
Improving Social Justice in COVID-19 Health Research: Interim Guidelines for Reporting Health Equity in Observational Studies

 , , , ,
, , , , 
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barr, D. We Are Not All in the Same Boat. We Are All in the Same Storm. 2021. Available online: https://www.damianbarr.com/latest/https/we-are-not-all-in-the-same-boat (accessed on 10 June 2021).
- Bambra, C.; Riordan, R.; Ford, J.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Allen, J. COVID-19: Exposing and amplifying inequalities. J. Epidemiol. Community Health 2020, 74, 681–682. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Addressing Human Rights as Key to the COVID-19 Response. 2021. Available online: https://www.who.int/publications/i/item/addressing-human-rights-as-key-to-the-covid-19-response (accessed on 10 June 2021).
- Burstrom, B.; Tao, W. Social determinants of health and inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef]
- Seligman, B.; Ferranna, M.; Bloom, D.E. Social determinants of mortality from COVID-19: A simulation study using NHANES. PLoS Med. 2021, 18, e1003490. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Kankam, H.K.N.; Majeed, A.; Esmail, A.; Williams, D.R. Mitigating ethnic disparities in covid-19 and beyond. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Germain, S.; Yong, A. COVID-19 Highlighting Inequalities in Access to Healthcare in England: A Case Study of Ethnic Minority and Migrant Women. Fem. Leg. Stud. 2020, 28, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Franco-Paredes, C.; Jankousky, K.; Schultzid, J.; Bernfeld, J.; Cullen, K.; Quan, N.G.; Kon, S.; Hotez, P.; Henao-Martínez, A.F.; Krsak, M. Covid-19 in jails and prisons: A neglected infection in a marginalized population. PLoS Negl. Trop. Dis. 2020, 14, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.C.; Kim, S.; Barberia, L.; Ribeiro, A.F.; Gurzenda, S.; Ribeiro, K.B.; Abbott, E.; Blossom, J.; Rache, B.; Singer, B.H. Spatiotemporal pattern of COVID-19 spread in Brazil. Science 2021, 372, 821–826. [Google Scholar] [CrossRef]
- Wadman, M. Blind spots thwart global coronavirus tracking. Science 2021, 372, 773–774. [Google Scholar] [CrossRef]
- Wright, L.; Steptoe, A.; Fancourt, D. Are we all in this together? Longitudinal assessment of cumulative adversities by socioeconomic position in the first 3 weeks of lockdown in the UK. J. Epidemiol. Community Health 2020, 74, 683–688. [Google Scholar] [CrossRef]
- Tipirneni, R. A Data-Informed Approach to Targeting Social Determinants of Health as the Root Causes of COVID-19 Disparities. Am. J. Public Health 2021, 111, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Pincus, T.; Esther, R.; DeWalt, D.A.; Callahan, L.F. Social conditions and self-management are more powerful determinants of health than access to care. Ann. Intern. Med. 1998, 129, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Sokka, T.; Kautiainen, H.; Pincus, T.; Toloza, S.; da Rocha Castelar Pinheiro, G.; Lazovskis, J.; Hetland, M.L.; Peets, T.; Immonen, K.; Maillefert, J.F.; et al. Disparities in rheumatoid arthritis disease activity according to gross domestic product in 25 countries in the QUEST-RA database. Ann. Rheum. Dis. 2009, 68, 1666–1672. [Google Scholar] [CrossRef] [Green Version]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Filc, D. The medical text: Between biomedicine and hegemony. Soc. Sci. Med. 2004, 59, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Upshaw, T.L.; Brown, C.; Smith, R.; Perri, M.; Ziegler, C.; Pinto, A.D. Social determinants of COVID-19 incidence and outcomes: A rapid review. PLoS ONE 2021, 16, e0248336. [Google Scholar] [CrossRef]
- Eker, S. Validity and usefulness of COVID-19 models. Humanit. Soc. Sci. Commun. 2020, 7, 1–5. [Google Scholar] [CrossRef]
- Galanis, G.; Hanieh, A. Incorporating Social Determinants of Health into Modelling of COVID-19 and other Infectious Diseases: A Baseline Socio-economic Compartmental Model. Soc. Sci. Med. 2021, 274, 113794. [Google Scholar] [CrossRef]
