
Workplace Well-Being and Intent to Stay by Health Care Workers Reassigned during the First COVID-19 Wave: Results of a Swiss Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.2.1. Outcomes
2.2.2. Independent Variables
2.3. Statistical Analyses
3. Results
3.1. Descriptive and Bivariate Analyses
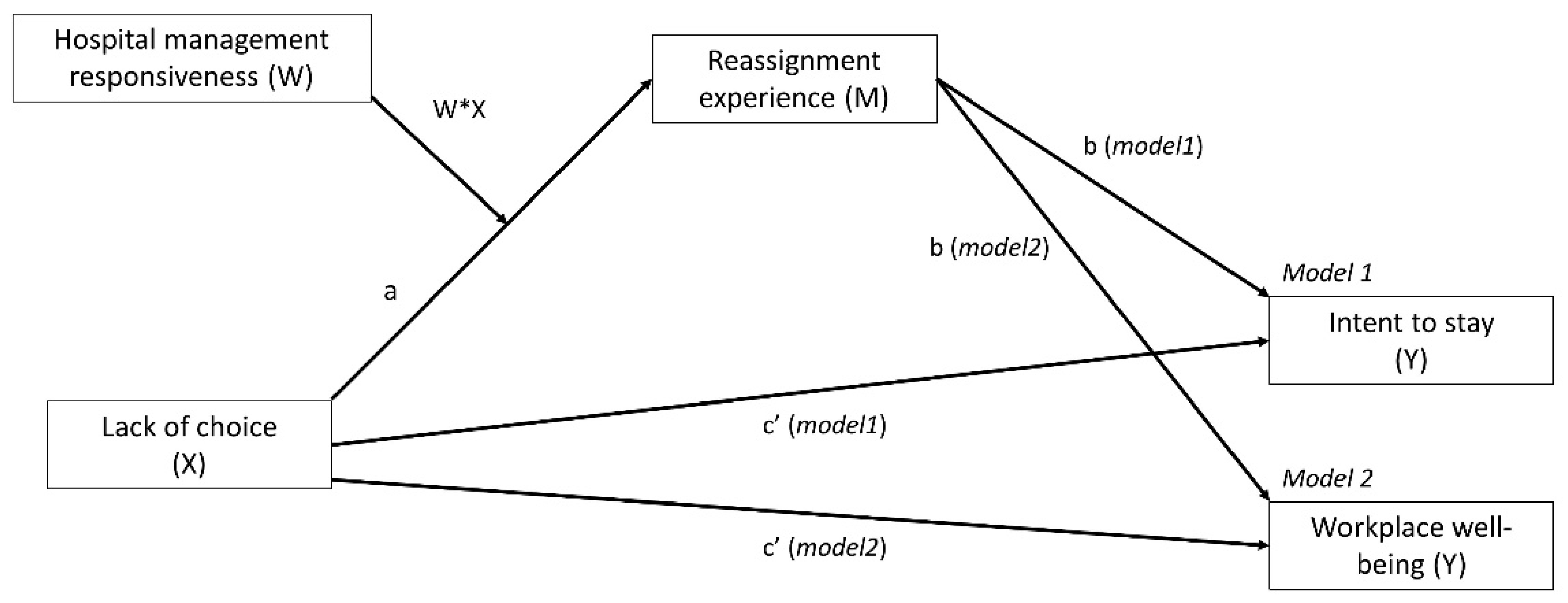
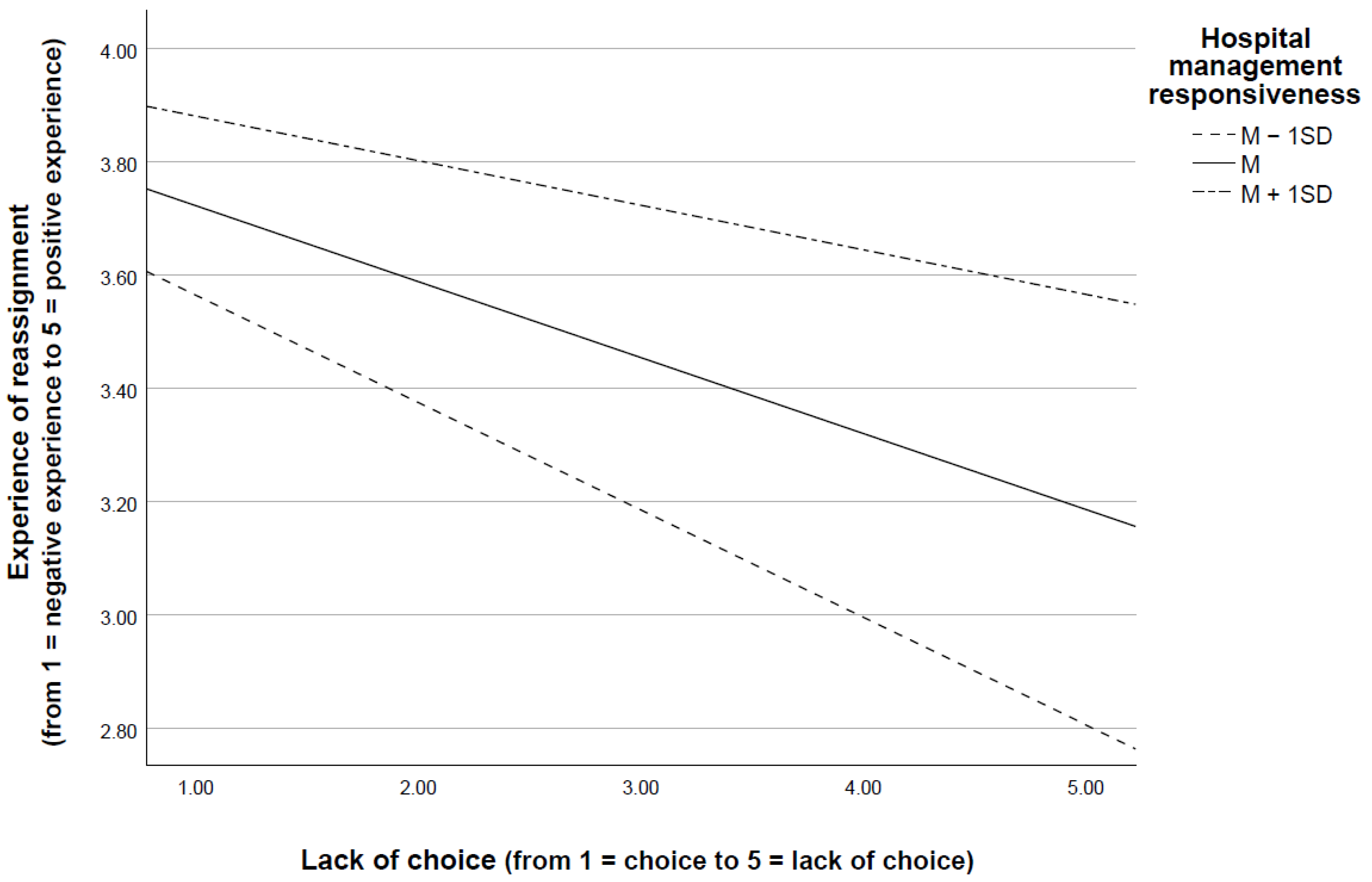
