
Conservative and Surgical Treatment of Talar Fractures: A Systematic Review and Meta-Analysis on Clinical Outcomes and Complications

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
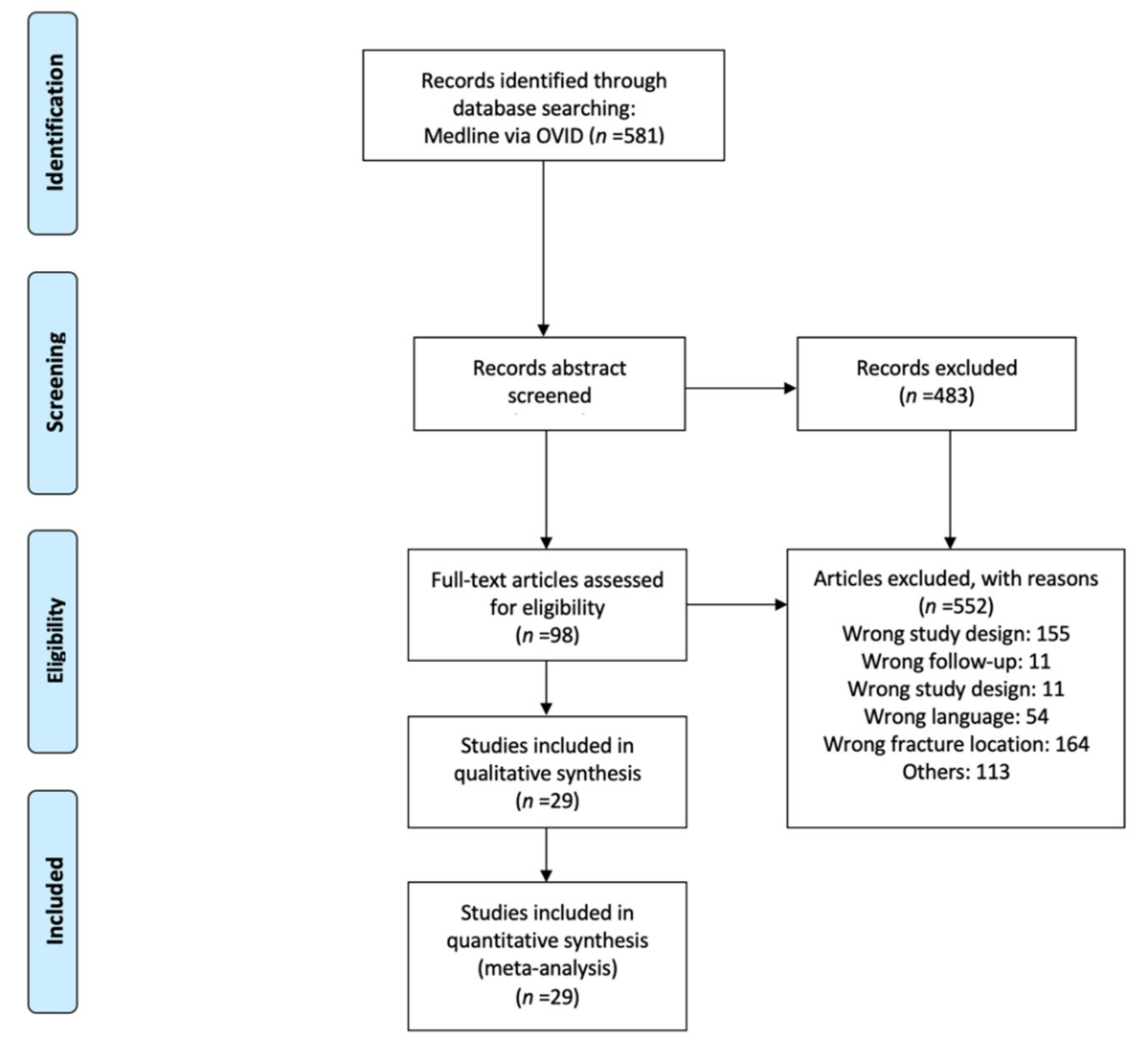
2.1. Study Selection
- 1.
- Reviews/meta-analysis
- 2.
- Case reports
- 3.
- Fractures not involving the talar body, neck, or head
- 4.
- Non-human studies
- 5.
- Non-German or English studies
- 6.
- Follow-up under six months
2.2. Data Extraction and Organization
- 1.
- Name of the author(s), name of the journal, year of publication, study type, level of evidence
- 2.
- Fracture localization (neck, body, head)
- 3.
- Number of patients and the examined talus fractures stratified by fracture location
- 4.
- Epidemiological data (age, sex)
- 5.
- Follow-up in months (average and range)
- 6.
- Number of patients in follow-up/dropouts
- 7.
- Number of patients with open fractures
- 8.
- Number of patients treated surgically
- 9.
- Time until surgery in days
- 10.
- Postoperative readjustment of the fractures (postoperative reduction)
- 11.
- Poor or no fracture healing (malunion/non-union)
- 12.
