1. Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for the coronavirus disease 2019 (COVID-19), has spread worldwide since the first reported case in Wuhan in late December 2019, becoming the primary threat to public health in all countries. Since the World Health Organization (WHO), on 11 March 2020, declared the COVID-19 pandemic, many countries, including Italy, launched public health security plans based on the promotion of social distancing, wearing anti-infection masks, and lockdown restrictions. These extreme measures induced lifestyle changes; in particular, quarantine caused a reduction in physical activity (PA) levels per week in all different age groups, leading to decreased levels of psychological well-being in Italy [
1]. Physical inactivity also plays a crucial role in non-communicable chronic disease, which is considered responsible for over three million premature deaths worldwide every year [
2]. The relationship between quarantine-imposed reduced PA levels and musculoskeletal pain (MP) is a topic of growing interest today. Sagát et al. [
3] showed how this extreme lifestyle change led to an increase in low back and neck pain prevalence in Riyadh’s population aged 18 to 64. Toprak et al. [
4] compared people who stayed home and continued to work during the three-month lockdown of the pandemic in Turkey, and found that those who stayed home had increased MP symptoms that were likely due to lower PA levels.
One of the social categories most affected by restricted mobility and reduced PA levels is students. Students typically spend many hours seated on non-ergonomic chairs and assuming incorrect postures to carry out their curricular activities, leading to a general musculoskeletal overload [
5]. Furthermore, while spending much time using laptops and smartphones to study and support leisure activities, they adopt incorrect postures, leading to musculoskeletal alteration and pain, especially to the neck and the spine [
6]. Haroon et al. [
7] reported a high incidence of MP in Karachi’s university medical students, identifying the usage of laptops for more than three hours per day as a risk factor for neck pain. Different studies [
8,
9,
10] conducted among university students highlighted a high percentage of them stating MP, especially at the neck and low back. Furthermore, inactive students commonly reported mild/moderate pain, while physically active students referred to severe pain with a higher frequency over the month than inactive ones.
This study aimed to survey the PA levels and their correlation to MP among university students from Italy, before and during the pandemic restriction, therefore analyzing the impact of COVID-19 restrictions on pain and fatigue affecting daily life activities.
4. Discussion
Imposed quarantine due to the COVID-19 pandemic imposed a severe reduction in daily activities and inevitably increased the onset of MP. In the available literature concerning the COVID-19 aspects, the relationship between PA reduction and MP has not yet been investigated. To the best of our knowledge, this is the first study discussing the relationship between the reduction of PA levels, SB increase, and MP onset in university students after one year of COVID-19 restrictions in Italy.