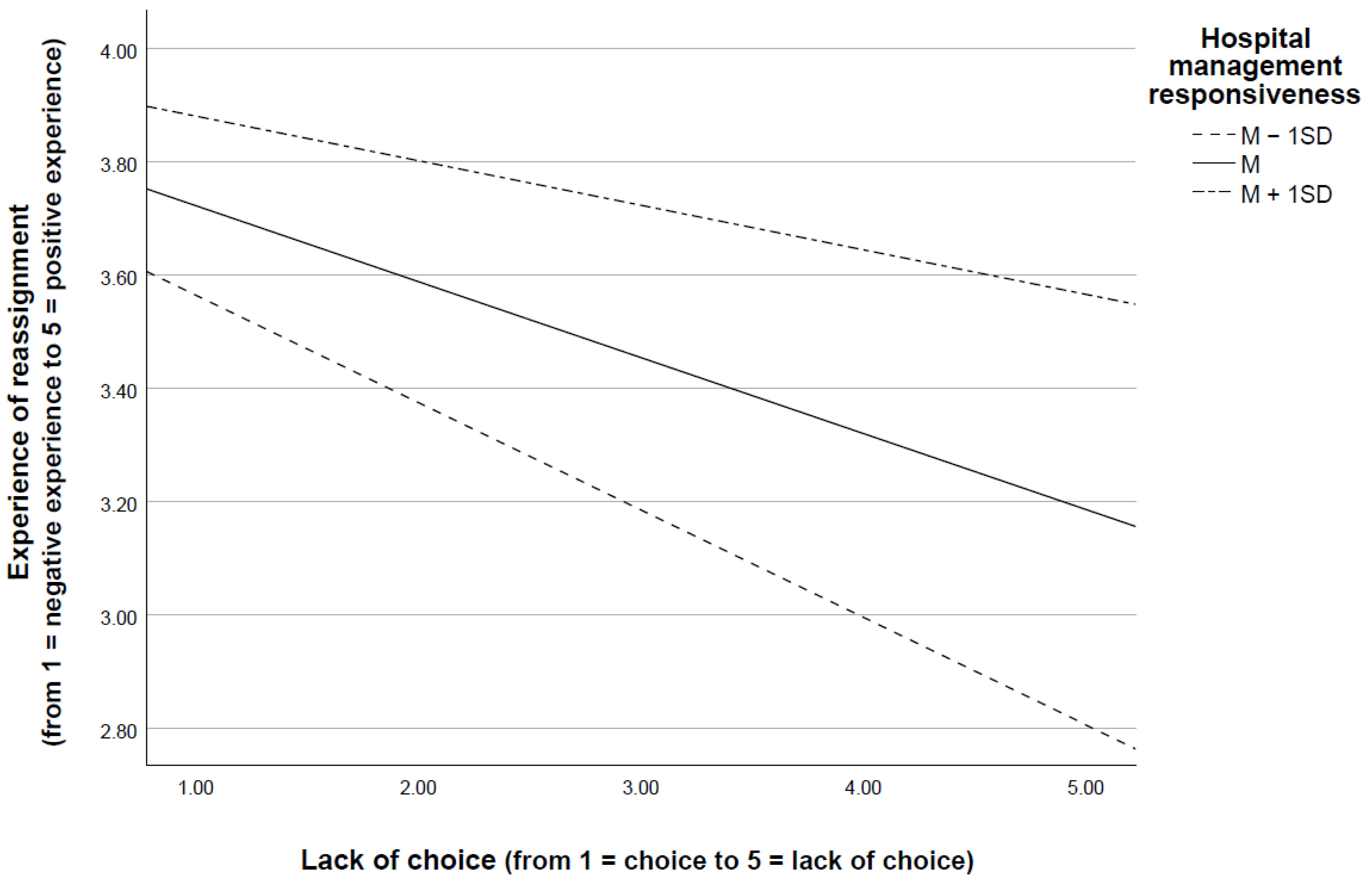
3.2. Moderated Mediation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Dependent Variable | |||||||||
|---|---|---|---|---|---|---|---|---|---|
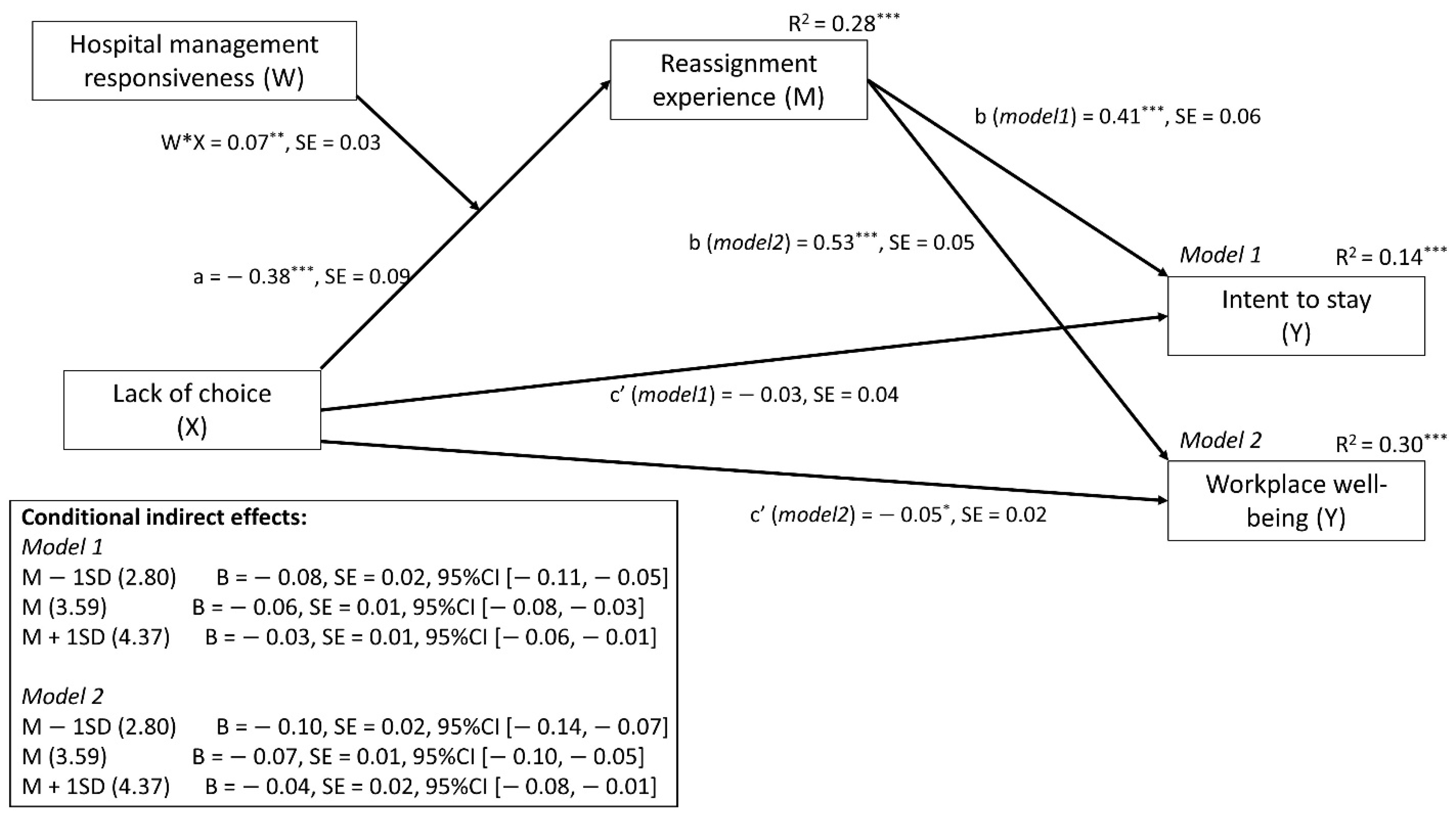
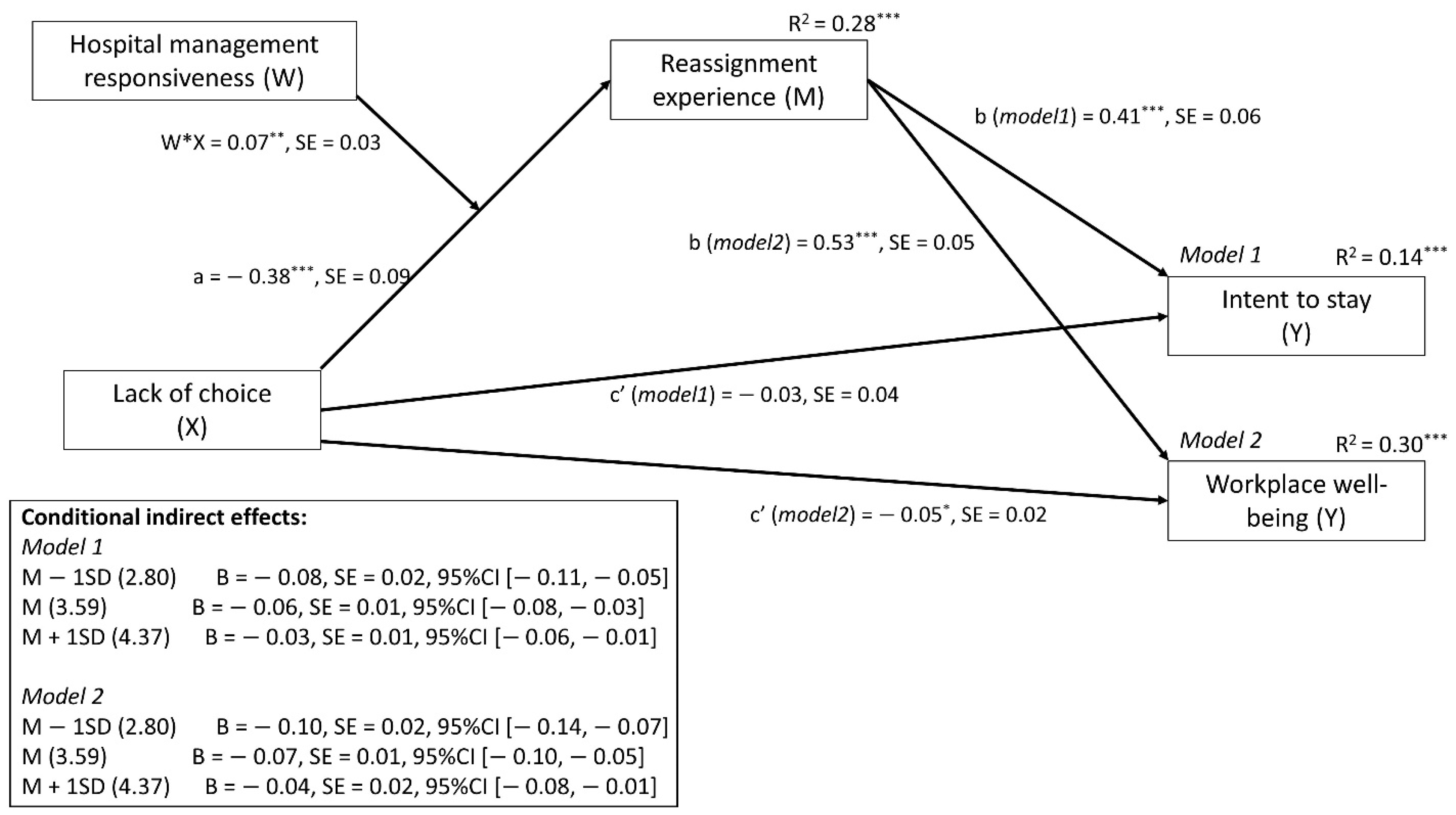
| Reassignment Experience (M) R2 = 0.28 *** | Intent to Stay (Model 1) R2 = 0.14 *** | Workplace Well-Being (Model 2) R2 = 0.30 *** | |||||||
