
Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Overview
2.2. Protocol and Registration
2.3. Search Strategy
2.4. Eligibility Criteria
2.5. Study Selection
2.6. Data Extraction
2.7. Quality Assessment
2.8. Evidence Synthesis
3. Results
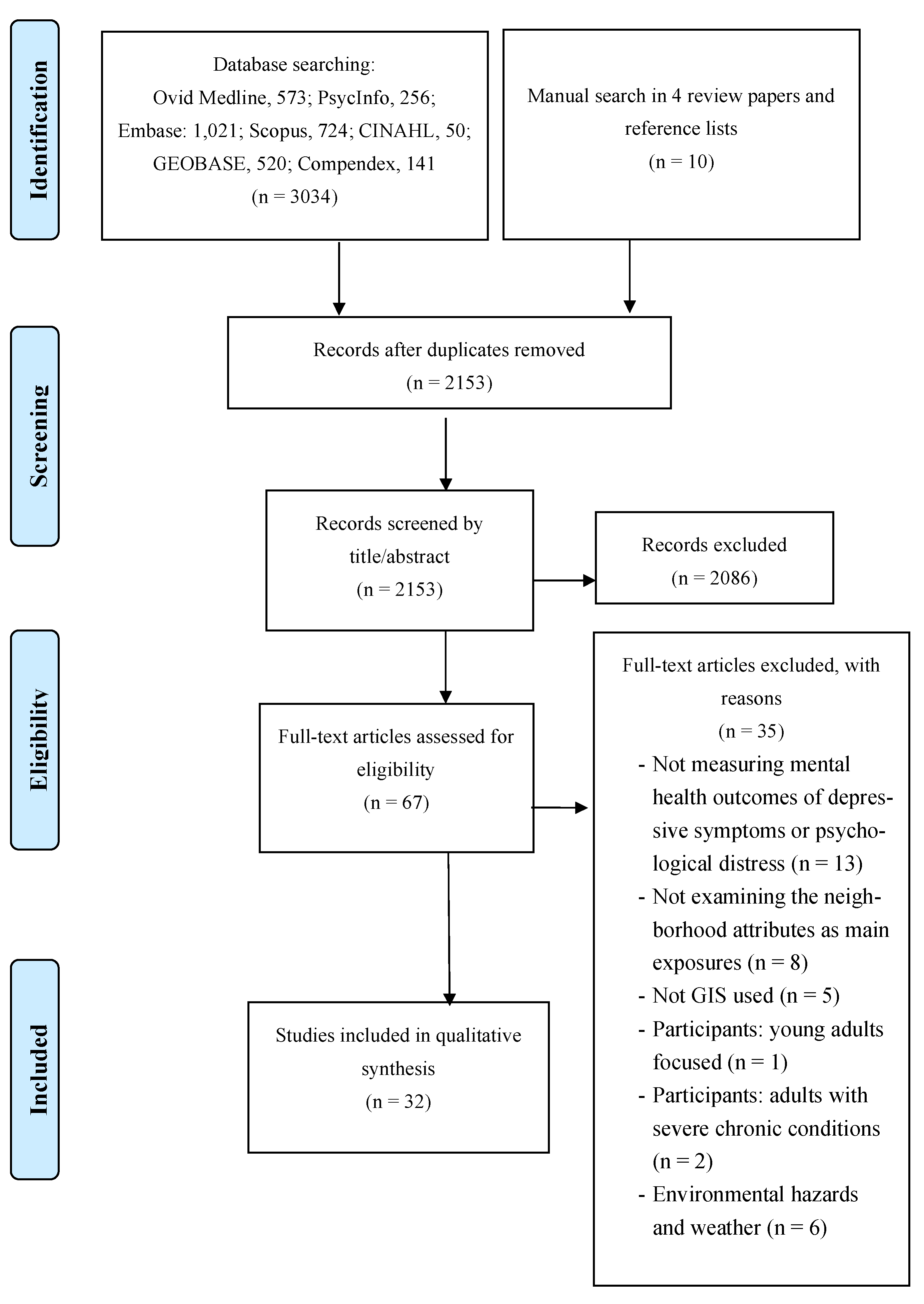
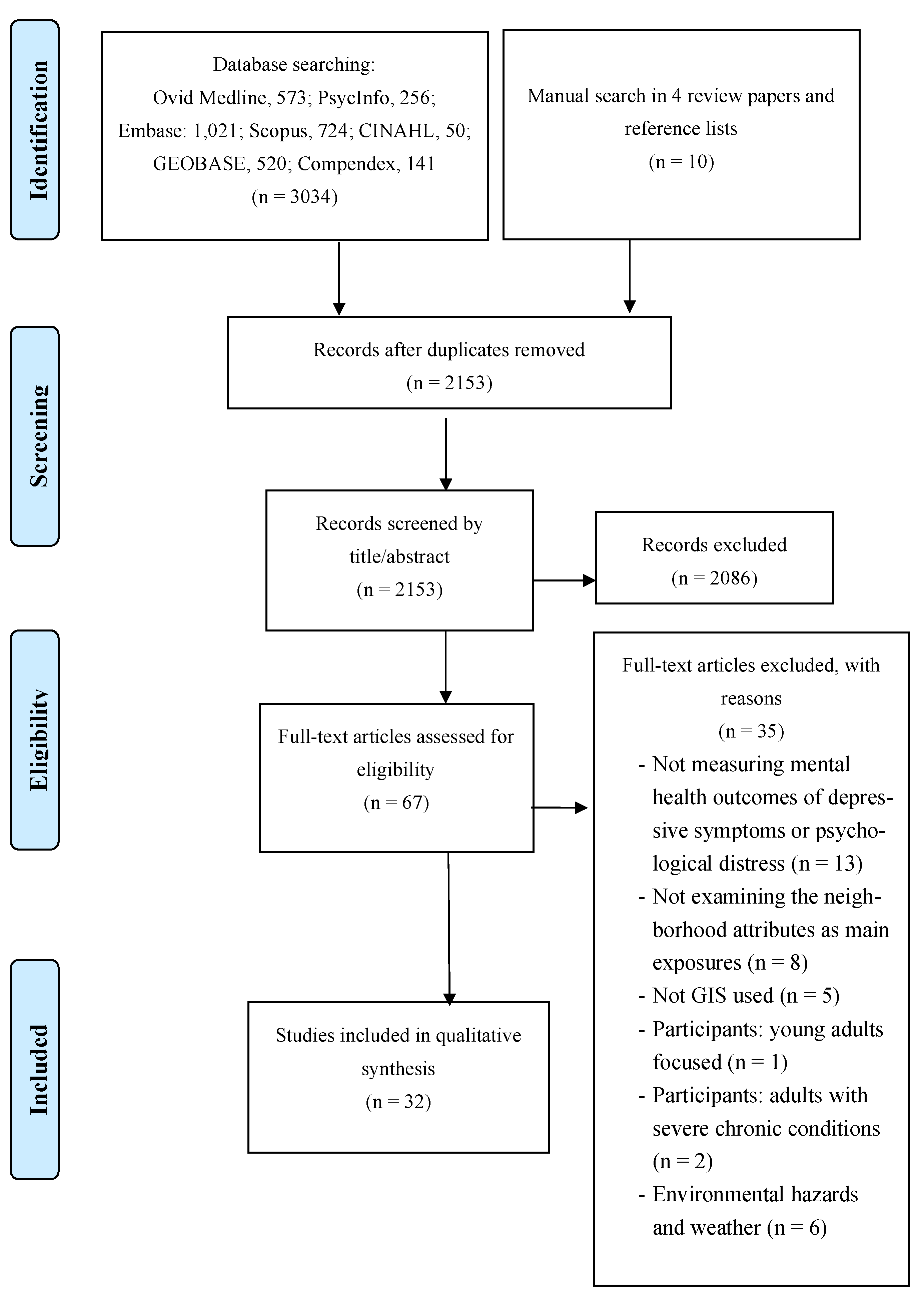
3.1. Study Identification
3.2. Study Characteristics
3.3. Study Quality

{kind=link}
| Author, Date | Clear Definition of Sample Inclusion Criteria | Study and Setting Described in Detail | Valid and Reliable Measurement of the Exposure | Identification of Confounding Factors | Strategies for Confounding Factors Described | Valid and Reliable Measurement of the Outcomes | Appropriate Statistical Analysis Used | Met Quality Criteria (%) |
|---|---|---|---|---|---|---|---|---|
| Ambrey, 2016a | Y | UN | Y | Y | Y | Y | Y | 85.7 |
| Ambrey, 2016b | Y | UN | Y | Y | Y | Y | Y | 85.7 |
| Annerstedt et al., 2012 | UN | Y | Y | Y | Y | Y | Y | 85.7 |
| Astell-Burt et al., 2013 | Y | Y | Y | Y | Y | Y | UN | 85.7 |
| Astell-Burt et al., 2019 | Y | Y | UN | Y | Y | Y | Y | 85.7 |
| Berke et al., 2007 | Y | Y | Y | Y | Y | Y | UN | 85.7 |
| Beyer et al., 2014 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Cromley et al., 2012 | Y | UN | Y | N | UN | Y | Y | 57.1 |
| DeGuzman et al., 2013 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Francis et al., 2012 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Gariepy et al., 2015a | Y | Y | Y | Y | Y | Y | Y | 100 |
| Gariepy et al., 2015b | Y | Y | Y | Y | Y | Y | Y | 100 |
| Ho et al., 2017 | Y | Y | UN | Y | Y | Y | Y | 85.7 |
| Ivey et al., 2015 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Koohsari et al., 2018 | Y | Y | Y | Y | Y | Y | UN | 85.7 |
| Mayne et al., 2018 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Moore et al., 2016 | Y | Y | UN | Y | Y | Y | Y | 85.7 |
| Noordzij et al., 2020 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Nutsford et al., 2016 | UN | Y | Y | Y | Y | Y | Y | 85.7 |
| Rantakokko et al., 2018 | Y | Y | Y | Y | Y | Y | UN | 85.7 |
| Saarloos et al., 2011 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Sakar et al., 2013 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Schootman et al., 2007 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Song et al., 2007 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Su et al., 2019 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Thomas et al., 2007 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Tomita et al., 2017a | Y | Y | Y | Y | Y | Y | Y | 100 |
| Tomita et al., 2017b | Y | Y | Y | Y | Y | Y | UN | 85.7 |
| Traoré et al., 2020 | UN | Y | UN | Y | Y | Y | Y | 71.4 |
| van den Bosch et al., 2015 | Y | Y | Y | Y | Y | Y | Y | 100 |
| Zhang et al., 2018 | Y | Y | UN | Y | Y | Y | Y | 85.7 |
| Zhang et al., 2019 | Y | Y | UN | Y | Y | Y | Y | 85.7 |
| Author, Date | Country | Study Area | Framework | Study Design | Participants | Data Sources (Population) | Data Sources (Neighborhoods) | Outcome Measure |
|---|---|---|---|---|---|---|---|---|
| Ambrey, 2016a | Australia | 7 major cities 1 | Empirical evidence | Cross-sectional | 6082 age 15+ adults | HILDA | PSMA Australia Limited Transport and Topography dataset | Kessler |
| Ambrey, 2016b | Australia | 7 major cities 1 | Empirical evidence | Cross-sectional | 6077 age 15+ adults | HILDA | PSMA Australia Limited Transport and Topography dataset; Australian Bureau of Statistics | Kessler |