The disease outbreak has changed young people’s lives who were used to spending most of the day away from home between study, work, commitments, friends, sports, and entertainment.
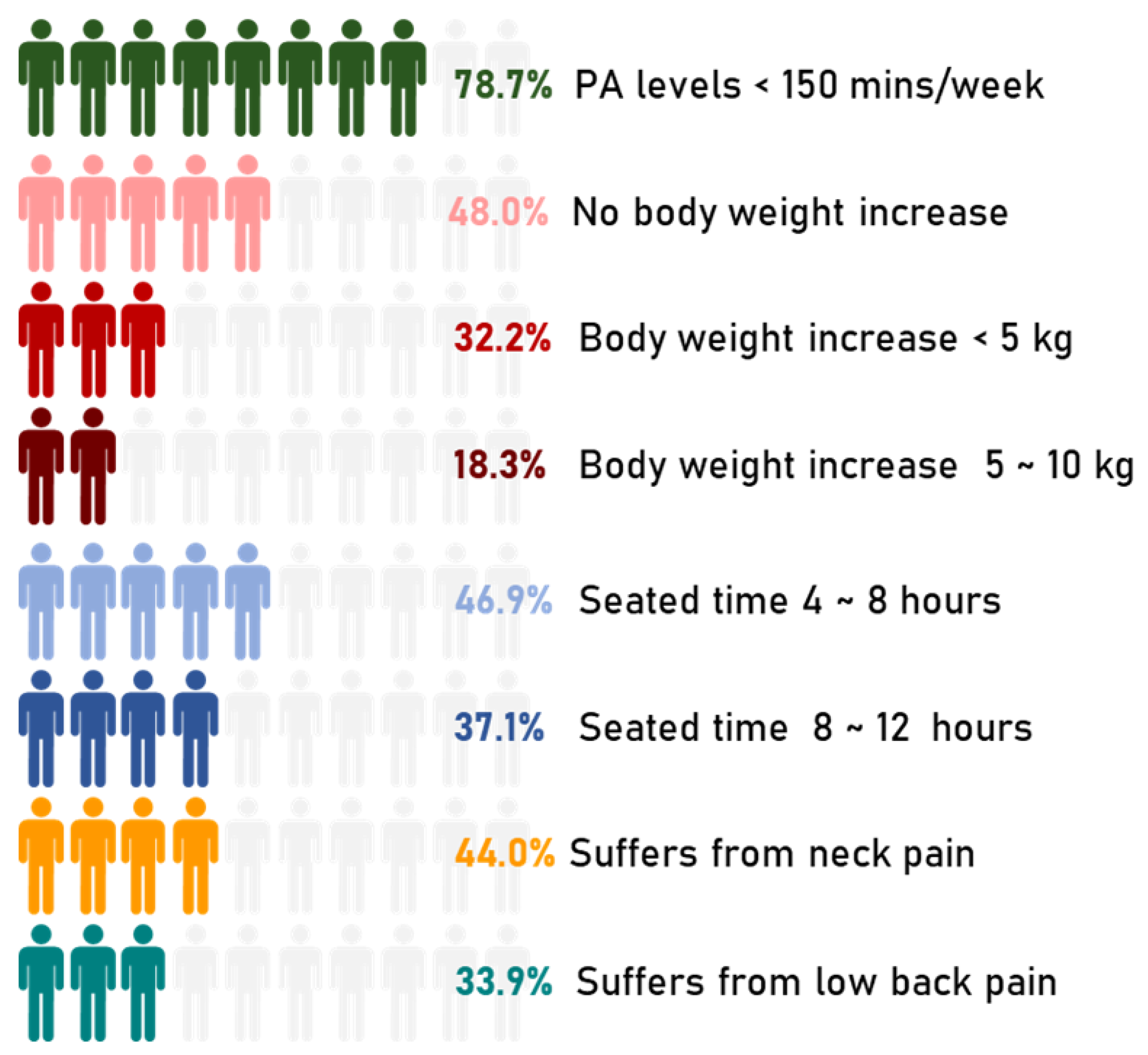
Figure 5 shows the primary outcomes of this study.
During the first pandemic period, March-May 2020, sport-related public facilities were closed, making it challenging to practice jogging, running, or walking long distances. Maugeri et al. [
17] conducted an epidemiological analysis during the first quarantine period on 2524 Italian subjects aged 18 and 70. PA levels suffered a moderate decrease, those who practiced moderate activity decreased by about 6%, while those who practiced intense activity by 11%. Some sports activities resumed from June but starting from October, with the increase in the number of infections, sports centers closed once more, and the red zones blocked the students at home again. This event did not permit the expected recovery of sports activities, so according to our data, about 30% of the participants did not return to the PA levels they had before the pandemic after one year of experiencing a pandemic.
Figure 6 shows how PA levels have changed between before and during the pandemic in one year. About 60% of those inactive before the pandemic did not change this behavior during the pandemic, while 35% practicing light activity before the pandemic became inactive during the pandemic. Interestingly, the highest percentage of people for each group, except for the inactive ones, is channeled into the light activity group. The increase of subjects performing light levels PA is due to the presence of those who started practicing PA (14.1%), probably to overcome the severe limitations of daily activities, and those who reduced their PA levels from moderate and high to light (27.1% and 23.1%, respectively). Among those who did not practice PA before the pandemic (19.9%), 40.2% started practicing PA during the pandemic. These findings contrast with Hall et al. [
18], are speculating that those already sedentary before the pandemic would hardly increase their PA levels during the pandemic. Several studies analyzed reduced PA and SB worldwide [
19,
20,
21,
22]. Many authors decreed a possible end of these conditions in the summer of 2020, although unfortunately, starting from October 2020, the severe limitations were back in effect in Italy. WHO guidelines of PA and SB [
23] recommend doing at least 150 min of moderate-intensity PA throughout the week and limiting sedentary time. In line with these guidelines, the students who reported MP were divided into two groups based on PA adherence. The data show a high prevalence of students reporting pain in the PA < 150 min/week group, representing 41.7% versus 8.8% of those performing PA ≥ 150 min/week.