| B | SE | 95% CI | B | SE | 95% CI | B | SE | 95% CI | |
| Lack of choice (X; direct effect) | −0.38 *** | 0.09 | [−0.56, −0.20] | −0.06 | 0.04 | [−0.13, 0.01] | −0.05 * | 0.02 | [−0.10, −0.01] |
| Reassignment experience (M) | -- | -- | -- | 0.41 *** | 0.06 | [0.29, 0.54] | 0.53 *** | 0.05 | [0.43, 0.64] |
| Hospital management responsiveness (W) | 0.14 *** | 0.09 | [-0.04, 0.32] | -- | -- | -- | -- | -- | -- |
| Lack of choice × Hospital management responsiveness (M * W) | 0.07 ** | 0.03 | [0.02, 0.12] | -- | -- | -- | -- | -- | -- |
| Conditional indirect Effects of Lack of choice | |||||||||
| Mean − 1 SD (2.80) | -- | -- | -- | −0.08 | 0.02 | [−0.11, −0.05] | −0.10 | 0.02 | [−0.14, −0.07] |
| Mean (3.60) | -- | -- | -- | −0.06 | 0.01 | [−0.08, −0.03] | −0.07 | 0.01 | [−0.10, −0.05] |
| Mean + 1 SD (4.40) | -- | -- | -- | −0.03 | 0.01 | [−0.06. −0.01] | −0.04 | 0.02 | [−0.08, −0.01] |
| Moderated mediation index (bootstrapped SE and IC) | -- | -- | -- | 0.03 | 0.01 | [0.01, 0.05] | 0.04 | 0.01 | [0.01, 0.06] |
References
- World Health Organisation Website. WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 19 August 2021).
