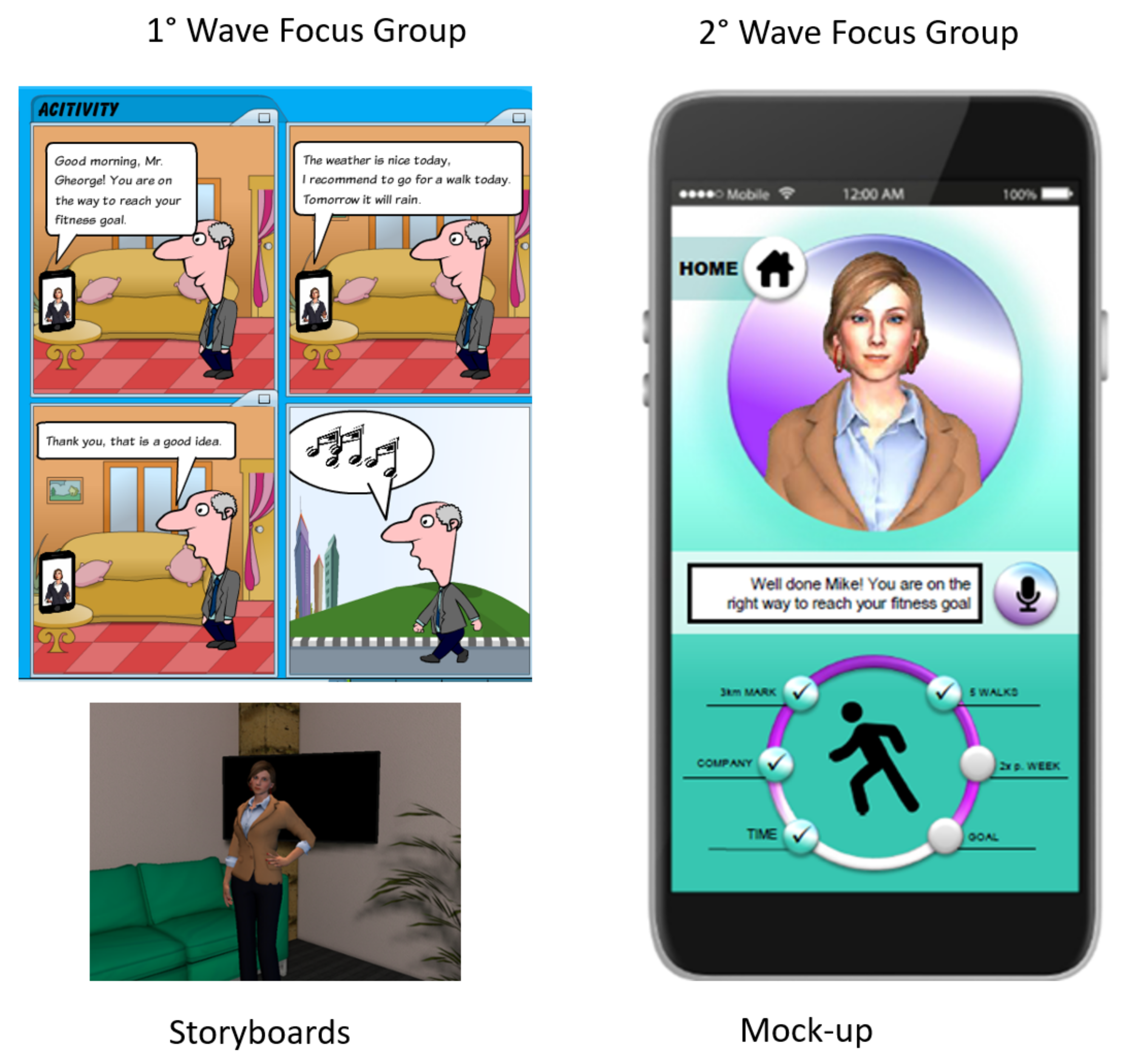
2.3. Data Collection Methodology and Tools
2.4. Data Analysis Methodology
3. Results
3.1. Participants’ Description
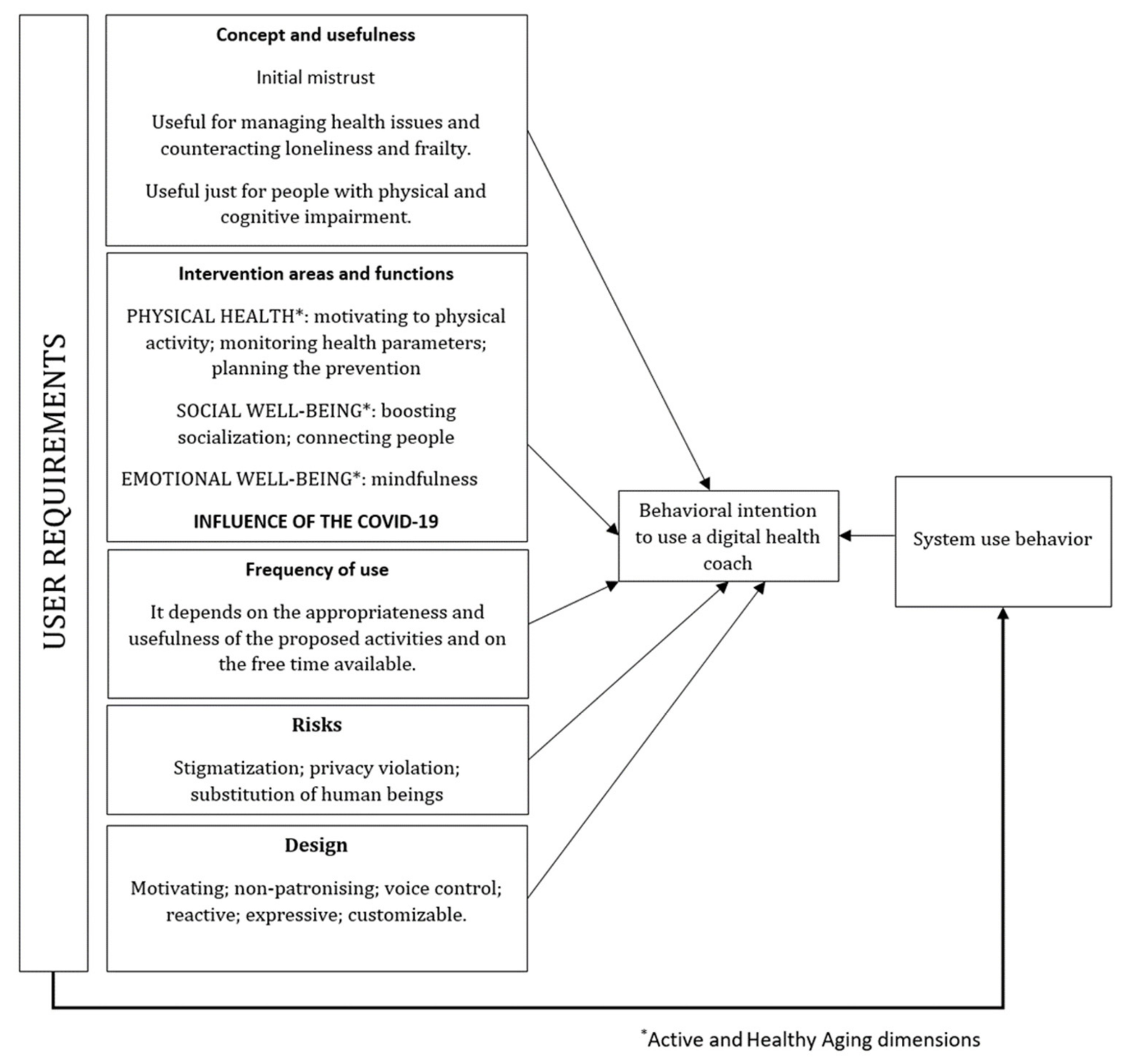
3.2. Overview of User Requirements as Determinants of Use S of a VC
3.3. What Are the User Requirements of a VC Based on an ECA for Motivating Older Adults in Transition to Retirement to Adopt a Healthy Lifestyle?
