
Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Demographic Information
2.2.2. Psychological Distress
2.2.3. COVID-19-Related Stress and Effects
2.2.4. COVID-19-Related Difficulties
2.3. Statistical Analyses
2.3.1. Japanese Workers’ Psychological Distress during the COVID-19 Pandemic
2.3.2. Assessment of COVID-19-Related Difficulties under Item Response Theory
2.3.3. Relationships between CORDI and Other Characteristics
3. Results
3.1. Japanese Workers’ Psychological Distress under the COVID-19 Pandemic
3.2. Assessment of COVID-19-Related Difficulties under Item Response Theory
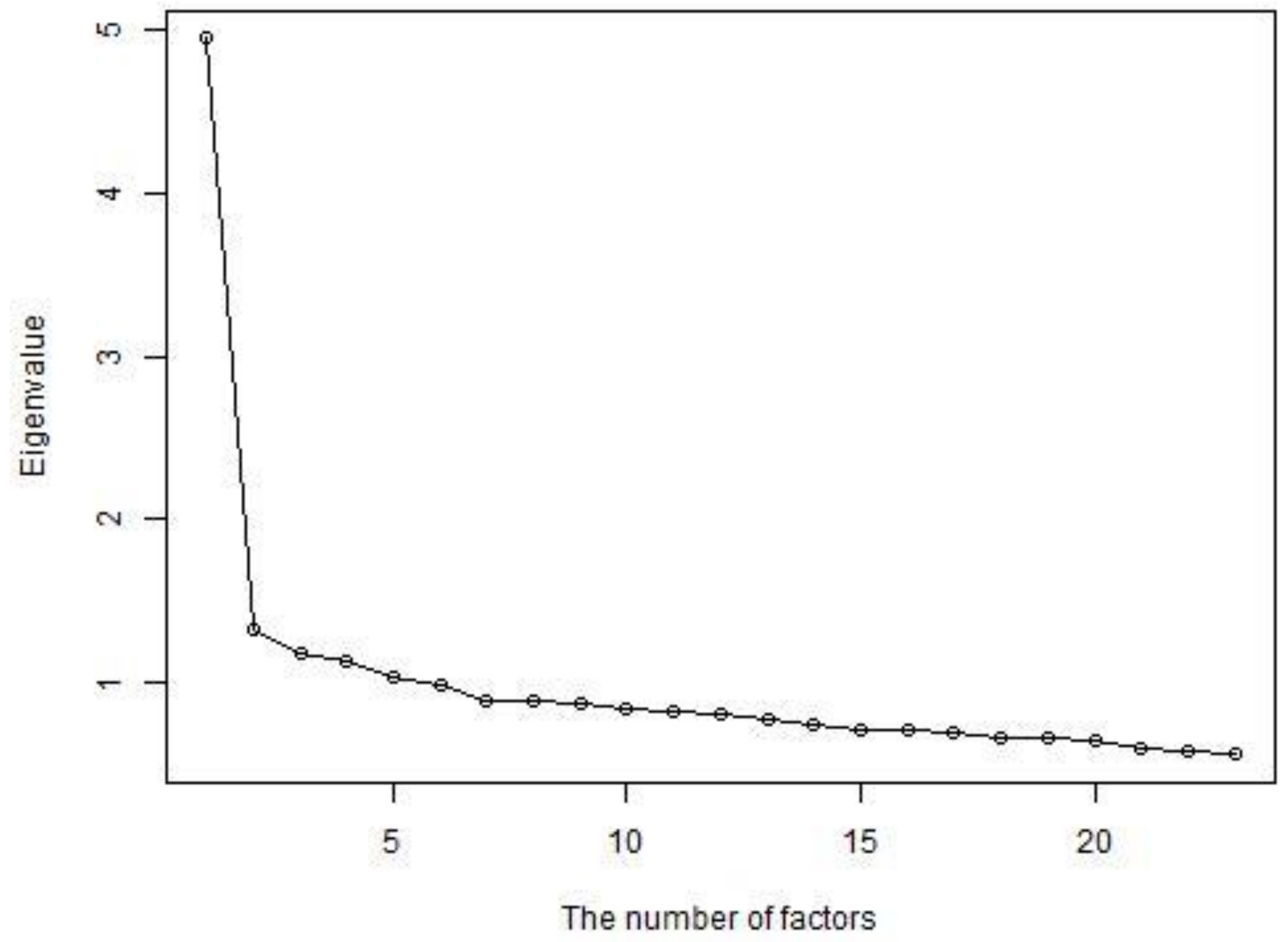
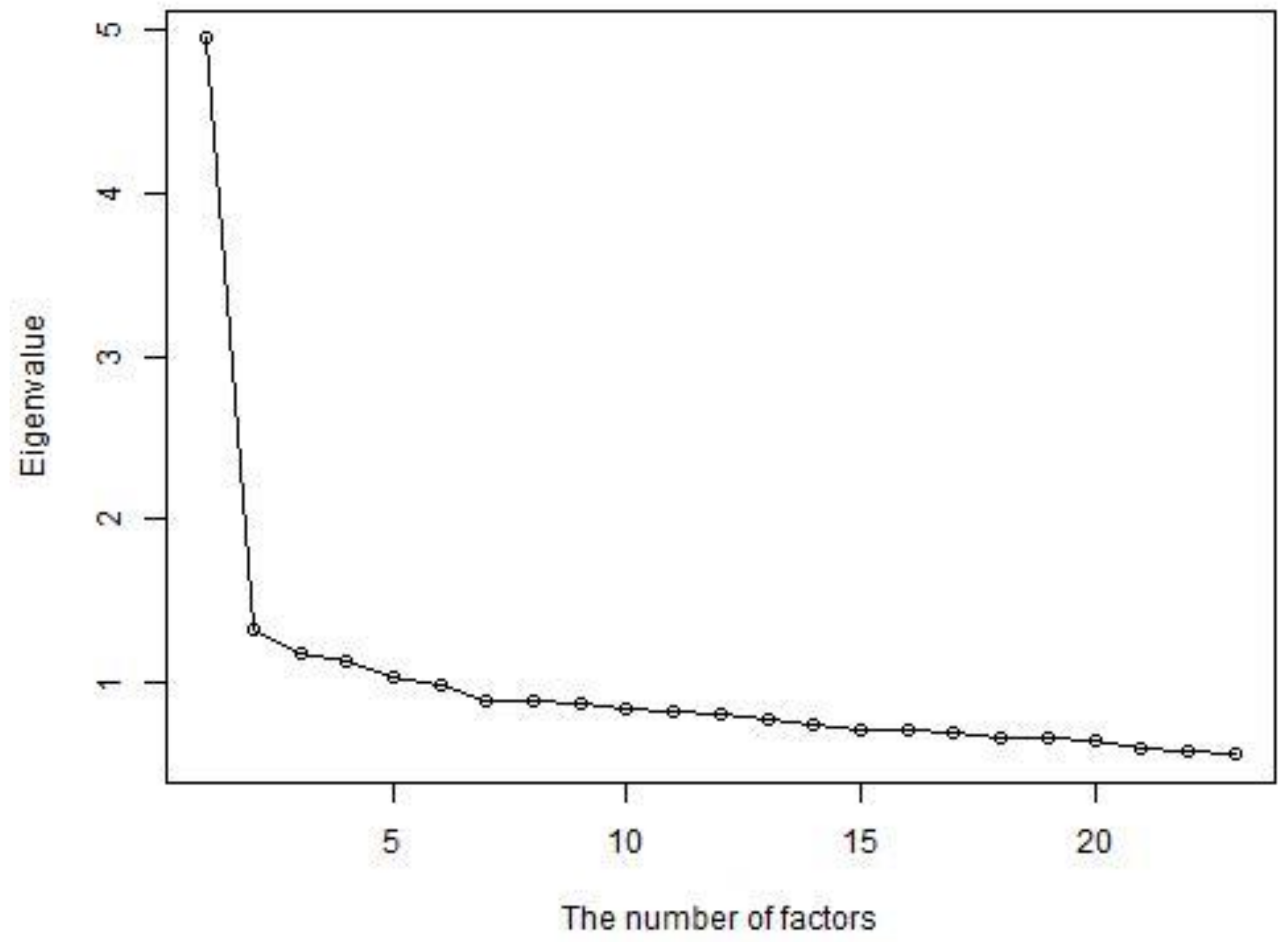
3.2.1. Assumption of Unidimensionality
3.2.2. Assumption of Local Independence
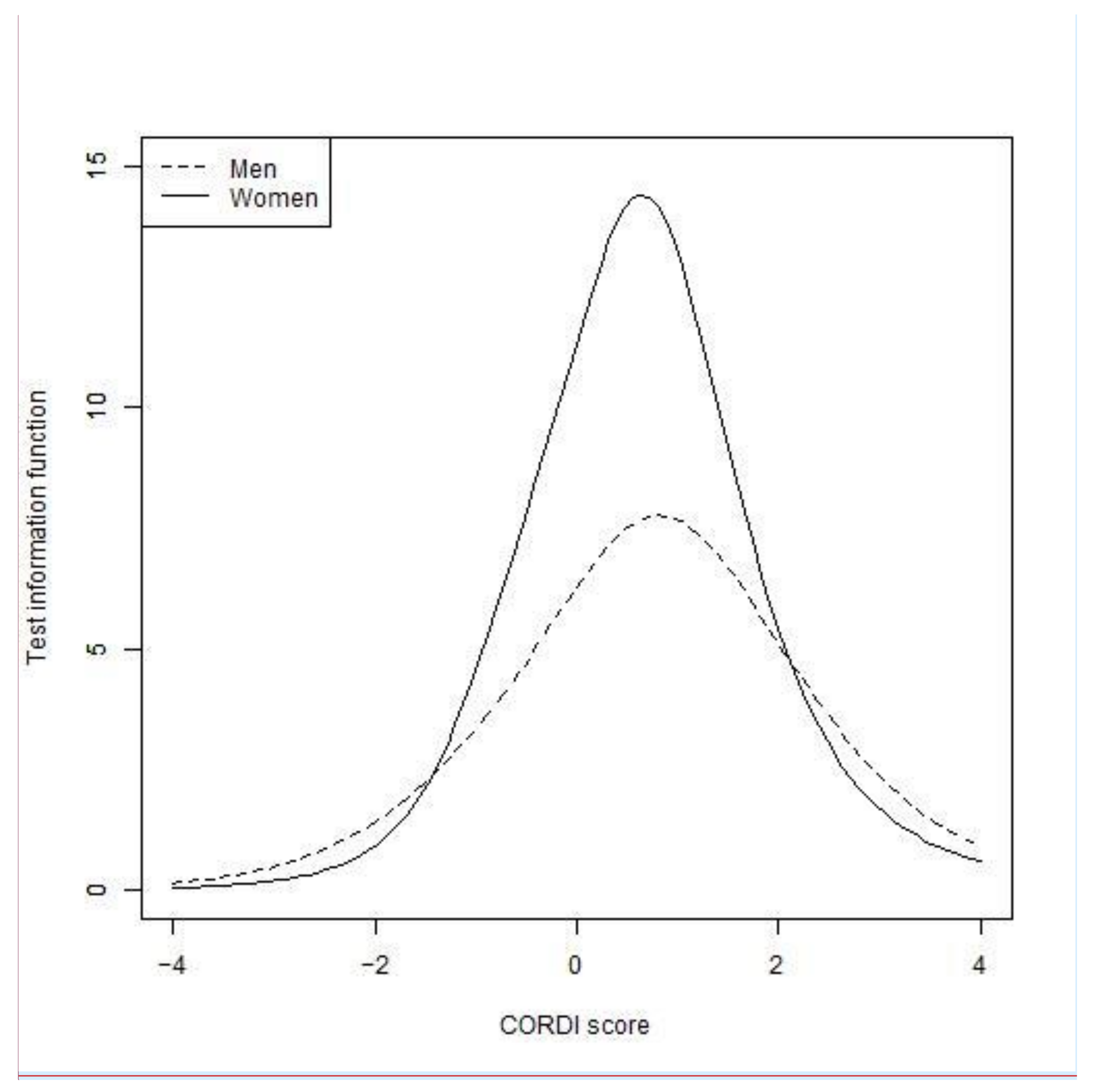
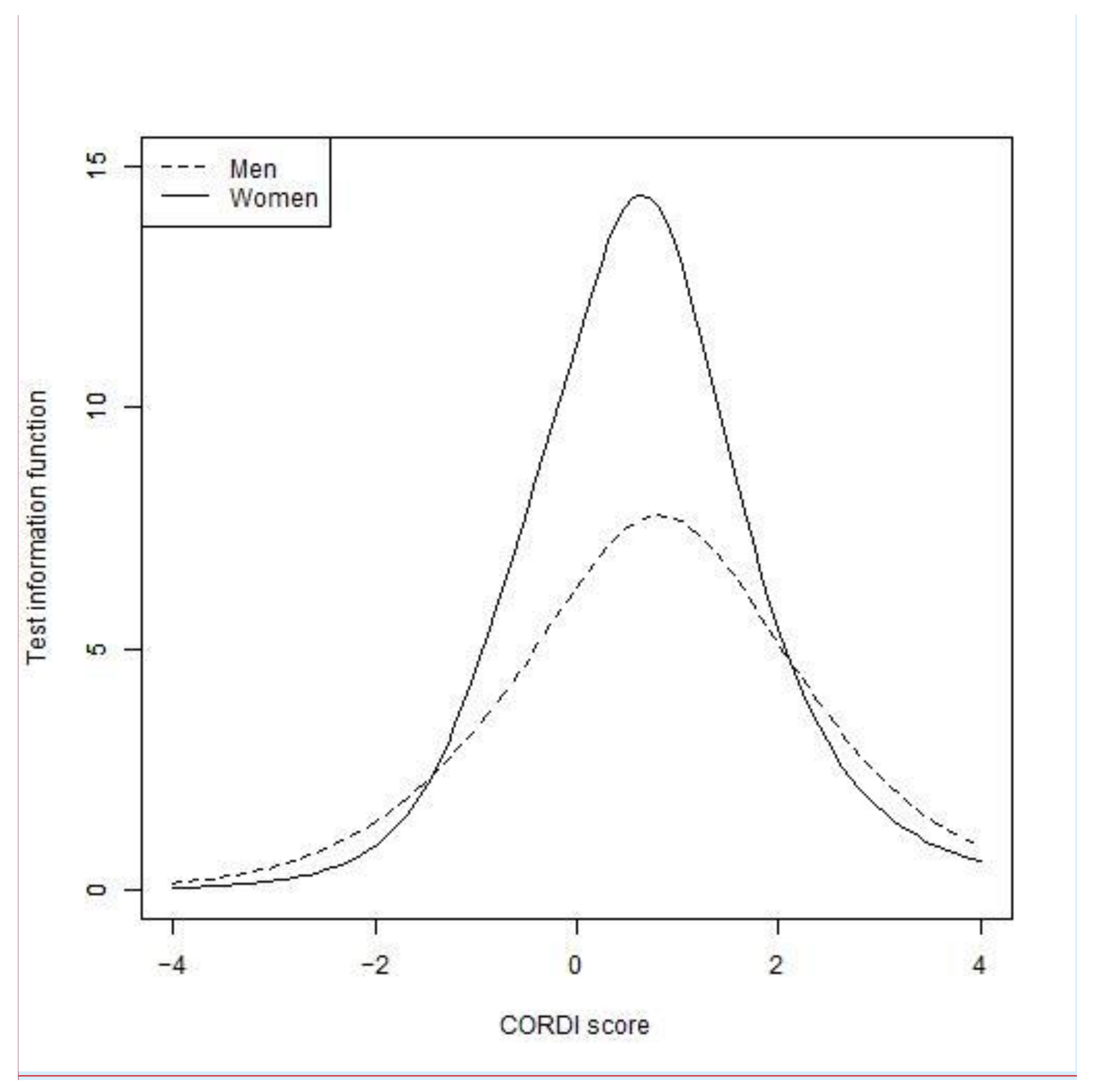
3.2.3. Differential Item Functioning between Men and Women
