
Air Pollution, Residential Greenness and Metabolic Dysfunction during Early Pregnancy in the INfancia y Medio Ambiente (INMA) Cohort

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
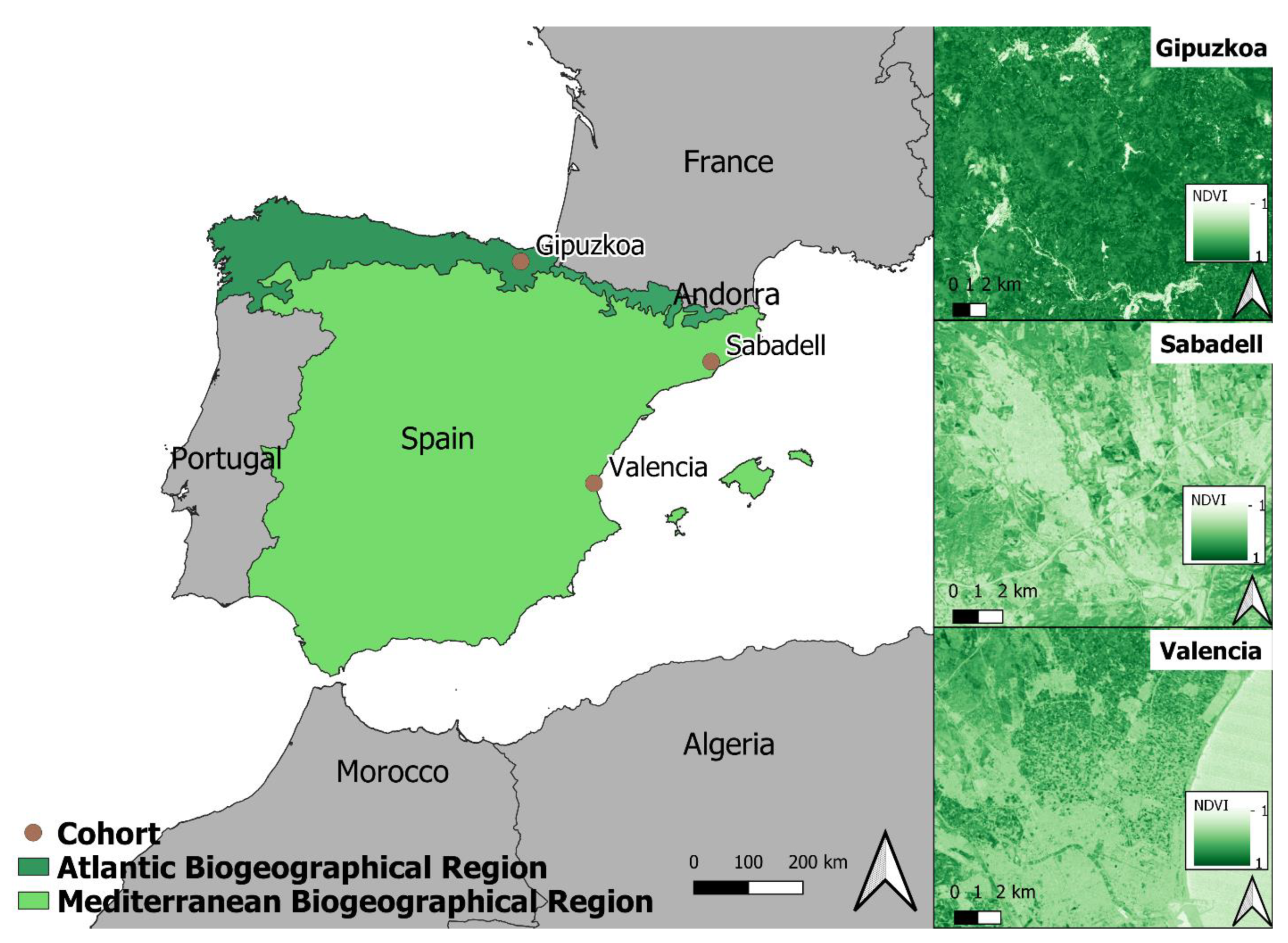
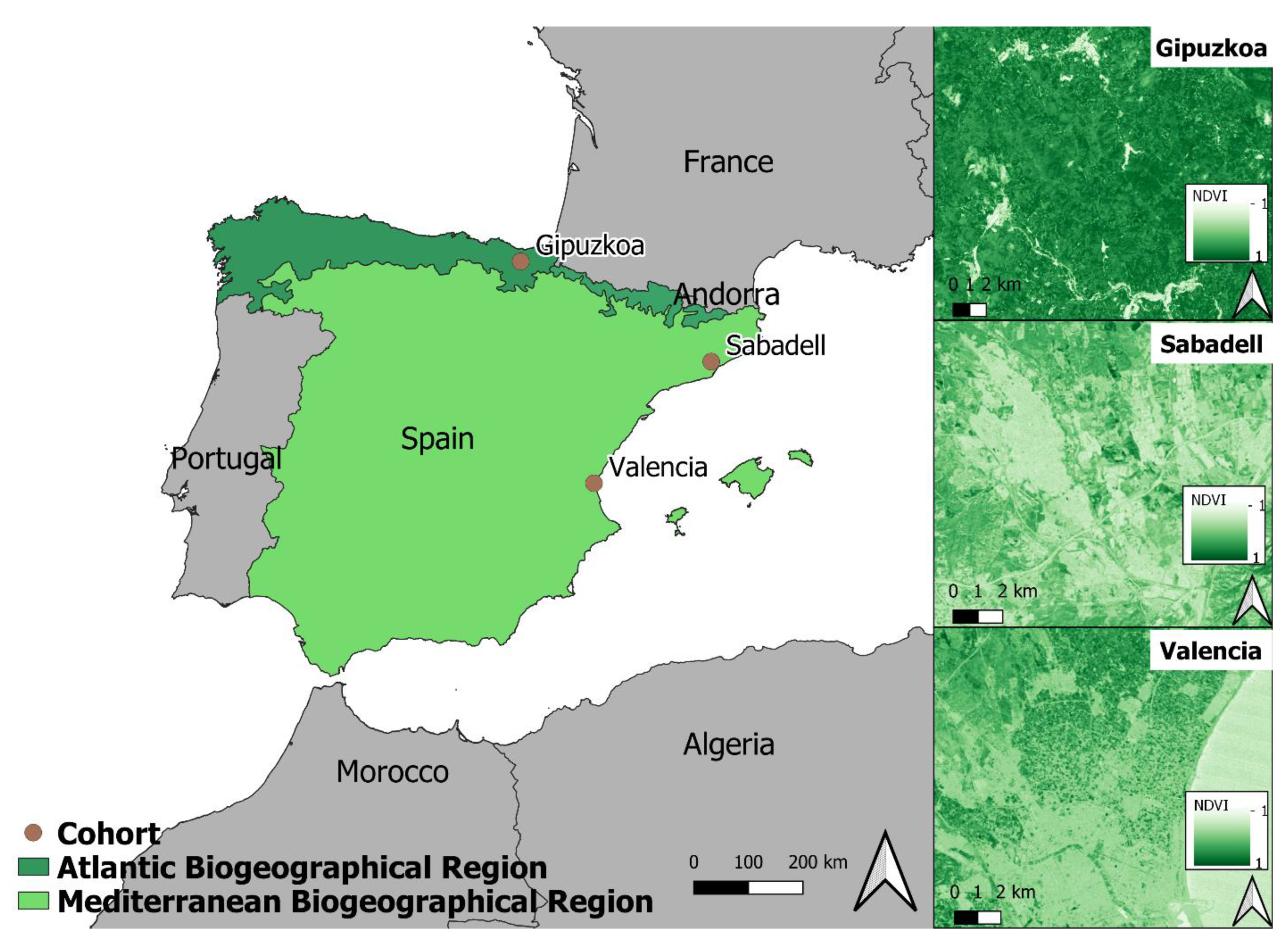
2.1. Study Population
2.2. Glucose Intolerance and Lipid Levels
2.3. NO2 and PM2.5 Exposures
2.4. Residential Greenness
2.5. Covariates
2.6. Statistical Analysis
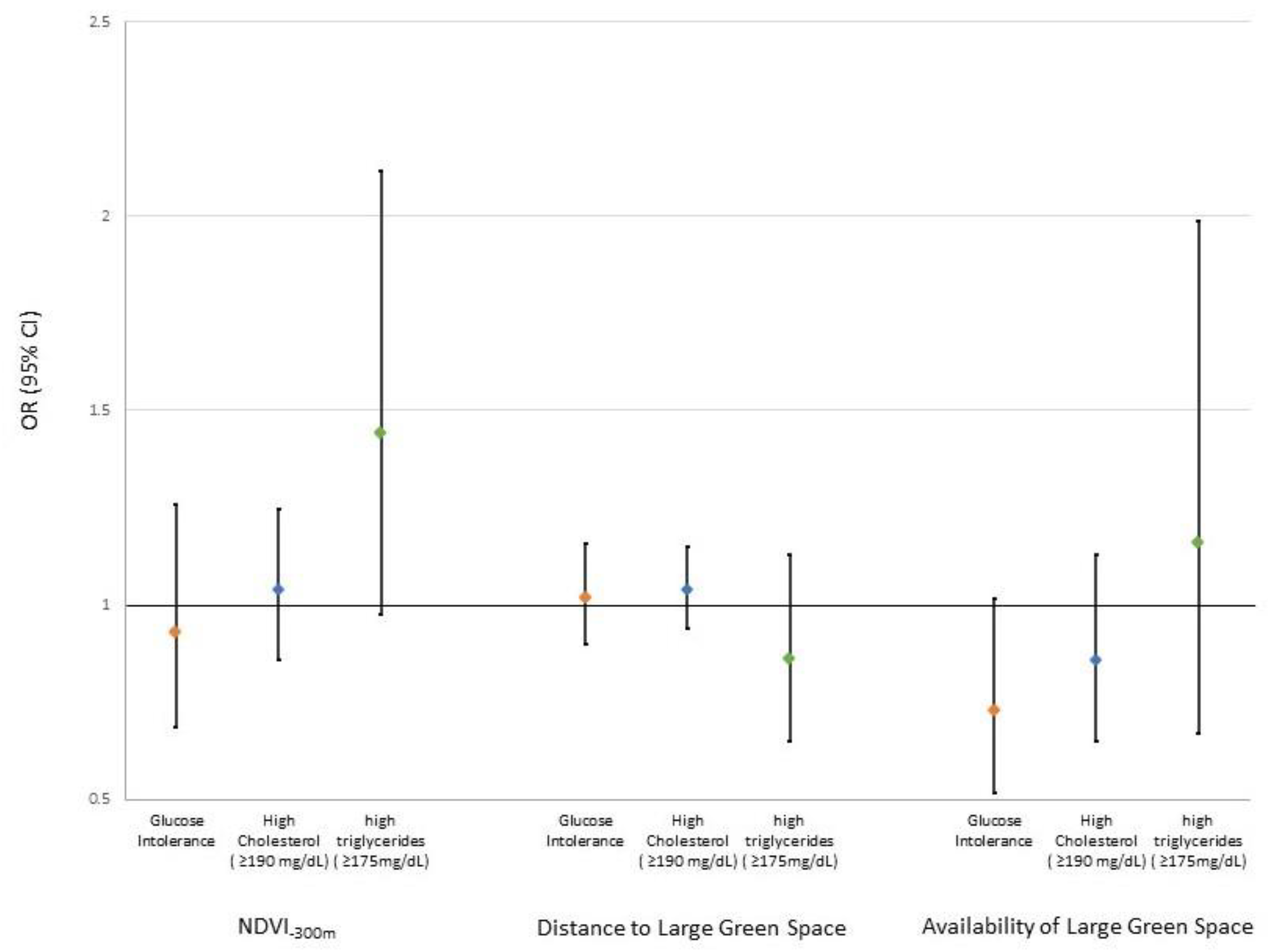
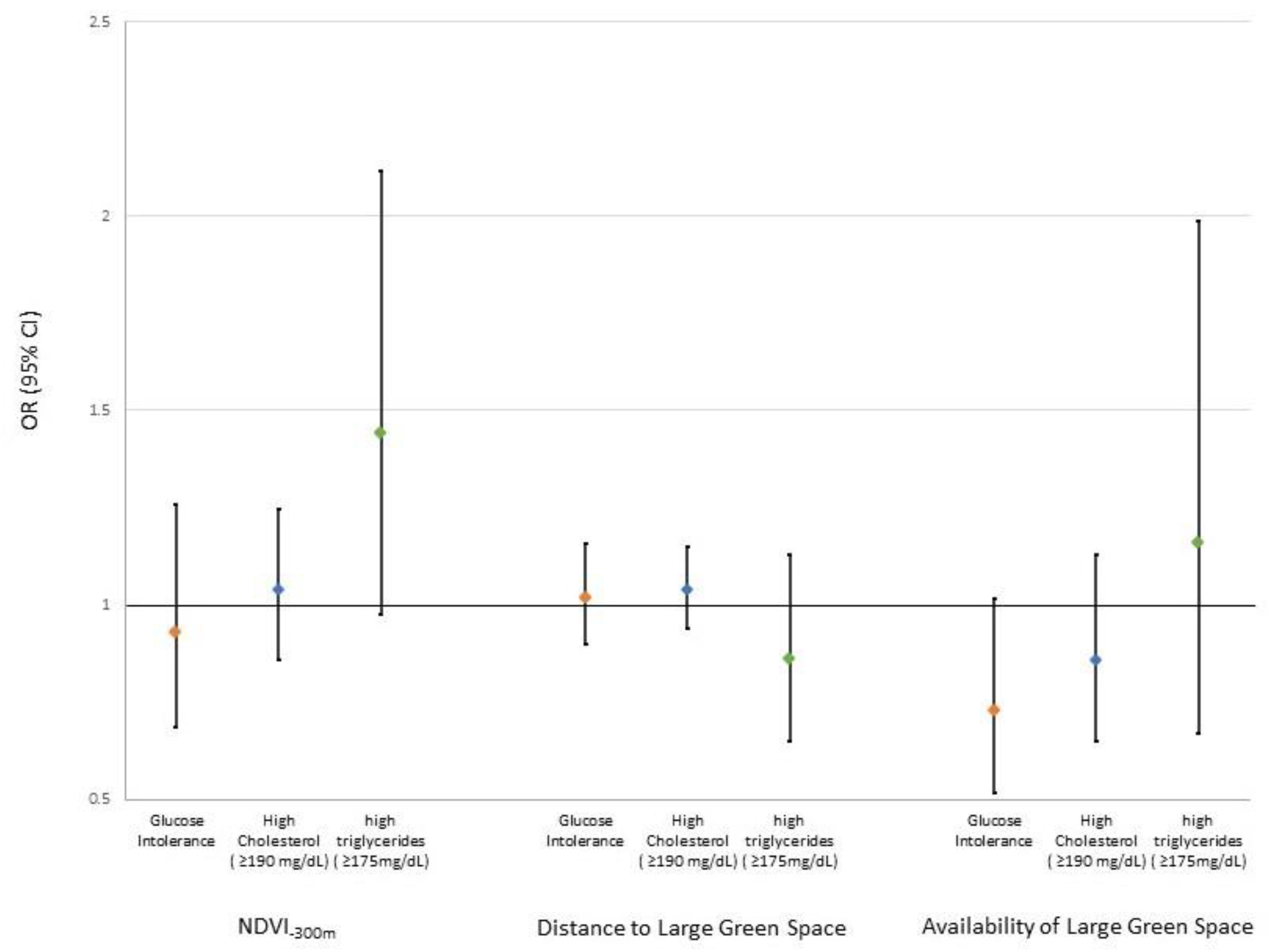
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [Green Version]
- Dennison, R.A.; Chen, E.S.; Green, M.E.; Legard, C.; Kotecha, D.; Farmer, G.; Sharp, S.J.; Ward, R.J.; Usher-Smith, J.A.; Griffin, S.J. The absolute and relative risk of type 2 diabetes after gestational diabetes: A systematic review and meta-analysis of 129 studies. Diabetes Res. Clin. Pract. 2020, 171, 108625. [Google Scholar] [CrossRef]
- Ryckman, K.K.; Spracklen, C.N.; Smith, C.J.; Robinson, J.G.; Saftlas, A.F. Maternal lipid levels during pregnancy and gestational diabetes: A systematic review and meta-analysis. BJOG 2015, 122, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Wild, R.; Weedin, E.A.; Wilson, D. Dyslipidemia in pregnancy. Cardiol. Clin. 2015, 33, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Enquobahrie, D.A.; Williams, M.A.; Butler, C.L.; Frederick, I.O.; Miller, R.S.; Luthy, D.A. Maternal plasma lipid concentrations in early pregnancy and risk of preeclampsia. Am. J. Hypertens. 2004, 17, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Vrijkotte, T.G.; Krukziener, N.; Hutten, B.A.; Vollebregt, K.C.; van Eijsden, M.; Twickler, M.B. Maternal lipid profile during early pregnancy and pregnancy complications and outcomes: The ABCD study. J. Clin. Endocrinol. Metab. 2012, 97, 3917–3925. [Google Scholar] [CrossRef]
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Dunne, F.; Lawlor, D.A. Hyperglycaemia and risk of adverse perinatal outcomes: Systematic review and meta-analysis. BMJ 2016, 354, i4694. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Moore, D.; Subramanian, A.; Cheng, K.K.; Toulis, K.A.; Qiu, X.; Saravanan, P.; Price, M.J.; Nirantharakumar, K. Gestational dyslipidaemia and adverse birthweight outcomes: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1256–1268. [Google Scholar] [CrossRef]