- Leslie, D.; Mazumder, A.; Peppin, A.; Wolters, M.K.; Hagerty, A. Does “AI” stand for augmenting inequality in the era of covid-19 healthcare? BMJ 2021, 372, n304. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. The concepts and principles of equity and health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Diderichsen, F.; Hallqvist, J.; Whitehead, M. Differential vulnerability and susceptibility: How to make use of recent development in our understanding of mediation and interaction to tackle health inequalities. Int. J. Epidemiol. 2019, 48, 268–274. [Google Scholar] [CrossRef]
- Fontanarosa, P.B.; Flanagin, A.; Ayanian, J.Z.; Bonow, R.O.; Bressler, N.M.; Christakis, D.; Disis, M.L.; Josephson, S.A.; Kibbe, M.R.; Öngür, D.; et al. Equity and the JAMA Network. JAMA Netw. Open 2021, 4, e2118381. [Google Scholar] [CrossRef] [PubMed]
- Rivara, F.P.; Bradley, S.M.; Catenacci, D.V.; Desai, A.N.; Ganguli, I.; Haneuse, S.J.P.A.; Inouye, S.K.; Jacobs, E.A.; Kan, K.; Kim, H.S.; et al. Structural Racism and JAMA Network Open. JAMA Network Open 2021, 4, e2120269. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, T.L.; Phillips, K.P. From SARS to pandemic influenza: The framing of high-risk populations. Nat. Hazards 2019, 98, 103–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholls, S.G.; Newson, A.J.; Ashcroft, R.E. The need for ethics as well as evidence in evidence-based medicine. J. Clin. Epidemiol. 2016, 77, 7–10. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Himmelstein, D.U.; Woolhandler, S. Health Insurance Status and Risk Factors for Poor Outcomes with COVID-19 among U.S. Health Care Workers: A Cross-Sectional Study. Ann. Intern. Med. 2020, 173, 410–412. [Google Scholar] [CrossRef]
- Glover, R.E.; van Schalkwyk, M.C.I.; Akl, E.A.; Kristjannson, E.; Lotfi, T.; Petkovic, J.; Petticrew, M.P.; Pottie, K.; Tugwell, P.; Welch, V.; et al. A framework for identifying and mitigating the equity harms of COVID-19 policy interventions. J. Clin. Epidemiol. 2020, 128, 35–48. [Google Scholar] [CrossRef]
- Tugwell, P.; Petticrew, M.; Kristjansson, E.; Welch, V.; Ueffing, E.; Waters, E.; Bonnefoy, J.; Morgan, A.; Doohan, E.; Kelly, M.P.; et al. Assessing equity in systematic reviews: Realising the recommendations of the Commission on Social Determinants of Health. BMJ 2010, 341, 873–877. [Google Scholar] [CrossRef] [Green Version]
- Petticrew, M.; Roberts, H. Evidence, hierarchies, and typologies: Horses for courses. J. Epidemiol. Community Health 2003, 57, 527–529. [Google Scholar] [CrossRef] [Green Version]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Pan, K.Y.; Kok, A.A.L.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; Oppen, P.V.; Giltay, E.J.; Penninx, B.W.J.H. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: A longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Rizvi, A.; Wasfi, R.; Enns, A.; Kristjansson, E. The impact of novel and traditional food bank approaches on food insecurity: A longitudinal study in Ottawa, Canada. BMC Public Health 2021, 21, 771. [Google Scholar] [CrossRef]
- Willows, N.D.; Veugelers, P.; Raine, K.; Kuhle, S. Prevalence and sociodemographic risk factors related to household food security in Aboriginal peoples in Canada. Public Health Nutr. 2009, 12, 1150–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, K.; Fox, C.; Abdalla, M.; Tatem, A.; Qirbi, N.; Lloyd-Braff, L.; Al-Shabi, K.; Ongwae, K.; Dyson, M.; Hassen, K. Estimating access to health care in Yemen, a complex humanitarian emergency setting: A descriptive applied geospatial analysis. Lancet Glob. Health 2020, 8, e1435–e1443. [Google Scholar] [CrossRef]
- Reporting Guidelines under Development for Observational Studies | The EQUATOR Network. Available online: https://www.equator-network.org/library/reporting-guidelines-under-development/reporting-guidelines-under-development-for-observational-studies/#STROBEeq (accessed on 10 June 2021).