3.2.4. Reliability and Convergent Validity of the Item Set
3.3. Relationships between CORDI and Other Variables
4. Discussion
4.1. Psychological Distress among Japanese Workers
4.2. Gender Gap in Difficulties Caused by the COVID-19 Pandemic
4.3. Gender Differences by Industry Types
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 18 May 2021).
- Our World in Data Coronavirus (COVID-19) Vaccinations—Statistics and Research. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 28 May 2021).
- Tashiro, A.; Shaw, R. COVID-19 Pandemic Response in Japan: What Is behind the Initial Flattening of the Curve? Sustainability 2020, 12, 5250. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 17 January 2021).
- Baldwin, R.; di Mauro, B.W. Economics in the Time of COVID-19; CEPR Press: London, UK, 2020; ISBN 978-1-912179-28-2. [Google Scholar]
- International Labour Organization COVID-19 and the World of Work: Impact and Policy Responses 2020. Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/documents/briefingnote/wcms_738753.pdf (accessed on 20 May 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The Socio-Economic Implications of the Coronavirus Pandemic (COVID-19): A Review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- The Japan Times. At Least 400,000 Chinese Travelers Expected to Cancel Trips to Japan by End of March. The Japan Times, 4 February 2020. [Google Scholar]
- Milne, G.J.; Xie, S. The Effectiveness of Social Distancing in Mitigating COVID-19 Spread: A Modelling Analysis. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Statistics Bureau of Japan Labour Force Survey. Available online: https://www.stat.go.jp/english/data/roudou/index.html (accessed on 28 May 2021).