- Nijs, H.; Benhalima, K. Gestational diabetes mellitus and the long-term risk for glucose intolerance and overweight in the offspring: A narrative review. J. Clin. Med. 2020, 9, 599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.C.; Talbott, E.O.; Roberts, J.M.; Catov, J.M.; Sharma, R.K.; Ritz, B. Particulate air pollution exposure and C-reactive protein during early pregnancy. Epidemiology 2011, 22, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Yi, L.; Wei, C.; Fan, W. Fine-particulate matter (PM2.5), a risk factor for rat gestational diabetes with altered blood glucose and pancreatic GLUT2 expression. Gynecol. Endocrinol. 2017, 33, 611–616. [Google Scholar] [CrossRef]
- Lim, C.C.; Thurston, G.D. Air pollution, oxidative stress, and diabetes: A life course epidemiologic perspective. Curr. Diabetes Rep. 2019, 19, 58. [Google Scholar] [CrossRef]
- Lowe, L.P.; Metzger, B.E.; Lowe, W.L., Jr.; Dyer, A.R.; McDade, T.W.; McIntyre, H.D.; HAPO Study Cooperative Research Group. Inflammatory mediators and glucose in pregnancy: Results from a subset of the hyperglycemia and adverse pregnancy Outcome (HAPO) Study. J. Clin. Endocrinol. Metab. 2010, 95, 5427–5434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Navab, M.; Pakbin, P.; Ning, Z.; Navab, K.; Hough, G.; Morgan, T.E.; Finch, C.E.; Araujo, J.A.; Fogelman, A.M.; et al. Ambient ultrafine particles alter lipid metabolism and HDL anti-oxidant capacity in LDLR-null mice. J. Lipid Res. 2013, 54, 1608–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darbre, P.D. Overview of air pollution and endocrine disorders. Int. J. Gen. Med. 2018, 11, 191–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eze, I.C.; Hemkens, L.G.; Bucher, H.C.; Hoffmann, B.; Schindler, C.; Kunzli, N.; Schikowski, T.; Probst-Hensch, N.M. Association between ambient air pollution and diabetes mellitus in Europe and North America: Systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 381–389. [Google Scholar] [CrossRef]
- He, D.; Wu, S.; Zhao, H.; Qiu, H.; Fu, Y.; Li, X.; He, Y. Association between particulate matter 2.5 and diabetes mellitus: A meta-analysis of cohort studies. J. Diabetes Investig. 2017, 8, 687–696. [Google Scholar] [CrossRef]