- Adams, J.G.; Walls, R.M. Supporting the health care workforce during the covid-19 global epidemic. JAMA 2020, 323, 1439. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Seale, H.; Leask, J.; Po, K.; MacIntyre, C.R. “Will they just pack up and leave?” Attitudes and intended behaviour of hospital health care workers during an influenza pandemic. BMC Health Serv. Res. 2009, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA 2020, 323, 2133. [Google Scholar] [CrossRef]
- Clark, C.C. In harm’s way: AMA physicians and the duty to treat. J. Med. Philos. 2005, 30, 65–87. [Google Scholar] [CrossRef] [PubMed]
- McConnell, D. Balancing the duty to treat with the duty to family in the context of the COVID-19 pandemic. J. Med. Ethics 2020, 46, 360–363. [Google Scholar] [CrossRef]
- Shabanowitz, R.B.; Reardon, J.E. Avian flu pandemic—Flight of the healthcare worker? HEC Forum 2009, 21, 365–385. [Google Scholar] [CrossRef]
- Damery, S.; Draper, H.; Wilson, S.; Greenfield, S.; Ives, J.; Parry, J.; Petts, J.; Sorell, T. Healthcare workers’ perceptions of the duty to work during an influenza pandemic. J. Med. Ethics 2009, 36, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Lim, M.K.; Chia, S.E.; Ko, S.M.; Qian, F.; Ng, V.; Tan, B.H.; Wong, K.S.; Chew, W.M.; Tang, H.K.; et al. Risk perception and impact of severe acute respiratory syndrome (SARS) on work and personal lives of healthcare workers in Singapore. Med. Care 2005, 43, 676–682. [Google Scholar] [CrossRef]
- Koh, Y.; Hegney, D.; Drury, V. Nurses’ perceptions of risk from emerging respiratory infectious diseases: A Singapore study. Int. J. Nurs. Pract. 2012, 18, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Sultan, M.A.S.; Løwe Sørensen, J.; Carlström, E.; Mortelmans, L.; Khorram-Manesh, A. Emergency healthcare providers’ perceptions of preparedness and willingness to work during disasters and public health emergencies. Healthcare 2020, 8, 442. [Google Scholar] [CrossRef]
- Martin, S.D.; Brown, L.; Reid, W.M. Predictors of nurses’ intentions to work during the 2009 influenza A (H1N1) pandemic. AJN Am. J. Nurs. 2013, 113, 24–31. [Google Scholar] [CrossRef]
- Shiao, J.S.-C.; Koh, D.; Lo, L.-H.; Lim, M.-K.; Guo, Y.L. Factors Predicting nurses’ consideration of leaving their job during the sars outbreak. Nurs. Ethics 2007, 14, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Colosi, B. 2021 NSI National Health Care Retention & RN Staffing Report. 2021. Available online: https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf (accessed on 19 August 2021).
- British Medical Association Website. Available online: https://www.bma.org.uk/advice-and-support/covid-19/what-the-bma-is-doing/covid-19-analysing-the-impact-of-coronavirus-on-doctors (accessed on 19 August 2021).
- Bensimon, C.M.; Tracy, C.S.; Bernstein, M.; Shaul, R.Z.; Upshur, R.E. A qualitative study of the duty to care in communicable disease outbreaks. Soc. Sci. Med. 2007, 65, 2566–2575. [Google Scholar] [CrossRef]
- Bryson, A. Managerial responsiveness to union and nonunion worker voice in Britain. Ind. Relat. J. Econ. Soc. 2004, 43, 213–241. [Google Scholar] [CrossRef]
- Holland, P.J.; Allen, B.C.; Cooper, B.K. Reducing burnout in Australian nurses: The role of employee direct voice and managerial responsiveness. Int. J. Hum. Resour. Manag. 2013, 24, 3146–3162. [Google Scholar] [CrossRef]
- Belfroid, E.; van Steenbergen, J.; Timen, A.; Ellerbroek, P.; Huis, A.; Hulscher, M. Preparedness and the importance of meeting the needs of healthcare workers: A qualitative study on Ebola. J. Hosp. Infect. 2017, 98, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef] [PubMed]
- Spalluto, L.B.; Planz, V.B.; Stokes, L.S.; Pierce, R.; Aronoff, D.M.; McPheeters, M.L.; Omary, R.A. Transparency and trust during the Coronavirus disease 2019 (COVID-19) Pandemic. J. Am. Coll. Radiol. 2020, 17, 909–912. [Google Scholar] [CrossRef]
- Marjanovic, Z.; Greenglass, E.R.; Coffey, S. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: An online questionnaire survey. Int. J. Nurs. Stud. 2007, 44, 991–998. [Google Scholar] [CrossRef]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.-W.; Oishi, S.; Biswas-Diener, R. New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 2009, 97, 143–156. [Google Scholar] [CrossRef]