The 72.2% of those with neck pain experienced it during the pandemic and mainly due to several hours of study, as expected since they had to attend courses through electronic devices due to the restriction measures. As reported by Mowatt et al. [
24], the most frequent health problems among those using electronic devices for several hours are computer vision syndrome, neck, shoulder, and back pain, and specifically, 89.9% of undergraduate university students have a prevalence of these health problems [
25]. Prolonged use of mobile phones, tablets, or laptops to attend online lessons or to spend time on social media may negatively affect neck and shoulders pain [
26]. This relationship, anyhow, has been validated by several epidemiological studies, which confirmed that assuming a wrong posture for many hours and having SB is strongly related to the severity of neck pain [
27,
28,
29,
30,
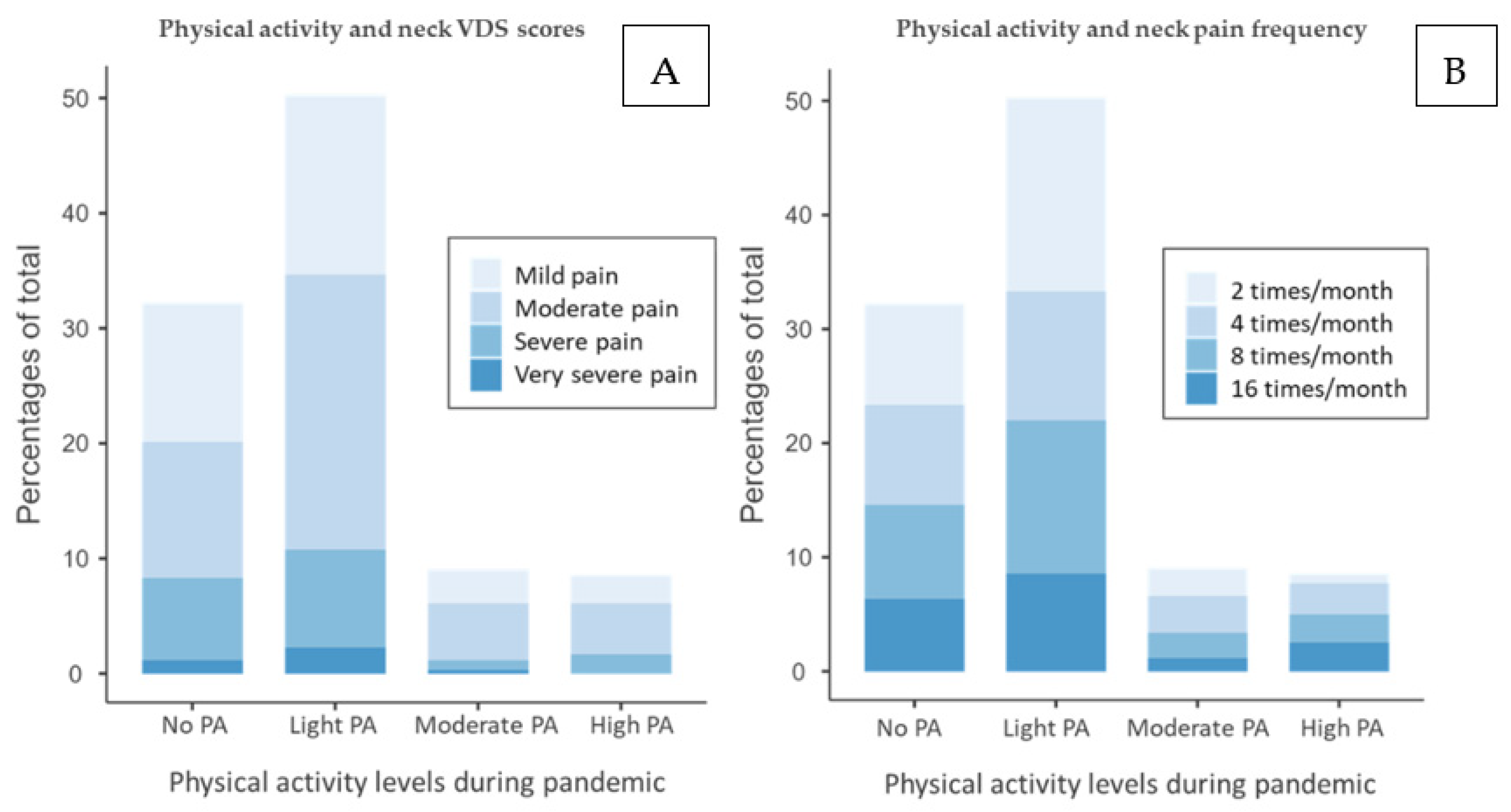
31]. Our data show how the levels of VDS score, and frequency of neck pain onset are considerably lower for students performing moderate to high PA levels compared to those with light or no PA levels. These findings confirm the hypothesis of a greater likelihood of having neck pain for those with low levels of PA as highlighted by Scarabottolo et al. [
32] and Guddal et al. [
33]. Conversely, we strongly disagree with Sitthipornvorakul et al. [
34], who assert strong evidence of no association between PA and neck pain.