- Type of surgical treatment
- 13.
- Frequency of early complications
- 14.
- Fracture classification
- 15.
- Number of patients with the respective degree of fracture severity, according to classification
- 16.
- Treatment result (result of the specific outcome scores)
- 17.
- Complications (AVN, osteoarthritis)
- 18.
- Frequency of joint stiffening (arthrodesis)
2.3. Assessment of the Methodological Quality of Included Studies
2.4. Statistics
3. Results
3.1. Study Characteristics and Qualitative Outcome Assessment
3.2. Assessment of the Methodological Quality
3.3. Quantitative Analysis
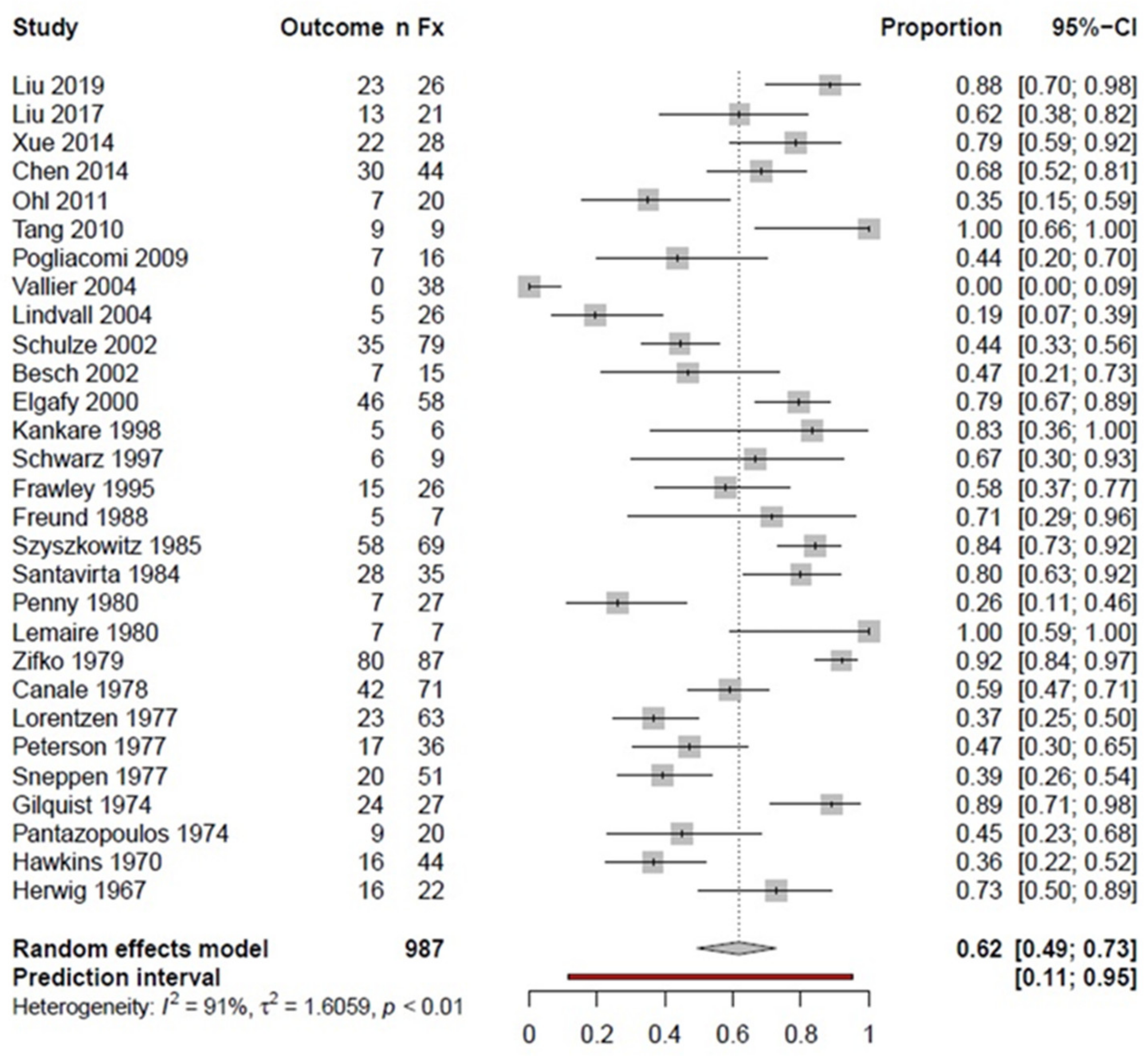
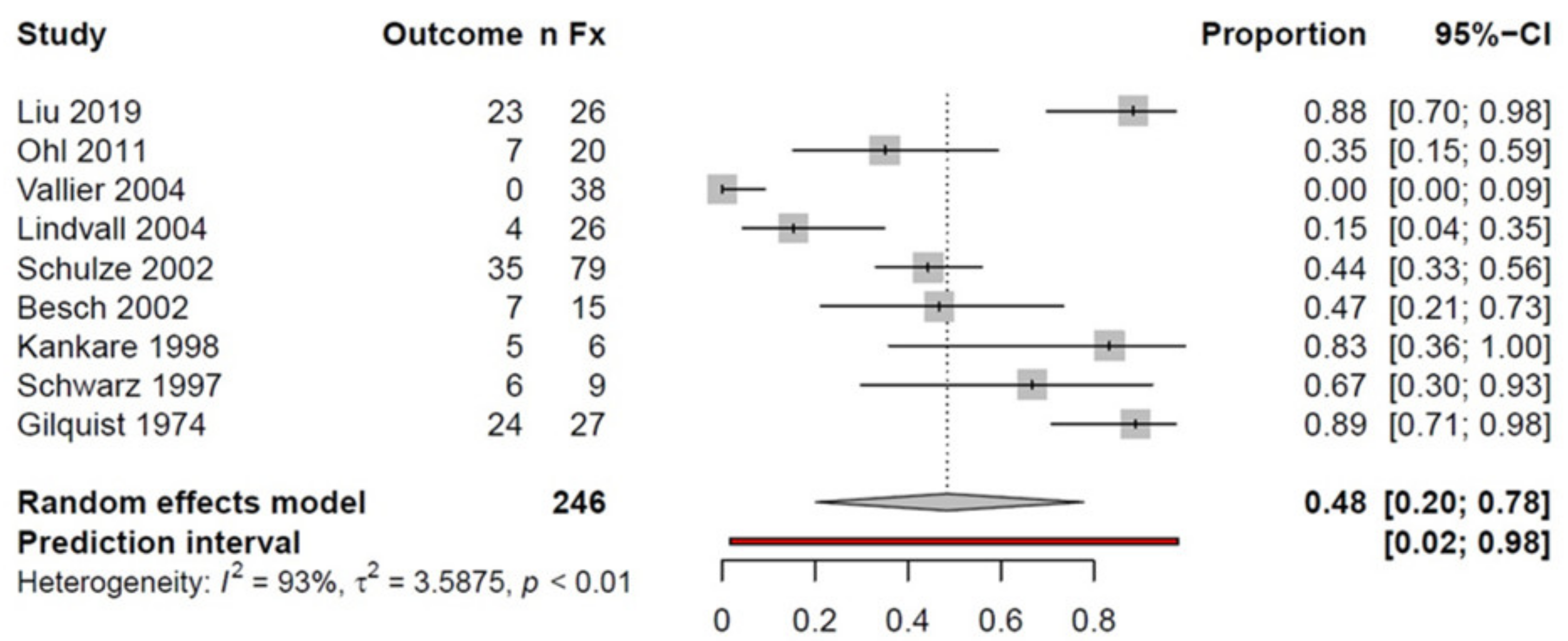
3.3.1. Success Rates
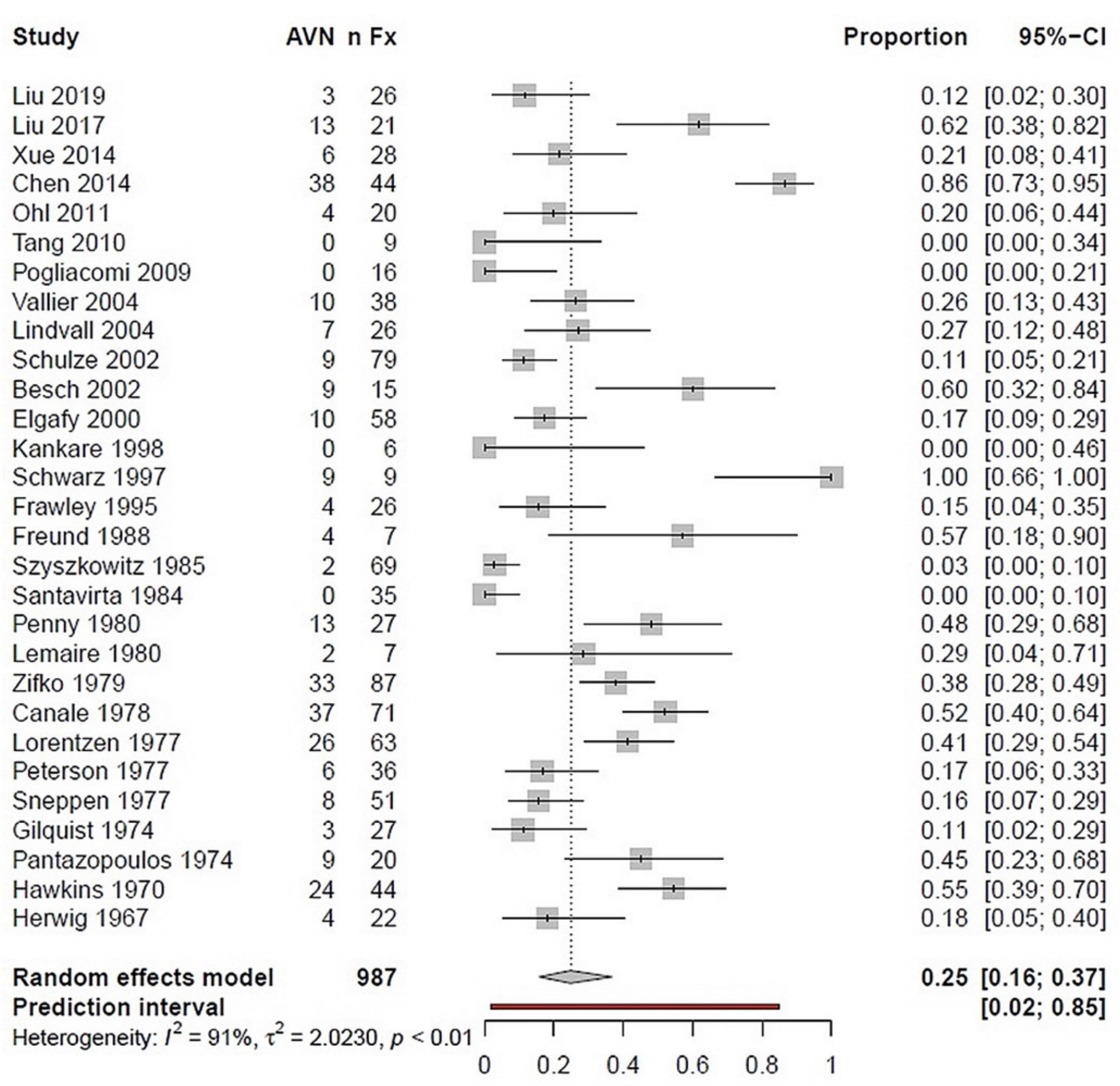
3.3.2. Complication Rate
4. Discussion
4.1. Pooled Talar Fractures
4.2. Talar Neck Fractures
4.3. Fracture Severity
4.4. Complications
4.5. Strengths and Limitations
4.6. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuner, E.H.; Lindenmaier, H.L. Zur Behandlung Der Talusfraktur. Unfallchirurgie 1983, 9, 35–40. [Google Scholar] [CrossRef]
- Richter, M.; Zech, S. Behandlung der Talusfraktur. OP J. 2007, 23, 104–109. [Google Scholar] [CrossRef][Green Version]
- Zwipp, H.; Rammelt, S. Posttraumatische Korrekturoperationen am Fuß. Zent. Chir 2003, 128, 218–226. [Google Scholar] [CrossRef]
- Hawkins, L.G. Fractures of the Neck of the Talus. J. Bone Jt. Surg. Am. 1970, 52, 991–1002. [Google Scholar] [CrossRef]
- Zwipp, H. Chirurgie des Fußes; Springer: Vienna, Hungary, 1994; ISBN 978-3-7091-7366-4. [Google Scholar]
- Canale, S.T.; Kelly, F.B. Fractures of the Neck of the Talus. Long-Term Evaluation of Seventy-One Cases. J. Bone Jt. Surg. Am. 1978, 60, 143–156. [Google Scholar] [CrossRef]
- Pennal, G.F. Fractures of the Talus. Clin. Orthop. Relat. Res. 1963, 30, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Berndt, A.L.; Harty, M. Transchondral Fractures (Osteochondritis Dissecans) of the Talus. J. Bone Jt. Surg. Am. 1959, 41-A, 988–1020. [Google Scholar] [CrossRef]
- Gregory, P.; DiPasquale, T.; Herscovici, D.; Sanders, R. Ipsilateral Fractures of the Talus and Calcaneus. Foot Ankle Int. 1996, 17, 701–705. [Google Scholar] [CrossRef]
- Sanders, D.W.; Busam, M.; Hattwick, E.; Edwards, J.R.; McAndrew, M.P.; Johnson, K.D. Functional Outcomes Following Displaced Talar Neck Fractures. J. Orthop. Trauma 2004, 18, 265–270. [Google Scholar] [CrossRef]
- Metzger, M.J.; Levin, J.S.; Clancy, J.T. Talar Neck Fractures and Rates of Avascular Necrosis. J. Foot Ankle Surg. 1999, 38, 154–162. [Google Scholar] [CrossRef]
- Rammelt, S.; Zwipp, H. Talar Neck and Body Fractures. Injury 2009, 40, 120–135. [Google Scholar] [CrossRef]