3.3.1. End-Users’ Feelings on the Concept and Usefulness of the Coaching System
3.3.2. End-Users’ Opinion on the Intervention Areas of the Virtual Coach
3.3.3. End-Users’ Opinions on the Frequency of Use of the Virtual Coach
3.3.4. End-Users’ Opinions on the Risks of the Virtual Coach
3.3.5. Design of the ECA
3.4. How Can a Virtual Coach System Address The Active and Healthy Ageing Dimensions, Even at COVID-19 Times?
3.4.1. The VC Functions Promoting Physical Health
3.4.2. The VC Functions Promoting Emotional Well-Being
3.4.3. The VC Functions Promoting Social Relationships and Participation
3.4.4. The Influence of the COVID-19 Outbreak on the End-Users’ Opinions about the Virtual Coach’s Coach Functions
4. Discussion
4.1. What Are the User Requirements of a VC Based on an ECA for Motivating Older Adults in Transition to Retirement to Adopt a Healthy Lifestyle?
4.2. How Can a Virtual Coach System Address The Active and Healthy Ageing Dimensions, Even at COVID-19 Time?
4.3. Suggestions for Future Design and Research
4.4. Study Limitations and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Issues | Questions |
|---|---|
| Feelings and needs on retirement (retirement representations) |
|
| Concept: feelings and needs regarding the coaching system |
|
| Functions and services |
|
| Appearance and usage |
|
| Issues | Questions |
|---|---|
| Frequency of use of the ECA in daily life |
|
| Design and usability |
|
| Tasks, functions and usefulness |
|
| Appearance |
|
| Issues | Questions |
|---|---|
| Physical health |
|
| Emotional well-being |
|
| Social inclusion/participation |
|
References
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: France, Paris, 2019; ISBN 9789264807662. [Google Scholar]
- Almirall, J.; Fortin, M. The coexistence of terms to describe the presence of multiple concurrent diseases. J. Comorb. 2013, 8, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Navickas, R.; Petric, V.K.; Feigl, A.B.; Seychell, M. Multimorbidity: What do we know? What should we do? J. Comorb. 2016, 17, 4–11. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, S.R.; Versnel, N.; Lemmens, L.C.; Molema, C.C.; Schellevis, F.G.; Nijpels, G.; Baan, C.A. Comprehensive care programs for patients with multiple chronic conditions: A systematic literature review. Health Policy 2012, 107, 108–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onder, G.; Palmer, K.; Navickas, R.; Jurevičienė, E.; Mammarella, F.; Strandzheva, M.; Mannucci, P.; Pecorelli, S.; Marengoni, A. Joint Action on Chronic Diseases and Promoting Healthy Aging across the Life Cycle (JA-CHRODIS). Time to face the challenge of multimorbidity. A European perspective from the joint action on chronic diseases and promoting healthy aging across the life cycle (JA-CHRODIS). Eur. J. Int. Med. 2015, 26, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, determinants and patterns of multimorbidity in primary care: A systematic review of observational studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef]
- World Health Organization. Basic Documents: Forty-Ninth Edition (Including Amendments Adopted up to 31 May 2019); World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000052-0. [Google Scholar]
- Sowa, A.; Tobiasz-Adamczyk, B.; Topór-Mądry, R.; Poscia, A.; la Milia, D.I. Predictors of healthy aging: Public health policy targets. BMC Health Serv. Res. 2016, 16 (Suppl. 5), 289. [Google Scholar] [CrossRef] [PubMed]
- Walker, A. The Future of Aging in Europe; Palgrave Macmillan: Basingtoke, UK, 2019; ISBN 9789811314162. [Google Scholar]
- World Health Organization. Active Aging: A Policy Framework. 2002. Available online: https://apps.who.int/iris/handle/10665/67215 (accessed on 2 August 2021).
