
Psychometric Evaluation of the Nurses Professional Values Scale-3: Indonesian Version


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Procedures
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Demographic Variables, Work-Related Variables, and Nurses’ Professional Values
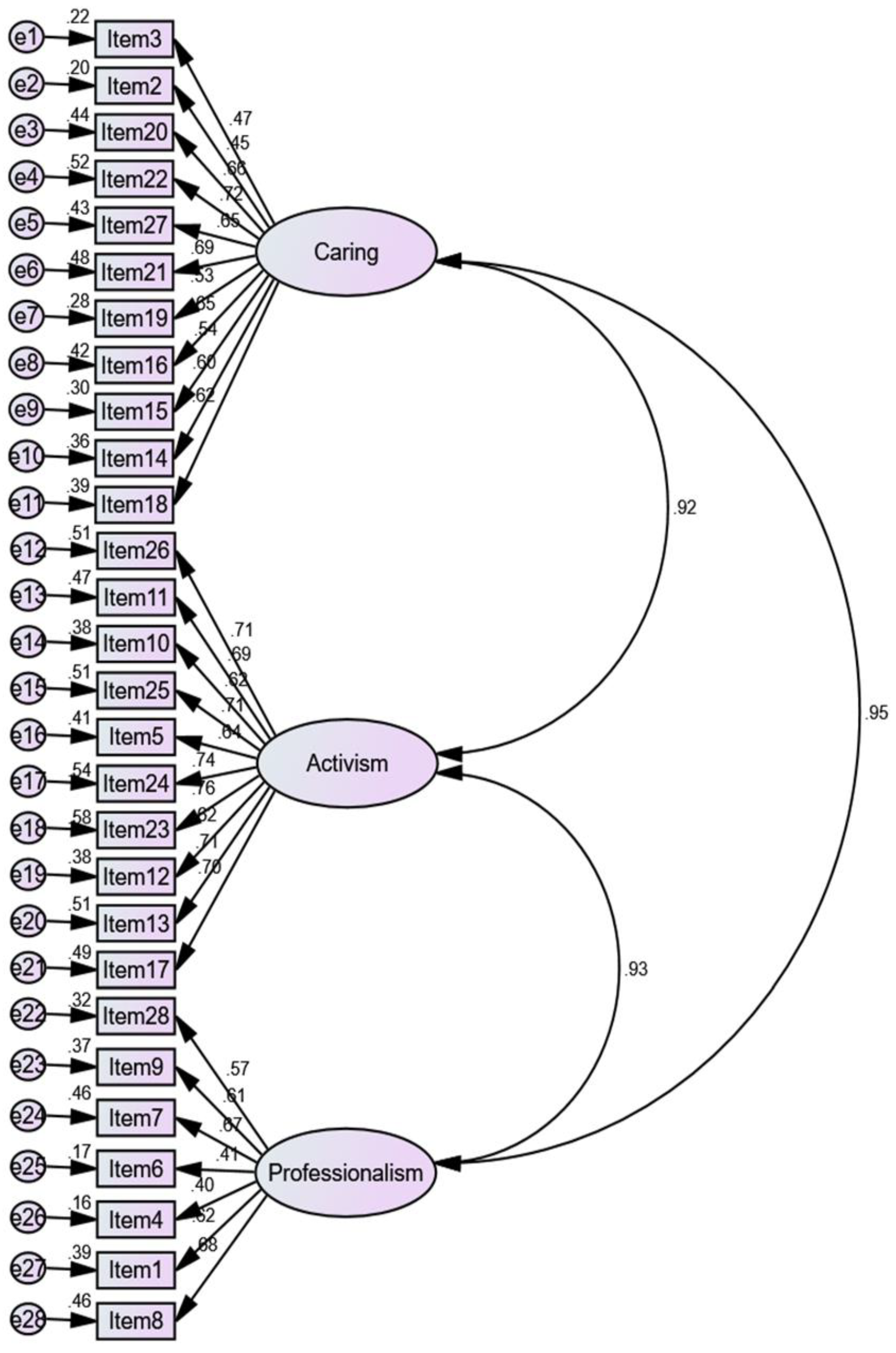
3.2. Validity Assessment
3.3. Reliability Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weis, D.; Schank, M.J. Development and psychometric evaluation of the Nurses Professional Values Scale--Revised. J. Nurs. Meas. 2009, 17, 221–231. [Google Scholar] [CrossRef]
- Weis, D.; Schank, M.J. An instrument to measure professional nursing values. J. Nurs. Scholarsh. 2000, 32, 201–204. [Google Scholar] [CrossRef]
- Haahr, A.; Norlyk, A.; Martinsen, B.; Dreyer, P. Nurses experiences of ethical dilemmas: A review. Nurs. Ethics 2020, 27, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Kaya, H.; Isik, B.; Senyuva, E.; Kaya, N. Personal and professional values held by baccalaureate nursing students. Nurs. Ethics 2016, 24, 716–731. [Google Scholar] [CrossRef] [PubMed]
- Weis, D.; Schank, M.J. Development and psychometric evaluation of the Nurses Professional Values Scale-3. J. Nurs. Meas. 2017, 25, 400–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, K.L.; Chong, M.C. Factors influencing professional values among Indonesian undergraduate nursing students. Nurse Educ. Pract. 2019, 41, 102648. [Google Scholar] [CrossRef]
- Lin, Y.H.; Wang, L.S. A Chinese version of the revised Nurses Professional Values Scale: Reliability and validity assessment. Nurse Educ. Today 2010, 30, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Basurto Hoyuelos, S.; Fraile, C.L.; Weis, D.; Urien Ede, L.; Elsden, C.A.; Schank, M.J. Nursing professional values: Validation of a scale in a Spanish context. Nurse Educ. Today 2010, 30, 107–112. [Google Scholar] [CrossRef]
- Nocerino, R.; Chiarini, M.; Marina, M. Nurse professional identity: Validation of the Italian version of the questionnaire Nurse Professional Values Scale-Revised. Clin. Ter. 2020, 171, e114–e119. [Google Scholar] [CrossRef]
- Schmidt, B.J.; McArthur, E.C. Professional nursing values: A concept analysis. Nurs. Forum 2018, 53, 69–75. [Google Scholar] [CrossRef]
- Poorchangizi, B.; Farokhzadian, J.; Abbaszadeh, A.; Mirzaee, M.; Borhani, F. The importance of professional values from clinical nurses’ perspective in hospitals of a medical university in Iran. BMC Med. Ethics 2017, 18, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poorchangizi, B.; Borhani, F.; Abbaszadeh, A.; Mirzaee, M.; Farokhzadian, J. Professional Values of Nurses and Nursing Students: A comparative study. BMC Med. Educ. 2019, 19, 438. [Google Scholar] [CrossRef] [PubMed]