- Welch, V.; Rizvi, A. STROBE-Equity Reporting Guidelines. 2020. Available online: https://osf.io/h57se/ (accessed on 22 June 2021).
- Glasziou, P.; Altman, D.G.; Bossuyt, P.; Boutron, I.; Clarke, M.; Julious, S.; Michie, S.; Moher, D.; Wager, E. Reducing waste from incomplete or unusable reports of biomedical research. Lancet 2014, 383, 267–276. [Google Scholar] [CrossRef]
- Turner, L.; Shamseer, L.; Altman, D.G.; Schulz, K.F.; Moher, D. Does use of the CONSORT Statement impact the completeness of reporting of randomised controlled trials published in medical journals? A Cochrane review. Syst. Rev. 2012, 1, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef] [Green Version]
- General Assembly. United Nations. United Nations Declaration on the Rights of Indigenous Peoples A/RES/61/295. 2007. Available online: https://www.un.org/development/desa/indigenouspeoples/declaration-on-the-rights-of-indigenous-peoples.html (accessed on 22 June 2021).
- Truth and Reconciliation Commission of Canada. Truth and Reconciliation Commission of Canada: Calls to Action; Government of Canada: Winnipeg, MB, Canada, 2015.
- Moher, D.; Schulz, K.F.; Simera, I.A.D. Guidance for Developers of Health Research Reporting Guidelines. PLoS Med. 2010, 7, e1000217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jull, J.; Petticrew, M.; Kristjansson, E.; Yoganathan, M.; Petkovic, J.; Tugwell, P.; Welch, V.; CONSORT-Equity 2017 and Boston Equity Symposium participants. Engaging knowledge users in development of the CONSORT-equity 2017 reporting guideline: A qualitative study using indepth interviews. Res. Involv. Engagem. 2018, 4, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.A.; Norheim, O.F.; Jull, J.; Cookson, R.; Sommerfelt, H.; Tugwell, P.; CONSORT-Equity and Boston Equity Symposium. CONSORT-Equity 2017 extension and elaboration for better reporting of health equity in randomised trials. BMJ 2017, 359, j5085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, S.; Babor, T.F.; De Castro, P.; Tort, S.; Curno, M. Sex and Gender Equity in Research: Rationale for the SAGER guidelines and recommended use. Res. Integr. Peer Rev. 2016, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, V.; Petticrew, M.; Tugwell, P.; Moher, D.; O’Neill, J.; Waters, E.; White, H. PRISMA-Equity 2012 Extension: Reporting Guidelines for Systematic Reviews with a Focus on Health Equity. PLoS Med. 2012, 9, e1001333. [Google Scholar] [CrossRef] [Green Version]
- Epistemonikos Foundation. Methods for the Special L.OVE of Coronavirus Infection (COVID-19). Available online: https://app.iloveevidence.com/covid19 (accessed on 15 June 2021).