- Elshahidi, M.H. Outdoor air pollution and gestational diabetes mellitus: A systematic review and meta-analysis. Iran. J. Public Health 2019, 48, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, W.; Li, Y.; Niu, Y.; Ding, Y.; Yu, X.; Zhu, B.; Duan, R.; Duan, H.; Kou, C.; Li, Y.; et al. Association between ambient air pollution and pregnancy complications: A systematic review and meta-analysis of cohort studies. Environ. Res. 2020, 185, 109471. [Google Scholar] [CrossRef]
- Hu, C.Y.; Gao, X.; Fang, Y.; Jiang, W.; Huang, K.; Hua, X.G.; Yang, X.J.; Chen, H.B.; Jiang, Z.X.; Zhang, X.J. Human epidemiological evidence about the association between air pollution exposure and gestational diabetes mellitus: Systematic review and meta-analysis. Environ. Res. 2020, 180, 108843. [Google Scholar] [CrossRef]
- Tang, X.; Zhou, J.B.; Luo, F.; Han, Y.; Heianza, Y.; Cardoso, M.A.; Qi, L. Air pollution and gestational diabetes mellitus: Evidence from cohort studies. BMJ Open Diabetes Res. Care 2020, 8, e000937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Wang, Q.; He, S.; Wu, K.; Ren, M.; Dong, H.; Di, J.; Yu, Z.; Huang, C. Ambient air pollution and gestational diabetes mellitus: A review of evidence from biological mechanisms to population epidemiology. Sci. Total Environ. 2020, 719, 137349. [Google Scholar] [CrossRef]
- Kang, J.; Liao, J.; Xu, S.; Xia, W.; Li, Y.; Chen, S.; Lu, B. Associations of exposure to fine particulate matter during pregnancy with maternal blood glucose levels and gestational diabetes mellitus: Potential effect modification by ABO blood group. Ecotoxicol. Environ. Saf. 2020, 198, 110673. [Google Scholar] [CrossRef]
- Ye, B.; Zhong, C.; Li, Q.; Xu, S.; Zhang, Y.; Zhang, X.; Chen, X.; Huang, L.; Wang, H.; Zhang, Z.; et al. The associations of ambient fine particulate matter exposure during pregnancy with blood glucose levels and gestational diabetes mellitus risk: A prospective cohort study in Wuhan, China. Am. J. Epidemiol. 2020, 189, 1306–1315. [Google Scholar] [CrossRef]