The 72.9% of the students with low back pain experienced it during the pandemic, mainly due to several hours of study, probably related to a wrong posture assumed during it, as for the neck pain. Stressors, fear of pain, and lack of PA, according to Amelot et al. [
35], are the most critical factors affecting LBP occurrence. Only PA levels have been evaluated in the present study, but psychosocial repercussions over mental health were present in line with another analysis conducted among the Italian population [
36]. As for neck pain, VDS score and frequency for low back pain was considerably lower for students with moderate to high PA levels, compared to those with light or no PA. These results are in line with Wedderkopp et al. [
36], where physically active students had a low predisposition to experiencing back pain. Likewise, Guddal et al. [
33] observed that moderate levels of PA were correlated to reduced LBP onset. However, as we highlighted in the results section, excessively high PA levels might increase the risk of spinal pain because intense activities might contribute to a wrong posture and lead to pain onset [
37].
Two studies [
38,
39] pointed the absence of correlation between a sedentary lifestyle and the occurrence of MP in medical students with LBP. Our data contrast these authors’ points of view because the OR between SB and low back pain was 1.79 (95% CI, 1.29–2.49),
Table A2. However, these authors did not clearly state what describes SB. While Moroder [
38] did not classify sitting time and PA levels threshold as sedentary, Chen S.M. [
39] considered only time spent sitting, omitting the PA levels. Even if this topic is still debated among the scientific community, our findings strongly agree with a recent meta-analysis published in Nature journal by Alzahrani et al. [
40], who highlighted the importance of medium to moderate PA levels to decrease the risk of LBP. Furthermore, epidemiological research has shown that assuming a wrong posture for a prolonged time, sitting for many hours, or simply taking part in SB are strong predictors of adverse health outcomes such as cardiovascular diseases [
41], diabetes [
42], cancer [
43], musculoskeletal pain [
44], or depression [
45]. In line with our investigations about SB and MP presence, Shrier and Feldman [
46,
47] identified the prolonged sitting position as a prevalent risk factor for MP onset. In general, it can be assumed that the more frequent students are physically inactive during the week, the more frequent is the risk of suffering from chronic pain [
48].
Concerning the pain relief strategies, Mimi Mun Yee Tse et al. [
49] conducted a similar study of university students in Hong Kong and stated a high percentage of them adopting pharmacological methods to contrast MP. This condition differs from our data, as our sample’s highest pain relief strategy was performing physical exercises or waiting until the pain resolves. Those experiencing pain should prefer non-pharmacological treatment initially, favoring exercises or rehabilitation protocols [
50] instead. Therefore, education for the young is needed to give them resources to manage their condition, such as exercises sheets, pain management guidelines, or prevention methods [
50,
51].
Further studies are needed to understand the aspects related to a sedentary lifestyle and pain. What is clear is that we must work on two fronts since, following this trend, the 2025 global PA target (10% reduction of physical inactivity) will not be met [
52]. Firstly, National governments should develop new approaches to engage the unwilling population to increase or start PA programs, especially after one year of restrictions. Secondly, there is a need to understand the reasons behind some students’ indifference towards PA, since, during the pandemic, they could have trained at home to counterbalance psychological and physiological distress [
53,
54]. The last decade’s general increase of physical inactivity prompted the WHO in 2018 to provide a plan until 2030 to encourage the world population to be more active [
55]. The aim is to invest in policies to promote sports activities, jogging, or just recreational activities to achieve different sustainable development goals by 2030. Trivial as it may seem, yet simply carrying out a student’s daily activities such as leaving home in the morning, going to university, walking with friends, or visiting a shop can be worth it to maintain an active body, and thus avoid the onset of pain [
56]. In line with WHO guidelines, we suggest the need to plan educational programs that encourage students to practice exercise. For instance, with the help of professionals, e.g., kinesiologists, universities could plan a 10-min break within lessons to perform simple exercises to keep the body active and avoid the classic pains from incorrect posture.
This study has some limitations that need to be considered in the results’ interpretation. First, the questionnaire was administered through online channels, which may determine a disinterest in answering all questions carefully. Second, it was a self-reported questionnaire, indicating an underestimation or overestimation of the self-conditions based on the questions. Third, a bias regarding PA levels before the pandemic may be present due to the time elapsed. Fourth, this study has a cross-sectional design, so inference must be evaluated carefully. Conversely, many responses, the presence of different check-questions useful to reduce the bias, the strong consistency due to a close age range, and the reduced likelihood of having other conditions that could lead to MP enhance the study’s strength.
In terms of future research, we expect to conduct further research like this after recovering entirely from the COVID-19 pandemic to determine if PA and SB levels retrieved after this social catastrophe and investigate how MPs can be modulated through daily exercises.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





