
“I’m So Tired”: Fatigue as a Persistent Physical Symptom among Working People Experiencing Exhaustion Disorder

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Psychological Distress
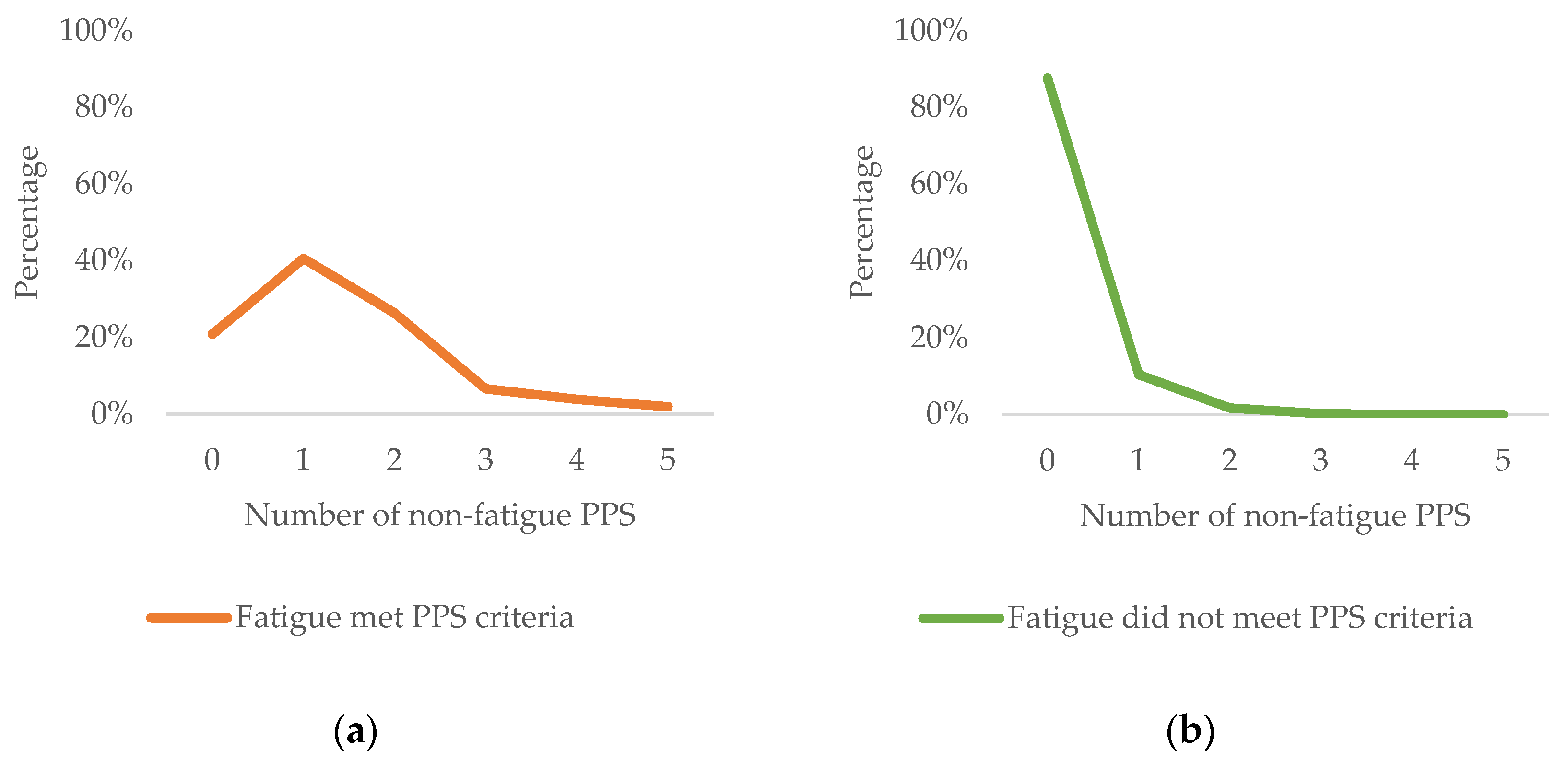
3.3. Number of Non-Fatigue PPSs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boter, H.; Mänty, M.; Hansen, A.M.; Hortobágyi, T.; Avlund, K. Self-Reported Fatigue and Physical Function in Late Mid-Life. J. Rehabil. Med. 2014, 46, 684–690. [Google Scholar] [CrossRef]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the General Population- Associations to Age, Sex, Socioeconomic Status, Physical Activity, Sitting Time and Self-Rated Health: The Northern Sweden MONICA Study 2014. BMC Public Health 2017, 17, 654–663. [Google Scholar] [CrossRef]
- Hagelin, C.L.; Wengström, Y.; Runesdotter, S.; Fürst, C.J. The Psychometric Properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in Four Different Populations. Acta Oncol. 2007, 46, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Cullen, W.; Kearney, Y.; Bury, G. Prevalence of Fatigue in General Practice. Ir. J. Med. Sci. 2002, 171, 10–12. [Google Scholar] [CrossRef]
- Gallagher, A.M.; Thomas, J.M.; Hamilton, W.T.; White, P.D. Incidence of Fatigue Symptoms and Diagnoses Presenting in UK Primary Care from 1990 to 2001. J. R. Soc. Med. 2004, 97, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Flóvenz, S.Ó.; Broddadóttir, E.; Brynjólfsson, S.; Agnarsdóttir, A.S.; Salkovskis, P.M.; Sigurðsson, J.F. Prevalence of Persistent Physical Symptoms and Association with Depression, Anxiety and Health Anxiety in Iceland. Icel. Med. J. 2021, 107, 67–73. [Google Scholar] [CrossRef]
- Rose, D.M.; Seidler, A.; Nübling, M.; Latza, U.; Brähler, E.; Klein, E.M.; Wiltink, J.; Michal, M.; Nickels, S.; Wild, P.S.; et al. Associations of Fatigue to Work-Related Stress, Mental and Physical Health in an Employed Community Sample. BMC Psychiatry 2017, 17, 167. [Google Scholar] [CrossRef] [PubMed]
- Kant, I.; Bultmann, U.; Schroer, K.; Beurskens, A.; van Amelsvoort, L.G.P.M.; Swaen, G. An Epidemiological Approach to Study Fatigue in the Working Population: The Maastricht Cohort Study. Occup. Environ. Med. 2003, 60, i32–i39. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Seong, S.; Park, S.; Lim, J.; Hong, S.; Cho, Y.; Kim, H. Korean Version of the Swedish Occupational Fatigue Inventory among Construction Workers: Cultural Adaptation and Psychometric Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 4302. [Google Scholar] [CrossRef] [PubMed]
- Eurofound. Burnout in the Workplace: A Review of Data and Policy Responses in the EU; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- Basu, N.; Yang, X.; Luben, R.N.; Whibley, D.; Macfarlane, G.J.; Wareham, N.J.; Khaw, K.-T.; Myint, P.K. Fatigue Is Associated with Excess Mortality in the General Population: Results from the EPIC-Norfolk Study. BMC Med. 2016, 14, 122. [Google Scholar] [CrossRef] [PubMed]
- European Agency for Safety and Health at Work. Calculating the Costs of Work-Related Stress and Psychosocial Risks: Literature Review; Publications Office: Luxembourg, 2014. [Google Scholar]