| Annerstedt et al., 2012/ van den Bosch et al., 2015 | Sweden | Scania region | Empirical evidence | Longitudinal cohort study | 9230/7549 2 age 18+ adults | Swedish registration system linked survey in a follow-up public health study | The National Land Survey of Sweden (Coordination of Information on the Environment); regional GIS databases; Swedish Environmental Protection Agency; County Administrative Board | Kessler |
| Astell-Burt et al., 2013 | Australia | New South Wales | Empirical evidence | Cross-sectional | 260,061 age 45+ adults | 45 and Up Study | Australian Bureau of Statistics | Kessler |
| Astell-Burt et al., 2019 | Australia | Sydney; Wollongong; Newcastle | Empirical evidence | Longitudinal cohort study | 46,786 age 45+ adults | 45 and Up Study | Geovision (Pitney Bowers Ltd.) | Kessler |
| Berke et al., 2007 | USA | King County | Social stress model | Cross-sectional | 740 age 65+ older adults | Adult Changes in Thought Study | Walkable and Bikable Communities Project (King County GIS Center) | CES-D |
| Beyer et al., 2014 | USA | Wisconsin | Attention Restoration/Stress Reduction Theory | Cross-sectional | 2479 age 21+ adults | Survey of the Health of Wisconsin | Landsat 5 Satellite imagery (USGS); National Land Cover Database | DASS |
| Cromley et al., 2012 | USA | New Jersey | Empirical evidence | Cross-sectional | 5554 age 50+ adults | ORANJ BOWL | US Census Bureau; The Uniform Crime Report State of New Jersey Division of State Police Uniform Crime Reporting Unit | CES-D |
| DeGuzman et al., 2013 | USA | San Antonio; Chicago; Boston | Conceptual framework 3 | Cross-sectional | 1697 adults (mean 38 years) | Welfare, Children and Families: A Three City Study | US Census Chicago Transit Authority and VIA Metropolitan Transit; US Census Bureau | BSI |
| Francis et al., 2012 | Australia | Perth | Social-ecological framework | Cross-sectional | 1230 age 18+ adults | RESIDential Environments Project | SENSIS | Kessler |
| Gariepy et al., 2015a | Canada | Quebec | Empirical evidence | Longitudinal cohort study | 372 age 18+ diabetic adults | Diabetes Health Study | DMTI Lightbox; Statistics Canada; Satellite imagery (Canadian Council on Geomatics) | PHQ |
| Gariepy et al., 2015b | Canada | National | Empirical evidence | Longitudinal cohort study | 7114 age 18+ adults | National Population Health Survey | DMTI Lightbox | CIDI-SFMD |
| Ho et al., 2017 | China | Hong Kong | Data-driven approach | Cross-sectional | 3930 age 65+ older adults | Cohort study | Hong Kong Planning Department; IKONOS multispectral imagery (Satellite imaging corporation) | GDS |
| Ivey et al., 2015 | US | Alameda; Cook; Allegheny; Wake; Curham Counties | Social-ecological framework | Cross-sectional | 870 age 65+ adults | Healthy Aging Research Network’s Walking Study | Environmental Systems Resource Institute Business Analyst; US Census Bureau | CES-D |
| Koohsari et al., 2018 | Australia | Melbourne | Social-ecological framework | Cross-sectional | 319 age 25+ adults | Australian Diabetes Obesity and Lifestyle Study | VicMap Features of Interest dataset (Department of Sustainability and Environment) | CES-D |
| Mayne et al., 2018 | Australia | Sydney | Empirical evidence | Cross-sectional | 91,142 age 45+ adults | 45 and Up Study | Census of Population and Housing; Australian Bureau of Statistics; New South Wales Department of Planning and Infrastructure; New | Kessler |
| Moore et al., 2016 | US | Forsyth County; NYC; Baltimore; St Paul; Chicago; LA | Empirical evidence | Longitudinal cohort study | 5475 age 45+ adults | Multi-Ethnic Study of Atherosclerosis | South Wales Department of Land and Property Information; Property Council of Australia and City of Sydney Council National Establishment Time Series database (Walls & Associates) | CES-D |