- Isay, M.; Wolvius, R.; Ochsner, P.E. Long-term results of talus fractures. Z Unf. Versicher. 1992, 85, 12–18. [Google Scholar]
- Adelaar, R.S. The Treatment of Complex Fractures of the Talus. Orthop. Clin. N. Am. 1989, 20, 691–707. [Google Scholar]
- Tscherne, H. Major Fractures of the Pilon, the Talus, and the Calcaneus Current Concepts of Treatment; Springer: Berlin, Germany, 1993; ISBN 978-3-642-77729-5. [Google Scholar]
- Lindvall, E.; Haidukewych, G.; DiPasquale, T.; Herscovici, D.; Sanders, R. Open Reduction and Stable Fixation of Isolated, Displaced Talar Neck and Body Fractures. J. Bone Jt. Surg. Am. 2004, 86, 2229–2234. [Google Scholar] [CrossRef]
- Vallier, H.A.; Nork, S.E.; Benirschke, S.K.; Sangeorzan, B.J. Surgical Treatment of Talar Body Fractures. J. Bone Jt. Surg. Am. 2004, 86-A Suppl. 1, 180–192. [Google Scholar] [CrossRef]
- Schulze, W.; Richter, J.; Russe, O.; Ingelfinger, P.; Muhr, G. Surgical Treatment of Talus Fractures: A Retrospective Study of 80 Cases Followed for 1-15 Years. Acta Orthop. Scand. 2002, 73, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Kundel, K.; Braun, W.; Scherer, A. Late results of central talus injuries. Unfallchirurg 1995, 98, 124–129. [Google Scholar] [PubMed]
- Daniels, T.R.; Smith, J.W.; Ross, T.I. Varus Malalignment of the Talar Neck. Its Effect on the Position of the Foot and on Subtalar Motion. J. Bone Jt. Surg. Am. 1996, 78, 1559–1567. [Google Scholar] [CrossRef]
- Rammelt, S.; Winkler, J.; Grass, R.; Zwipp, H. Reconstruction after Talar Fractures. Foot Ankle Clin. 2006, 11, 61–84. [Google Scholar] [CrossRef] [PubMed]
- Sangeorzan, B.J.; Wagner, U.A.; Harrington, R.M.; Tencer, A.F. Contact Characteristics of the Subtalar Joint: The Effect of Talar Neck Misalignment. J. Orthop. Res. 1992, 10, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Elgafy, H.; Ebraheim, N.A.; Tile, M.; Stephen, D.; Kase, J. Fractures of the Talus: Experience of Two Level 1 Trauma Centers. Foot Ankle Int. 2000, 21, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Rammelt, S.; Grass, R.; Brenner, P.; Zwipp, H. Septische Talusnekrose nach drittgradig offener Talusfraktur im Rahmen eines komplexen Fußtraumas (floating talus). Trauma Berufskrankh 2001, 3, S230–S235. [Google Scholar] [CrossRef]
- Rzesacz, E.H.; Culemann, U.; Illgner, A.; Reilmann, H. Der Homologe Talusersatz Nach Talektomie Bei Infekt Und Septischer Talusnekrose. Der. Unf. 1997, 100, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.R.; Jacobs, B.; Campbell, R.D. Fractures of the Talus. J. Trauma 1966, 6, 443–468. [Google Scholar] [CrossRef] [PubMed]
- Kenwright, J.; Taylor, R.G. Major injuries of the talus. J. Bone Jt. Surgery Br. Vol. 1970, 52-B, 36–48. [Google Scholar] [CrossRef]