- Hassard, J.; Teoh, K.R.H.; Visockaite, G.; Dewe, P.; Cox, T. The Cost of Work-Related Stress to Society: A Systematic Review. J. Occup. Health Psychol. 2018, 23, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Nijrolder, I.; van der Windt, D.; de Vries, H.; van der Horst, H. Diagnoses during Follow-up of Patients Presenting with Fatigue in Primary Care. Can. Med. Assoc. J. CMAJ 2009, 181, 683–687. [Google Scholar] [CrossRef] [PubMed]
- National Board of Health and Welfare. Exhaustion Disorder (Utmattningssyndrom—Stressrelaterad Psykisk Ohälsa); Socialstyrelsen: Stockholm, Sweden, 2003. [Google Scholar]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Persson, R.; Österberg, K.; Viborg, N.; Jönsson, P.; Tenenbaum, A. Two Swedish Screening Instruments for Exhaustion Disorder: Cross-Sectional Associations with Burnout, Work Stress, Private Life Stress, and Personality Traits. Scand. J. Public Health 2017, 45, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Lindblom, K.M.; Linton, S.J.; Fedeli, C.; Bryngelsson, I.-L. Burnout in the Working Population: Relations to Psychosocial Work Factors. Int. J. Behav. Med. 2006, 13, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Lindert, J.; Müller-Nordhorn, J.; Soares, J.F. Age and Distress of Women–Results of a Representative Population-Based Study. Arch. Womens Ment. Health 2009, 12, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Norlund, S.; Reuterwall, C.; Höög, J.; Janlert, U.; Slunga Järvholm, L. Work Situation and Self-Perceived Economic Situation as Predictors of Change in Burnout—A Prospective General Population-Based Cohort Study. BMC Public Health 2015, 15, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Lexén, A.; Kåhlin, I.; Erlandsson, L.-K.; Håkansson, C. Occupational Health among Swedish Occupational Therapists: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 3379. [Google Scholar] [CrossRef]
- Asplund, S.; Åhlin, J.; Åström, S.; Hedlund, M.; Lindgren, B.-M.; Ericson-Lidman, E. Self-Rated Exhaustion Disorder and Associated Health-Related Factors among Municipal Employees in Rural Areas of Northern Sweden. Int. Arch. Occup. Environ. Health 2021, 94, 659–668. [Google Scholar] [CrossRef]
- Persson, R.; Österberg, K. Repeated Assessment of Work-Related Exhaustion: The Temporal Stability of Ratings in the Lund University Checklist for Incipient Exhaustion. BMC Res. Notes 2020, 13, 304. [Google Scholar] [CrossRef]
- Glise, K.; Hadzibajramovic, E.; Jonsdottir, I.H.; Ahlborg, G., Jr. Self-Reported Exhaustion: A Possible Indicator of Reduced Work Ability and Increased Risk of Sickness Absence among Human Service Workers. Int. Arch. Occup. Environ. Health 2010, 83, 511–520. [Google Scholar] [CrossRef]
- Ahola, K.; Toppinen-Tanner, S.; Seppänen, J. Interventions to Alleviate Burnout Symptoms and to Support Return to Work among Employees with Burnout: Systematic Review and Meta-Analysis. Burn. Res. 2017, 4, 1–11. [Google Scholar] [CrossRef]
- Wallensten, J.; Åsberg, M.; Wiklander, M.; Nager, A. Role of Rehabilitation in Chronic Stress-Induced Exhaustion Disorder: A Narrative Review. J. Rehabil. Med. 2019, 51, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Richardson, K.M.; Rothstein, H.R. Effects of Occupational Stress Management Intervention Programs: A Meta-Analysis. Database Abstr. Rev. Eff. DARE Qual. Assess. Rev. Internet 2008, 13, 69–93. [Google Scholar] [CrossRef] [PubMed]