| Noordzij et al., 2020 | Netherlands | Eindhoven | Psycho-evolutionary theory | Longitudinal cohort study | 3175 age 15+ adults | GLOBE | Bestand Bodemegruik (Statistics Netherlands) | MHI |
| Nutsford et al., 2016 | New Zealand | Wellington | Empirical evidence | Cross-sectional | 442 age 15+ adults | New Zealand Health Survey | Land Class DataBase II; Department of Conservation land register; Land Information New Zealand parcel database; Land Information New Zealand (LINZ) | Kessler |
| Rantakokko et al., 2018 | Finland | Central Finland | Empirical evidence | Cross-sectional | 848 age 75+ adults | GEOage Project; Life-space mobility in old age Project | Finnish Environment Institute | CES-D |
| Saarloos et al., 2011 | Australia | Perth, Western Australia | Empirical evidence | Cross-sectional | 5218 65+ male adults | Health in Men Study | Western Australia Department for Planning and Infrastructure; Australian Bureau of Statistics | GDS |
| Sakar et al., 2013 | UK | Caerphilly, South Wales | Empirical evidence | Cross-sectional | 687 age 65+ male adults | Caerphilly Prospective Study | UK Ordnance Survey Master Map dataset; Landsat 7 dataset (USGS); UK Office of National Statistics | GHQ |
| Schootman et al., 2007 | US | St Louis, MO | Social disorganization theory | Longitudinal cohort study | 998 middle-age African Americans | African American Health Study | US Census Bureau | CES-D |
| Song et al., 2007 | US | LA | Stress process in neighborhood context | Cross-sectional | 1503 age 18+ adults | Chinese American Psychiatric Epidemiologic Study survey | US Census Bureau; LA GIS center | SCL-90-R |
| Su et al., 2019 | Spain | Barcelona | Empirical evidence | Cross-sectional | 3461 age 18+ adults | 2011 Barcelona Health Survey | WorldView2 imagery (DigitalGlobal); RapidEye imagery (RapidEye AG); Landsat8 imagery (USGS) | GHQ |
| Thomas et al., 2007 | UK | Neath Port Talbot County Borough, South Wales | Empirical evidence | Cross-sectional | 1508 age 16+ adults | Housing And Neighborhood And Health | Neath Port Talbot County Borough Council | GHQ |
| Tomita et al., 2017a | South Africa | National | Empirical evidence | Longitudinal cohort study | 11,156 age 15+ adults | SA-NIDS | National Aeronautics and Space Administration MODIS satellite (MOD13A3) | CES-D |
| Tomita et al., 2017b | South Africa | KwaZulu-Natal Province | Behavioral Model of Health Services Use framework | Longitudinal cohort study | 4309 age 15+ adults | SA-NIDS | KZN Department of Health | CES-D |
| Traoré et al., 2020 | France | Paris | Empirical evidence | Cross-sectional | 3006 age 15+ adults | SIRS | INSEE | MINI |
| Zhang et al., 2018/2019 | China | Hong Kong | Social-ecological model | Cross-sectional | 909 age 65+ adults | Active Lifestyle and the Environment in Chinese Seniors Project | Census and Statistics, Lands, and Planning Department of HKSAR | GDS |
3.4. Neighborhood Attributes and Geographical Unit
3.5. Use of Geographic Information Systems
3.6. Association of Neighborhood Attributes with Mental Health Outcomes
4. Discussion
4.1. Use of GIS in Measuring Neighborhood
4.2. GIS-Derived Measurements
4.3. Neighborhood Definitions
4.4. Effects of GIS-Derived Neighborhood Attributes on Mental Health
4.5. Strength and Limitations
4.6. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
- exp Geographic Information Systems/
- (geographic* information system* or GIS or geospatial or spatial analysis).mp.