- Zhang, H.; Dong, H.; Ren, M.; Liang, Q.; Shen, X.; Wang, Q.; Yu, L.; Lin, H.; Luo, Q.; Chen, W.; et al. Ambient air pollution exposure and gestational diabetes mellitus in Guangzhou, China: A prospective cohort study. Sci. Total Environ. 2020, 699, 134390. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, X.; Yang, X.; Dong, T.; Hu, W.; Guan, Q.; Tun, H.M.; Chen, Y.; Chen, R.; Sun, Z.; et al. Increased risk of gestational diabetes mellitus in women with higher prepregnancy ambient PM (2.5) exposure. Sci. Total Environ. 2020, 730, 138982. [Google Scholar] [CrossRef] [PubMed]
- Hehua, Z.; Yang, X.; Qing, C.; Shanyan, G.; Yuhong, Z. Dietary patterns and associations between air pollution and gestational diabetes mellitus. Environ. Int. 2021, 147, 106347. [Google Scholar] [CrossRef]
- Melody, S.M.; Wills, K.; Knibbs, L.D.; Ford, J.; Venn, A.; Johnston, F. Maternal exposure to ambient air pollution and pregnancy complications in Victoria, Australia. Int. J. Environ. Res. Public Health 2020, 17, 2572. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Ao, J.; Cai, J.; Luo, Z.; Martin, R.; Donkelaar, A.V.; Kan, H.; Zhang, J. Fine particular matter and its constituents in air pollution and gestational diabetes mellitus. Environ. Int. 2020, 142, 105880. [Google Scholar] [CrossRef]
- Fleisch, A.F.; Kloog, I.; Luttmann-Gibson, H.; Gold, D.R.; Oken, E.; Schwartz, J.D. Air pollution exposure and gestational diabetes mellitus among pregnant women in Massachusetts: A cohort study. Environ. Health 2016, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [Green Version]
- den Braver, N.R.; Lakerveld, J.; Rutters, F.; Schoonmade, L.J.; Brug, J.; Beulens, J.W.J. Built environmental characteristics and diabetes: A systematic review and meta-analysis. BMC Med. 2018, 16, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.C.; Lombard, J.; Wang, K.; Byrne, M.M.; Toro, M.; Plater-Zyberk, E.; Feaster, D.J.; Kardys, J.; Nardi, M.I.; Perez-Gomez, G.; et al. Neighborhood greenness and chronic health conditions in medicare beneficiaries. Am. J. Prev. Med. 2016, 51, 78–89. [Google Scholar] [CrossRef] [PubMed]
- de Keijzer, C.; Basagaña, X.; Tonne, C.; Valentín, A.; Alonso, J.; Antó, J.M.; Nieuwenhuijsen, M.J.; Kivimäki, M.; Singh-Manoux, A.; Sunyer, J.; et al. Long-term exposure to greenspace and metabolic syndrome: A whitehall II study. Environ. Pollut. 2019, 255, 113231. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.Y.; Markevych, I.; Heinrich, J.; Bloom, M.S.; Qian, Z.; Geiger, S.D.; Vaughn, M.; Liu, S.; Guo, Y.; Dharmage, S.C.; et al. Residential greenness and blood lipids in urban-dwelling adults: The 33 Communities Chinese Health Study. Environ. Pollut. 2019, 250, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Egorov, A.I.; Griffin, S.M.; Converse, R.R.; Styles, J.N.; Sams, E.A.; Wilson, A.; Jackson, L.E.; Wade, T.J. Vegetated land cover near residence is associated with reduced allostatic load and improved biomarkers of neuroendocrine, metabolic and immune functions. Environ. Res. 2017, 158, 508–521. [Google Scholar] [CrossRef]
- Zhan, Y.; Liu, J.; Lu, Z.; Yue, H.; Zhang, J.; Jiang, Y. Influence of residential greenness on adverse pregnancy outcomes: A systematic review and dose-response meta-analysis. Sci. Total Environ. 2020, 718, 137420. [Google Scholar] [CrossRef] [PubMed]
- Young, C.; Laurent, O.; Chung, J.H.; Wu, J. Geographic distribution of healthy resources and adverse pregnancy outcomes. Matern. Child Health J. 2016, 20, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Choe, S.A.; Kauderer, S.; Eliot, M.N.; Glazer, K.B.; Kingsley, S.L.; Carlson, L.; Awad, Y.A.; Schwartz, J.D.; Savitz, D.A.; Wellenius, G.A. Air pollution, land use, and complications of pregnancy. Sci. Total Environ. 2018, 645, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.; Chen, X.; Xu, S.; Li, Y.; Zhang, B.; Cao, Z.; Zhang, Y.; Liang, S.; Hu, K.; Xia, W. Effect of residential exposure to green space on maternal blood glucose levels, impaired glucose tolerance, and gestational diabetes mellitus. Environ. Res. 2019, 176, 108526. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Yang, B.; Lin, S.; Bloom, M.S.; Nie, Z.; Ou, Y.; Mai, J.; Wu, Y.; Gao, X.; Dong, G.; et al. Associations of greenness with gestational diabetes mellitus: The guangdong registry of Congenital Heart Disease (GRCHD) study. Environ. Pollut. 2020, 266, 115127. [Google Scholar] [CrossRef] [PubMed]
- Guxens, M.; Ballester, F.; Espada, M.; Fernandez, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardon, A.; Torrent, M.; et al. Cohort profile: The INMA--INfancia y Medio Ambiente--(Environment and childhood) project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellitus, D. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus, Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003, 26 (Suppl. S1), S5–S20. [Google Scholar]