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and Social Isolation during the COVID-19 Pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef] [PubMed]
- Prime Minister’s Office of Japan. [COVID-19] Government Responses on the Coronavirus Disease 2019 (Ongoing Topics). Available online: http://japan.kantei.go.jp/ongoingtopics/_00013.html (accessed on 4 June 2021).
- Hoang, V.T.; Al-Tawfiq, J.A.; Gautret, P. The Tokyo Olympic Games and the Risk of COVID-19. Curr. Trop. Med. Rep. 2020, 7, 126–132. [Google Scholar] [CrossRef]
- Logie, C.H.; Turan, J.M. How Do We Balance Tensions between COVID-19 Public Health Responses and Stigma Mitigation? Learning from HIV Research. AIDS Behav. 2020, 24, 2003–2006. [Google Scholar] [CrossRef] [Green Version]
- Roberto, K.J.; Johnson, A.F.; Rauhaus, B.M. Stigmatization and Prejudice during the COVID-19 Pandemic. Adm. Theory Prax. 2020, 42, 364–378. [Google Scholar] [CrossRef]
- Shimizu, K.; Tokuda, Y.; Shibuya, K. Japan Should Aim to Eliminate Covid-19. BMJ 2021, 372, n294. [Google Scholar] [CrossRef]
- NHK Jishukukeisatsu Aitsugu Syakai No Bundan Fusegu Reiseinataiou Wo Shingatakorona [Increased COVID-19 Vigilantes: Keep a Cool Head for Society, COVID-19]. NHK News, 9 May 2020. (In Japanese)
- Shimazu, A.; Nakata, A.; Nagata, T.; Arakawa, Y.; Kuroda, S.; Inamizu, N.; Yamamoto, I. Psychosocial Impact of COVID-19 for General Workers. J. Occup. Health 2020, 62, e12132. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Inoue, A.; Sekijima, K. Teleworker Performance in the COVID-19 Era in Japan. Asian Econ. Pap. 2021, 20, 175–192. [Google Scholar] [CrossRef]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.-A.; Ellis, L.; Polson, R.; O’Malley, C.M. A Rapid Review of the Impact of COVID-19 on the Mental Health of Healthcare Workers: Implications for Supporting Psychological Well-Being. BMC Public Health 2021, 21, 104. [Google Scholar] [CrossRef]
- Mehta, S.; Machado, F.; Kwizera, A.; Papazian, L.; Moss, M.; Azoulay, É.; Herridge, M. COVID-19: A Heavy Toll on Health-Care Workers. Lancet Respir. Med. 2021, 9, 226–228. [Google Scholar] [CrossRef]
- Bagcchi, S. Stigma during the COVID-19 Pandemic. Lancet Infect. Dis. 2020, 20, 782–782. [Google Scholar] [CrossRef]
- American Psychological Association Guidelines for Psychological Practice for People with Low-Income and Economic Marginalization 2019. Available online: https://www.apa.org/about/policy/guidelines-low-income.pdf (accessed on 15 August 2021).
- Ali, S.R.; Fall, K.; Hoffman, T. Life without Work: Understanding Social Class Changes and Unemployment through Theoretical Integration. J. Career Assess. 2012, 21, 111–126. [Google Scholar] [CrossRef]
- Matthews, K.A.; Gallo, L.C. Psychological Perspectives on Pathways Linking Socioeconomic Status and Physical Health. Annu. Rev. Psychol. 2010, 62, 501–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, K.I.; Moser, K. Unemployment Impairs Mental Health: Meta-Analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Fraser, T.; Aldrich, D.P. The Dual Effect of Social Ties on COVID-19 Spread in Japan. Sci. Rep. 2021, 11, 1596. [Google Scholar] [CrossRef] [PubMed]
- Holton, M.K.; Barry, A.E.; Chaney, J.D. Employee Stress Management: An Examination of Adaptive and Maladaptive Coping Strategies on Employee Health. Work 2016, 53, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xia, Q.; Xiong, Z.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z. The Psychological Distress and Coping Styles in the Early Stages of the 2019 Coronavirus Disease (COVID-19) Epidemic in the General Mainland Chinese Population: A Web-Based Survey. PLoS ONE 2020, 15, e0233410. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Kikuchi, H.; Machida, M.; Nakamura, I.; Saito, R.; Odagiri, Y.; Kojima, T.; Watanabe, H.; Fukui, K.; Inoue, S. Changes in Psychological Distress during the COVID-19 Pandemic in Japan: A Longitudinal Study. J. Epidemiol. 2020, 30, 522–528. [Google Scholar] [CrossRef]
- Salazar de Pablo, G.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of Coronavirus Syndromes on Physical and Mental Health of Health Care Workers: Systematic Review and Meta-Analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Mæhlisen, M.H.; Pasgaard, A.A.; Mortensen, R.N.; Vardinghus-Nielsen, H.; Torp-Pedersen, C.; Bøggild, H. Perceived Stress as a Risk Factor of Unemployment: A Register-Based Cohort Study. BMC Public Health 2018, 18, 728. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Okamoto, S. Increase in Suicide Following an Initial Decline during the COVID-19 Pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-S.; Stuckler, D.; Yip, P.; Gunnell, D. Impact of 2008 Global Economic Crisis on Suicide: Time Trend Study in 54 Countries. BMJ 2013, 347, f5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Choi, Y.J.; Sawada, Y. How Is Suicide Different in Japan? Jpn. World Econ. 2009, 21, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Coope, C.; Gunnell, D.; Hollingworth, W.; Hawton, K.; Kapur, N.; Fearn, V.; Wells, C.; Metcalfe, C. Suicide and the 2008 Economic Recession: Who Is Most at Risk? Trends in Suicide Rates in England and Wales 2001–2011. Soc. Sci. Med. 2014, 117, 76–85. [Google Scholar] [CrossRef]
- Ding, Y.; Du, X.; Li, Q.; Zhang, M.; Zhang, Q.; Tan, X.; Liu, Q. Risk Perception of Coronavirus Disease 2019 (COVID-19) and Its Related Factors among College Students in China during Quarantine. PLoS ONE 2020, 15, e0237626. [Google Scholar] [CrossRef]
- Takahashi, A.M.; Takahashi, S. Gender Salary Differences in Economics Departments in Japan. Econ. Educ. Rev. 2011, 30, 1306–1319. [Google Scholar] [CrossRef] [Green Version]
- UN Women Policy Brief: The Impact of COVID-19 on Women 2020. Available online: https://asiapacific.unwomen.org/-/media/headquarters/attachments/sections/library/publications/2020/policy-brief-the-impact-of-covid-19-on-women-en.pdf?la=en&vs=1406 (accessed on 18 May 2021).