- World Health Organization. World Report on Aging and Health; World Health Organization: Geneva, Switzerland, 2015; ISBN 9789240694811. [Google Scholar]
- Bosch-Farré, C.; Garre-Olmo, J.; Bonmatí-Tomàs, A.; Malagón-Aguilera, M.C.; Gelabert-Vilella, S.; Fuentes-Pumarola, C.; Juvinyà-Canal, D. Prevalence and related factors of Active and Healthy Aging in Europe according to two models: Results from the Survey of Health, Aging and Retirement in Europe (SHARE). PLoS ONE 2018, 13, 1–19. [Google Scholar] [CrossRef]
- European Commission. Green Paper on Aging. 2021. Available online: https://ec.europa.eu/info/sites/info/files/1_en_act_part1_v8_0.pdf (accessed on 2 August 2021).
- Marmot, M.; Wilkinson, R.G. Health and the psychosocial environment at work. In Social Determinants of Health, 2nd ed.; Marmot, M., Wilkinson, R.G., Eds.; Oxford University Press: Strasbourg, France, 2006; ISBN 9780198565895. [Google Scholar]
- Tobiasz-Adamczyk, B.; Brzyski, P. Psychosocial work conditions as predictors of quality of life at the beginning of older age. Int. J. Occup. Med. Environ. Health 2005, 18, 43–52. [Google Scholar] [PubMed]
- Lynch, J.; Smith, G.D. A life course approach to chronic disease epidemiology. Annu. Rev. Public Health 2005, 26, 1–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osler, M. The life course perspective: A challenge for public health research and prevention. Eur. J. Public Health 2006, 16, 230. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.M. A comparison of young, middle-aged, and older adult treatment-seeking pathological gamblers. Gerontologist 2002, 42, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Tun, S.Y.Y.; Madanian, S.; Parry, D. Clinical Perspective on Internet of Things Applications for Care of the Elderly. Electronics 2020, 9, 1925. [Google Scholar] [CrossRef]
- Lahti, J.; Laaksonen, M.; Lahelma, E.; Rahkonen, O. Changes in leisure-time physical activity after transition to retirement: A follow-up study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 36. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 2 August 2021).
- Hershenson, D.B. Reconceptualizing retirement: A statuses-based approach. J. Aging Stud. 2016, 38, 1–5. [Google Scholar] [CrossRef]
- Lucas, A.; Daniel, F.; Guadalupe, S.; Massano-Cardoso, I.; Vicente, H. Time spent in retirement, health and well-being. Eur. Psychiatry 2017, 41, 339–340. [Google Scholar] [CrossRef]
- Wetzel, M.; Huxhold, O.; Tesch-Römer, C. Transition into Retirement Affects Life Satisfaction: Short- and Long-Term Development Depends on Last Labor Market Status and Education. Soc. Indic. Res. 2016, 125, 991–1009. [Google Scholar] [CrossRef]
- Atchley, R.C. The Sociology of Retirement, 1st ed.; John Wiley & Sons Inc.: New York, NY, USA, 1976; ISBN 0470035978. [Google Scholar]
- Wang, M.; Henkens, K.; Van Solinge, H. Retirement adjustment: A review of theoretical and empirical advancements. Am. Psychol. 2011, 66, 204–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolodziej, I.W.K.; García-Gómez, P. Saved by retirement: Beyond the mean effect on mental health. Soc. Sci. Med. 2019, 225, 85–97. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.; Heraty, N.; Cross, C.; Cleveland, J. Who is considered an ‘older worker’? Extending our conceptualisation of ‘older’ from an organisational decision maker perspective. Hum. Resour. Manag. J. 2014, 24, 374–393. [Google Scholar] [CrossRef] [Green Version]
- Santini, S.; Socci, M.; Principi, A. Health and wellbeing during the transition to retirement: The more the fears the less the actions? In Proceedings of the Third ISA Conference, Vienna, Austria, 10–14 July 2016; Book of abstract: 238. Available online: https://isaconf.confex.com/isaconf/forum2016/webprogram/Paper76971 (accessed on 2 August 2021).