- Nordestgaard, B.G.; Langsted, A.; Mora, S.; Kolovou, G.; Baum, H.; Bruckert, E.; Watts, G.F.; Sypniewska, G.; Wiklund, O.; Borén, J.; et al. Fasting is not routinely required for determination of a lipid profile: Clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European atherosclerosis society and european federation of clinical chemistry and laboratory medicine. Eur. Heart J. 2016, 37, 1944–1958. [Google Scholar] [PubMed] [Green Version]
- Beelen, R.; Hoek, G.; Vienneau, D.; Eeftens, M.; Dimakopoulou, K.; Pedeli, X.; Tsai, M.-Y.; Künzli, N.; Schikowski, T.; Marcon, A. Development of NO2 and NOx land use regression models for estimating air pollution exposure in 36 study areas in Europe–the ESCAPE project. Atmos. Environ. 2013, 72, 10–23. [Google Scholar] [CrossRef]
- Pedersen, M.; Giorgis-Allemand, L.; Bernard, C.; Aguilera, I.; Andersen, A.M.; Ballester, F.; Beelen, R.M.; Chatzi, L.; Cirach, M.; Danileviciute, A.; et al. Ambient air pollution and low birthweight: A European cohort study (ESCAPE). Lancet Respir. Med. 2013, 1, 695–704. [Google Scholar] [CrossRef]
- Stafoggia, M.; Bellander, T.; Bucci, S.; Davoli, M.; de Hoogh, K.; De’ Donato, F.; Gariazzo, C.; Lyapustin, A.; Michelozzi, P.; Renzi, M.; et al. Estimation of daily PM (10) and PM (2.5) concentrations in Italy, 2013–2015, using a spatiotemporal land-use random-forest model. Environ. Int. 2019, 124, 170–179. [Google Scholar] [CrossRef]
- Weier, J.; Herring, D. Measuring Vegetation (NDVI & EVI). Available online: https://earthobservatory.nasa.gov/features/MeasuringVegetation (accessed on 21 December 2020).
- Institute of Medicine and National Research Council. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Fernández-Barrés, S.; Romaguera, D.; Valvi, D.; Martínez, D.; Vioque, J.; Navarrete-Muñoz, E.M.; Amiano, P.; Gonzalez-Palacios, S.; Guxens, M.; Pereda, E.; et al. Mediterranean dietary pattern in pregnant women and offspring risk of overweight and abdominal obesity in early childhood: The INMA birth cohort study. Pediatr. Obes. 2016, 11, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2015. [Google Scholar]
- Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide; World Health Organization: Geneva, Switzerland, 2006.