- 1 or 2
- exp Mental Health/
- exp Mental Disorders/
- exp Mental Health Services/
- exp Hospitals, Psychiatric/
- (mental health or depress* or distress “psychological distress”).mp.
- 4 or 5 or 6 or 7 or 8
- 3 and 9
- Limit 10 to (all journals and english language)
- (TITLE-ABS-KEY (“GIS” OR “geographic Information system” OR “geographical information system” OR “geographic information systems” OR geospatial OR “spatial analysis”) AND TITLE-ABS-KEY (mental AND health AND OR depress* OR distress OR “psychological distress”)) AND (LIMIT-TO (LANGUAGE, “English”))
- Additional limit article
- AB (“geographic information system” OR gis OR “geographical information system” OR (“geographic information systems” OR “geographical information systems” OR geospatial OR “spatial analysis”) AND AB (mental health OR depress* OR “psychological distress”)
- Limit English and limit research article
- ((((GIS OR “geographic information system” OR “geographical information system” OR “geographic information systems” OR “geographical information systems” OR geospatial OR “spatial analysis”) WN ALL) AND ((“mental health” OR depress* OR “psychological distress”) WN ALL))) AND ({english} WN LA))
- Limit journal article
References
- Rehm, J.; Shield, K.D. Global Burden of Disease and the Impact of Mental and Addictive Disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef]
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [Green Version]
- Larson, S.L.; Owens, P.L.; Ford, D.; Eaton, W. Depressive Disorder, Dysthymia, and Risk of Stroke. Stroke 2001, 32, 1979–1983. [Google Scholar] [CrossRef] [Green Version]
- Penninx, B.W.; Beekman, A.T.; Honig, A.; Deeg, D.J.; Schoevers, R.A.; Van Eijk, J.T.; Van Tilburg, W. Depression and cardiac mortality: Results from a community-based longitudinal study. Arch. Gen. Psychiatry. 2001, 58, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wu, X.; Lai, W.; Long, E.; Zhang, X.; Li, W.; Zhu, Y.; Chen, C.; Zhong, X.; Liu, Z.; et al. Prevalence of depression and depressive symptoms among outpatients: A systematic review and meta-analysis. BMJ Open 2017, 7, e017173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Depression. Available online: http://www.who.int/news-room/fact-sheets/detail/depression (accessed on 30 January 2020).
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Mental health: A call for action by world health ministers. In Mental Health: A Call for Action by World Health Ministers; World Health Organization: Geneva, Switzerland, 2001; Available online: https://www.mhinnovation.net/sites/default/files/downloads/resource/Mental%20Health%20A%20Call%20for%20Action%20by%20World%20Health%20Ministers.pdf (accessed on 30 January 2020).
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 13 April 2021).
- Alegría, M.; NeMoyer, A.; Bague, I.F.; Wang, Y.; Alvarez, K. Social Determinants of Mental Health: Where We Are and Where We Need to Go. Curr. Psychiatry Rep. 2018, 20, 95. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.E.; Rubin, V. Why Place Matters: Building a Movement for Healthy Communities. PolicyLink. Available online: https://www.policylink.org/sites/default/files/WHYPLACEMATTERS_FINAL.PDF (accessed on 30 January 2020).
- Curtis, S. Space, Place and Mental Health; Ashgate Publishing Ltd.: Farnham, UK, 2010. [Google Scholar]
- Glass, T.A.; Balfour, J.L. Neighborhoods, aging, and functional limitations. Health Place 2003, 1, 303–334. [Google Scholar]
- Maas, J.; Verheij, R.A.; De Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Age-friendly Cities: A Guide. Available online: https://www.who.int/ageing/publications/Global_age_friendly_cities_Guide_English.pdf (accessed on 23 April 2020).