- Abdelrahman, M. Personality Traits, Risk Perception, and Protective Behaviors of Arab Residents of Qatar during the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Turner, H.A. Gender and Social Support: Taking the Bad with the Good? Sex Roles 1994, 30, 521–541. [Google Scholar] [CrossRef]
- Inter-Agency Standing Committee. Interim Guidance: Gender Alert for COVID-19 Outbreak 2020. Available online: https://interagencystandingcommittee.org/system/files/2021-03/IASC%20Interim%20Guidance%20on%20COVID-19%20-%20Gender%20Alert.pdf (accessed on 18 May 2021).
- Embretson, S.E.; Reise, S.P. Item Response Theory for Psychologists; Multivariate Applications Series; Lawrence Erlbaum Associates: Mahwah, NY, USA, 2000; ISBN 0-8058-2819-2. [Google Scholar]
- MHLW Open data. Available online: https://www.mhlw.go.jp/stf/covid-19/open-data.html (accessed on 1 July 2021).
- Karako, K.; Song, P.; Chen, Y.; Tang, W.; Kokudo, N. Overview of the Characteristics of and Responses to the Three Waves of COVID-19 in Japan during 2020–2021. BioScience Trends 2021, 15, 1–8. [Google Scholar] [CrossRef]
- Fukushima Prefecture Fukushima Kennai No Shingata Korona Uirusu Hassei Joukyou [COVID-19 Outbreak State in Fukushima]. Available online: https://www.pref.fukushima.lg.jp/sec/21045c/fukushima-hasseijyoukyou.html (accessed on 2 July 2021).
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The Performance of the Japanese Version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.; Walters, E.E.; Zaslavsky, A.M. Short Screening Scales to Monitor Population Prevalences and Trends in Non-Specific Psychological Distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening Performance of K6/K10 and Other Screening Instruments for Mood and Anxiety Disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Cross Marketing. Shingata Corona Uirus Seikatsu Eikyoudo Tyousa: Dai Nana Kai [Report of the 7th survey for lifestyle under the COVID-19 pandemic] 2020. 2011. Available online: https://www.cross-m.co.jp/report/health/20200622corona/ (accessed on 20 May 2021). (In Japanese).
- Midorikawa, H.; Aiba, M.; Lebowitz, A.; Taguchi, T.; Shiratori, Y.; Ogawa, T.; Takahashi, A.; Takahashi, S.; Nemoto, K.; Arai, T.; et al. Confirming Validity of The Fear of COVID-19 Scale in Japanese with a Nationwide Large-Scale Sample. PLoS ONE 2021, 16, e0246840. [Google Scholar] [CrossRef]
- Survey Research Center. Daisankai Shingatakoronauirusukansensyou ni Kansuru Kokumin Anke-to [The 3rd survey regarding COVID-19] 2020. Available online: https://www.surece.co.jp/wp_surece/wp-content/uploads/2020/06/20200609.pdf (accessed on 20 May 2021). (In Japanese).
- R Core Team. In R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Wickham, H. stringr: Simple, Consistent Wrappers for Common String Operations. 2019. Available online: https://CRAN.R-project.org/package=stringr (accessed on 23 April 2021).
- Wickham, H.; Francois, R.; Henry, L.; Muller, K. dplyr: A Grammar of Data Manipulation. 2021. Available online: https://CRAN.R-project.org/package=dplyr (accessed on 23 April 2021).
- Ludecke, D.; Makowski, D.; Waggoner, P.; Patil, I. performance: Assessment of Regression Models Performance. CRAN 2020. Available online: https://easystats.github.io/performance/ (accessed on 23 April 2021). [CrossRef]
- Partchev, I.; Maris, G. irtoys: A Collection of Functions Related to Item Response Theory (IRT). 2017. Available online: https://CRAN.R-project.org/package=irtoys (accessed on 23 April 2021).
- Magis, D.; Beland, S.; Tuerlinckx, F.; Boeck, P.D. A General Framework and an R Package for the Detection of Dichotomous Differential Item Functioning. Behav. Res. Methods 2010, 42, 847–862. [Google Scholar] [CrossRef] [Green Version]
- Fox, J. polycor: Polychoric and Polyserial Correlations. 2019. Available online: https://CRAN.R-project.org/package=polycor (accessed on 23 April 2021).
- MHLW Comprehensive Survey of Living Conditions in 2019: Mental state in residents over fifteen years old, gender, employing, job type. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450061&tstat=000001141126&cycle=7&year=20190&month=0&tclass1=000001141142&tclass2=000001142126&stat_infid=000031964357&tclass3val=0 (accessed on 21 April 2021).