- Salomonsson, S.; Santoft, F.; Lindsäter, E.; Ejeby, K.; Ingvar, M.; Ljótsson, B.; Öst, L.-G.; Lekander, M.; Hedman-Lagerlöf, E. Effects of Cognitive Behavioural Therapy and Return-to-Work Intervention for Patients on Sick Leave Due to Stress-Related Disorders: Results from a Randomized Trial. Scand. J. Psychol. 2020, 61, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Lindsäter, E.; Axelsson, E.; Salomonsson, S.; Santoft, F.; Ejeby, K.; Ljótsson, B.; Åkerstedt, T.; Lekander, M.; Hedman-Lagerlöf, E. Internet-Based Cognitive Behavioral Therapy for Chronic Stress: A Randomized Controlled Trial. Psychother. Psychosom. 2018, 87, 296–305. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Boraxbekk, C.-J.; Stenlund, T.; Järvholm, L.S.; Neely, A.S. Effects of a Process-Based Cognitive Training Intervention for Patients with Stress-Related Exhaustion. Stress 2015, 18, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Glise, K.; Ahlborg, G.; Jonsdottir, I.H. Course of Mental Symptoms in Patients with Stress-Related Exhaustion: Does Sex or Age Make a Difference? BMC Psychiatry 2012, 12, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Glise, K.; Jonsdottir, I.H.; Ahlborg, G. Prevalence and Course of Somatic Symptoms in Patients with Stress-Related Exhaustion: Does Sex or Age Matter. BMC Psychiatry 2014, 14, 118. [Google Scholar] [CrossRef] [PubMed]
- Grossi, G.; Santell, B. Quasi-Experimental Evaluation of a Stress Management Programme for Female County and Municipal Employees on Long-Term Sick Leave Due to Work-Related Psychological Complaints. J. Rehabil. Med. 2009, 41, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Leone, S.S.; Huibers, M.J.; Knottnerus, J.A.; Kant, Ij. A Comparison of the Course of Burnout and Prolonged Fatigue: A 4-Year Prospective Cohort Study. J. Psychosom. Res. 2008, 65, 31–38. [Google Scholar] [CrossRef]
- Salomonsson, S.; Santoft, F.; Lindsäter, E.; Ejeby, K.; Ljótsson, B.; Öst, L.-G.; Ingvar, M.; Lekander, M.; Hedman-Lagerlöf, E. Cognitive–Behavioural Therapy and Return-to-Work Intervention for Patients on Sick Leave Due to Common Mental Disorders: A Randomised Controlled Trial. Occup. Environ. Med. 2017, 74, 905–912. [Google Scholar] [CrossRef]
- Willert, M.V.; Thulstrup, A.M.; Bonde, J.P. Effects of a Stress Management Intervention on Absenteeism and Return to Work—Results from a Randomized Wait-List Controlled Trial. Scand. J. Work Environ. Health 2011, 37, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Glise, K.; Wiegner, L.; Jonsdottir, I.H. Long-Term Follow-up of Residual Symptoms in Patients Treated for Stress-Related Exhaustion. BMC Psychol. 2020, 8, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Lander, F.; Friche, C.; Tornemand, H.; Andersen, J.H.; Kirkeskov, L. Can We Enhance the Ability to Return to Work among Workers with Stress-Related Disorders? BMC Public Health 2009, 9, 372–376. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics, 11th ed.; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Marks, E.M.; Hunter, M.S. Medically Unexplained Symptoms: An Acceptable Term? Br. J. Pain 2015, 9, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Picariello, F.; Ali, S.; Moss-Morris, R.; Chalder, T. The Most Popular Terms for Medically Unexplained Symptoms: The Views of CFS Patients. J. Psychosom. Res. 2015, 78, 420–426. [Google Scholar] [CrossRef]