- Bilal, U.; Tabb, L.P.; Barber, S.; Diez Roux, A.V. Spatial Inequities in COVID-19 Testing, Positivity, Confirmed Cases, and Mortality in 3 U.S. Cities. Ann. Intern. Med. 2021, 174, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, R.; Bendayan, R.; Ashworth, M.; Bean, D.M.; Dodhia, H.; Durbaba, S.; O’Gallagher, K.; Palmer, C.; Curcin, V.; Aitken, E.; et al. A case-control and cohort study to determine the relationship between ethnic background and severe COVID-19. EClinicalMedicine 2020, 28, 100574. [Google Scholar] [CrossRef] [PubMed]
- Cattelan, A.M.; Sasset, L.; Di Meco, E.; Cocchio, S.; Barbaro, F.; Cavinato, S.; Gardin, S.; Carretta, G.; Donato, D.; Crisanti, A.; et al. An integrated strategy for the prevention of sars-cov-2 infection in healthcare workers: A prospective observational study. Int. J. Environ. Res. Public Health 2020, 17, 5785. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Mekonnen, H.S.; Azagew, A.W.; Wubneh, C.A.; Belay, G.M.; Assimamaw, N.T.; Agegnehu, C.D.; Azale, T.; Azene, Z.N.; Merid, M.W.; Muluneh, A.G.; et al. Community’s misconception about COVID-19 and its associated factors among Gondar town residents, Northwest Ethiopia. Trop. Med. Health 2020, 48, 1–9. [Google Scholar] [CrossRef]
- D’ambrosi, F.; Iurlaro, E.; Tassis, B.; Di Maso, M.; Erra, R.; Cetera, G.E.; Cesano, N.; Di Martino, D.; Ossola, M.W.; Ferrazzi, E.M. Sociodemographic characteristics of pregnant women tested positive for COVID-19 admitted to a referral center in Northern Italy during lockdown period. J. Obstet. Gynaecol. Res. 2021, 47, 1751–1756. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Vega, M.F.; Soto-Cabezas, M.G.; Cárdenas, F.; Martel, K.S.; Valle, A.; Valverde, J.; Vidal-Anzardo, M.; Falcón, M.E.; Munayco, C.V.; Peru COVID-19 Working Group. SARS-CoV-2 prevalence associated to low socioeconomic status and overcrowding in an LMIC megacity: A population-based seroepidemiological survey in Lima, Peru. EClinicalMedicine 2021, 34, 100801. [Google Scholar] [CrossRef] [PubMed]
- Bajos, N.; Jusot, F.; Pailhé, A.; Spire, A.; Martin, C.; Meyer, L.; Lydié, N.; Franck, J.-E.; Zins, M. When lockdown policies amplify social inequalities in COVID-19 infections: Evidence from a cross-sectional population-based survey in France. BMC Public Health 2021, 21, 705. [Google Scholar] [CrossRef] [PubMed]
