
Did “Kayoinoba” Prevent the Decline of Mental and Physical Functions and Frailty for the Home-Based Elderly during the COVID-19 Pandemic?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Respondents
2.2. Operation of “Kayoinoba” under Self-Quarantine, Due to the Spread of COVID-19
2.3. Evaluation of Mental and Physical Function and Frailty
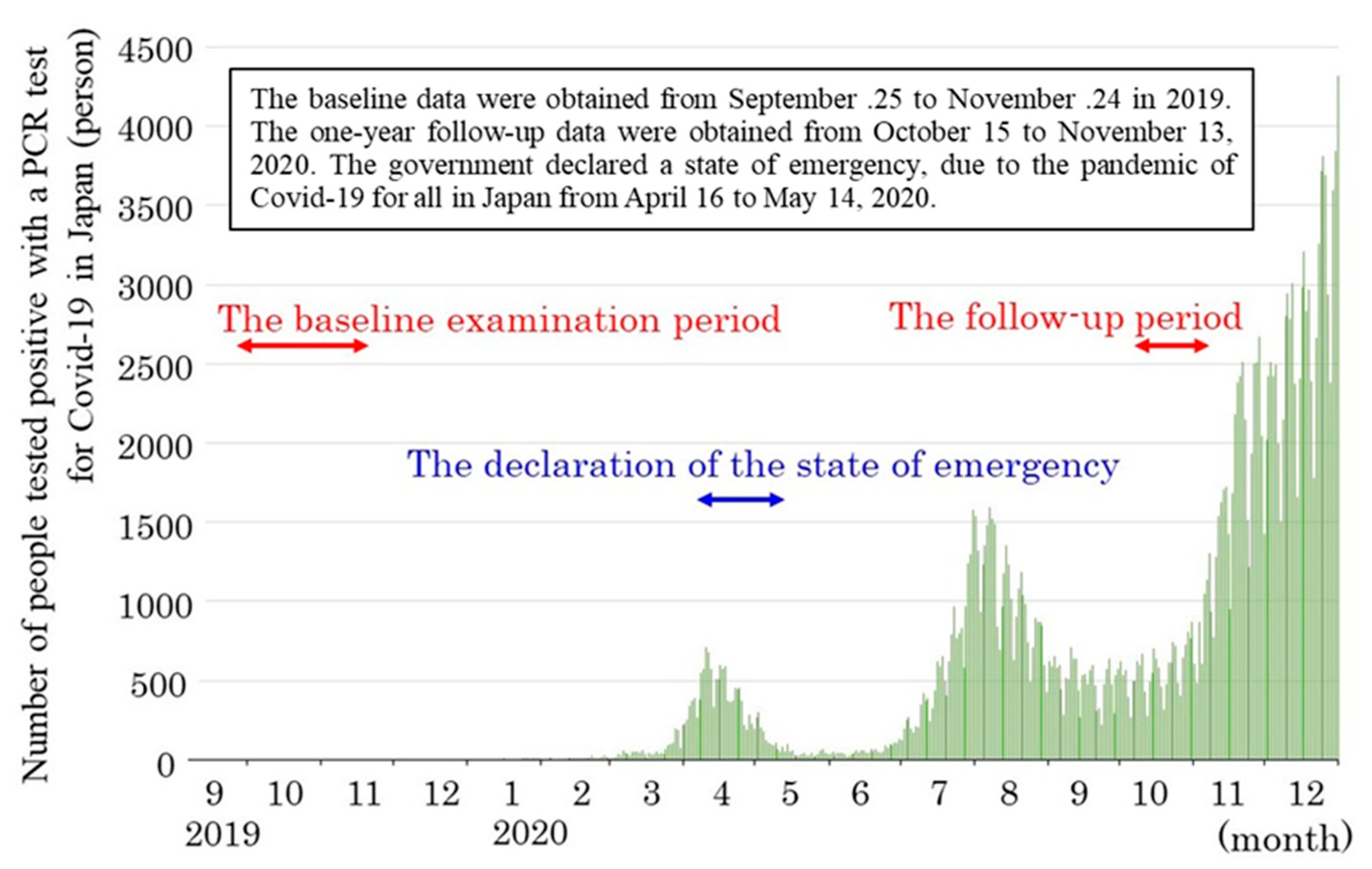
2.4. Survey Time and Method
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Morgan, V.; Birtus, M.; Zauskova, A. Medical Internet of Things-based Healthcare Systems, Wearable Biometric Sensors, and Personalized Clinical Care in Remotely Monitoring and Caring for Confirmed or Suspected COVID-19 Patients. Am. J. Med. Res. 2021, 8, 81–90. [Google Scholar]
- Bailey, L. Wearable Internet of Things Healthcare Systems, Virtual Care, and Real-Time Clinical Monitoring in Assessing and Treating Patients with COVID-19 Symptoms. Am. J. Med. Res. 2021, 8, 91–100. [Google Scholar]
- Campbell, K. Smart Telemedicine Diagnosis Systems, Biomedical Big Data, and Telehealth Outpatient Monitoring in COVID-19 Screening, Testing, and Treatment. Am. J. Med.Res. 2021, 8, 101–111. [Google Scholar]
- Newburn, F. Gender Differences in Behavior and Attitudes toward COVID-19: Perceived Risk of Infection, Negative Cognitive Emotions, and Sleep Disturbances. J. Res. Gend. Stud. 2020, 10, 117–127. [Google Scholar]
- Sampson, G. Gender-based Differences of Contagious Negative Emotions, Notable Psychological Distress, and Mental Health Burden during the COVID-19 Outbreak. J. Res. Gend. Stud. 2020, 10, 128–137. [Google Scholar]
- Crawford, S. Gender-related Irritability, Confusion, Anger, and Frustration Associated with COVID-19 Infection and Mortality. J. Res. Gend. Stud. 2020, 10, 138–147. [Google Scholar]