- Lorentzen, J.E.; Christensen, S.B.; Krogsoe, O.; Sneppen, O. Fractures of the Neck of the Talus. Acta Orthop. Scand. 1977, 48, 115–120. [Google Scholar] [CrossRef]
- Penny, J.N.; Davis, L.A. Fractures and Fracture-Dislocations of the Neck of the Talus. J. Trauma 1980, 20, 1029–1037. [Google Scholar] [CrossRef]
- Baumhauer, J.F.; Alvarez, R.G. Controversies in Treating Talus Fractures. Orthop. Clin. N. Am. 1995, 26, 335–351. [Google Scholar] [CrossRef]
- Fortin, P.T.; Balazsy, J.E. Talus Fractures: Evaluation and Treatment. J. Am. Acad. Orthop. Surg. 2001, 9, 114–127. [Google Scholar] [CrossRef]
- Wirth, C.J. Fuß; Georg Thieme Verlag: Stuttgart, Germany, 2002; ISBN 978-3-13-126241-7. [Google Scholar]
- Halvorson, J.J.; Winter, S.B.; Teasdall, R.D.; Scott, A.T. Talar Neck Fractures: A Systematic Review of the Literature. J. Foot Ankle Surg. 2013, 52, 56–61. [Google Scholar] [CrossRef]
- Patel, R.; Van Bergeyk, A.; Pinney, S. Are Displaced Talar Neck Fractures Surgical Emergencies? A Survey of Orthopaedic Trauma Experts. Foot Ankle Int. 2005, 26, 378–381. [Google Scholar] [CrossRef]
- Sneppen, O.; Christensen, S.B.; Krogsoe, O.; Lorentzen, J. Fracture of the Body of the Talus. Acta Orthop. Scand. 1977, 48, 317–324. [Google Scholar] [CrossRef]
- Dodd, A.; Lefaivre, K.A. Outcomes of Talar Neck Fractures: A Systematic Review and Meta-Analysis. J. Orthop. Trauma 2015, 29, 210–215. [Google Scholar] [CrossRef]
- Leonetti, D.; Di Matteo, B.; Barca, P.; Cialdella, S.; Traina, F.; Arcidiacono, M.; Kon, E.; Tigani, D. Complications after Displaced Talar Neck Fracture: Results from a Case Series and a Critical Review of Literature. TOORTHJ 2018, 12, 567–575. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Jordan, R.; Lotfi, N.; Chapman, A.W.P. Talar Head Fracture: A Case Report, Systematic Review and Suggested Algorithm of Treatment. Foot 2015, 25, 258–264. [Google Scholar] [CrossRef] [PubMed]
- PRISMA-P Group; Mohar, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of Surgical Outcome after Patellar Tendinopathy: Clinical Significance of Methodological Deficiencies and Guidelines for Future Studies. Victorian Institute of Sport Tendon Study Group. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.G.; Swiontkowski, M.F.; Heckman, J.D. Introducing Levels of Evidence to the Journal. J. Bone Jt. Surg. Am. 2003, 85, 1–3. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously Misleading Results Using Inverse of Freeman-Tukey Double Arcsine Transformation in Meta-Analysis of Single Proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef]
