
Self-Reported Diabetes Mellitus and Tooth Extraction Due to Periodontal Disease and Dental Caries in the Japanese Population

 , ,
, ,
Abstract
1. Introduction
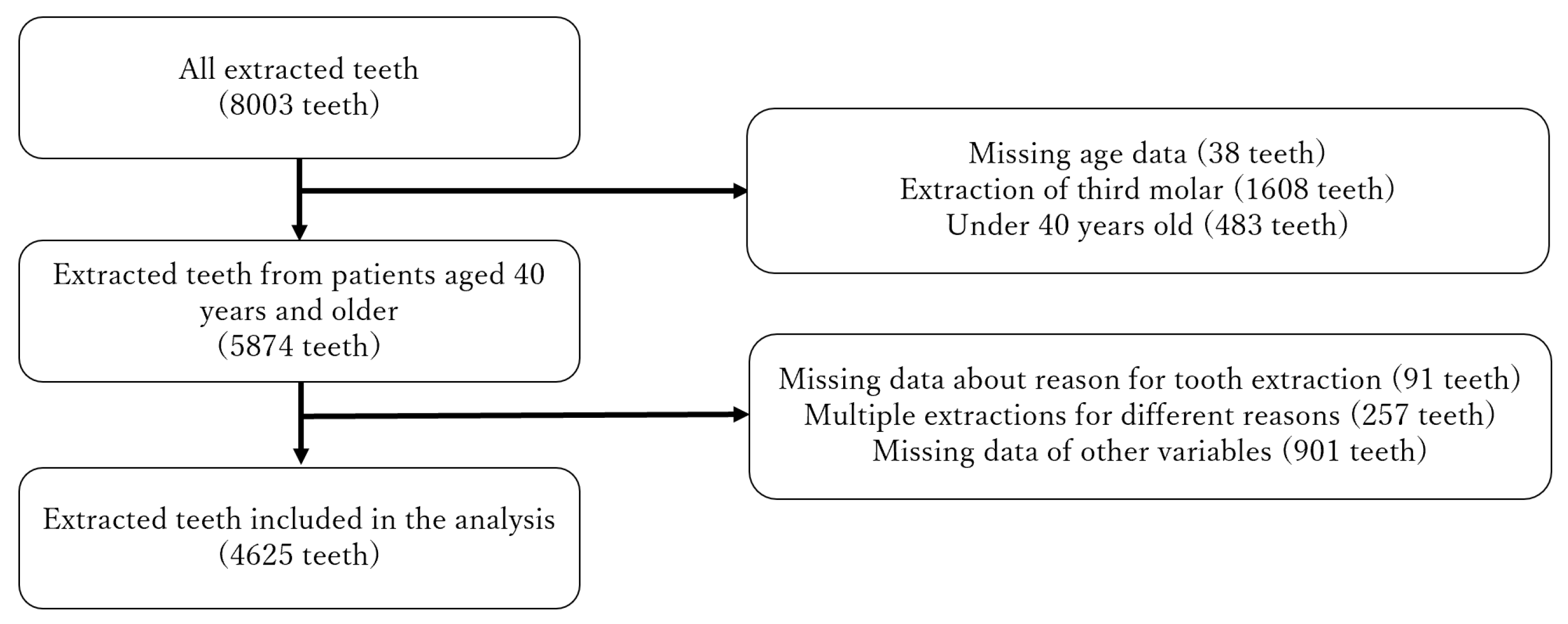
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Reasons for Tooth Extraction
2.3. Diabetes Mellitus and Other Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leite, R.S.; Marlow, N.M.; Fernandes, J.K.; Hermayer, K. Oral Health and type 2 diabetes. Am. J. Med. Sci. 2013, 345, 271–273. [Google Scholar] [CrossRef]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef]
- Graves, D.T.; Ding, Z.; Yang, Y. The impact of diabetes on periodontal diseases. Periodontol. 2000 2020, 82, 214–224. [Google Scholar] [CrossRef]
- Borgnakke, W.S.; Ylöstalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, S135–S152. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Graziani, F.; Hasturk, H. Effects of periodontal disease on glycemic control, complications, and incidence of diabetes mellitus. Periodontol. 2000 2020, 83, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.S.; Amaro, I.F.; Caramelo, F.; Paula, A.; Marto, C.M.; Ferreira, M.M.; Botelho, M.F.; Carrilho, E.V. Dental caries, diabetes mellitus, metabolic control and diabetes duration: A systematic review and meta-analysis. J. Esthet. Restor. Dent. 2020, 32, 291–309. [Google Scholar] [CrossRef] [PubMed]
- de Lima, A.K.A.; Dos Santos, J.A.; Stefani, C.M.; de Lima, A.D.; Damé-Teixeira, N. Diabetes mellitus and poor glycemic control increase the occurrence of coronal and root caries: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 3801–3812. [Google Scholar] [CrossRef] [PubMed]
- Latti, B.R.; Kalburge, J.V.; Birajdar, S.B.; Latti, R.G. Evaluation of relationship between dental caries, diabetes mellitus and oral microbiota in diabetics. J. Oral. Maxillofac. Pathol. JOMFP 2018, 22, 282. [Google Scholar] [CrossRef] [PubMed]
- López-Gómez, S.A.; González-López, B.S.; Scougall-Vilchis, R.J.; Pontigo-Loyola, A.P.; Márquez-Corona, M.L.; Villalobos-Rodelo, J.J.; Rueda-Ibarra, V.; Medina-Solís, C.E. Tooth loss in patients with and without diabetes: A large-scale, cross-sectional study of Mexican adults. J. Am. Dent. Assoc. 2020, 151, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Noda, T.; Nishioka, Y.; Imamura, T.; Kamijo, H.; Sugihara, N. Evaluation of tooth loss among patients with diabetes mellitus using the National Database of Health Insurance Claims and Specific Health Checkups of Japan. Int. Dent. J. 2020, 70, 308–315. [Google Scholar] [CrossRef]
- Taylor, G.W.; Manz, M.C.; Borgnakke, W.S. Diabetes, periodontal diseases, dental caries, and tooth loss: A review of the literature. Compend. Contin. Educ. Dent. 2004, 25, 179–184. [Google Scholar]