- Shinohara, T.; Saida, K.; Tanaka, S.; Murayama, A. Do lifestyle measures to counter COVID-19 affect frailty rates in elderly community dwelling? Protocol for cross-sectional and cohort study. BMJ Open 2020, 10, e040341. [Google Scholar] [CrossRef]
- Shinohara, S.; Saida, K.; Tanaka, S.; Murayama, A. Association between frailty and changes in lifestyle and physical or psychological conditions among older adults affected by the coronavirus disease 2019 countermeasures in Japan. Geriatr. Gerontol. Int. 2021, 21, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Fujiwara, Y.; Kumagai, S.; Watanabe, S.; Yoshida, Y.; Motohashi, Y.; Shinkai, S. The frequency of going outdoors, and physical, psychological and social functioning among community-dwelling older adults. Jpn. J. Public Health 2004, 51, 168–180. [Google Scholar]
- Annual Report on the Aging Society. 2020. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2020/pdf/2020.pdf (accessed on 23 May 2021).
- Arai, H. Significance of frailty. Jpn. J. Geriatr. 2014, 51, 497–501. [Google Scholar]
- Iijima, K. Elderly people and society: Including oral frailty. J. Jpn. Soc. Int. Med. 2018, 107, 2469–2477. [Google Scholar] [CrossRef] [Green Version]
- Murayama, H.; Kobayashi, E.; Okamoto, S.; Fukaya, T.; Ishizaki, T.; Liang, J.; Shinkai, S. National prevalence of frailty in the older Japanese population: Findings from a nationally representative survey. Arch. Gerontol. Geriatr. 2020, 91, 104220. [Google Scholar] [CrossRef]
- Shimada, H.; Makizato, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Guideline for Promoting Care Prevention through Community Development. 2017. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-12300000-Roukenkyo\wku/0000166414.pdf (accessed on 29 May 2021).