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and Associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092–102092. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental Health Consequences during the Initial Stage of the 2020 Coronavirus Pandemic (COVID-19) in Spain. BrainBehav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression Among People Affected by versus People Unaffected by Quarantine During the COVID-19 Epidemic in Southwestern China. Med Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Toyoda, H. Koumokuhannouriron: Nyuumonhen [Item Response Theory: Introduction], 2nd ed.; Tokei library; Asakura Publishing: Tokyo, Japan, 2012; p. 71. ISBN 978-4-254-12795-9. [Google Scholar]
- Yen, W.M. Effects of Local Item Dependence on the Fit and Equating Performance of the Three-Parameter Logistic Model. Appl. Psychol. Meas. 1984, 8, 125–145. [Google Scholar] [CrossRef]
- Yen, W.M.; Fitzpatrick, A.R. Item response theory. In Educational Measurement; American Council on Education/Praeger: Washington, DC, USA, 2006; pp. 187–220. ISBN 978-0-275-98125-9. [Google Scholar]
- Toyoda, H. Tokuikoumokukinoou (DIF): IRT ni motozukuhouhou [Differential item functioning (DIF): Methods based on IRT]. In Koumokuhannouriron: Chukyuuhen [Item Response Theory: Intermediate]; Tokei library; Asakura Publishing: Tokyo, Japan, 2013; ISBN 978-4-254-12798-0. [Google Scholar]
- Lord, F.M. Applications of Item Response Theory to Practical Testing Problems; Routledge: New York, NY, USA, 1980; ISBN 0-89859-006-X. [Google Scholar]
- Allen, T.D.; Golden, T.D.; Shockley, K.M. How Effective Is Telecommuting? Assessing the Status of Our Scientific Findings. Psychol. Sci. Public Interest 2015, 16, 40–68. [Google Scholar] [CrossRef]
- Inter-Agency Standing Committee. Basic Psychosocial Skills: A Guide for COVID-19 Responders 2020. Available online: https://interagencystandingcommittee.org/system/files/2020-05/Basic%20Psychosocial%20Skills-%20A%20Guide%20for%20COVID-19%20Responders.pdf (accessed on 20 May 2021).
- Tomczyk, S.; Rahn, M.; Schmidt, S. Social Distancing and Stigma: Association between Compliance with Behavioral Recommendations, Risk Perception, and Stigmatizing Attitudes during the COVID-19 Outbreak. Front. Psychol. 2020, 11, 1821. [Google Scholar] [CrossRef]
- Anzai, A.; Nishiura, H. “Go To Travel” Campaign and Travel-Associated Coronavirus Disease 2019 Cases: A Descriptive Analysis, July–August 2020. J. Clin. Med. 2021, 10, 398. [Google Scholar] [CrossRef] [PubMed]
- Austin, K.W. 4 Tips for Critically Evaluating Data in the Media. Available online: https://spsp.org/news-center/announcements/tips-evaluating-scientifc-data?_zs=9E8eX&_zl=VBG62 (accessed on 20 May 2021).
- Khatri, P.; Singh, S.R.; Belani, N.K.; Yeong, Y.L.; Lohan, R.; Lim, Y.W.; Teo, W.Z. YouTube as Source of Information on 2019 Novel Coronavirus Outbreak: A Cross Sectional Study of English and Mandarin Content. Travel Med. Infect. Dis. 2020, 35, 101636. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.J. Sport and Exercise during and beyond the COVID-19 Pandemic. Eur. J. Prev. Cardiol. 2020, 27, 1239–1241. [Google Scholar] [CrossRef]
- MHLW Shintaikatsudou, Undo [Physical Activity and Exercise]. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/b2.html (accessed on 3 June 2021).
- Taylor, S.E.; Klein, L.C.; Lewis, B.P.; Gruenewald, T.L.; Gurung, R.A.R.; Updegraff, J.A. Biobehavioral Responses to Stress in Females: Tend-and-Befriend, Not Fight-or-Flight. Psychol. Rev. 2000, 107, 411–429. [Google Scholar] [CrossRef]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender Differences in Anxiety Disorders: Prevalence, Course of Illness, Comorbidity and Burden of Illness. J. Psychiatr. Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehaghi, B.F.; Teimori-Boghsani, G.; Ghavamabadi, L.I.; Mohammadi, A. Public Eye toward COVID-19: A Systematic Review. Open Access Maced. J. Med Sci. 2020, 8, 61–65. [Google Scholar] [CrossRef]
- Dragano, N.; Lunau, T. Technostress at Work and Mental Health: Concepts and Research Results. Curr. Opin. Psychiatry 2020, 33, 407–413. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| All | 3464 | ||
| Gender | men | 2613 | 75.4% |
| women | 847 | 24.5% | |
| other | 4 | 0.1% | |
| Age | 10s | 43 | 1.2% |
| 20s | 744 | 21.5% | |
| 30s | 981 | 28.3% | |
| 40s | 1036 | 29.9% | |
| 50s | 597 | 17.2% | |
| 60s | 61 | 1.8% | |
| Nationality | Japanese | 3445 | 99.5% |
| other | 18 | 0.5% | |
| Family members | presence | 1694 | 48.9% |
| absence | 1769 | 51.1% | |
| Disability certificate | presence | 36 | 1.0% |
| absence | 3426 | 98.9% | |
| Underlying diseases | presence | 281 | 8.1% |
| absence | 3179 | 91.8% | |
| History of mental disorders | presence | 114 | 3.3% |
| absence | 3347 | 96.6% | |
| Isolation experience | experienced | 51 | 1.5% |
| not experienced | 3411 | 98.5% | |
| Infection experience | experienced | 35 | 1.0% |