- González-Rábago, Y.; Cabezas-Rodríguez, A.; Martín, U. Social inequalities in health determinants in spanish children during the covid-19 lockdown. Int. J. Environ. Res. Public Health 2021, 18, 4087. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.S.; Souza Araújo, A.A.; de Oliveira, J.R.; Carrat, F. COVID-19 mortality among Indigenous people in Brazil: A nationwide register-based study. J. Public Health 2021, 43, e250–e251. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.; Tugwell, P.; Petticrew, M.; de Montigny, J.; Ueffing, E.; Kristjansson, B.; McGowan, J.; Benkhalti Jandu, M.; Wells, G.A.; Brand, K.; et al. How effects on health equity are assessed in systematic reviews of interventions. Cochrane Database Syst. Rev. 2010, 2010, MR000028. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, S.; Katz, E.G.; Darmstadt, G.L. Gender and the impact of COVID-19 on demand for and access to health care: Analysis of data from Kenya, Nigeria, and South Africa. Lancet Glob. Health 2021, 9, S7. [Google Scholar] [CrossRef]
- Press, V.G.; Huisingh-Scheetz, M.; Arora, V.M. Inequities in Technology Contribute to Disparities in COVID-19 Vaccine Distribution. JAMA Health Forum 2021, 2, e210264. [Google Scholar] [CrossRef]
- Krieger, N.; Fee, E. Man-made medicine and women’s health: The biopolitics of sex/gender and race/ethnicity. Int. J. Health Serv. 1994, 24, 265–283. [Google Scholar] [CrossRef]
- Browne, A.J.; Fiske, J.A. First nations women’s encounters with mainstream health care services. West. J. Nurs. Res. 2001, 23, 126–147. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanf. Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- Van Herk, K.; Smith, D.; Andrew, C. Identity matters: Aboriginal mothers’ experiences of accessing care. Contemp. Nurse 2011, 37, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Morton Ninomiya, M.E.; Pollock, N.J. Reconciling community-based Indigenous research and academic practices: Knowing principles is not always enough. Soc. Sci. Med. 2017, 172, 28–36. [Google Scholar] [CrossRef]
- Mashford-Pringle, A.; Pavagadhi, K. Using OCAP and IQ as frameworks to address a history of trauma in indigenous health research. AMA J. Ethics 2020, 22, E868–E873. [Google Scholar] [CrossRef] [PubMed]