- Besch, L.; Drost, J.; Egbers, H.-J. Die Behandlung der seltenen Talusluxationsfrakturen Analyse von 23 Verletzungen: Analyse von 23 Verletzungen. Unfallchirurg 2002, 105, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, W.; Deng, L.; Song, W. The Prognostic Value of the Hawkins Sign and Diagnostic Value of MRI after Talar Neck Fractures. Foot Ankle Int. 2014, 35, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Frawley, P.A.; Hart, J.A.L.; Young, D.A. Treatment Outcome of Major Fractures of the Talus. Foot Ankle Int. 1995, 16, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Freund, K.G. Complicated Fractures of the Neck of the Talus. Foot Ankle 1988, 8, 203–207. [Google Scholar] [CrossRef]
- Gilquist, J.; Oretop, N.; Stenström, A.; Rieger, A.; Wennberg, E. Late Results after Vertical Fracture of the Talus. Injury 1974, 6, 173–179. [Google Scholar] [CrossRef]
- Herwig, K. Treatment results of fresh talus fractures. Z Unf. Berufskr 1967, 60, 91–106. [Google Scholar]
- Kankare, J.; Rokkanen, P. Dislocated Fractures of the Talus Treated with Biodegradable Internal Fixation. Arch Orthop. Trauma Surg. 1998, 117, 62–64. [Google Scholar] [CrossRef]
- Lemaire, R.G.; Bustin, W. Screw Fixation of Fractures of the Neck of the Talus Using a Posterior Approach. J. Trauma 1980, 20, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, Z.; Zeng, W.; Xiong, Y.; Lin, Y.; Zhong, H.; Wu, J. Surgical Management of Hawkins Type III Talar Neck Fracture through the Approach of Medial Malleolar Osteotomy and Mini-Plate for Fixation. J. Orthop. Surg. Res. 2017, 12, 111. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Ge, J.; Zheng, X.; Wu, C.; Yan, Q.; Yang, H.; Zou, J. Therapeutic Efficacy Analysis of Talar Fracture Internal Fixation with Lateral Malleolar Osteotomy. Med. Sci. Monit. 2019, 25, 3463–3468. [Google Scholar] [CrossRef]
- Ohl, X.; Harisboure, A.; Hemery, X.; Dehoux, E. Long-Term Follow-up after Surgical Treatment of Talar Fractures: Twenty Cases with an Average Follow-up of 7.5 Years. Int. Orthop. 2011, 35, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Pantazopoulos, T.; Galanos, P.; Vayanos, E.; Mitsou, A.; Hartofilakidis-Garofalidis, G. Fractures of the Neck of the Talus. Acta Orthop. Scand. 1974, 45, 296–306. [Google Scholar] [CrossRef]
- Peterson, L.; Goldie, I.F.; Irstam, L. Fracture of the Neck of the Talus. A Clinical Study. Acta Orthop. Scand. 1977, 48, 696–706. [Google Scholar] [CrossRef]
- Pogliacomi, F.; De Filippo, M.; Soncini, G.; Frattini, M. Talar Fractures: Long-Term Results. Acta Biomed. 2009, 80, 219–224. [Google Scholar] [PubMed]
- Santavirta, S.; Seitsalo, S.; Kiviluoto, O.; Myllynen, P. Fractures of the Talus. J. Trauma 1984, 24, 986–989. [Google Scholar] [CrossRef]
- Schwarz, N.; Eschberger, J.; Kramer, J.; Posch, E. Radiologische Und Histologische Beobachtungen an Zentralen Talusfrakturen. Der. Unf. 1997, 100, 449–456. [Google Scholar] [CrossRef]