| not experienced | 3428 | 99.0% | |
| Industry type | public employees | 1350 | 39.0% |
| manufacturing workers | 1135 | 32.8% | |
| hotel and restaurant workers | 788 | 22.7% | |
| transport workers | 135 | 3.9% | |
| health care workers | 55 | 1.6% | |
| Job position | administrative position | 883 | 25.5% |
| not administrative position | 2581 | 74.5% | |
| Employment status | full-time | 3230 | 93.2% |
| not full-time | 233 | 6.7% | |
| Education attainment | junior high/high school | 1760 | 50.8% |
| vocational or junior college | 493 | 14.2% | |
| university or graduate school | 1211 | 35.0% | |
| Annual income | <150 | 177 | 5.1% |
| [×104 JPY] | 150–199 | 98 | 2.8% |
| 200–299 | 335 | 9.7% | |
| 300–399 | 615 | 17.8% | |
| 400–499 | 747 | 21.6% | |
| 500–699 | 1027 | 29.6% | |
| 700–999 | 422 | 12.2% | |
| ≥1000 | 42 | 1.2% |
| Predictor | b | 95% CI | |
|---|---|---|---|
| Gender (ref = men) | 0.10 * | [0.06, 0.14] | |
| women | |||
| Age | 0.03 * | [0.01, 0.04] | |
| Nationality (ref = others) | −0.16 | [−0.33, 0.02] | |
| Japanese | |||
| Underlying diseases (ref = absence) | 0.15 * | [0.10, 0.20] | |
| presence | |||
| History of mental disorder (ref = absence) | 0.63 * | [0.56, 0.69] | |
| presence | |||
| Infection experience (ref = absence) | 0.21 * | [0.07, 0.34] | |
| presence | |||
| Industry types (ref = public employees) | |||
| manufacturing workers | 0.03 | [−0.002, 0.07] | |
| hotel and restaurant workers | −0.06 * | [−0.10, −0.02] | |
| transport workers | −0.17 * | [−0.26, −0.09] | |
| health care workers | 0.01 | [−0.10, 0.12] | |
| Job positions (ref = none) | −0.04 * | [−0.08, −0.0002] | |
| administrative worker | |||
| Education attainment (ref = junior high/ high school) | |||
| vocational or junior college | −0.02 | [−0.05, 0.0004] | |
| university or graduate school | −0.01 | [−0.05, 0.02] | |
| Annual income (ref = <150 [ten thousand yen]) | |||
| 150–199 | −0.24 * | [−0.35, −0.14] | |
| 200–299 | −0.07 | [−0.16, 0.01] | |
| 300–399 | 0.13 * | [0.06, 0.21] | |
| 400–499 | 0.07 * | [0.01, 0.14] | |
| 500–699 | 0.02 | [−0.04, 0.07] | |
| 700–999 | 0.07 * | [0.03, 0.12] | |
| ≥1000 | 0.01 | [−0.02, 0.05] | |
| Nagelkerke’s R2 | 0.18 | ||
| Test of deviance (χ2(20)) | 648.53 * | ||
| n | % | Final Item Set for IRT | |
|---|---|---|---|
| 1 Concerns about being laid off or unemployed | 304 | 9.2% | |
| 2 Income has decreased or is under threat of decreasing | 1071 | 32.3% | integrated (CoI 1) |
| 3 Government compensation is difficult to get (e.g., strict restrictions, complexity of procedures) | 210 | 6.3% | |
| 4 The business performance of my company has deteriorated or is under threat of deteriorating | 1076 | 32.5% | integrated (CoI 1) |
| 5 Worry that the Japanese economy will get worse | 1737 | 52.4% | included |
| 6 Work styles have changed (e.g., telework, staggered work hours) | 764 | 23.1% | included |
| 7 Teleworking is not possible or is difficult | 1028 | 31.0% | included |
| 8 Criteria for work absence when symptoms similar to those of COVID-19 appear (low fever, lassitude etc.) are unclear | 659 | 19.9% | included |
| 9 Workload has increased | 694 | 21.0% | |
| 10 Work efficiency has decreased | 712 | 21.5% | included |
| 11 Anxiety that I may be infected | 2370 | 71.6% | integrated (CoI 2) |
| 12 Anxiety that my family members may be infected | 2379 | 71.8% | integrated (CoI 2) |
| 13 Fatigue from taking measures against COVID-19 infection (e.g., hand washing, gargling, masks) | 1007 | 30.4% | included |
| 14 No one to ask for help when I need it | 327 | 9.9% | |
| 15 Concerns that hospitals and other facilities will be unable to cope with the increased number of infected people | 970 | 29.3% | included |
| 16 PCR test is not available for me | 203 | 6.1% | |
| 17 Unable to go to the hospital owing to chronic illness or cold | 627 | 18.9% | included |
| 18 Housing has been lost or is under threat of being lost | 50 | 1.5% | |
| 19 My family’s or my personal information and activities were made public or are under threat of being made public if we are infected | 1147 | 34.6% | integrated (CoI 3) |
| 20 In the COVID-19 context, discrimination in public spaces was experienced or anticipated (e.g., restricted work attendance, forced changes in work content) | 785 | 23.7% | integrated (CoI 3) |
| 21 In the COVID-19 context, slander by neighbours or co-workers was experienced or anticipated | 890 | 26.9% | integrated (CoI 3) |
| 22 Family conflicts have increased (including domestic violence) | 96 | 2.9% | |
| 23 Difficulty in interacting and getting along with people (e.g., having to wear a mask when talking to people) | 1253 | 37.8% | included |
| 24 Uncertain about what is the correct information about SARS CoV-2 | 944 | 28.5% | included |
| 25 Every day, news about SARS CoV-2 appears on the Internet and TV | 1347 | 40.7% | included |