- Chalder, T.; Willis, C. “Lumping” and “Splitting” Medically Unexplained Symptoms: Is There a Role for a Transdiagnostic Approach? J. Ment. Health 2017, 26, 187–191. [Google Scholar] [CrossRef]
- Dimsdale, J.; Sharma, N.; Sharpe, M. What Do Physicians Think of Somatoform Disorders? Psychosomatics 2011, 52, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Wessely, S.; Nimnuan, C.; Sharpe, M. Functional Somatic Syndromes: One or Many? Lancet 1999, 354, 936–939. [Google Scholar] [CrossRef]
- Petersen, M.W.; Schröder, A.; Jørgensen, T.; Ørnbøl, E.; Dantoft, T.M.; Eliasen, M.; Thuesen, B.H.; Fink, P. The Unifying Diagnostic Construct of Bodily Distress Syndrome (BDS) Was Confirmed in the General Population Elsevier Enhanced Reader. J. Psychosom. Res. 2020, 128, 109868. [Google Scholar] [CrossRef]
- Petersen, M.W.; Schröder, A.; Jørgensen, T.; Ørnbøl, E.; Meinertz Dantoft, T.; Eliasen, M.; Benros, M.E.; Fink, P. Irritable Bowel, Chronic Widespread Pain, Chronic Fatigue and Related Syndromes Are Prevalent and Highly Overlapping in the General Population: DanFunD. Sci. Rep. 2020, 10, 3273. [Google Scholar] [CrossRef] [PubMed]
- Nimnuan, C.; Hotopf, M.; Wessely, S. Medically Unexplained Symptoms: An Epidemiological Study in Seven Specialities. J. Psychosom. Res. 2001, 51, 361–367. [Google Scholar] [CrossRef]
- Reid, S.; Wessely, S.; Crayford, T.; Hotopf, M. Medically Unexplained Symptoms in Frequent Attenders of Secondary Health Care: Retrospective Cohort Study. Br. Med. J. 2001, 322, 767. [Google Scholar] [CrossRef]
- Roca, M.; Gili, M.; Garcia-Garcia, M.; Salva, J.; Vives, M.; Garcia Campayo, J.; Comas, A. Prevalence and Comorbidity of Common Mental Disorders in Primary Care. J. Affect. Disord. 2009, 119, 52–58. [Google Scholar] [CrossRef]
- De Waal, M.W.M.; Arnold, I.A.; Eekhof, J.A.H.; van Hemert, A.M. Somatoform Disorders in General Practice—Prevalence, Functional Impairment and Comorbidity with Anxiety and Depressive Disorders. Br. J. Psychiatry 2004, 184, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Orav, E.; Bates, D.; Barsky, A. Somatization Increases Disability Independent of Comorbidity. J. Gen. Intern. Med. 2009, 24, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Steinbrecher, N.; Koerber, S.; Frieser, D.; Hiller, W. The Prevalence of Medically Unexplained Symptoms in Primary Care. Psychosomatics 2011, 52, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Bekhuis, E.; Boschloo, L.; Rosmalen, J.G.M.; Schoevers, R.A. Differential Associations of Specific Depressive and Anxiety Disorders with Somatic Symptoms. J. Psychosom. Res. 2015, 78, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Den Boeft, M.; Twisk, J.W.R.; Hoekstra, T.; Terluin, B.; Penninx, B.W.J.H.; van der Wouden, J.C.; Numans, M.E.; van der Horst, H.E. Medically Unexplained Physical Symptoms and Work Functioning over 2 Years: Their Association and the Influence of Depressive and Anxiety Disorders and Job Characteristics.