- Morita, M.; Kimura, T.; Kanegae, M.; Ishikawa, A.; Watanabe, T. Reasons for extraction of permanent teeth in Japan. Community Dent. Oral Epidemiol. 1994, 22, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Sugihara, S.; Kamijo, H.; Morita, M.; Kawato, T.; Tsuneishi, M.; Kobayashi, K.; Hasuike, Y.; Sato, T. Reasons for Tooth Extractions in Japan: The Second Nationwide Survey. Int. Dent. J. 2021, in press. [Google Scholar] [CrossRef]
- The Ministry of Health, Labour, and Welfare. National Health and Nutrition Survey. 2012. Available online: https://www.nibiohn.go.jp/eiken/english/research/pdf/nhns2012.pdf (accessed on 1 August 2021).
- Al-Shammari, K.F.; Al-Khabbaz, A.K.; Al-Ansari, J.M.; Neiva, R.; Wang, H.L. Risk indicators for tooth loss due to periodontal disease. J. Periodontol. 2005, 76, 1910–1918. [Google Scholar] [CrossRef] [PubMed]
- Goto, A.; Morita, A.; Goto, M.; Sasaki, S.; Miyachi, M.; Aiba, N.; Kato, M.; Terauchi, Y.; Noda, M.; Watanabe, S. Validity of diabetes self-reports in the Saku diabetes study. J. Epidemiol. 2013, 23, 295–300. [Google Scholar] [CrossRef]
- Fukuda, Y.; Nakao, H.; Yahata, Y.; Imai, H. Are health inequalities increasing in Japan? The trends of 1955 to 2000. BioSci. Trends 2007, 1, 38–42. [Google Scholar]
- Jacobs, A.J. Japan’s Evolving Nested Municipal Hierarchy: The Race for Local Power in the 2000s. Urban Stud. Res. 2011, 2011, 692764. [Google Scholar] [CrossRef]
- Kocher, T.; König, J.; Borgnakke, W.S.; Pink, C.; Meisel, P. Periodontal complications of hyperglycemia/diabetes mellitus: Epidemiologic complexity and clinical challenge. Periodontol. 2000 2018, 78, 59–97. [Google Scholar] [CrossRef] [PubMed]
- Greenblatt, A.P.; Salazar, C.R.; Northridge, M.E.; Kaplan, R.C.; Taylor, G.W.; Finlayson, T.L.; Qi, Q.; Badner, V. Association of diabetes with tooth loss in Hispanic/Latino adults: Findings from the Hispanic Community Health Study/Study of Latinos. BMJ Open Diabetes Res. Care 2016, 4, e000211. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Kim, D.W.; Kim, M.Y.; Kim, Y.T.; Yoon, J.H. The effect of diabetes on tooth loss caused by periodontal disease: A nationwide population-based cohort study in South Korea. J. Periodontol. 2019, 90, 576–583. [Google Scholar] [CrossRef]
- Haseeb, M.; Khawaja, K.I.; Ataullah, K.; Munir, M.B.; Fatima, A. Periodontal disease in type 2 diabetes mellitus. J. Coll. Physicians Surg. Pak. 2012, 22, 514–518. [Google Scholar] [PubMed]