- Haseda, M.; Takagi, D.; Kondo, K.; Kondo, N. Effectiveness of community organizing interventions on social activities among older residents in Japan: A JAGES quasi-experimental study. Soc. Sci. Med. 2019, 240, 112527. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef] [PubMed]
- Satake, S. Kihon checklist and frailty. Jpn. J. Geriatr. 2018, 55, 319–328. [Google Scholar]
- Morita, Y.; Arai, T.; Fujita, H.; Watanabe, S. Two-year changes in the Kihon Checklist and initiations of long-term care in community-dwelling elderly. Rigakuryoho Kagaku 2021, 36, 7–14. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toda, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Ogawa, K.; Fujiwara, Y.; Yoshida, H.; Nishi, M.; Fukaya, T.; Kim, M.; Amano, H.; Lee, S.; Watanabe, N.; Shinkai, S. The validity of the “Kihon Check-list” as an index of frailty and its biomarkers and inflammatory markers in elderly people. Jpn. J. Geriatr. 2011, 48, 545–552. [Google Scholar] [CrossRef]
- Haberman, S.J. The analysis of residuals in cross-classified tables. Biometrics 1973, 29, 205–220. [Google Scholar] [CrossRef]
- Rubin, D.B.; Schenker, N. Multiple imputation in health-care databases: An overview and some applications. Stat. Med. 1991, 10, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, M.; Shirayama, Y.; Yanagisawa, S. Tendency in health and living function of the elderly who participate in “kayoinoba”: Comparison due to differences in program content. Journal of Sikoku Public Health Society. 2021, 66, 73–77. [Google Scholar]
- Ohashi, M.; Yoda, T.; Imai, N.; Fujii, T.; Watanabe, K.; Tashi, H.; Shibuya, Y.; Watanabe, J.; Endo, N. Five-year longitudinal study of frailty prevalence and course assessed using the Kihon Checklist among community-dwelling older adults in Japan. Res. Sq. 2020, 11, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kulmala, J.; Nykanen, I.; Hartikainen, S. Frailty as a predictor of all-cause mortality in older men and women. Geriatr. Gerontol. Int. 2014, 14, 899–905. [Google Scholar] [CrossRef]
- Peterson, M.J.; Guiliani, C.; Morey, M.C.; Pieper, C.F.; Evenson, K.R.; Mercer, V.M.; Cohen, H.J.; Visser, M.; Kritchevsky, S.B.; Goodpaster, B.H.; et al. Physical activity as a preventive factor for frailty: The health, aging, and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Demirtas, H.; Hedeker, D. An imputation strategy for incomplete longitudinal ordinal data. Stat. Med. 2008, 27, 4086–4093. [Google Scholar] [CrossRef]
- Graham, J.W.; Schafer, J.L. On the Performance of Multiple Imputation for Multivariate Data with Small Sample Size; Statistical Strategies for Small Sample Research; Hoyle, R., Ed.; Sage: Thousand Oaks, CA, USA, 1999; pp. 1–29. [Google Scholar]



{kind=link}
{kind=link}
| No. | Question | Answer | |
| 1 | Do you go out by bus or train by yourself? | 0. Yes | 1. No |
| 2 | Do you go shopping to buy your daily necessities by yourself? | 0. Yes | 1. No |
| 3 | Do you manage your own deposits and savings at the bank? | 0. Yes | 1. No |
| 4 | Do you sometimes visit your friends? | 0. Yes | 1. No |
| 5 | Do you tum to your family or friends for advice? | 0. Yes | 1. No |
| 6 | Do you normally climb stairs without using handrails or walls for support? | 0. Yes | 1. No |
| 7 | Do you normally stand up from a chair without any aids? | 0. Yes | 1. No |
| 8 | Do you normally walk continuously for 15 min? | 0. Yes | 1. No |
| 9 | Have you experienced a fall in the past year? | 1. Yes | 0. No |
| 10 | Do you have a fear of falling while walking? | 1. Yes | 0. No |
| 11 | Have you lost 2 kg or more in the past 6 months? | 1. Yes | 0. No |
| 12 | Height: cm, weight: kg, BMI: kg/m² If BMI is less than 18.5, this item is scored | 1. Yes | 0. No |
| 13 | Do you have any difficulties eating tough foods compared to 6 months ago? | 1. Yes | 0. No |
| 14 | Have you choked on your tea or soup recently? | 1. Yes | 0. No |
| 15 | Do you often experience having a dry mouth? | 1. Yes | 0. No |