- Posluszny, L.; Hawley, D.A. Comparing Professional Values of Sophomore and Senior Baccalaureate Nursing Students. J. Nurs. Educ. 2017, 56, 546–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alabdulaziz, H.; Cruz, J.P.; Alasmee, N.A.; Almazan, J.U. Psychometric analysis of the Nurses’ Professional Values Scale-3 Arabic version among student nurses. Int. Nurs. Rev. 2021. [Google Scholar] [CrossRef] [PubMed]
- Dellafiore, F.; Grugnetti, A.M.; Caruso, R.; Prinzivalli, G.; Luca, M.; Grugnetti, G.; Belloni, S.; Magon, A.; Arrigoni, C. “Nurses Professional Values Scale-Three”: A validation study among Italian nurses and nursing students. J. Nurs. Meas. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meyers, L.S.; Gamst, G.; Guarino, A.J. Applied Multivariate Research: Design and Interpretation; SAGE Publication: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Fornell, C.; Larckle, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage: Hampshire, UK, 2019. [Google Scholar]
- Collier, J.E. Applied Structural Equation Modeling Using AMOS; Routledge: New York, NY, USA, 2020. [Google Scholar]
- Kline, R.B. Principle and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA; London, UK, 2016. [Google Scholar]
- Gaskin, J.; James, M.; Lim, J. AMOS Plugin: Master Validity Tool. Available online: https://www.youtube.com/watch?v=JqySgMU_qMQ (accessed on 26 May 2021).
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; MacCallum, R.C.; Wegener, D.T.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Knekta, E.; Runyon, C.; Eddy, S. One size doesn’t fit all: Using factor analysis to gather validity evidence when using surveys in your research. CBE Life Sci. Educ. 2019, 18, rm1. [Google Scholar] [CrossRef] [PubMed]
- Worthington, R.L.; Whittaker, T.A. Scale development research: A content analysis and recommendations for best practices. Couns. Psychol. 2016, 34, 806–838. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage: Los Angeles, CA, USA; Washington, DC, USA, 2013. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson Education: New York, NY, USA, 2019. [Google Scholar]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Gaskin, J.; Lim, J. AMOS Plugin: Model Fit Measure. Available online: https://www.youtube.com/watch?v=wV6UudZSBCA (accessed on 26 May 2021).