- Yoshino, K.; Ishizuka, Y.; Watanabe, H.; Fukai, K.; Sugihara, N.; Matsukubo, T. Sex- and age-based differences in single tooth loss in adults. Bull. Tokyo Dent. Coll. 2015, 56, 63–67. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Miyachi, T. Clinical evaluation and risk analysis for partially edentulous arch. Ann. Jpn. Prosthodont. Soc. 2013, 5, 21–27. [Google Scholar] [CrossRef]
- Passanezi, E.; Sant’Ana, A.C.P. Role of occlusion in periodontal disease. Periodontol. 2000 2019, 79, 129–150. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Self-Reported Diabetes Mellitus | ||||
|---|---|---|---|---|---|
| Yes (N = 455) | No (N = 4170) | p-Value a | |||
| N | % | n | % | ||
| Sex | <0.001 | ||||
| Male | 262 | 57.6 | 2001 | 48.0 | |
| Female | 193 | 42.4 | 2169 | 52.0 | |
| Age (years) | <0.001 | ||||
| 40–49 | 11 | 2.4 | 417 | 10.0 | |
| 50–59 | 42 | 9.2 | 728 | 17.5 | |
| 60–69 | 145 | 31.9 | 1188 | 28.5 | |
| 70–79 | 173 | 38.0 | 1148 | 27.5 | |
| ≥80 | 84 | 18.5 | 689 | 16.5 | |
| Location | 0.071 | ||||
| Rural | 388 | 85.3 | 3411 | 81.8 | |
| Urban | 67 | 14.7 | 759 | 18.2 | |
| Number of teeth before extraction | <0.001 | ||||
| <20 | 273 | 60.0 | 1994 | 47.8 | |
| ≥20 | 182 | 40.0 | 2176 | 52.2 | |
| Smoking status | >0.999 | ||||
| Current smoker | 92 | 20.2 | 842 | 20.2 | |
| Nonsmoker | 363 | 79.8 | 3328 | 79.8 | |
| Tooth type | <0.001 | ||||
| Anterior | 187 | 41.1 | 1349 | 32.4 | |
| Premolar | 134 | 29.5 | 1149 | 27.6 | |
| Molar | 134 | 29.5 | 1672 | 40.1 | |
| Reason for tooth extraction | 0.002 | ||||
| Dental caries | 98 | 21.5 | 1026 | 24.6 | |
| Periodontal disease | 252 | 55.4 | 1947 | 46.7 | |
| Others | 105 | 23.1 | 1197 | 28.8 | |
| Reason for Tooth Extraction | <20 Teeth | ≥20 Teeth | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Self-Reported Diabetes Mellitus | Self-Reported Diabetes Mellitus | |||||||||
| Yes (N = 273) | No (N = 1994) | p-Value a | Yes (N = 182) | No (N = 2176) | p-Value a | |||||
| n | % | n | % | n | % | n | % | |||
| Dental caries | 59 | 21.6 | 502 | 25.2 | 0.411 | 39 | 21.4 | 524 | 24.1 | 0.014 |
| Periodontal disease | 163 | 59.7 | 1119 | 56.1 | 89 | 48.9 | 828 | 38.1 | ||
| Other reasons | 51 | 40.3 | 875 | 43.9 | 54 | 29.7 | 824 | 37.9 | ||
| Reason for Tooth Extraction | Anterior | Premolar | Molar | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Self-Reported Diabetes Mellitus | p-Value | Self-Reported Diabetes Mellitus | p-Value | Self-Reported Diabetes Mellitus | p-Value | ||||||||||
| Yes | No | Yes | No | Yes | No | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||||
| Upper | 0.009 | 0.759 | 0.969 | ||||||||||||
| Dental caries | 14 | 13.0 | 177 | 22.4 | 20 | 28.2 | 174 | 27.6 | 18 | 26.5 | 226 | 27.8 | |||
| Periodontal disease | 70 | 64.8 | 393 | 49.7 | 30 | 42.3 | 244 | 38.7 | 33 | 48.5 | 384 | 47.3 | |||