- Hankivsky, O.; Grace, D.; Hunting, G.; Giesbrecht, M.; Fridkin, A.; Rudrum, S.; Ferlatte, O.; Clark, N. An intersectionality-based policy analysis framework: Critical reflections on a methodology for advancing equity. Int. J. Equity Health 2014, 13, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indigenous Community Research Partnerships Can Help Address Health Inequities. Available online: https://theconversation.com/indigenous-community-research-partnerships-can-help-address-health-inequities-152705 (accessed on 10 June 2021).
- Hoeyer, K.; Bauer, S.; Pickersgill, M. Datafication and accountability in public health: Introduction to a special issue. Soc. Stud. Sci. 2019, 49, 459–475. [Google Scholar] [CrossRef] [PubMed]
- Indigenous Research Training | Queen’s University. Available online: https://www.queensu.ca/indigenous/decolonizing-and-indigenizing/community-research-partnerships-training (accessed on 9 June 2021).
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. BMJ 2017, 358, 3453. [Google Scholar] [CrossRef] [Green Version]
- Hill, R.; Walsh, F.J.; Davies, J.; Sparrow, A.; Mooney, M.; Central Land Council; Wise, R.M.; Tengö, M. Knowledge co-production for Indigenous adaptation pathways: Transform post-colonial articulation complexes to empower local decision-making. Glob. Environ. Chang. 2020, 65, 102161. [Google Scholar] [CrossRef]
- Sugimoto, C.R.; Ahn, Y.Y.; Smith, E.; Macaluso, B.; Larivière, V. Factors affecting sex-related reporting in medical research: A cross-disciplinary bibliometric analysis. Lancet 2019, 393, 550–559. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
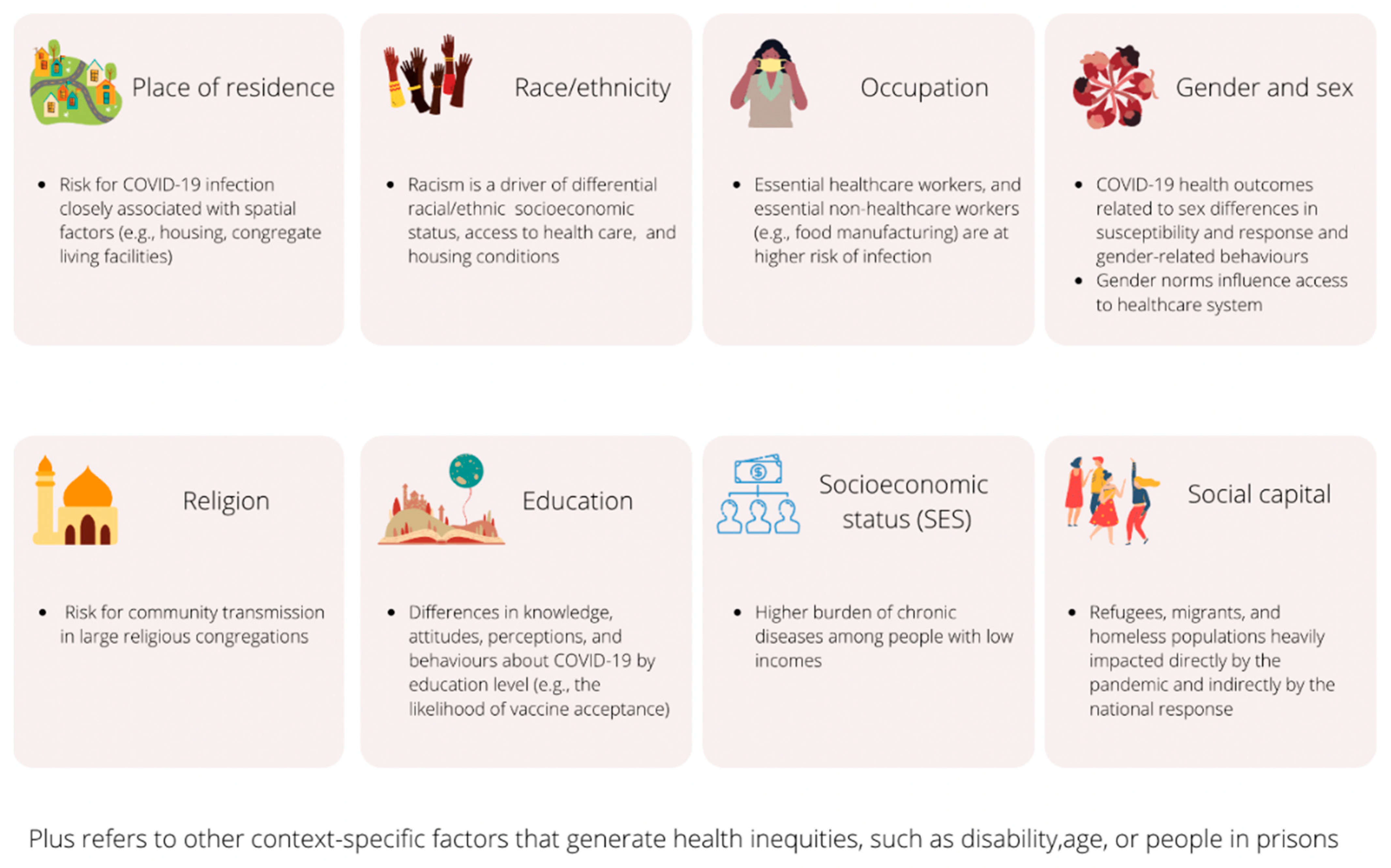
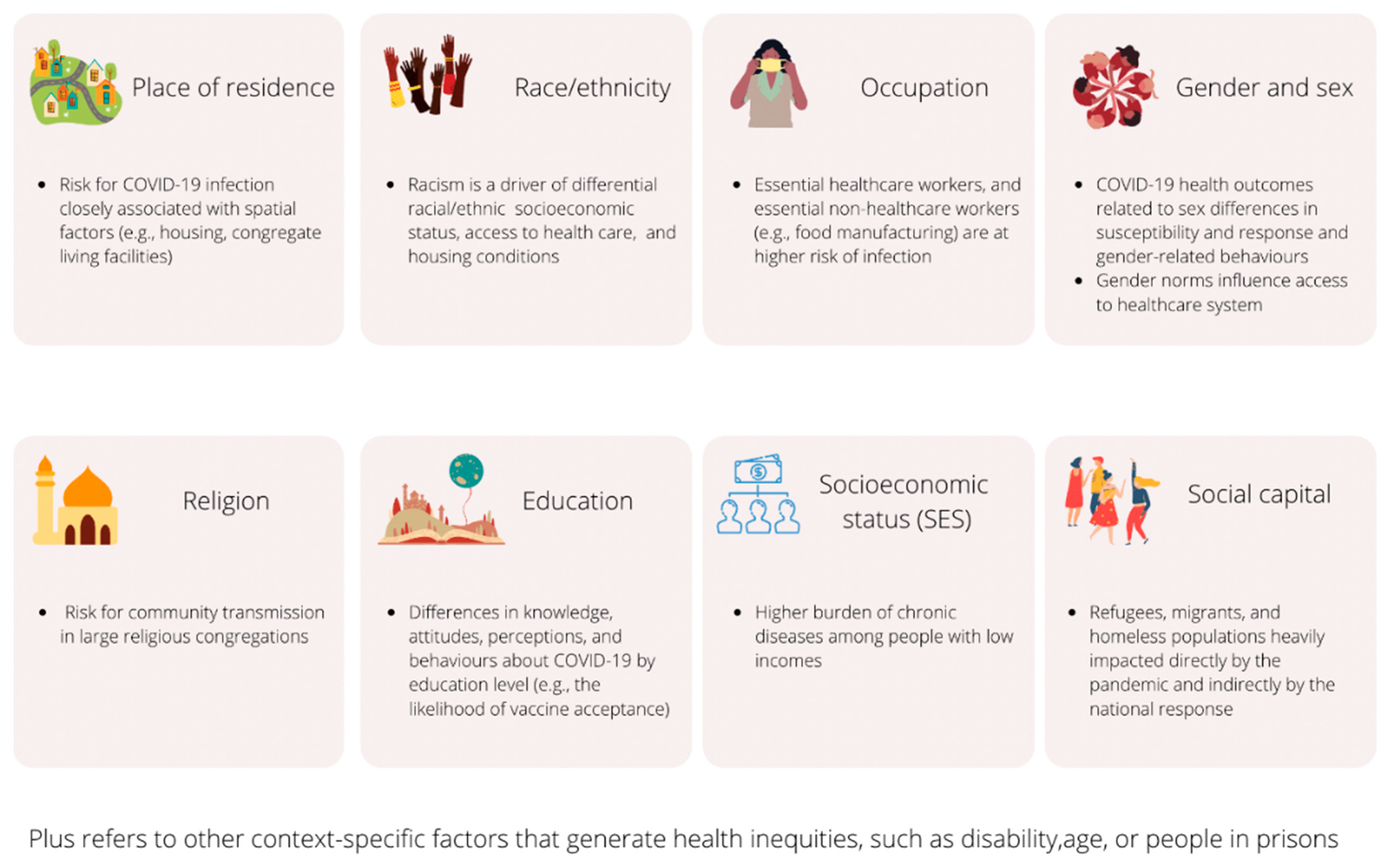
| PROGRESS-Plus Factors | Level of Analysis | Context Country Data Source | Gap or Focus Approaches * | Topic | Differences in Health Opportunities | Research Question | Study Design |
|---|---|---|---|---|---|---|---|
| Place of residence | Group | United States Zip code tabulation area | Gap | Incidence Testing access | Differential exposure and susceptibility | What is the characterisation of spatial inequities in COVID-19 testing, positivity, confirmed cases, and mortality during the first 6 months of the pandemic? [51] | Ecological |