- Silver, E.; Mulvey, E.P.; Swanson, J.W. Neighborhood structural characteristics and mental disorder: Faris and Dunham revisited. Soc. Sci. Med. 2002, 55, 1457–1470. [Google Scholar] [CrossRef]
- Mair, C.; Roux, A.V.D.; Galea, S. Are Neighborhood Characteristics Associated with Depressive Symptoms? A Critical Review. J. Community Health 2008, 62, 940–946. [Google Scholar] [CrossRef]
- Gong, Y.; Palmer, S.; Gallacher, J.; Marsden, T.; Fone, D. A systematic review of the relationship between objective measurements of the urban environment and psychological distress. Environ. Int. 2016, 96, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Julien, D.; Richard, L.; Gauvin, L.; Kestens, Y. Neighborhood characteristics and depressive mood among older adults: An integrative review. Int. Psychogeriatr. 2012, 24, 1207–1225. [Google Scholar] [CrossRef] [Green Version]
- Barnett, A.; Zhang, C.J.; Johnston, J.M.; Cerin, E. Relationships between the neighborhood environment and depression in older adults: A systematic review and meta-analysis. Int. Psychogeriatr. 2018, 30, 1153–1176. [Google Scholar] [CrossRef]
- Cromley, E.K.; McLafferty, S.L. GIS and Public Health; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Francis, J.; Wood, L.; Knuiman, M.; Giles-Corti, B. Quality or quantity? Exploring the relationship between Public Open Space attributes and mental health in Perth, Western Australia. Soc. Sci. Med. 2012, 74, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Ivey, S.L.; Kealey, M.; Kurtovich, E.; Hunter, R.H.; Prohaska, T.R.; Bayles, C.M.; Satariano, W.A. Neighborhood characteristics and depressive symptoms in an older population. Aging Ment. Health 2014, 19, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Koohsari, M.J.; Badland, H.; Mavoa, S.; Villanueva, K.; Francis, J.; Hooper, P.; Owen, N.; Giles-Corti, B. Are public open space attributes associated with walking and depression? Cities 2018, 74, 119–125. [Google Scholar] [CrossRef]
- Zhang, C.; Barnett, A.; Sit, C.H.P.; Lai, P.; Johnston, J.M.; Lee, R.S.Y.; Cerin, E. Cross-sectional associations of objectively assessed neighbourhood attributes with depressive symptoms in older adults of an ultra-dense urban environment: The Hong Kong ALECS study. BMJ Open 2018, 8, e020480. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.J.; Barnett, A.; Sit, C.H.; Lai, P.C.; Johnston, J.M.; Lee, R.S.; Cerin, E. To what extent does physical activity explain the associations between neighborhood environment and depressive symptoms in older adults living in an Asian metropolis? Ment. Health Phys. Act. 2019, 16, 96–104. [Google Scholar] [CrossRef]
- Galster, G. On the Nature of Neighbourhood. Urban Stud. 2001, 38, 2111–2124. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoch-Ruppen, J.; Ehlert, U.; Uggowitzer, F.; Weymerskirch, N.; La Marca-Ghaemmaghami, P. Women’s Word Use in Pregnancy: Associations With Maternal Characteristics, Prenatal Stress, and Neonatal Birth Outcome. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evdence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia; Available online: https://synthesismanual.jbi.global (accessed on 30 January 2020).
- Ambrey, C. An investigation into the synergistic wellbeing benefits of greenspace and physical activity: Moving beyond the mean. Urban For. Urban Green. 2016, 19, 7–12. [Google Scholar] [CrossRef]
- Ambrey, C. Greenspace, physical activity and well-being in Australian capital cities: How does population size moderate the relationship? Public Health 2016, 133, 38–44. [Google Scholar] [CrossRef]
- Annerstedt, M.; Östergren, P.O.; Björk, J.; Grahn, P.; Skärbäck, E.; Währborg, P. Green qualities in the neighbourhood and mental health–results from a longitudinal cohort study in Southern Sweden. BMC Public Health 2012, 12, 337. [Google Scholar] [CrossRef] [Green Version]
- Bosch, M.A.V.D.; Östergren, P.-O.; Grahn, P.; Skärbäck, E.; Währborg, P. Moving to Serene Nature May Prevent Poor Mental Health—Results from a Swedish Longitudinal Cohort Study. Int. J. Environ. Res. Public Health 2015, 12, 7974–7989. [Google Scholar] [CrossRef] [Green Version]
- Astell-Burt, T.; Feng, X.; Kolt, G. Mental health benefits of neighbourhood green space are stronger among physically active adults in middle-to-older age: Evidence from 260,061 Australians. Prev. Med. 2013, 57, 601–606. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X. Association of Urban Green Space with Mental Health and General Health Among Adults in Australia. JAMA Netw. Open 2019, 2, e198209. [Google Scholar] [CrossRef] [Green Version]
- Mayne, D.J.; Morgan, G.G.; Jalaludin, B.B.; Bauman, A.E. Does Walkability Contribute to Geographic Variation in Psychosocial Distress? A Spatial Analysis of 91,142 Members of the 45 and Up Study in Sydney, Australia. Int. J. Environ. Res. Public Health 2018, 15, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, A.; Vandormael, A.; Cuadros, D.; Di Minin, E.; Heikinheimo, V.; Tanser, F.; Slotow, R.; Burns, J.K. Green environment and incident depression in South Africa: A geospatial analysis and mental health implications in a resource-limited setting. Lancet Planet. Health 2017, 1, e152–e162. [Google Scholar] [CrossRef]
- Tomita, A.; Vandormael, A.; Cuadros, D.; Slotow, R.; Tanser, F.; Burns, J.K. Proximity to healthcare clinic and depression risk in South Africa: Geospatial evidence from a nationally representative longitudinal study. Soc. Psychiatry Psychiatr. Epidemiology 2017, 52, 1023–1030. [Google Scholar] [CrossRef]