- Vichitvanichphong, S.; Talaei-Khoei, A.; Kerr, D.; Ghapanchi, A.H. Adoption of assistive technologies for aged care: A realist review of recent studies. In Proceedings of the 47th Hawaii International Conference on System Sciences (HICSS), Waicoloa, HI, USA, 6–9 January 2014; pp. 2706–2715. [Google Scholar] [CrossRef]
- De Angeli, A.; Jovanović, M.; McNeill, A.; Coventry, L. Desires for active aging technology. Int. J. Hum. Comput. Stud. 2020, 138, 102412. [Google Scholar] [CrossRef]
- Schneider, C.; Trukeschitz, B.; Rieser, H. Measuring the Use of the Active and Assisted Living Prototype CARIMO for Home Care Service Users: Evaluation Framework and Results. Appl. Sci. 2020, 101, 38. [Google Scholar] [CrossRef] [Green Version]
- Bevilacqua, R.; Casaccia, S.; Cortellessa, G.; Astell, A.; Lattanzio, F.; Corsonello, A.; D’Ascoli, P.; Paolini, S.; Di Rosa, M.; Rossi, L.; et al. Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Aging Population. Int. J. Environ. Res. Public Health 2020, 17, 5930. [Google Scholar] [CrossRef] [PubMed]
- Stara, V.; Santini, S.; Kropf, J.; D’Amen, B. Exploring the effectiveness of digital health coaching programs among older employees in transition to retirement: A systematic literature review. J. Med. Internet Res. 2020, 22, e17809. [Google Scholar] [CrossRef]
- Cook, R.F.; Hersch, R.K.; Schlossberg, D.; Leaf, S.L. A web-based health promotion program for older workers: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e82. [Google Scholar] [CrossRef] [PubMed]
- Irvine, A.B.; Gelatt, V.A.; Seeley, J.R.; Macfarlane, P.; Gau, J.M. Web-based intervention to promote physical activity by sedentary older adults: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e19. [Google Scholar] [CrossRef] [Green Version]
- Seifert, A.; Cotton, S.R.; Xie, B. A Double Burden of Exclusion? Digital and Social Exclusion of Older Adults in Times of COVID-19. J. Gerontol. Ser. B 2021, 76, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Kramer, L.L.; Ter Stal, S.; Mulder, B.C.; De Vet, E.; Van Velsen, L. Developing Embodied Conversational Agents for Coaching People in a Healthy Lifestyle: Scoping Review. J. Med. Internet Res. 2020, 22, e14058. [Google Scholar] [CrossRef] [PubMed]
- Provoost, S.; Lau, H.M.; Ruwaard, J.; Riper, H. Embodied conversational agents in clinical psychology: A scoping review. J. Med. Internet Res. 2017, 19, e151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luria, M.; Reig, S.; Tan, X.Z.; Steinfeld, A.; Forlizzi, J.; Zimmerman, J. Re-embodiment and co-embodiment: Exploration of social presence for robots and conversational agents. In Proceedings of the DIS 2019 International Conference on Designing Interactive Systems, San Diego, CA, USA, 23–28 June 2019; ACM Press: San Diego, CA, USA, 2019; pp. 633–644. [Google Scholar] [CrossRef]
- Stal, S.; Kramer, L.L.; Tabak, M.; Akker, O.D.H.; Hermens, H. Design features of embodied conversational agents in eHealth: A literature review. Int. J. Hum. Comput. Stud. 2020, 138, 102409. [Google Scholar] [CrossRef]
- Czaja, S.; Boot, W.; Charness, N.; Rogers, W. Individual differences. In Designing for Older Adults: Principles and Creative Human Factors Approaches, 3rd ed.; Czaja, S., Boot, W., Charness, N., Rogers, W., Eds.; CRC press: Boca Raton, FL, USA, 2019; pp. 33–47. ISBN 9781138053663. [Google Scholar]
- Davis, F.D.; Venkatesh, V. Toward Preprototype User Acceptance Testing of New Information Systems: Implications for Software Project Management. IEEE Trans. Eng. Manag. 2004, 31–46. [Google Scholar] [CrossRef]
- Kim, S.S.; Malhotra, N.K. A Longitudinal Model of Continued IS Use: An Integrative View of Four Mechanisms Underlying Post-Adoption Phenomena. Manag. Sci. 2005, 741–755. [Google Scholar] [CrossRef]
- Limayem, M.; Hirt, S.G.; Cheung, C.M.K. How Habit Limits the Predictive Power of Intentions: The Case of IS Continuance. MIS Q. 2007, 705–737. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Thong, J.Y.L.; Xu, X. Consumer acceptance and use of information technology. Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Ergonomics of Human-System Interaction—Part 210: Human-Centred Design for Interactive Systems. ISO 9241-210:2010. Available online: http://www.iso.org/iso/catalogue_detail.htm?csnumber=52075 (accessed on 22 May 2021).