- Szyszkowitz, R.; Reschauer, R.; Seggl, W. Eighty-Five Talus Fractures Treated by ORIF with Five to Eight Years of Follow-up Study of 69 Patients. Clin. Orthop. Relat. Res. 1985, 199, 97–107. [Google Scholar] [CrossRef]
- Tang, H.; Han, K.; Li, M.; Zhang, Q.; Xie, Y.; Tang, X.; Xu, H.; Mao, N. Treatment of Hawkins Type II Fractures of Talar Neck by a Vascularized Cuboid Pedicle Bone Graft and Combined Internal and External Fixation: A Preliminary Report on Nine Cases. J. Trauma 2010, 69, E1–E5. [Google Scholar] [CrossRef]
- Xue, Y.; Zhang, H.; Pei, F.; Tu, C.; Song, Y.; Fang, Y.; Liu, L. Treatment of Displaced Talar Neck Fractures Using Delayed Procedures of Plate Fixation through Dual Approaches. Int. Orthop. 2014, 38, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Zifko, B.; Wittich, H. Classification and treatment results of various types of talus fractures. Hefte Unf. 1979, 134, 14–24. [Google Scholar]
- Dumont, C.; Fuchs, M.; Burchhardt, H.; Tezval, M.; Wachowski, M.; Stürmer, K. Wie sind die klinischen Ergebnisse operativ behandelter Talusfrakturen? Z Orthop Unf. 2007, 145, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Kostuj, T.; Schaper, K.; Baums, M.N.; Lieske, S. Eine Validierung des AOFAS-Ankle-Hindfoot-Scale für den deutschen Sprachraum. Fuß Sprunggelenk 2014, 12, 100–106. [Google Scholar] [CrossRef]
- Madeley, N.J.; Wing, K.J.; Topliss, C.; Penner, M.J.; Glazebrook, M.A.; Younger, A.S. Responsiveness and Validity of the SF-36, Ankle Osteoarthritis Scale, AOFAS Ankle Hindfoot Score, and Foot Function Index in End Stage Ankle Arthritis. Foot Ankle Int. 2012, 33, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.; Fortin, P.; DiPasquale, T.; Walling, A. Operative Treatment in 120 Displaced Intraarticular Calcaneal Fractures. Results Using a Prognostic Computed Tomography Scan Classification. Clin. Orthop. Relat. Res. 1993, 290, 87–95. [Google Scholar]
- Mazur, J.M.; Schwartz, E.; Simon, S.R. Ankle Arthrodesis. Long-Term Follow-up with Gait Analysis. J. Bone Jt. Surg. Am. 1979, 61, 964–975. [Google Scholar] [CrossRef]
- Alton, T.; Patton, D.J.; Gee, A.O. Classifications in Brief: The Hawkins Classification for Talus Fractures. Clin. Orthop. Relat. Res. 2015, 473, 3046–3049. [Google Scholar] [CrossRef]
- Williams, T.; Barba, N.; Noailles, T.; Steiger, V.; Pineau, V.; Carvalhana, G.; Le Jacques, B.; Clave, A.; Huten, D. Total Talar Fracture—Inter-and Intra-Observer Reproducibility of Two Classification Systems (Hawkins and AO) for Central Talar Fractures. Orthop. Traumatol. Surg. Res. 2012, 98, S56-65. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Drummond Filho, M.L.; Verzani, M.A.; Rosa, A.F.; Pimenta, C.J.; Grynwald, J.; Cliquet Junior, A. Fractures of the Neck of the Talus: Evaluation of Reproducibility of Hawkins’ Classification. Acta Ortop. Bras. 2012, 20, 170–173. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration, John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Jordan, R.K.; Bafna, K.R.; Liu, J.; Ebraheim, N.A. Complications of Talar Neck Fractures by Hawkins Classification: A Systematic Review. J. Foot Ankle Surg. 2017, 56, 817–821. [Google Scholar] [CrossRef]