- Li, J.; Zhou, C.; Xu, H.; Brook, R.D.; Liu, S.; Yi, T.; Wang, Y.; Feng, B.; Zhao, M.; Wang, X.; et al. Ambient air pollution is associated with HDL (High-Density Lipoprotein) dysfunction in healthy adults. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 513–522. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Chen, R.; Cai, J.; Cui, X.; Huang, N.; Kan, H. Short-term exposure to fine particulate air pollution and genome-wide DNA methylation: A randomized, double-blind, crossover trial. Environ. Int. 2018, 120, 130–136. [Google Scholar] [CrossRef]
- Bartels, Ä.; O’Donoghue, K. Cholesterol in pregnancy: A review of knowns and unknowns. Obstet. Med. 2011, 4, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Gaio, V.; Roquette, R.; Dias, C.M.; Nunes, B. Ambient air pollution and lipid profile: Systematic review and meta-analysis. Environ. Pollut. 2019, 254, 113036. [Google Scholar] [CrossRef] [PubMed]
- McGuinn, L.A.; Schneider, A.; McGarrah, R.W.; Ward-Caviness, C.; Neas, L.M.; Di, Q.; Schwartz, J.; Hauser, E.R.; Kraus, W.E.; Cascio, W.E.; et al. Association of long-term PM (2.5) exposure with traditional and novel lipid measures related to cardiovascular disease risk. Environ. Int. 2019, 122, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.Y.; Bloom, M.S.; Markevych, I.; Qian, Z.M.; Vaughn, M.G.; Cummings-Vaughn, L.A.; Li, S.; Chen, G.; Bowatte, G.; Perret, J.L.; et al. Exposure to ambient air pollution and blood lipids in adults: The 33 communities Chinese health study. Environ. Int. 2018, 119, 485–492. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.Y.; Guo, Y.; Markevych, I.; Qian, Z.M.; Bloom, M.S.; Heinrich, J.; Dharmage, S.C.; Rolling, C.A.; Jordan, S.S.; Komppula, M.; et al. Association of long-term exposure to ambient air pollutants with risk factors for cardiovascular disease in China. JAMA Netw. Open 2019, 2, e190318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Paquet, C.; Coffee, N.T.; Haren, M.T.; Howard, N.J.; Adams, R.J.; Taylor, A.W.; Daniel, M. Food environment, walkability, and public open spaces are associated with incident development of cardio-metabolic risk factors in a biomedical cohort. Health Place 2014, 28, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Farukhi, Z.; Mora, S. Assessing the dyslipidemias: To fast or not to fast? Curr. Opin. Endocrinol. Diabetes Obes. 2021, 28, 97–103. [Google Scholar] [CrossRef]
- Rhew, I.C.; Vander Stoep, A.; Kearney, A.; Smith, N.L.; Dunbar, M.D. Validation of the normalized difference vegetation index as a measure of neighborhood greenness. Ann. Epidemiol. 2011, 21, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Browning, M.; Lee, K. Within what distance does “Greenness” best predict physical health? A systematic review of articles with GIS buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Characteristic | All Cohorts | Gipuzkoa | Sabadell | Valencia |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |
| Age | ||||
| Mean ± SD | 30.4 ± 4.4 | 31.4 ± 3.7 | 30.2 ± 4.6 | 29.8 ± 4.7 |
| Min–Max | 15–45.5 | 18–43 | 16.3–45.5 | 15–43 |
| Missing | 16 (0.71) | - | 16 (2.1) | - |
| Education | ||||
| Primary school | 572 (25.3) | 86 (13.5) | 201 (25.9) | 28 (3.3) |
| Secondary school | 889 (39.3) | 232 (36.5) | 308 (39.6) | 285 (35.5) |
| University | 708 (31.3) | 316 (49.7) | 204 (26.3) | 349 (41.1) |
| Missing | 94 (4.2) | 2 (0.3) | 64 (8.2) | 188 (22.1) |
| Total Physical Activity (METs/hour/day) in previous year, first trimester | ||||
| Mean ± SD | 37.9 ± 3.7 | 38.2 ± 3.6 | 37.9 ± 3.7 | 37.7 ± 3.8 |
| Min–Max | 29–54 | 31.2–51.6 | 30.2–54 | 29–53 |
| Missing | 168 7.4) | 13 (2) | 123 (15.8) | 32 (3.8) |
| Relative Mediterranean diet score (rMED), first trimester | ||||
| Low score (1–7) | 925 (40.9) | 167 (26.3) | 289 (37.2) | 469 (55.2) |
| Medium score (8–9) | 579 (25.6) | 192 (30.2) | 190 (24.5) | 197 (23.2) |
| High score (10–15) | 593 (26.2) | 267 (42) | 175 (22.5) | 151 (17.8) |
| Missing | 166 (7.3) | 10 (1.6) | 123 (15.8) | 33 (3.9) |
| Body Mass Index (BMI) | ||||
| Under weight (<18.5 kg/m2) | 103 (4.6) | 24 (3.8) | 37 (4.8) | 42 (4.9) |
| Normal weight (≥18.5 and <25 kg/m2) | 1531 (67.7) | 480 (75.5) | 500 (64.4) | 551 (64.8) |
| Overweight (≥25 & <30 kg/m2) | 395 (17.5) | 101 (15.9) | 145 (18.7) | 149 (17.5) |
| Obese (≥30 kg/m2) | 177 (7.8) | 31 (4.9) | 68 (8.8) | 78 (9.2) |
| Missing | 57 (2.5) | - | 27 (3.5) | 30 (3.5) |
| Smoking, first trimester | ||||
| No | 1429 (63.2) | 519 (81.6) | 601 (77.4) | 587 (69.1) |