| Race, ethnicity, culture, or language | Individual | England Hospital and primary care health records | Gap | Prognosis | Differential susceptibility | Are there differences in risk of hospitalisation with severe COVID-19 and/or in-hospital mortality across ethnic groups? [52] | Mixed: cohort and case-control |
| Occupation | Individual | Italy Ad hoc database | Focus | Infection prevention and control | Differential exposure | What is the effectiveness of an integrated infection control surveillance system among healthcare workers involved in the first management of suspected or confirmed COVID-19 patients? [53] | Prospective cohort |
| Gender | Group | 19 countries from Africa, Asia, Europe, North America, and South America Country-level data | Gap | Vaccination | Differential acceptability | Are demographics, including gender, independently associated with vaccine acceptance? [54] | Cross-sectional |
| Sex | Individual | Sweden, United Kingdon, United States | Gap | Prognosis | Differential susceptibility | What are symptoms associated with short and long COVID adjusting for sex and age? [55] | Prospective cohort |
| Religion | Individual | Ethiopia City-level urban, community-based | Gap | Knowledge, attitudes, perceptions | Differential acceptability | What are factors associated with perception toward COVID-19? [56] | Cross-sectional |
| Education | Individual | Italy City-level Hospital health records | Gap | Prevalence | Differential exposure | What are sociodemographic characteristics, including education level, associated with COVID-19 disease among pregnant females admitted to hospital for pregnancy health care? [57] | Cross-sectional |
| Socioeconomic status | Individual | Peru City-level, Population-based survey | Gap | Prevalence | Differential exposure | What is the seroprevalence of SARS-CoV-2 antibodies in Lima [stratified by socioeconomic status and other variables]? [58] | Cross-sectional |
| Social capital | Group | France Population-based survey | Gap | Policy impact | Differential community effectiveness | What is the impact of lockdown policies on different social classes in France? [59] | Cross-sectional |