(Report). BMC Fam. Pract. 2016, 17, 46. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Spitzer, R.L.; Williams, J.B.W.; Mussell, M.; Schellberg, D.; Kroenke, K. Depression, Anxiety and Somatization in Primary Care: Syndrome Overlap and Functional Impairment. Gen. Hosp. Psychiatry 2008, 30, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Budtz-Lilly, A.; Vestergaard, M.; Fink, P.; Carlsen, A.H.; Rosendal, M. Patient Characteristics and Frequency of Bodily Distress Syndrome in Primary Care: A Cross-Sectional Study. Br. J. Gen. Pract. 2015, 65, e617–e623. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Gilmour, H. Medically Unexplained Physical Symptoms (MUPS) among Adults in Canada: Comorbidity, Health Care Use and Employment. Health Rep. 2017, 28, 3. [Google Scholar] [PubMed]
- Aamland, A.; Malterud, K.; Werner, E.L. Patients with Persistent Medically Unexplained Physical Symptoms: A Descriptive Study from Norwegian General Practice. BMC Fam. Pract. 2014, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Momsen, A.H.; Nielsen, C.V.; Nielsen, M.B.D.; Rugulies, R.; Jensen, C. Work Participation and Health-Related Characteristics of Sickness Absence Beneficiaries with Multiple Somatic Symptoms. Public Health 2016, 133, 75–82. [Google Scholar] [CrossRef]
- Loengaard, K.; Bjorner, J.B.; Fink, P.K.; Burr, H.; Rugulies, R. Medically Unexplained Symptoms and the Risk of Loss of Labor Market Participation--a Prospective Study in the Danish Population. BMC Public Health 2015, 15, 844. [Google Scholar] [CrossRef] [PubMed]
- Rask, M.T.; Ørnbøl, E.; Rosendal, M.; Fink, P. Long-Term Outcome of Bodily Distress Syndrome in Primary Care: A Follow-up Study on Health Care Costs, Work Disability, and Self-Rated Health. Psychosom. Med. 2017, 79, 345–357. [Google Scholar] [CrossRef]
- Barsky, A.J.; Orav, E.J.; Bates, D.W. Somatization Increases Medical Utilization and Cost Independent of Psychiatric and Medical Comorbidity. Arch. Gen. Psychiatry 2005, 62, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Gill, N.S.; Teodorczuk, A.; Li, Z.; Sun, J. The Efficacy of Cognitive Behavioural Therapy in Somatoform Disorders and Medically Unexplained Physical Symptoms: A Meta-Analysis of Randomized Controlled Trials. J. Affect. Disord. 2019, 245, 98–112. [Google Scholar] [CrossRef]
- Sanders, S.; Coppin, S.; Moulson, H.; Meola, J.; Meyrick, J. What adaptions are effective to cognitive behavioural interventions for adults with long-term conditions and medically unexplained symptoms? A systematic review. Ansiedad Estrés 2020, 26, 188–201. [Google Scholar] [CrossRef]
- Kleinstäuber, M.; Witthöft, M.; Hiller, W. Efficacy of Short-Term Psychotherapy for Multiple Medically Unexplained Physical Symptoms: A Meta-Analysis. Clin. Psychol. Rev. 2011, 31, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Kleinstäuber, M.; Allwang, C.; Bailer, J.; Berking, M.; Brünahl, C.; Erkic, M.; Gitzen, H.; Gollwitzer, M.; Gottschalk, J.-M.; Heider, J.; et al. Cognitive Behaviour Therapy Complemented with Emotion Regulation Training for Patients with Persistent Physical Symptoms: A Randomised Clinical Trial. Psychother. Psychosom. 