- Strickland, O.L. Using factor analysis for validity assessment: Practical considerations. J. Nurs. Meas. 2003, 11, 203–205. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis; Lawrence Erlbaum Associate: Hillsdale, NJ, USA, 1992. [Google Scholar]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Garson, G.D. Validity and Reliability; Statistical Associates Publishing: Asheboro, NC, USA, 2013. [Google Scholar]
- ANA. Code of Ethics for Nurses with Interpretive Statements; American Nurses Association: Washington, DC, USA, 2015. [Google Scholar]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2014, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Fain, J.A. Reading, Understanding, and Applying Nursing Research, 5th ed.; F. A. Davis Company: Philadelphia, PA, USA, 2017. [Google Scholar]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research: Appraising Evidence for Nursing Practice, 9th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]

{kind=link}
| Variables | EFA | CFA | Total | Caring | Activism | Professionalism | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N1 (%) | N2 (%) | N (%) | M (SD) | rs/U/H | p | M (SD) | rs/U/H | p | M (SD) | rs/U/H | p | |
| Age (years), M (SD) | 33.12 (7.87) | 33.36 (7.22) | 33.24 (7.54) | 36.51 (4.95) | −0.218 | <0.001 | 35.84 (5.54) | −0.184 | <0.001 | 29.05 (4.08) | −0.168 | <0.001 |
| Gender | 36743.50 | 0.434 | 36684.00 | 0.415 | 37144.00 | 0.563 | ||||||
| Male | 90 (30.00) | 94 (31.30) | 184 (30.70) | 36.25 (5.44) | 35.54 (5.59) | 28.92 (4.04) | ||||||
| Female | 210 (70.00) | 206 (68.70) | 416 (63.30) | 36.62 (4.72) | 35.98 (5.53) | 29.11 (4.09) | ||||||
| Religion | 830.50 | 0.828 | 834.00 | 0.836 | 853.00 | 0.887 | ||||||
| Muslim | 299 (99.70) | 298 (99.30) | 597 (99.50) | 36.50 (4.95) | 35.83 (5.52) | 29.05 (4.06) | ||||||
| Christian | 1 (0.30) | 2 (0.70) | 3 (0.50) | 37.67 (6.66) | 38.00 (10.44) | 30.00 (7.94) | ||||||
| Marital status | 7.36 | 0.025 | 7.15 | 0.028 | 4.01 | 0.135 | ||||||
| Married | 234 (78.00) | 169 (56.30) | 403 (67.20) | 36.19 (4.95) | 35.55 (5.44) | 28.92 (3.98) | ||||||
| Not married | 65 (21.70) | 129 (43.00) | 194 (32.30) | 37.07 (4.88) | 36.34 (5.69) | 29.28 (4.26) | ||||||
| Divorce | 1 (0.30) | 2 (0.70) | 3 (0.50) | 42.67 (4.04) | 43.33 (3.51) | 33.00 (2.00) | ||||||
| Nurse education level | 9.71 | 0.008 | 16.72 | <0.001 | 15.40 | <0.001 | ||||||
| Diploma | 171 (57.00) | 170 (56.70) | 341 (56.80) | 35.85 (4.87) | 34.97 (5.25) | 28.52 (4.06) | ||||||
| Bachelor’s | 129 (43.00) | 128 (42.70) | 257 (42.80) | 37.34 (4.90) | 36.96 (5.68) | 29.73 (3.97) | ||||||
| Master’s | 0 (.00) | 2 (.70) | 2 (0.30) | 41.00 (9.90) | 42.00 (11.31) | 34.00 (7.07) | ||||||
| Nurse’s expertise | 18.72 | <0.001 | 24.79 | <0.001 | 17.27 | 0.001 | ||||||
| Advanced nurse | 90 (30.00) | 76 (25.30) | 166 (27.70) | 35.53 (5.12) | 35.11 (5.47) | 28.78 (4.05) | ||||||
| Supervisor nurse | 26 (8.70) | 22 (7.30) | 48 (8.00) | 35.60 (4.26) | 34.88 (4.95) | 28.56 (4.33) | ||||||
| Associate nurse | 155 (51.70) | 202 (67.30) | 357 (59.50) | 36.89 (4.93) | 35.92 (5.49) | 29.01 (3.96) | ||||||
| Senior nursing student | 29 (9.70) | 0 (0.00) | 29 (4.80) | 38.97 (3.96) | 40.66 (5.25) | 32.03 (4.25) | ||||||
| Type of job | 18403.50 | 0.447 | 17102.50 | 0.089 | 16683.00 | 0.046 | ||||||