- Biz, C.; Golin, N.; De Cicco, M.; Maschio, N.; Fantoni, I.; Frizziero, A.; Belluzzi, E.; Ruggieri, P. Long-Term Radiographic and Clinical-Functional Outcomes of Isolated, Displaced, Closed Talar Neck and Body Fractures Treated by ORIF: The Timing of Surgical Management. BMC Musculoskelet. Disord. 2019, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, V.J.A.; Westermann, R.; Mooers, B.; Karam, M.; Wolf, B. Timing of Surgical Reduction and Stabilization of Talus Fracture-Dislocations. Am. J. Orthop. 2017, 46, E408–E413. [Google Scholar]
- Lee, C.; Brodke, D.; Perdue, P.W.; Patel, T. Talus Fractures: Evaluation and Treatment. J. Am. Acad. Orthop. Surg. 2020, 28, e878–e887. [Google Scholar] [CrossRef] [PubMed]
- Bull, P.E.; Berlet, G.C.; Canini, C.; Hyer, C.F. Rate of Malunion Following Bi-Plane Chevron Medial Malleolar Osteotomy. Foot Ankle Int. 2016, 37, 620–626. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Step | Search Terms and Operators |
|---|---|
| 1 | Talus/ |
| 2 | Tarsal bones/ |
| 3 | exp Tarsal joints/ |
| 4 | Ankle Joint/ |
| 5 | Foot injuries/ |
| 6 | 1 or 2 or 3 or 4 or 5 |
| 7 | Fractures, Bone/ |
| 8 | 6 and 7 |
| 9 | talus.tw./ |
| 10 | 8 and 9 |
| 11 | fracture * tw./ |
| 12 | 10 and 11 |
| 13 | exp animals/not humans/ |
| 14 | 12 not 13 |
| Step | Criterion | Subcriterion | Score |
|---|---|---|---|
| Coleman Methodology Score Part A (Max. 60 points) | |||
| 1. | Study size | >60 | 10 |
| 41–60 | 7 | ||
| 20–40 | 4 | ||
| <20 or no information | 0 | ||
| 2. | Mean follow-up (in months) | >24 | 5 |
| 12–24 | 2 | ||
| <12, no information or unclear | 0 | ||
| 3. | Number of different surgeries performed for each outcome included | Only one procedure performed | 10 |
| >1 procedure performed, but used in at least 90% of patients | 7 | ||
| No information, unclear, or use of only one procedure in less than 90% of the patients included | 0 | ||
| 4. | Type of study | Randomized controlled | 15 |
| Prospective cohort | 10 | ||
| Retrospective cohort | 0 | ||
| 5. | Diagnostic certainty (use of sonography, MRI, or histopathology to confirm the diagnosis) | 100% of patients | 5 |
| >80% of patients | 3 | ||
| <80% of patients | 0 | ||
| 6. | Description of the surgical therapy procedure | Adequate (surgical technique mentioned and described in detail) | 5 |