- Fisher, C.D. Conceptualizing and measuring wellbeing at work. In Wellbeing; Cooper, C.L., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2014; pp. 1–25. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Hayes, A.F. An index and test of linear moderated mediation. Multivar. Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef] [PubMed]
- Coto, J.; Restrepo, A.; Cejas, I.; Prentiss, S. The impact of COVID-19 on allied health professions. PLoS ONE 2020, 15, e0241328. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Tan, B.Y.; Kanneganti, A.; Lim, L.J.; Tan, M.; Chua, Y.X.; Tan, L.; Sia, C.H.; Denning, M.; Goh, E.T.; Purkayastha, S.; et al. Burnout and associated factors among health care workers in Singapore during the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 1751–1758.e5. [Google Scholar] [CrossRef]
- Barry, J.M. The Great Influenza: The Epic Story of the Deadliest Plague in History; Penguin Books: New York, NY, USA, 2005; p. 546. [Google Scholar]
- Hilliard, M.T. The duty to care: When health care workers face personal risk. Natl. Cathol. Bioeth. Q. 2007, 7, 673–682. [Google Scholar] [CrossRef]
- Mackler, N.; Wilkerson, W.; Cinti, S. Will First-Responders Show Up for Work During a Pandemic? Lessons from a Smallpox Vaccination Survey of Paramedics. Disaster Manag. Response 2007, 5, 45–48. [Google Scholar] [CrossRef]
- Qureshi, K.; Gershon, R.R.M.; Sherman, M.F.; Straub, M.T.; Gebbie, E.; Mccollum, M.; Erwin, M.M.J.; Morse, S.S. Health care workers’ ability and willingness to report to duty during catastrophic disasters. J. Hered. 2005, 82, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Cowden, T.; Cummings, G.; Profetto-McGrath, J. Leadership practices and staff nurses’ intent to stay: A systematic review. J. Nurs. Manag. 2011, 19, 461–477. [Google Scholar] [CrossRef]
- Wong, T.W.; Yau, J.K.; Chan, C.L.; Kwong, R.S.; Ho, S.M.; Lau, C.C.; Lau, F.L.; Lit, C.H. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur. J. Emerg. Med. 2005, 12, 13–18. [Google Scholar] [CrossRef]
- Savitsky, B.; Radomislensky, I.; Hendel, T. Nurses’ occupational satisfaction during Covid-19 pandemic. Appl. Nurs. Res. 2021, 59, 151416. [Google Scholar] [CrossRef]
- Di Trani, M.; Mariani, R.; Ferri, R.; De Berardinis, D.; Frigo, M.G. From resilience to burnout in healthcare workers during the COVID-19 emergency: The role of the ability to tolerate uncertainty. Front. Psychol. 2021, 12, 646435. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, B.P.; Hanses, F.; Salzberger, B. Influenza pandemic and professional duty: Family or patients first? A survey of hospital employees. BMC Public Health 2006, 6, 311–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malm, H.; May, T.; Francis, L.; Omer, S.B.; Salmon, D.; Hood, R. Ethics, pandemics, and the duty to treat. Am. J. Bioeth. 2008, 8, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Simonds, A.K.; Sokol, D.K. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur. Respir. J. 2009, 34, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Ives, J.; Greenfield, S.; Parry, J.M.; Draper, H.; Gratus, C.; Petts, J.I.; Sorell, T.; Wilson, S. Healthcare workers’ attitudes to working during pandemic influenza: A qualitative study. BMC Public Health 2009, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Karasek, R.A. Job Demands, job decision latitude, and mental strain: Implications for job redesign. Adm. Sci. Q. 1979, 24, 285. [Google Scholar] [CrossRef]
- Nei, D.; Snyder, L.A.; Litwiller, B.J. Promoting retention of nurses. Health Care Manag. Rev. 2015, 40, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.C. The development of a method of measuring job satisfaction: The Cornell studies. In Personnel and Industrial Psychology, 3rd ed.; Dorsey Press: Homewood, IL, USA, 1974; pp. 272–279. [Google Scholar]