- Schootman, M.; Andresen, E.M.; Wolinsky, F.; Malmstrom, T.K.; Miller, J.P.; Miller, D.K. Neighbourhood environment and the incidence of depressive symptoms among middle-aged African Americans. J. Epidemiology Community Health 2007, 61, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Saarloos, D.; Alfonso, H.; Giles-Corti, B.; Middleton, N.; Almeida, O. The Built Environment and Depression in Later Life: The Health In Men Study. Am. J. Geriatr. Psychiatry 2011, 19, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, C.; Gallacher, J.; Webster, C. Urban built environment configuration and psychological distress in older men: Results from the Caerphilly study. BMC Public Health 2013, 13, 695. [Google Scholar] [CrossRef] [Green Version]
- Cromley, E.K.; Wilson-Genderson, M.; Pruchno, R.A. Neighborhood characteristics and depressive symptoms of older people: Local spatial analyses. Soc. Sci. Med. 2012, 75, 2307–2316. [Google Scholar] [CrossRef]
- Traoré, M.; Vuillermoz, C.; Chauvin, P.; Deguen, S. Influence of Individual and Contextual Perceptions and of Multiple Neighborhoods on Depression. Int. J. Environ. Res. Public Health 2020, 17, 1958. [Google Scholar] [CrossRef] [Green Version]
- Noordzij, J.M.; A Beenackers, M.; Groeniger, J.O.; Van Lenthe, F.J. Effect of changes in green spaces on mental health in older adults: A fixed effects analysis. J. Epidemiol. Community Health 2019, 74, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gariepy, G.; Kaufman, J.; Blair, A.; Kestens, Y.; Schmitz, N. Place and health in diabetes: The neighbourhood environment and risk of depression in adults with Type 2 diabetes. Diabet. Med. 2015, 32, 944–950. [Google Scholar] [CrossRef]
- Thomas, H.; Weaver, N.; Patterson, J.; Jones, P.; Bell, T.; Playle, R.; Dunstan, F.; Palmer, S.; Lewis, G.; Araya, R. Mental health and quality of residential environment. Br. J. Psychiatry 2007, 191, 500–505. [Google Scholar] [CrossRef] [Green Version]
- Su, J.G.; Dadvand, P.; Nieuwenhuijsen, M.; Bartoll, X.; Jerrett, M. Associations of green space metrics with health and behavior outcomes at different buffer sizes and remote sensing sensor resolutions. Environ. Int. 2019, 126, 162–170. [Google Scholar] [CrossRef] [PubMed]
- DeGuzman, P.B.; Merwin, E.I.; Bourguignon, C. Population Density, Distance to Public Transportation, and Health of Women in Low-Income Neighborhoods. Public Heal. Nurs. 2013, 30, 70–78. [Google Scholar] [CrossRef]
- Nutsford, D.; Pearson, A.L.; Kingham, S.; Reitsma, F. Residential exposure to visible blue space (but not green space) associated with lower psychological distress in a capital city. Health Place 2016, 39, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.C.; Lau, K.K.-L.; Yu, R.; Wang, D.; Woo, J.; Kwok, T.C.Y.; Ng, E. Spatial Variability of Geriatric Depression Risk in a High-Density City: A Data-Driven Socio-Environmental Vulnerability Mapping Approach. Int. J. Environ. Res. Public Health 2017, 14, 994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Gee, G.C.; Fan, Y.; Takeuchi, D.T. Do physical neighborhood characteristics matter in predicting traffic stress and health outcomes? Transp. Res. Part F. Traffic Psychol. Behav. 2007, 10, 164–176. [Google Scholar] [CrossRef] [Green Version]
- Berke, E.M.; Gottlieb, L.M.; Moudon, A.V.; Larson, E.B. Protective Association between Neighborhood Walkability and Depression in Older Men. J. Am. Geriatr. Soc. 2007, 55, 526–533. [Google Scholar] [CrossRef]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to Neighborhood Green Space and Mental Health: Evidence from the Survey of the Health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gariépy, G.; Thombs, B.D.; Kestens, Y.; Kaufman, J.S.; Blair, A.; Schmitz, N. The Neighbourhood Built Environment and Trajectories of Depression Symptom Episodes in Adults: A Latent Class Growth Analysis. PLoS ONE 2015, 10, e0133603. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.A.; Hirsch, J.; August, C.; Mair, C.; Sanchez, B.N.; Roux, A.V.D. Neighborhood Social Resources and Depressive Symptoms: Longitudinal Results from the Multi-Ethnic Study of Atherosclerosis. J. Hered. 2016, 93, 572–588. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Berkman, L.F. (Eds.) Neighborhoods and Health; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Rantakokko, M.; Keskinen, K.E.; Kokko, K.; Portegijs, E. Nature diversity and well-being in old age. Aging Clin. Exp. Res. 2017, 30, 527–532. [Google Scholar] [CrossRef]
- Deng, Y. Challenges and complications in neighborhood mapping: From neighborhood concept to operationalization. J. Geogr. Syst. 2016, 18, 229–248. [Google Scholar] [CrossRef]
- Eisler, A.D.; Eisler, H.; Yoshida, M. Perception of human ecology: Cross-cultural and gender comparisons. J. Environ. Psychol. 2003, 23, 89–101. [Google Scholar] [CrossRef]
- Siordia, C.; Saenz, J. What is a “Neighborhood”? Definition in studies about depressive symptoms in older persons. J. Frailty Aging. 2013, 2, 153. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4573636/pdf/nihms574398.pdf (accessed on 10 July 2020). [PubMed]
- Ambrey, C.; Fleming, C. Public Greenspace and Life Satisfaction in Urban Australia. Urban Stud. 2013, 51, 1290–1321. [Google Scholar] [CrossRef]
- Blakely, T.A.; Woodward, A.J. Ecological effects in multi-level studies. J. Epidemiol. Commun. Health 2000, 54, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Author, Date | Attributes | Measurement Details | Geographical Unit |
|---|---|---|---|
| Environmental Characteristics | |||
| Ambrey, 2016a; 2016b | Green spaces |
| Census Collection District |
| Annerstedt et al., 2012; van den Bosch et al., 2015 | Green qualities |
| 300 m radial buffer |
| Astell-Burt et al., 2013 | Green spaces |
| 1 km radial buffer |