| Others | 24 | 22.2 | 221 | 27.9 | 21 | 29.6 | 213 | 33.8 | 17 | 25.0 | 202 | 24.9 | |||
| Total | 108 | 100 | 791 | 100 | 71 | 100 | 631 | 100 | 68 | 100 | 812 | 100 | |||
| Lower | 0.859 | 0.151 | |||||||||||||
| Dental caries | 12 | 15.2 | 93 | 16.7 | 17 | 27.0 | 132 | 25.5 | 0.506 | 17 | 25.8 | 224 | 26.0 | ||
| Periodontal disease | 58 | 73.4 | 393 | 70.4 | 29 | 46.0 | 209 | 40.3 | 32 | 48.5 | 324 | 37.7 | |||
| Others | 9 | 11.4 | 72 | 12.9 | 17 | 27.0 | 177 | 34.2 | 17 | 25.8 | 312 | 36.3 | |||
| Total | 79 | 100 | 558 | 100 | 63 | 100 | 518 | 100 | 66 | 100 | 860 | 100 | |||
| Model 1 a | Model 2 b | Model 3 c | Model 4 d | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Dental Caries | ||||||||||||
| Diabetes mellitus | ||||||||||||
| No | 1 | 1 | 1 | 1 | ||||||||
| Yes | 0.70 | 0.58–0.86 | <0.001 | 0.87 | 0.71–1.06 | 0.169 | 0.87 | 0.71–1.06 | 0.171 | 0.85 | 0.68–1.06 | 0.14 |
| Periodontal Disease | ||||||||||||
| Diabetes mellitus | ||||||||||||
| No | 1 | 1 | 1 | 1 | ||||||||
| Yes | 1.417 | 1.17–1.72 | <0.001 | 1.31 | 1.07–1.59 | 0.008 | 1.23 | 1.01–1.51 | 0.026 | 1.23 | 1.01–1.50 | 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, S.; Sugihara, N.; Kamijo, H.; Morita, M.; Kawato, T.; Tsuneishi, M.; Kobayashi, K.; Hasuike, Y.; Sato, T. Self-Reported Diabetes Mellitus and Tooth Extraction Due to Periodontal Disease and Dental Caries in the Japanese Population. Int. J. Environ. Res. Public Health 2021, 18, 9024. https://doi.org/10.3390/ijerph18179024
Suzuki S, Sugihara N, Kamijo H, Morita M, Kawato T, Tsuneishi M, Kobayashi K, Hasuike Y, Sato T. Self-Reported Diabetes Mellitus and Tooth Extraction Due to Periodontal Disease and Dental Caries in the Japanese Population. International Journal of Environmental Research and Public Health. 2021; 18(17):9024. https://doi.org/10.3390/ijerph18179024
Chicago/Turabian StyleSuzuki, Seitaro, Naoki Sugihara, Hideyuki Kamijo, Manabu Morita, Takayuki Kawato, Midori Tsuneishi, Keita Kobayashi, Yoshihiro Hasuike, and Tamotsu Sato. 2021. "Self-Reported Diabetes Mellitus and Tooth Extraction Due to Periodontal Disease and Dental Caries in the Japanese Population" International Journal of Environmental Research and Public Health 18, no. 17: 9024. https://doi.org/10.3390/ijerph18179024
APA StyleSuzuki, S., Sugihara, N., Kamijo, H., Morita, M., Kawato, T., Tsuneishi, M., Kobayashi, K., Hasuike, Y., & Sato, T. (2021). Self-Reported Diabetes Mellitus and Tooth Extraction Due to Periodontal Disease and Dental Caries in the Japanese Population. International Journal of Environmental Research and Public Health, 18(17), 9024. https://doi.org/10.3390/ijerph18179024