| 16 | Do you go out at least once a week? | 0. Yes | 1. No |
| 17 | Do you go out less frequently compared to last year? | 1. Yes | 0. No |
| 18 | Do your family or your friends point out your memory loss? E.g., “You always ask the same question over and over again.” | 1. Yes | 0. No |
| 19 | Do you make a call by looking up phone numbers? | 0. Yes | 1. No |
| 20 | Do you find yourself not knowing today’s date? | 1. Yes | 0. No |
| 21 | In the last two weeks have you felt a lack of fulfilment in your daily life? | 1. Yes | 0. No |
| 22 | In the last two weeks have you felt a lack of joy when doing the things you used to enjoy? | 1. Yes | 0. No |
| 23 | In the last two weeks have you felt any difficulty in doing what you could do easily before? | 1. Yes | 0. No |
| 24 | In the last two weeks have you felt helpless? | 1. Yes | 0. No |
| 25 | In the last two weeks have you felt tired without a reason? | 1. Yes | 0. No |
| Domains | Relevant Questions | Cut-Off Point with/without Each Risk | |
| Lifestyle | #1–20 | Ten or more negative answers | |
| Physical function | #6–10 | Three or more negative answers | |
| Nutrition | #11, #12 | Negative answers to both questions | |
| Oral function | #13, #14, #15 | Two or more negative answers | |
| Socialization | #16, #17 | An answer of “No” to #16 | |
| Cognitive function | #18, #19, #20 | One or more negative answers | |
| Depressive mood | #21–25 | Two or more negative answers | |
| Attributes | Numbers (%) |
|---|---|
| Sex | |
| Females | 85 (84.2) |
| Males | 16 (15.8) |
| Age (ys.) | |
| 65–74 | 37 (36.6) |
| ≥75 | 64 (63.4) |
| Living style | |
| Alone | 22 (21.8) |
| Couple | 35 (34.7) |
| with child/children | 44 (43.5) |
| Affluence for living | |
| Affluence | 28 (27.7) |
| Normal | 18 (17.8) |
| Non affluence | 55 (54.5) |
| Everyday | Once a Week | Once a Month | Once a Year | |
|---|---|---|---|---|
| Baseline | 2 (2.0) | 64 (63.4) | 35 (34.6) | 0 (0.0) |
| One-year follow-up | 3 (3.0) | 68 (67.3) | 29 (28.7) | 1 (1.0) |
| Improved | Unchanged | Worsened | Adjusted Residuals for Worsened Transition | |
|---|---|---|---|---|
| Lifestyle | 5 (5.0) | 91 (90.0) | 5 (5.0) | −0.90 |
| Physical function | 13 (12.9) | 75 (74.2) | 13 (12.9) | 2.50 * |
| Nutrition | 0 (0) | 101 (100) | 0 (0) | −3.00 * |
| Oral function | 11 (10.9) | 81 (80.2) | 9 (8.9) | 0.80 |
| Socialization | 4 (4.0) | 94 (93.0) | 3 (3.0) | −1.70 |
| Cognitive function | 19 (18.8) | 71 (70.3) | 11 (10.9) | 1.60 |
| Depressive mood | 15 (14.9) | 77 (76.2) | 9 (8.9) | 0.80 |
| One-Year Follow-Up | |||
|---|---|---|---|
| Robust | Frailty | ||
| Baseline | Robust | 72 (71.3)/6.0 * | 5 (5.0)/−6.0 * |
| Frailty | 9 (8.9)/−6.0 * | 15 (14.9)/6.0 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitamura, M.; Goto, T.; Fujiwara, S.; Shirayama, Y. Did “Kayoinoba” Prevent the Decline of Mental and Physical Functions and Frailty for the Home-Based Elderly during the COVID-19 Pandemic? Int. J. Environ. Res. Public Health 2021, 18, 9502. https://doi.org/10.3390/ijerph18189502
Kitamura M, Goto T, Fujiwara S, Shirayama Y. Did “Kayoinoba” Prevent the Decline of Mental and Physical Functions and Frailty for the Home-Based Elderly during the COVID-19 Pandemic? International Journal of Environmental Research and Public Health. 2021; 18(18):9502. https://doi.org/10.3390/ijerph18189502
Chicago/Turabian StyleKitamura, Mio, Takaharu Goto, Shinji Fujiwara, and Yasuhiko Shirayama. 2021. "Did “Kayoinoba” Prevent the Decline of Mental and Physical Functions and Frailty for the Home-Based Elderly during the COVID-19 Pandemic?" International Journal of Environmental Research and Public Health 18, no. 18: 9502. https://doi.org/10.3390/ijerph18189502
APA StyleKitamura, M., Goto, T., Fujiwara, S., & Shirayama, Y. (2021). Did “Kayoinoba” Prevent the Decline of Mental and Physical Functions and Frailty for the Home-Based Elderly during the COVID-19 Pandemic? International Journal of Environmental Research and Public Health, 18(18), 9502. https://doi.org/10.3390/ijerph18189502