2019, 88, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-Y.; Lee, J.-S.; Park, S.-Y.; Kim, S.-J.; Son, C.-G. Systematic Review of Randomized Controlled Trials for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Malouff, J.M.; Thorsteinsson, E.B.; Rooke, S.E.; Bhullar, N.; Schutte, N.S. Efficacy of Cognitive Behavioral Therapy for Chronic Fatigue Syndrome: A Meta-Analysis. Clin. Psychol. Rev. 2008, 28, 736–745. [Google Scholar] [CrossRef] [PubMed]
- White, P.; Goldsmith, K.; Johnson, A.; Potts, L.; Walwyn, R.; DeCesare, J.; Baber, H.; Burgess, M.; Clark, L.; Cox, D.; et al. Comparison of Adaptive Pacing Therapy, Cognitive Behaviour Therapy, Graded Exercise Therapy, and Specialist Medical Care for Chronic Fatigue Syndrome (PACE): A Randomised Trial. Lancet 2011, 377, 823–836. [Google Scholar] [CrossRef]
- Huibers, M.J.H.; Beurskens, A.; Prins, J.B.; Kant, I.J.; Bazelmans, E.; Van Schayck, C.P.; Knottnerus, J.A.; Bleijenberg, G. Fatigue, Burnout, and Chronic Fatigue Syndrome among Employees on Sick Leave: Do Attributions Make the Difference? Occup. Environ. Med. 2003, 60, i26–i31. [Google Scholar] [CrossRef] [PubMed]
- Leone, S.S.; Huibers, M.J.H.; Knottnerus, J.A.; Kant, I.J. Similarities, Overlap and Differences between Burnout and Prolonged Fatigue in the Working Population. QJM 2007, 100, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Maroti, D.; Bileviciute-Ljungar, I. Similarities and Differences between Health-Related Quality of Life in Patients with Exhaustion Syndrome and Chronic Fatigue Syndrome. Fatigue Biomed. Health Behav. 2018, 6, 208–219. [Google Scholar] [CrossRef]
- Maroti, D.; Molander, P.; Bileviciute-Ljungar, I. Differences in Alexithymia and Emotional Awareness in Exhaustion Syndrome and Chronic Fatigue Syndrome. Scand. J. Psychol. 2017, 58, 52–61. [Google Scholar] [CrossRef]
- Wiegner, L.; Hange, D.; Björkelund, C.; Ahlborg, G. Prevalence of Perceived Stress and Associations to Symptoms of Exhaustion, Depression and Anxiety in a Working Age Population Seeking Primary Care—An Observational Study. BMC Fam. Pract. 2015, 16, 38–46. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.M.D. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Mundt, J.; Marks, I.; Shear, M.; Greist, J. The Work and Social Adjustment Scale: A Simple Measure of Impairment in Functioning. Br. J. Psychiatry 2002, 180, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Leone, S.S.; Wessely, S.; Huibers, M.J.; Knottnerus, J.A.; Kant, Ij. Two Sides of the Same Coin? On the History and Phenomenology of Chronic Fatigue and Burnout. Psychol. Health 2011, 26, 449–464. [Google Scholar] [CrossRef]
- Toft, T.; Fink, P.E.R.; Oernboel, E.V.A.; Christensen, K.A.J.; Frostholm, L.; Olesen, F. Mental Disorders in Primary Care: Prevalence and Co-Morbidity among Disorders. Results from the Functional Illness in Primary Care (FIP) Study. Psychol. Med. 2005, 35, 1175–1184. [Google Scholar] [CrossRef]
- Flóvenz, S.Ó.; Salkovskis, P.M.; Svansdóttir, E.; Andersen, K. Non-Cardiac Chest Pain as a Persistent Physical Symptom and Its Relationship with Other Persistent Physical Symptoms, Psychological Distress and Workability. (submitted).