| Plus | Individual Children | Spain | Focus | Policy impact | Differential exposure and equity distribution effects | Are social determinants of children’s health unequally distributed during the COVID-19 lockdown? [60] | Cross-sectional |
| Indigenous Peoples | Individual | Brazil Nationwide register | Focus | Incidence | Differential exposure and accessibility to healthcare | What is the burden of COVID-19 on the Indigenous population? [61] | Cohort |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antequera, A.; Lawson, D.O.; Noorduyn, S.G.; Dewidar, O.; Avey, M.; Bhutta, Z.A.; Chamberlain, C.; Ellingwood, H.; Francis, D.; Funnell, S.; et al. Improving Social Justice in COVID-19 Health Research: Interim Guidelines for Reporting Health Equity in Observational Studies. Int. J. Environ. Res. Public Health 2021, 18, 9357. https://doi.org/10.3390/ijerph18179357
Antequera A, Lawson DO, Noorduyn SG, Dewidar O, Avey M, Bhutta ZA, Chamberlain C, Ellingwood H, Francis D, Funnell S, et al. Improving Social Justice in COVID-19 Health Research: Interim Guidelines for Reporting Health Equity in Observational Studies. International Journal of Environmental Research and Public Health. 2021; 18(17):9357. https://doi.org/10.3390/ijerph18179357
Chicago/Turabian StyleAntequera, Alba, Daeria O. Lawson, Stephen G. Noorduyn, Omar Dewidar, Marc Avey, Zulfiqar A. Bhutta, Catherine Chamberlain, Holly Ellingwood, Damian Francis, Sarah Funnell, and et al. 2021. "Improving Social Justice in COVID-19 Health Research: Interim Guidelines for Reporting Health Equity in Observational Studies" International Journal of Environmental Research and Public Health 18, no. 17: 9357. https://doi.org/10.3390/ijerph18179357
APA StyleAntequera, A., Lawson, D. O., Noorduyn, S. G., Dewidar, O., Avey, M., Bhutta, Z. A., Chamberlain, C., Ellingwood, H., Francis, D., Funnell, S., Ghogomu, E., Greer-Smith, R., Horsley, T., Juando-Prats, C., Jull, J., Kristjansson, E., Little, J., Nicholls, S. G., Nkangu, M., ... Welch, V. (2021). Improving Social Justice in COVID-19 Health Research: Interim Guidelines for Reporting Health Equity in Observational Studies. International Journal of Environmental Research and Public Health, 18(17), 9357. https://doi.org/10.3390/ijerph18179357