- Lu, H.; Zhao, Y.; While, A. Job satisfaction among hospital nurses: A literature review. Int. J. Nurs. Stud. 2019, 94, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Crede, M.; Chernyshenko, O.S.; Stark, S.; Dalal, R.S.; Bashshur, M. Job satisfaction as mediator: An assessment of job satisfaction’s position within the nomological network. J. Occup. Organ. Psychol. 2007, 80, 515–538. [Google Scholar] [CrossRef]
- Bayarçelik, E.B.; Findikli, M.A. The mediating effect of job satisfaction on the relation between organizational justice perception and intention to leave. Procedia-Soc. Behav. Sci. 2016, 235, 403–411. [Google Scholar] [CrossRef]

| Characteristics | A n (%) | B n (%) | C n (%) |
|---|---|---|---|
| Count. | 436 | 2811 | 8645 |
| Gender | |||
| Women | 327 (76.6) | 2129 (78.1) | 6510 (75.3) |
| Men | 100 (3.4) | 598 (21.9) | 2135 (24.7) |
| Age | |||
| <30 years | 95 (22.1) | 507 (18.5) | 1729 (20.0) |
| 30–39 years | 119 (27.7) | 739 (27.0) | 2282 (26.4) |
| 40–49 years | 125 (29.1) | 687 (25.0) | 2058 (23.8) |
| ≥50 years | 91 (21.2) | 807 (29.5) | 2576 (29.8) |
| Length of professional experience | |||
| <3 years | 96 (22.3) | 659 (24.1) | 3130 (36.2) |
| 3–5 years | 97 (22.5) | 554 (20.2) | 1565 (18.1) |
| 6–10 years | 80 (18.6) | 557 (20.4) | 1279 (14.8) |
| >10 years | 158 (36.7) | 967 (35.3) | 2671 (30.9) |
| Professional group | |||
| Administration (patients’ reception staff) and logistics | 34 (7.9) | 702 (24.9) | 2447 (28.3) |
| Physicians | 36 (8.4) | 191 (6.9) | 1020 (11.8) |
| Nurses and nurse assistants | 273 (63.9) | 1323 (47.1) | 3882 (44.9) |
| Other HCWs (e.g., psychologists, physiotherapists, radiologists, pharmacists) | 81 (19.0) | 463 (16.4) | 752 (8.7) |
| Other (e.g., students) | 12 (2.8) | 132 (4.7) | 545 (6.3) |
| Reassignments | |||
| No reassignment | NA | 1960 (70.6) | -- |
| Reassignment in a facility not dedicated to COVID-19 patient care 1 | NA | 382 (13.7) | -- |
| Reassignment to COVID-19 patient care facilities | NA | 436 (15.7) | -- |
| Having had symptoms compatible with COVID-19 | |||
| Yes and confirmed by a positive test | 16 (3.7) | 113 (4.1) | -- |
| Yes but not confirmed by a test | 59 (13.5) | 258 (9.3) | -- |
| Yes but the test was negative | 56 (12.8) | 284 (10.2) | |
| No or don’t know | 305 (70.0) | 2122 (76.4) | -- |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|
| 1. Gender | 0.00 | −0.04 | 0.00 | 0.02 | −0.04 | −0.05 | 0.00 | 0.01 |
| 2. Age | -- | 0.60 *** | −0.09 | 0.07 | −0.07 | 0.05 | 0.04 | 0.02 |
| 3. Length work. exp. | -- | −0.08 | 0.02 | −0.02 | 0.05 | 0.02 | −0.05 | |
| 4. Threat of infection | -- | 0.18 ** | −0.18 ** | −0.21 ** | −0.08 | −0.09 | ||
| 5. Lack of choice | -- | −0.35 *** | −0.22 *** | −0.28 *** | −0.19 *** | |||
| 6. Reass. experience | -- | 0.45 *** | 0.54 *** | 0.32 *** | ||||
| 7. Hosp. man. respons. | -- | 0.53 *** | 0.49 *** | |||||
| 8. WWB | -- | 0.49 *** | ||||||
| 9. Intent to stay | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilles, I.; Mabire, C.; Perriraz, M.; Peytremann-Bridevaux, I. Workplace Well-Being and Intent to Stay by Health Care Workers Reassigned during the First COVID-19 Wave: Results of a Swiss Survey. Int. J. Environ. Res. Public Health 2021, 18, 8976. https://doi.org/10.3390/ijerph18178976
Gilles I, Mabire C, Perriraz M, Peytremann-Bridevaux I. Workplace Well-Being and Intent to Stay by Health Care Workers Reassigned during the First COVID-19 Wave: Results of a Swiss Survey. International Journal of Environmental Research and Public Health. 2021; 18(17):8976. https://doi.org/10.3390/ijerph18178976
Chicago/Turabian StyleGilles, Ingrid, Cédric Mabire, Margaux Perriraz, and Isabelle Peytremann-Bridevaux. 2021. "Workplace Well-Being and Intent to Stay by Health Care Workers Reassigned during the First COVID-19 Wave: Results of a Swiss Survey" International Journal of Environmental Research and Public Health 18, no. 17: 8976. https://doi.org/10.3390/ijerph18178976
APA StyleGilles, I., Mabire, C., Perriraz, M., & Peytremann-Bridevaux, I. (2021). Workplace Well-Being and Intent to Stay by Health Care Workers Reassigned during the First COVID-19 Wave: Results of a Swiss Survey. International Journal of Environmental Research and Public Health, 18(17), 8976. https://doi.org/10.3390/ijerph18178976