- Chung, S.; Domino, M.E.; Stearns, S.C.; Popkin, B.M. Retirement and physical activity: Analyses by occupation and wealth. Am. J. Prev. Med. 2009, 36, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Noble, H.; Smith, J. Issues of validity and reliability in qualitative research. Evid. Based Nurs. 2015, 18, 34–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuckartz, U. Realizing Mixed-Methods Approach with MAXQDA. Available online: https://www.maxqda.com/download/MixMethMAXQDA-Nov01-2010.pdf (accessed on 2 August 2021).
- DeSantis, L.; Ugarriza, D.N. The Concept of Theme as Used in Qualitative Nursing Research. West. J. Nurs. Res. 2000, 22, 351–372. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Bondas, T.; Turunen, H. Content Analysis and Thematic Analysis: Implications for Conducting a Qualitative Descriptive Study. J. Nurs. Health Sci. 2013, 5, 398–405. [Google Scholar] [CrossRef]
- Plat, S. Thematic Analysis Software: How It Works & Why You Need It. Available online: https://getthematic.com/insights/thematic-analysis-software/ (accessed on 2 August 2021).
- Mayring, P. Qualitative Content Analysis. Forum Qual Soc Res 2000. 1. Available online: http://qualitative-reserach.net/fqs/fqs-e/2-00inhalt-e.htm (accessed on 28 June 2021).
- Moretti, F.; Vliet van, L.; Benzing, J.; Deledda, G.; Mazzi, M.; Rimondini, M.; Zimmermann, C.; Fletcher, I. A standardized approach to qualitative analysis of focus group discussions from different countries. Patient Educ. Couns. 2011, 82, 420–428. [Google Scholar] [CrossRef] [Green Version]
- Rabiee, F. Focus-group interview and data analysis. Proc. Nutr. Soc. 2004, 63, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Guba, E.G.; Lincoln, Y.S. Competing paradigm in qualitative research. In Handbook of Qualitative Research, 5th ed.; Denzin, N.K., Lincoln, Y.S., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 105–117. [Google Scholar]
- Morse, J.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification strategies for establishing reliability validity in qualitative research. Int. J. Qual. Res. 2002, 1, 1–19. [Google Scholar] [CrossRef]
- Slevin, E.; Sines, D. Enhancing the truthfulness, consistency, and transferability of a qualitative study: Using a manifold of approaches. Nurse Res. 2000, 7, 79–98. [Google Scholar] [CrossRef]
- Fraser, S.; Greenhalgh, T. Coping with complexity: Educating for capability. BMJ 2001, 323, 799–803. [Google Scholar] [CrossRef]
- Sandelowski, M. Rigor or rigor mortis: The problem of rigor in qualitative research revisited. ANS Adv. Nurs. Sci. 1993, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Milne-Ives, M.; de Cock, C.; Lim, E.; Shehadeh, M.H.; de Pennington, N.; Mole, G.; Normando, E.; Meinert, E. The Effectiveness of Artificial Intelligence Conversational Agents in Health Care: Systematic Review. J. Med. Internet Res. 2020, 22, e20346. [Google Scholar] [CrossRef] [PubMed]
- Ghanvatkar, S.; Kankanhalli, A.; Rajan, V. User models for personalized physical activity interventions: Scoping review. J. Med. Internet Res. Mhealth Uhealth 2019, 7, e11098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, H.; Poole, M. What is personalization? perspectives on the design and implementation of personalization in information systems. J. Organ. Comput. Electron. Commer. 2006, 16, 179–202. [Google Scholar] [CrossRef]