| Yes | 675 (29.8) | 77 (12.1) | 119 (15.3) | 195 (22.9) |
| Missing | 159 (7.0) | 40 (6.3) | 57 (7.3) | 68 (8) |
| Alcohol Consumption, first trimester | ||||
| Mean ± SD | 0.3 ± 1.3 | 0.2 ± 0.7 | 0.4 ± 1.4 | 0.4 ± 1.5 |
| Min–Max | 0–15.2 | 0–7.8 | 0–15.2 | 0–14.4 |
| Missing | 166 (7.3) | 10 (1.6) | 123 (15.8) | 33 (3.9) |
| Gravidity | ||||
| 1 | 992 (43.8) | 282 (44.3) | 333 (42.9) | 377 (44.4) |
| 2 | 788 (34.8) | 245 (38.5) | 271 (34.9) | 272 (32) |
| 3+ | 443 (19.6) | 109 (17.1) | 161 (20.7) | 173 (20.4) |
| Missing | 40 (1.8) | - | 12 (1.5) | 28 (3.3) |
| Gestational Weight Gain | ||||
| Within IOM Guidelines | 745 (32.9) | 227 (35.7) | 243 (31.3) | 275 (32.4) |
| Below IOM Guidelines | 468 (20.7) | 194 (30.5) | 116 (14.9) | 158 (18.6) |
| Above IOM Guidelines | 720 (31.8) | 140 (22.0) | 240 (30.9) | 340 (40) |
| Missing | 330 (14.6) | 75 (11.8) | 178 (22.9) | 77 (9.06) |
| Urbanicity of residence | ||||
| Semi-urban/rural | 122 (5.4) | 316 (49.7) | - | 121 (14.2) |
| Urban | 1704 (75.3) | 320 (50.3) | 656 (84.4) | 728 (85.7) |
| Missing | 122 (5.4) | - | 121 (15.6) | 1 (0.12) |
| PM2.5 (µg/m3) Mean ± SD | 21.3 ± 5.2 | 16.2 ± 2.1 | 21.9 ± 4.0 | 24.6 ± 4.8 |
| NO2 (µg/m3) Mean ± SD | 28.2 ± 16.0 | 14.4 ± 4.3 | 37.7 ± 13.1 | 31.1 ± 16.8 |
| NDVI 100 m Mean ± SD | 0.2 ± 0.1 | 0.4 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 |
| NDVI 300 m Mean ± SD | 0.3 ± 0.1 | 0.4 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 |
| NDVI 500 m Mean ± SD | 0.3 ± 0.2 | 0.5 ± 0.1 | 0.2 ± 0.1 | 0.2 ± 0.1 |
| Outcome | All Cohorts | Gipuzkoa | Sabadell | Valencia |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |
| Glucose intolerance | ||||
| No | 1682 (74.3) | 538 (84.6) | 390 (50.2) | 754 (88.7) |
| Yes | 268 (11.8) | 40 (6.3) | 186 (23.9) | 42 (4.9) |
| Missing | 313 (13.8) | 58 (9.1) | 201 (25.9) | 54 (6.4) |
| Total Cholesterol | ||||
| Normal (<190 mg/dL) | 915 (40.4) | 299 (47.0) | 332 (42.7) | 284 (33.4) |
| High (≥190 mg/dL) | 1074 (47.5) | 321 (50.5) | 302 (38.9) | 451 (53.1) |
| Missing | 274 (12.1) | 16 (2.5) | 143 (18.4) | 115 (13.5) |
| Total Triglycerides | ||||
| Normal (<175 mg/dL) | 1857 (82.1) | 598 (94.0) | 585 (75.3) | 674 (79.3) |
| High (≥175 mg/dL) | 130 (5.7) | 22 (3.5) | 49 (6.3) | 59 (6.9) |
| Missing | 276 (12.2) | 16 (2.5) | 143 (18.4) | 117 (13.8) |
| Outcome | Glucose Intolerance | High Total Cholesterol (≥190 mg/dL) | High Total Triglycerides (≥175 mg/dL) |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| PM2.5 | |||
| per 5 µg/m3 | 1.02 (0.85, 1.21) | 0.99 (0.88, 1.11) | 0.95 (0.76, 1.18) |
| High (≥25 µg/m3) | 1.16 (0.82 1.63) b | 1.14 (0.90, 1.44) | 0.89 (0.58, 1.37) |
| NO2 | |||
| per 10 µg/m3 | 0.99 (0.89, 1.11) | 1.05 (0.98, 1.13) | 0.85 (0.74, 0.98) |
| High (≥39.8 µg/m3) | 1.05 (0.76, 1.44) c | 1.11 (0.88, 1.39) | 0.70 (0.45, 1.08) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rammah, A.; Whitworth, K.W.; Amos, C.I.; Estarlich, M.; Guxens, M.; Ibarluzea, J.; Iñiguez, C.; Subiza-Pérez, M.; Vrijheid, M.; Symanski, E. Air Pollution, Residential Greenness and Metabolic Dysfunction during Early Pregnancy in the INfancia y Medio Ambiente (INMA) Cohort. Int. J. Environ. Res. Public Health 2021, 18, 9354. https://doi.org/10.3390/ijerph18179354
Rammah A, Whitworth KW, Amos CI, Estarlich M, Guxens M, Ibarluzea J, Iñiguez C, Subiza-Pérez M, Vrijheid M, Symanski E. Air Pollution, Residential Greenness and Metabolic Dysfunction during Early Pregnancy in the INfancia y Medio Ambiente (INMA) Cohort. International Journal of Environmental Research and Public Health. 2021; 18(17):9354. https://doi.org/10.3390/ijerph18179354
Chicago/Turabian StyleRammah, Amal, Kristina W. Whitworth, Christopher I. Amos, Marisa Estarlich, Mònica Guxens, Jesús Ibarluzea, Carmen Iñiguez, Mikel Subiza-Pérez, Martine Vrijheid, and Elaine Symanski. 2021. "Air Pollution, Residential Greenness and Metabolic Dysfunction during Early Pregnancy in the INfancia y Medio Ambiente (INMA) Cohort" International Journal of Environmental Research and Public Health 18, no. 17: 9354. https://doi.org/10.3390/ijerph18179354
APA StyleRammah, A., Whitworth, K. W., Amos, C. I., Estarlich, M., Guxens, M., Ibarluzea, J., Iñiguez, C., Subiza-Pérez, M., Vrijheid, M., & Symanski, E. (2021). Air Pollution, Residential Greenness and Metabolic Dysfunction during Early Pregnancy in the INfancia y Medio Ambiente (INMA) Cohort. International Journal of Environmental Research and Public Health, 18(17), 9354. https://doi.org/10.3390/ijerph18179354