| 26 Food supplies have or may become insufficient | 188 | 5.7% | |
| 27 Daily necessities have or may become insufficient (e.g., tissue paper, toilet paper, diapers, sanitary products, preserved foods) | 412 | 12.4% | integrated (CoI 4) |
| 28 Preventive products have or may become insufficient (e.g., masks, disinfectant) | 808 | 24.4% | integrated (CoI 4) |
| 29 Living expenses have increased (e.g., food expenses) | 613 | 18.5% | included |
| 30 Child’s school or kindergarten has been closed or restricted | 457 | 13.8% | integrated (CoI 5) |
| 31 Reduced opportunities to interact with friends and distant family members | 1727 | 52.1% | included |
| 32 Increased burden of housework (e.g., cooking, laundry, cleaning, childcare) | 297 | 9.0% | |
| 33 No longer able to attend weddings, funerals, school or company events | 1085 | 32.8% | included |
| 34 Lack of exercise for myself and my family | 627 | 18.9% | included |
| 35 Lost/limited transportation due to avoidance of crowds | 538 | 16.2% | included |
| 36 I have too much time | 323 | 9.8% | |
| 37 Adverse effects on child development worry me (e.g., lost learning, decreased academic performance, lack of exercise) | 640 | 19.3% | integrated (CoI 5) |
| 38 No longer able to go out as much as before (e.g., hobbies, lessons, shopping, eating out, live concerts) | 1746 | 52.7% | included |
| 39 Worry that I will not be able to live if I am infected (e.g., securing food, taking care of children) | 961 | 29.0% | included |
| Item No. | Men | Women | Lord’s χ2 | ||
|---|---|---|---|---|---|
| Discrimination | Difficulty | Discrimination | Difficulty | ||
| 5 | 1.23 (0.07) | −0.15 (0.04) | 1.24 (0.15) | 0.32 (0.07) | 51.50 * |
| 6 | 0.93 (0.07) | 1.38 (0.09) | 0.72 (0.17) | 2.60 (0.51) | 17.00 * |
| 7 | 1.04 (0.07) | 1.02 (0.07) | 1.55 (0.17) | 0.71 (0.07) | 7.61 * |
| 8 | 1.02 (0.07) | 1.68 (0.11) | 0.92 (0.16) | 1.76 (0.24) | 0.57 |
| 10 | 0.89 (0.07) | 1.51 (0.11) | 0.93 (0.18) | 2.36 (0.38) | 55.21* |
| 13 | 0.92 (0.06) | 1.11 (0.08) | 1.41 (0.17) | 0.85 (0.08) | 7.36 * |
| 15 | 1.76 (0.10) | 0.81 (0.04) | 2.13 (0.21) | 0.73 (0.05) | 3.76 |
| 17 | 1.22 (0.08) | 1.57 (0.09) | 1.49 (0.19) | 1.27 (0.11) | 1.75 |
| 23 | 1.33 (0.08) | 0.55 (0.05) | 2.19 (0.21) | 0.50 (0.05) | 17.24 * |
| 24 | 1.26 (0.08) | 1.00 (0.06) | 2.14 (0.22) | 0.75 (0.06) | 13.92 * |
| 25 | 1.33 (0.08) | 0.43 (0.04) | 1.93 (0.19) | 0.42 (0.05) | 11.72 * |
| 29 | 1.16 (0.08) | 1.69 (0.10) | 1.82 (0.21) | 1.10 (0.08) | 13.78 * |
| 31 | 1.30 (0.07) | 0.07 (0.04) | 1.92 (0.20) | −0.10 (0.05) | 11.94 * |
| 33 | 1.36 (0.08) | 0.77 (0.05) | 1.63 (0.18) | 0.68 (0.06) | 2.74 |
| 34 | 1.05 (0.08) | 1.71 (0.11) | 1.88 (0.21) | 1.16 (0.09) | 14.14 * |
| 35 | 1.35 (0.09) | 1.62 (0.09) | 1.84 (0.22) | 1.29 (0.10) | 3.93 |
| 38 | 1.44 (0.08) | 0.08 (0.04) | 1.89 (0.20) | −0.21 (0.06) | 18.65 * |
| 39 | 1.79 (0.10) | 0.84 (0.04) | 2.67 (0.26) | 0.64 (0.05) | 9.34 * |
| CoI 1 | 0.72 (0.05) | 0.02 (0.06) | 0.91 (0.14) | 1.02 (0.13) | 114.99 * |
| CoI 2 | 1.47 (0.09) | −1.22 (0.06) | 2.57 (0.29) | −0.62 (0.07) | 54.52 * |
| CoI 3 | 1.23 (0.07) | 0.42 (0.04) | 1.43 (0.16) | 0.32 (0.06) | 1.13 |
| CoI 4 | 1.18 (0.08) | 1.32 (0.08) | 2.05 (0.20) | 0.63 (0.05) | 41.25 * |
| CoI 5 | 1.27 (0.08) | 1.23 (0.07) | 1.17 (0.16) | 1.26 (0.13) | 1.03 |
| Predictor | b | 95% CI |
|---|---|---|
| Gender (ref = men) women | 0.45 * | [0.33, 0.56] |
| Age | 0.15 * | [0.10, 0.19] |
| Family members (ref = none) presence | 0.28 * | [0.19, 0.38] |
| Underlying diseases (ref = absence) presence | 0.19 * | [0.03, 0.35] |
| Industry types (ref = public employees) | ||
| manufacturing workers | 0.13 * | [0.03, 0.23] |
| hotel and restaurant workers | 0.14 * | [0.02, 0.26] |
| transport workers | 0.22 | [−0.01, 0.44] |
| health care workers | 0.14 | [−0.20, 0.48] |
| Employment status (ref = full-time) not | −0.21 * | [−0.41, −0.01] |
| Radj2 | 0.05 | |
| F (9, 3302) | 20.36 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, T.; Maeda, M.; Takebayashi, Y.; Sato, H. Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers. Int. J. Environ. Res. Public Health 2021, 18, 8656. https://doi.org/10.3390/ijerph18168656
Kobayashi T, Maeda M, Takebayashi Y, Sato H. Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers. International Journal of Environmental Research and Public Health. 2021; 18(16):8656. https://doi.org/10.3390/ijerph18168656
Chicago/Turabian StyleKobayashi, Tomoyuki, Masaharu Maeda, Yui Takebayashi, and Hideki Sato. 2021. "Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers" International Journal of Environmental Research and Public Health 18, no. 16: 8656. https://doi.org/10.3390/ijerph18168656
APA StyleKobayashi, T., Maeda, M., Takebayashi, Y., & Sato, H. (2021). Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers. International Journal of Environmental Research and Public Health, 18(16), 8656. https://doi.org/10.3390/ijerph18168656