- Kocaballi, A.B.; Berkovsky, S.; Quiroz, J.C.; Laranjo, L.; Tong, H.L.; Rezazadegan, D.; Briatore, A.; Coiera, E. The Personalization of Conversational Agents in Health Care: Systematic Review. J. Med. Internet Res. 2019, 21, e15360. [Google Scholar] [CrossRef] [Green Version]
- Cheetham, M. The Uncanny Valley Hypothesis and beyond. Front. Psychol. 2017, 8, 1738. [Google Scholar] [CrossRef] [Green Version]
- Tschöpe, N.; Reiser, J.; Oehl, M. Exploring the Uncanny Valley Effect in Social Robotics. In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction (HRI ‘17), New York, NY, USA, 6–9 March 2017; Association for Computing Machinery: New York, NY, USA; pp. 307–308. [Google Scholar] [CrossRef]
- Schmied, M.; Igerc, I.; Schneider, C. A Digital Health Coach for Younger Seniors—User Centred Requirements Collection. Stud. Health Technol. Inform. 2020, 271, 137–144. [Google Scholar] [CrossRef]
| Wave 1 | Older Workers | Retirees | Colleagues Relatives | Total Country | Male | Female | Mean Age |
| Austria | 7 | 6 | 4 | 17 | 7 | 10 | 59 |
| Italy | 5 | 5 | 5 | 15 | 7 | 8 | 59.8 |
| The Netherlands | 6 | 3 | 4 | 13 | 7 | 6 | 65.6 |
| Total | 18 | 14 | 13 | 45 | 21 | 24 | 61.4 |
| Wave 2 | Older Workers | Retirees | Colleagues Relatives | Total Country | Male | Female | Mean Age |
| Austria | 4 | 4 | 3 | 11 | 7 | 4 | 57 |
| Italy | 5 | 5 | 5 | 15 | 7 | 8 | 59.8 |
| The Netherlands | 16 | 12 | 6 | 34 | 15 | 19 | 64 |
| Total | 25 | 21 | 14 | 60 | 29 | 31 | 60.2 |
| Country | Gender | Mean Age | Interviewees | Total | |||
|---|---|---|---|---|---|---|---|
| Male | Female | Retirees | Colleagues of Retirees | Older Workers | |||
| Austria | 4 | 5 | 60.2 | 5 | 0 | 4 | 9 |
| Italy | 6 | 8 | 60 | 5 | 8 | 1 | 14 |
| The Netherlands | 3 | 1 | 65.5 | 4 | 0 | 0 | 4 |
| Total | 13 | 14 | 61.9 | 14 | 8 | 5 | 27 |
| RQ1 Which Are the User Requirements of a VC Based on an ECA for Training Older Adults in Transition to Retirement and Motivating Them to Adopt Healthy Lifestyle? | RQ2 How Can a VC Mirror the Healthy Ageing Dimensions, Especially during COVID-19 Times? | ||
|---|---|---|---|
| User Requirements Themes | Codes | User Requirements Themes | Codes |
| End-users’ opinion on the VC functions | Encouraging healthy lifestyle (A and NL). Supporting financial planning and concrete activities of retirees (NL). Supporting older people during the transition for managing financial aspects, social activities, health and life style, legal issues (A, IT). Helping people with physical and cognitive limitations (NL). Use of the virtual coach at company level for informing older workers on retirement legal and financial issues (IT). Virtual coach running on portable device (A, IT, NL). Stimulating retirees’ socialization, interests and brain activities (IT). | Physical activity functions | Monitoring end-users’ health (A) Motivating older workers and retirees to practice physical activity (A, IT, NL). Customising physical activities especially for people with special chronic disease (A). Reminding and planning health prevention and screening appointments (IT). Stimulating brain activity (A, NL). |
| Frequency of use of the VC | Every day use of the virtual coach (A and NL). The use of the virtual coach depends on the free time available, so it is most for retirees (NL). The use of the virtual coach depends on one’s mood (A). The use of the virtual coach depends on users’ family relationships and social condition (IT). | Emotional well-being functions | Helping older workers and retirees have a meaningful life and find purpose in life. Reduce stress and hindering depression (A, IT, NL). Informing users on retirement legislations. |