| Astell-Burt et al., 2019 | Green spaces |
| 1.6 km network buffer |
| Beyer et al., 2014 | Green spaces |
| block group |
| Gariepy et al., 2015a | Green exposure |
| 500, 1000, 1500 m radial buffers |
| Ho et al., 2017 | Vegetation |
| 400 m radial buffer |
| Noordzij et al., 2020 | Green exposure |
| 300, 500, 1000 m radial buffer |
| Rantakokko et al., 2018 | Nature diversity |
| 500 m radial buffer |
| Sakar et al., 2013 | Green exposure Slope variability |
| 500 m radial buffer 1 km network buffer |
| Song et al., 2007 | Green parkland ratio |
| block group |
| Su et al., 2019 | Greenness exposure |
| 50, 100, 250, 500 m radial buffers |
| Tomita et al., 2017a | Greenness exposure |
| 1 km resolution grid |
| Environmental Characteristics | |||
| Nutsford et al., 2016 | Visibility of green and blue spaces |
| <300 m, 300 m–3 km, 3–6 km, 6–15 km from centroids of meshblocks |
| Infrastructure Characteristics | |||
| Berke et al., 2007 | Walkability |
| 100, 500, 1000 m radial buffers |
| DeGuzman et al., 2013 | Public transportation |
| Not applicable |
| Mayne et al., 2018 | Walkability |
| Postal area |
| Saarloos et al., 2011 | Walkability |
| Census Collection District |
| Street connectivity |
| ||
| Land-use mix |
| ||
| Land-use availability |
| ||
| Sakar et al., 2013 | Physical accessibility |
| 1200, 3000, N-m |
| Street connectivity |
| 1 km network buffer | |
| Land-use configuration |
| ||
| Song et al., 2007 | Internal connectivity Major street Land-use diversity |
| block group |
| Zhang et al., 2018; 2019 | Street intersection density |
| 400, 800 m network buffers |
| Residential Characteristics | |||
| Ho et al., 2017 | Environmental measures |
| 400 m radial buffer |
| Residential Characteristics | |||
| Saarloos et al., 2011 | Residential development density |
| Census Collection District |
| Sakar et al., 2013 | Dwelling level configuration |
| 30 m kernel surrounding |
| Song et al., 2007 | Residential density |
| block group |
| Zhang et al., 2018; 2019 | Residential density |
| 400, 800 m network buffers |
| Proximity Characteristics | |||
| Francis et al., 2012 | Quantity of POS |
| 1600 m network buffer |
| Gariepy et al., 2015a | Neighborhood resources |
| 500, 1000, 1500 m radial buffers |
| Gariepy et al., 2015b | Neighborhood resources |
| 500 m radial buffer |
| Ivey et al., 2015 | Neighborhood businesses |
| 400 m radial buffer |
| Koohsari et al., 2018 | Quantity of POS |
| 200, 400, 800, 1000, 1600 m network buffers |
| Moore et al., 2016 | Social engagement destinations |
| 1 mile buffer |
| Proximity Characteristics | |||
| Thomas et al., 2007 | Geographical accessibility score |
| 1: <300 m, 300–500 m, >500 m; 2: <600 m, 600–800 m, >800 m; 3: <800 m, 800–1900 m, >1900 m; 4: <1300 m, 1300–1900 m, >1900 m |
| Tomita et al., 2017b | Primary Healthcare Clinic |
| 6 km radial buffer as a threshold |
| Zhang et al., 2018; 2019 | Neighborhood resources |
| 400, 800 m network buffers |
| Social and Demographic Characteristics | |||
| Cromley et al., 2012 | Poverty Residential stability |
| census tract |
| Crime |
| ||
| DeGuzman et al., 2013 | Residential density |
| block group |
| Gariepy et al., 2015a | Neighborhood deprivation |
| census block |
| Ivey et al., 2015 | Neighborhood socioeconomic status |
| census tract |
| Sakar et al., 2013 | Area-level deprivation |
| Lower Super Output Area |
| Shootman et al., 2007 | Deprivation index |
| census tract, block group |
| Song et al., 2007 | Neighborhood poverty Vehicle burden |
| block group |
| Social and Demographic Characteristics | |||
| Traoré et al., 2020 | Income level |
| residential census block, workplace census block, frequented census block |
| Cumulative exposure to deprivation | Group 1: Poor neighborhoods only Group 2: Wealthy neighborhoods only Group 3: Neighborhoods of different types | ||
| Data Acquisition | Data Preprocessing | Data Analysis | Data Presentation | |||
|---|---|---|---|---|---|---|
| Neighborhood | Measurement | |||||
| Neighborhood Attribute | Neighborhood Unit | Participant | ||||
| Ambrey (2016a) | topological data | area | admin | admin | ||
| Ambrey (2016b) | topological data; admin data | area | admin | admin | ||
| Annerstedt et al., (2012) | topological data | area | buffering (radial) | geocoding | ||
| Astell-Burt et al., (2013) | topological data | area | buffering (radial) | centroid (meshblock) | mapping: neighborhood attribute | |
| Astell-Burt et al., (2019) | line data; image data | area | buffering (network) | centroid (meshblock) | ||
| Berke et al., (2007) | point, line data | buffering (radial) | geocoding | mapping: neighborhood attribute | ||
| Beyer et al., (2014) | topological data; image data | area | admin | geocoded (address) | mapping: neighborhood attribute | |
| Cromley et al., (2012) | admin data | admin | admin | exploratory data analysis, global/local spatial autocorrelation, geostatistic, spatial weights | mapping: estimate | |
| DeGuzman et al., (2013) | point data; admin data | distance | admin | centroid (block group) | ||
| Francis et al., (2012) | point, line data | volume | buffering (network) | geocoding | ||
| Gariepy et al., (2015a) | image data; point, line data; admin data | area, volume, length | buffering (radial) | centroid (postal code) | ||
| Gariepy et al., (2015b) | point data | volume | buffering (radial) | centroid (postal code) | ||
| Ho et al., (2017) | image data;admin data | area | buffering (radial) | geocoding | exploratory data analysis | mapping: estimate |
| Ivey et al., (2015) | point data; admin data | volume | buffering (radial) | geocoding | ||