- Rask, M.T.; Rosendal, M.; Fenger-Grøn, M.; Bro, F.; Ørnbøl, E.; Fink, P. Sick Leave and Work Disability in Primary Care Patients with Recent-Onset Multiple Medically Unexplained Symptoms and Persistent Somatoform Disorders: A 10-Year Follow-up of the FIP Study. Gen. Hosp. Psychiatry 2015, 37, 53–59. [Google Scholar] [CrossRef]
- Mellner, C.; Krantz, G.; Lundberg, U. Medically Unexplained Symptoms in Women as Related to Physiological Stress Responses. Stress Health 2005, 21, 45–52. [Google Scholar] [CrossRef]
- Conversano, C.; Carmassi, C.; Bertelloni, C.A.; Marchi, L.; Micheloni, T.; Carbone, M.G.; Pagni, G.; Tagliarini, C.; Massimetti, G.; Bazzichi, L. Potentially Traumatic Events, Post-Traumatic Stress Disorder and Post-Traumatic Stress Spectrum in Patients with Fibromyalgia. Clin. Exp. Rheumatol. 2019, 37, 39–43. [Google Scholar] [PubMed]
- Fischer, S.; Doerr, J.M.; Strahler, J.; Mewes, R.; Thieme, K.; Nater, U.M. Stress Exacerbates Pain in the Everyday Lives of Women with Fibromyalgia Syndrome—The Role of Cortisol and Alpha-Amylase. Psychoneuroendocrinology 2016, 63, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Van Houdenhove, B.; Luyten, P. Stress, Depression and Fibromyalgia. Acta Neurol. Belg. 2006, 106, 149. [Google Scholar] [PubMed]
- Grossi, G.; Perski, A.; Osika, W.; Savic, I. Stress-Related Exhaustion Disorder–Clinical Manifestation of Burnout? A Review of Assessment Methods, Sleep Impairments, Cognitive Disturbances, and Neuro-Biological and Physiological Changes in Clinical Burnout. Scand. J. Psychol. 2015, 56, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Ridsdale, L.; Evans, A.; Jerrett, W.; Mandalia, S.; Osler, K.; Vora, H. Patients with Fatigue in General Practice: A Prospective Study. Br. Med. J. 1993, 307, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.; Chalder, T. Overcoming Chronic Fatigue. A Self-Help Guide Using Cognitive Behavioural Techniques; Robinson: London, UK, 2009. [Google Scholar]


{kind=link}
| Demographic Variables | All Participants | Fatigue Met PPS Criteria | Fatigue Did Not Meet PPS Criteria | χ2 |
|---|---|---|---|---|
| Gender | ||||
| Female | 892 (81.8%) | 100 (94.3%) | 792 (80.5%) | 12.351 *** |
| Male | 198 (18.2%) | 6 (5.7%) | 192 (19.5%) | |
| Age | ||||
| 30 years or younger | 60 (5.5%) | 6 (5.7%) | 54 (5.5%) | 0.006 |
| 31–50 years | 699 (64.1%) | 68 (64.2%) | 631 (64.1%) | |
| 51–70 years | 331 (30.4%) | 32 (30.2%) | 299 (30.4%) | |
| Education completed | ||||
| Undergraduate degree | 465 (42.7%) | 52 (49.1%) | 413 (42.0%) | 1.964 |
| Graduate degree | 625 (57.3%) | 54 (50.9%) | 571 (58.0%) | |
| Marital status | ||||
| Single | 128 (11.8%) | 17 (16.2%) | 111 (11.4%) | 2.971 |