| Risks | Stigmatization, privacy violation, substitution of users’ decision making capability (A, IT, NL). | Social relationships functions | Promoting the community construction (IT). Foster retirees’ social relationships (IT). Helping older workers and retirees share and discuss objectives and goals (IT). Promoting the competition among the users for reaching the goals (A, NL). |
| Design of the ECA | Voice control and setting (A, IT, NL). Reactive (A, IT, NL). Customizable (age, gender, outfit, voice) (A, IT, NL). More expressive and sympathetic (IT). Convincing, motivating and respectful language (i.e., not directive and patronising) (A, IT, NL). Bright and no purple background (IT). Interactive icons giving motivating feedback (e. g. “Well done! You reached your goal!”). Pleasant text field and colours (A, NL). | Useful functions during the COVID-19 outbreak in the 3 realms of health | Encouraging retirees and older workers in smart-working to practice indoor physical and yoga exercises (A, IT, NL). Encouraging retirees re-start going out as soon as possible, according to the restrictions (A, IT, NL). Providing information on movement/social restrictions measures (A, NL). Providing mindfulness exercises, virtual visits, courses and games for emotional well-being (A, IT, NL). Suggesting e-learning opportunities (NL). It might help people ask for social and health support (NL). Creating groups of users based on common interests (e.g., history, bricolage, etc.) (IT). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santini, S.; Stara, V.; Galassi, F.; Merizzi, A.; Schneider, C.; Schwammer, S.; Stolte, E.; Kropf, J. User Requirements Analysis of an Embodied Conversational Agent for Coaching Older Adults to Choose Active and Healthy Ageing Behaviors during the Transition to Retirement: A Cross-National User Centered Design Study. Int. J. Environ. Res. Public Health 2021, 18, 9681. https://doi.org/10.3390/ijerph18189681
Santini S, Stara V, Galassi F, Merizzi A, Schneider C, Schwammer S, Stolte E, Kropf J. User Requirements Analysis of an Embodied Conversational Agent for Coaching Older Adults to Choose Active and Healthy Ageing Behaviors during the Transition to Retirement: A Cross-National User Centered Design Study. International Journal of Environmental Research and Public Health. 2021; 18(18):9681. https://doi.org/10.3390/ijerph18189681
Chicago/Turabian StyleSantini, Sara, Vera Stara, Flavia Galassi, Alessandra Merizzi, Cornelia Schneider, Sabine Schwammer, Elske Stolte, and Johannes Kropf. 2021. "User Requirements Analysis of an Embodied Conversational Agent for Coaching Older Adults to Choose Active and Healthy Ageing Behaviors during the Transition to Retirement: A Cross-National User Centered Design Study" International Journal of Environmental Research and Public Health 18, no. 18: 9681. https://doi.org/10.3390/ijerph18189681
APA StyleSantini, S., Stara, V., Galassi, F., Merizzi, A., Schneider, C., Schwammer, S., Stolte, E., & Kropf, J. (2021). User Requirements Analysis of an Embodied Conversational Agent for Coaching Older Adults to Choose Active and Healthy Ageing Behaviors during the Transition to Retirement: A Cross-National User Centered Design Study. International Journal of Environmental Research and Public Health, 18(18), 9681. https://doi.org/10.3390/ijerph18189681