| Koohasari et al., (2018) | point, line, polygon data | distance, volume | buffering (network) | geocoding | ||
| Mayne et al., (2018) | topological data;line data | volume | geocoded (statistical division/postal code) | exploratory data analysis | mapping: estimate | |
| Moore et al., (2016) | point data | volume | buffering (radial) | geocoding | ||
| Noordzij et al., (2020) | topological data | distance, volume | buffering (radial) | geocoding | mapping: neighborhood attribute | |
| Nutsford et al., (2016) | topological data | area | centroid (meshblock) | mapping: neighborhood attribute | ||
| Rantakokko et al., (2018) | topological data | area | buffering (radial) | geocoding | ||
| Saarloos et al., (2011) | point, line data; admin data | volume, length | geocoded (statistical division) | |||
| Sakar et al., (2013) | topological data;image data; point, line data;admin data | area, volume, distance | buffering (radial and network) | geocoding | exploratory data analysis | mapping: estimate |
| Schootman et al., (2007) | admin data | geocoded (statistical division) | ||||
| Song et al., (2007) | point, line, polygon data; admin data | area, volume, length | geocoded (statistical division) | |||
| Su et al., (2019) | image data | area | buffering (radial) | geocoding | mapping: study location, comparison of datasets | |
| Tomas et al., (2007) | point data | distance | admin | |||
| Tomita et al., (2017a) | image data | area | GPS coordinate (household) | |||
| Tomita et al., (2017b) | point data | distance | GPS coordinate (household) | mapping: neighborhood attribute | ||
| Traoré et al., (2020) | admin data | geocoded (statistical division) | mapping; outcome attribute | |||
| van den Bosch et al., (2015) | topological data | area | buffering (radial) | geocoding | mapping: neighborhood attribute | |
| Zhang et al., (2018) | point, line data; admin data | volume | buffering (network) | geocoding | ||
| Zhang et al., (2019) | point, line data; admin data | volume | buffering (network) | geocoding | ||
| Neighborhood Attribute | Psychological Distress | Depressive Symptoms | |||
|---|---|---|---|---|---|
| # Studies | # Studies with Significant Effect (Moderating Effect) | # Studies | # Studies with Significant Effect (Moderating Effect) | ||
| Residential | Average building height | -- | -- | 1 | 1 |
| Dwelling level configuration | 1 | (1) | -- | -- | |
| % Residential area | -- | -- | 1 | 1 | |
| Residential development density | -- | -- | -- | -- | |
| Residential density | -- | -- | 3 | 0 | |
| Variation of building height | -- | -- | 1 | 1 | |
| Infrastructure | Accessibility of streets | 1 | (1) | -- | -- |
| Distance to public transportation | 1 | 0 | -- | -- | |
| Internal connectivity | -- | -- | 1 | 0 | |
| Land-use availability | -- | -- | 1 | (1) | |
| Land-use configuration | 1 | (1) | 1 | 1 | |
| Land-use mix | 1 | (1) | 1 | 1 | |
| Land-use diversity | -- | -- | 1 | 0 | |
| Major street | -- | -- | 1 | (1) | |
| Street connectivity | 1 | 0 | 1 | 0 | |
| Street intersection density | -- | --- | 2 | 0 | |
| Walkability | 1 | 0 | 2 | (1) | |
| Sociodemographic | Cumulative exposure to deprivation | -- | -- | 1 | -- |
| Neighborhood deprivation | 1 | (1) | 3 | (1) | |
| Neighborhood poverty | -- | -- | 2 | 1 | |
| Neighborhood socioeconomic status | -- | -- | 1 | 0 | |
| Residential income level | -- | -- | 1 | -- | |
| Residential density (population) | 1 | 0 | -- | -- | |
| Residential stability (population) | -- | -- | 1 | 1 | |
| Vehicle burden | -- | -- | 1 | (1) | |
| Public services | Crime | -- | -- | 1 | 1 |
| Distance to nearest public open space | -- | -- | 1 | 0 | |
| Size of nearest public open space | -- | -- | 1 | 0 | |
| Total number of public open spaces | 1 | 0 | 1 | 0 | |
| Total size of public open spaces | 1 | 0 | 1 | 0 | |
| Environmental | Access to green qualities | 2 | (2) | -- | -- |
| Blue space visibility | 1 | 1 | -- | -- | |
| Green exposure (NDVI) | 2 | 1 | 4 | 1 (1) | |
| Green space visibility | 1 | 0 | -- | -- | |
| Green parkland ratio | -- | -- | 1 | (1) | |
| Nature diversity | -- | -- | 1 | 0 | |
| Nearest green space | -- | -- | 1 | 1 | |
| Nearest green or blue space | -- | -- | 1 | 1 | |
| Nearest green or agricultural space | -- | -- | 1 | 1 | |
| Nearest green, blue or agricultural space | -- | -- | 1 | 1 | |
| Slope variability | 1 | 1 | -- | -- | |
| % grass | 1 | (1) | -- | -- | |
| % green spaces | 3 | (2) | 1 | 1 | |
| % low-lying vegetation | 1 | 0 | -- | -- | |
| % tree canopy | 1 | 1 | 1 | 1 | |
| Neighborhood resources | Density of businesses | -- | -- | 1 | 0 |
| Geographical accessibility score | 1 | 0 | -- | -- | |
| Neighborhood resources | -- | -- | 2 | (2) | |
| Proximity to nearest PHCC | -- | -- | 1 | 1 | |
| Social engagement destinations | -- | -- | 1 | (1) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.-S.; McMorris, B.J.; Pruinelli, L.; Song, Y.; Kaas, M.J.; Wyman, J.F. Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8597. https://doi.org/10.3390/ijerph18168597
Park Y-S, McMorris BJ, Pruinelli L, Song Y, Kaas MJ, Wyman JF. Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8597. https://doi.org/10.3390/ijerph18168597
Chicago/Turabian StylePark, Young-Shin, Barbara J. McMorris, Lisiane Pruinelli, Ying Song, Merrie J. Kaas, and Jean F. Wyman. 2021. "Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8597. https://doi.org/10.3390/ijerph18168597
APA StylePark, Y.-S., McMorris, B. J., Pruinelli, L., Song, Y., Kaas, M. J., & Wyman, J. F. (2021). Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review. International Journal of Environmental Research and Public Health, 18(16), 8597. https://doi.org/10.3390/ijerph18168597