| Full time | 258 (86.00) | 268 (89.30) | 526 (87.70) | 36.46 (4.82) | 35.69 (5.41) | 28.91 (3.94) | ||||||
| Part-time | 42 (14.00) | 32 (10.70) | 74 (12.30) | 36.86 (5.83) | 36.97 (6.33) | 30.11 (4.82) | ||||||
| Working experience (years) | 21.22 | <0.001 | 10.56 | 0.005 | 11.72 | 0.003 | ||||||
| <5 | 54 (18.00) | 85 (28.30) | 139 (23.20) | 38.12 (5.65) | 36.75 (6.10) | 29.74 (4.45) | ||||||
| 5–14 | 189 (63.00) | 154 (51.30) | 343 (57.20) | 36.28 (4.70) | 35.95 (5.52) | 29.09 (4.04) | ||||||
| ≥15 | 57 (19.00) | 61 (20.30) | 118 (19.70) | 35.29 (4.29) | 34.47 94.62) | 28.14 (3.53) | ||||||
| Items | Factor | Communality | ||
|---|---|---|---|---|
| Caring | Activism | Professionalism | ||
| Item 3 | 0.84 | 0.82 | ||
| Item 2 | 0.82 | 0.81 | ||
| Item 20 | 0.69 | 0.73 | ||
| Item 22 | 0.69 | 0.74 | ||
| Item 27 | 0.66 | 0.73 | ||
| Item 21 | 0.68 | 0.65 | ||
| Item 19 | 0.66 | 0.76 | ||
| Item 16 | 0.63 | 0.58 | ||
| Item 15 | 0.55 | 0.61 | ||
| Item 14 | 0.54 | 0.67 | ||
| Item 18 | 0.49 | 0.54 | ||
| Item 26 | 0.76 | 0.72 | ||
| Item 11 | 0.72 | 0.72 | ||
| Item 10 | 0.70 | 0.69 | ||
| Item 25 | 0.68 | 0.72 | ||
| Item 5 | 0.67 | 0.74 | ||
| Item 24 | 0.63 | 0.79 | ||
| Item 23 | 0.63 | 0.66 | ||
| Item 12 | 0.58 | 0.67 | ||
| Item 13 | 0.59 | 0.72 | ||
| Item 17 | 0.56 | 0.65 | ||
| Item 28 | 0.75 | 0.69 | ||
| Item 9 | 0.74 | 0.68 | ||
| Item 7 | 0.68 | 0.75 | ||
| Item 6 | 0.60 | 0.67 | ||
| Item 4 | 0.59 | 0.59 | ||
| Item 1 | 0.58 | 0.63 | ||
| Item 8 | 0.53 | 0.59 | ||
| Eigenvalue | 16.21 | 1.24 | 0.86 | |
| Percentage of variance | 57.91% | 4.42% | 3.07% | |
| Total variance explained of the factor model | 65.40% | |||
| Kaiser–Meyer–Olkin measure of sampling adequacy | 0.96 | |||
| Bartlett’s test of sphericity | X2 | 7867.74 | ||
| df | 378 | |||
| p | <0.001 | |||
| Items | Mean | SD | CITC | SMCs | AID |
|---|---|---|---|---|---|
| Factor 1: Caring (Cronbach’s α = 0.94) | |||||
| Item 3. Protect health and safety of the patient/public | 4.04 | 0.70 | 0.67 | 0.67 | 0.93 |
| Item 2. Respect the inherent dignity, values, and human rights of individuals | 4.02 | 0.71 | 0.68 | 0.68 | 0.93 |
| Item 20. Confront practitioners with questionable or inappropriate practice | 3.70 | 0.73 | 0.77 | 0.73 | 0.93 |
| Item 22. Practice guided by principles of fidelity and respect for person | 3.82 | 0.74 | 0.81 | 0.72 | 0.92 |
| Item 27. Engage in consultation/collaboration to provide optimal care | 3.74 | 0.76 | 0.76 | 0.65 | 0.93 |
| Item 21. Protect rights of participants in research | 3.81 | 0.74 | 0.76 | 0.66 | 0.93 |
| Item 19. Safeguard patient’s right to confidentiality and privacy | 4.12 | 0.76 | 0.75 | 0.67 | 0.93 |
| Item 16. Act as a patient advocate | 3.53 | 0.71 | 0.64 | 0.55 | 0.93 |
| Item 14. Accept responsibility and accountability for own practice | 3.66 | 0.72 | 0.71 | 0.60 | 0.93 |
| Item 15. Protect moral and legal rights of patients | 4.01 | 0.76 | 0.79 | 0.73 | 0.93 |
| Item 18. Provide care without bias or prejudice to patients and populations | 3.69 | 0.73 | 0.71 | 0.52 | 0.93 |
| Factor 2: Activism (Cronbach’s α = 0.95) | |||||
| Item 26. Take action to influence legislators and other policy makers to improve health care | 3.56 | 0.78 | 0.75 | 0.62 | 0.94 |
| Item 11. Recognize the role of professional nursing associations in shaping health policy | 3.78 | 0.75 | 0.78 | 0.69 | 0.94 |