| Married/relationship | 880 (81.4%) | 79 (75.2%) | 801 (82.1%) | |
| Separated/widowed | 73 (6.8%) | 9 (8.6%) | 564 (6.6%) | |
| Employment | ||||
| Executives and managers | 290 (26.9%) | 32 (30.8%) | 258 (26.5%) | 3.292 |
| Specialists | 398 (36.9%) | 32 (30.8%) | 366 (37.6%) | |
| Specialists in human services | 335 (31.1%) | 36 (34.6%) | 299 (30.7%) | |
| Specialised workers | 9 (0.8%) | 0 (0.0%) | 9 (0.9%) | |
| Retail, service and other | 46 (4.3%) | 4 (3.8%) | 42 (4.3%) | |
| Total | 1090 (100%) | 106 (9.7%) | 984 (90.3%) |
| Measures | All Participants | Fatigue Met PPS Criteria | Fatigue Did Not Meet PPS Criteria | Sig. | Effect Size |
|---|---|---|---|---|---|
| Means | M (SD) | M (SD) | M (SD) | T | r |
| PHQ-9 | 9.34 (4.6) | 11.63 (5.0) | 9.08 (4.5) | −5.36 *** | 0.17 |
| GAD-7 | 7.73 (4.6) | 9.49 (5.1) | 7.52 (4.5) | −4.14 *** | 0.13 |
| WSAS | 13.04 (8.4) | 20.07 (8.6) | 12.22 (8.0) | −9.33 *** | 0.28 |
| Cut-offs | N (%) | N (%) | N (%) | χ2 | OR [95% CI] |
| PHQ-9≥10 | 389 (35.7%) | 60 (56.6%) | 392 (33.4%) | 16.44 *** | 2.43 [1.6–3.8] |
| GAD-7≥10 | 290 (26.6%) | 44 (41.5%) | 246 (25.0%) | 10.98 *** | 2.04 [1.3–3.1] |
| WSAS≥10 | 581 (53.3%) | 91 (85.8%) | 490 (49.8%) | 44.37 *** | 9.29 [4.3–20.3] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broddadóttir, E.; Flóvenz, S.Ó.; Gylfason, H.F.; Þormar, Þ.; Einarsson, H.; Salkovskis, P.; Sigurðsson, J.F. “I’m So Tired”: Fatigue as a Persistent Physical Symptom among Working People Experiencing Exhaustion Disorder. Int. J. Environ. Res. Public Health 2021, 18, 8657. https://doi.org/10.3390/ijerph18168657
Broddadóttir E, Flóvenz SÓ, Gylfason HF, Þormar Þ, Einarsson H, Salkovskis P, Sigurðsson JF. “I’m So Tired”: Fatigue as a Persistent Physical Symptom among Working People Experiencing Exhaustion Disorder. International Journal of Environmental Research and Public Health. 2021; 18(16):8657. https://doi.org/10.3390/ijerph18168657
Chicago/Turabian StyleBroddadóttir, Elín, Sigrún Ólafsdóttir Flóvenz, Haukur Freyr Gylfason, Þórey Þormar, Hjalti Einarsson, Paul Salkovskis, and Jón Friðrik Sigurðsson. 2021. "“I’m So Tired”: Fatigue as a Persistent Physical Symptom among Working People Experiencing Exhaustion Disorder" International Journal of Environmental Research and Public Health 18, no. 16: 8657. https://doi.org/10.3390/ijerph18168657
APA StyleBroddadóttir, E., Flóvenz, S. Ó., Gylfason, H. F., Þormar, Þ., Einarsson, H., Salkovskis, P., & Sigurðsson, J. F. (2021). “I’m So Tired”: Fatigue as a Persistent Physical Symptom among Working People Experiencing Exhaustion Disorder. International Journal of Environmental Research and Public Health, 18(16), 8657. https://doi.org/10.3390/ijerph18168657