| Item 10. Advance the profession through active involvement in health-related activities | 3.80 | 0.69 | 0.74 | 0.63 | 0.94 |
| Item 5. Participate in peer review | 3.63 | 0.72 | 0.72 | 0.53 | 0.94 |
| Item 25. Promote mutual peer support and collegial interactions to ensure quality care and professional satisfaction | 3.60 | 0.70 | 0.81 | 0.69 | 0.94 |
| Item 24. Participate in professional efforts to advance global health | 3.76 | 0.75 | 0.86 | 0.78 | 0.94 |
| Item 23. Actively promote health of populations | 3.69 | 0.73 | 0.78 | 0.67 | 0.94 |
| Item 12. Establish collaborative partnerships to reduce health care disparities | 3.74 | 0.72 | 0.77 | 0.64 | 0.94 |
| Item 13. Assume responsibility for meeting health needs of diverse populations | 3.70 | 0.73 | 0.80 | 0.65 | 0.94 |
| Item 17. Participate in nursing research and/or implement research findings appropriate to practice | 3.59 | 0.71 | 0.75 | 0.60 | 0.94 |
| Factor 3: Professionalism (Cronbach’s α = 0.89) | |||||
| Item 28. Recognize professional boundaries | 3.77 | 0.75 | 0.63 | 0.46 | 0.88 |
| Item 9. Seek additional education to update knowledge and skills to maintain | 3.81 | 0.73 | 0.66 | 0.48 | 0.87 |
| Item 6. Establish standards as a guide for practice | 3.89 | 0.75 | 0.70 | 0.54 | 0.87 |
| Item 7. Promote and maintain standards where planned learning activities for students take place | 3.73 | 0.80 | 0.78 | 0.64 | 0.86 |
| Item 1. Engage in ongoing self-evaluation | 3.59 | 0.72 | 0.68 | 0.47 | 0.87 |
| Item 4. Assume responsibility for personal well-being | 3.71 | 0.79 | 0.56 | 0.38 | 0.88 |
| Item 8. Initiate actions to improve environments of practice | 3.64 | 0.81 | 0.74 | 0.59 | 0.86 |
| Overall Cronbach’s α = 0.97 | |||||
| Factor | Original Model | Model after EFA | ||
|---|---|---|---|---|
| Items | Reliability | Items | Reliability | |
| Caring | 15, 18, 19, 2, 3, 22, 16, 14, 21, 20 | 0.885 | 3, 2, 20, 22, 27, 21, 19, 16, 15, 14, 18 | 0.937 |
| Activism | 24, 23, 26, 12, 13, 11, 10, 17, 25, 27 | 0.912 | 26, 11, 10, 25, 5, 24, 23, 12, 13, 17 | 0.946 |
| Professionalism | 6, 7, 5, 8, 1, 9, 4, 28 | 0.799 | 28, 9, 7, 6, 4, 1, 8 | 0.886 |
| Overall | 0.944 | 0.974 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asiandi, A.; Erlina, M.; Lin, Y.-H.; Huang, M.-C. Psychometric Evaluation of the Nurses Professional Values Scale-3: Indonesian Version. Int. J. Environ. Res. Public Health 2021, 18, 8810. https://doi.org/10.3390/ijerph18168810
Asiandi A, Erlina M, Lin Y-H, Huang M-C. Psychometric Evaluation of the Nurses Professional Values Scale-3: Indonesian Version. International Journal of Environmental Research and Public Health. 2021; 18(16):8810. https://doi.org/10.3390/ijerph18168810
Chicago/Turabian StyleAsiandi, Asiandi, Meli Erlina, Yu-Hua Lin, and Mei-Chih Huang. 2021. "Psychometric Evaluation of the Nurses Professional Values Scale-3: Indonesian Version" International Journal of Environmental Research and Public Health 18, no. 16: 8810. https://doi.org/10.3390/ijerph18168810
APA StyleAsiandi, A., Erlina, M., Lin, Y.-H., & Huang, M.-C. (2021). Psychometric Evaluation of the Nurses Professional Values Scale-3: Indonesian Version. International Journal of Environmental Research and Public Health, 18(16), 8810. https://doi.org/10.3390/ijerph18168810