| Moderate (surgical technique mentioned, but no detailed description) | 3 | ||
| Inadequate (surgical technique not mentioned) or unclear | 0 | ||
| 7. | Description of postoperative rehabilitation | Well-described and > 80% of patients compliant to therapy | 10 |
| Well-described and 60–80% of patients compliant to therapy | 5 | ||
| No protocol described or < 60% of patients compliant to therapy | 0 | ||
| Coleman Methodology Score Part B (Max. 40 points) | |||
| 1. | Outcome criteria (0 points are awarded in this section if the outcome criteria are not defined precisely) | Clearly defined measures for outcome | 2 |
| Follow-up examination and evaluation of the outcome clearly defined | 2 | ||
| Use of outcome criteria with good reliability | 3 | ||
| Use of outcome criteria with good sensitivity | 3 | ||
| 2. | Procedure for outcome-assessment | Patients called in for a follow-up examination | 5 |
| Examiner independent of the surgeon | 4 | ||
| Assessment is documented in writing | 3 | ||
| Completion of the assessment with minimal involvement of the examiner | 3 | ||
| 3. | Description of patient selection | Selection criteria specified and unbiased | 5 |
| Recruitment rate > 80% | 5 | ||
| Recruitment rate < 80% | 3 | ||
| Exclusion criteria clearly described or 100% recruitment rate | 5 | ||
| Author and Year | Study Design | Localization | NoFx | NoSFx | Conservative or Closed Fixation | ORIF | External Restraint | Other Primary Intervention |
|---|---|---|---|---|---|---|---|---|
| Liu 2019 | Retrospective | TN, TB | 26 | 26 | 23 | |||
| Liu 2017 | Retrospective | TN | 22 | 21 | 21 | |||
| Xue 2014 | Retrospective | TN | 31 | 22 | 9 | 22 | ||
| Chen 2014 | Retrospective | TN | 44 | 38 | 38 | |||
| Ohl 2011 | Retrospective | TN, TB | 20 | 20 | 20 | |||
| Tang 2010 | Retrospective | TN | 9 | 9 | 9 | |||
| Pogliacomi 2009 | Retrospective | TN, TB, TH | 16 | 13 | NR | |||
| Vallier 2004 | Retrospective | TN, TB | 56 | 56 | 37 | 19 | ||
| Lindvall 2004 | Retrospective | TN, TB | 26 | 26 | NR | 7 | ||
| Schulze 2002 | Retrospective | TN, TB | 80 | 80 | 67 | 1 | 12 | |
| Besch 2002 | Retrospective | TN, TB | 23 | 23 | 22 | 5 | 4 | |
| Elgafy 2000 | Retrospective | TN, TB | 60 | 48 | ||||
| Kankare 1998 | Retrospective | TN, TB | 6 | 6 | 8 | |||
| Schwarz 1997 | Retrospective | TN, TB | 19 | 9 | 5 | |||
| Frawley 1995 | Retrospective | TN, TB, TH | 28 | 20 | 20 | |||
| Freund 1988 | Retrospective | TN | 7 | 7 | 2 | 3 | 2 | |
| Szyszkowitz 1985 | Retrospective | TN, TB | 85 | 85 | 23 | 54 | 8 | |
| Santavirta 1984 | Retrospective | TN, TB, TH | 35 | 11 | 7 | 4 | ||
| Penny 1980 | Retrospective | TN | 40 | 30 | NR | 9 | ||
| Lemaire 1980 | Retrospective | TH | 7 | 7 | 7 | |||
| Zifko 1979 | Retrospective | TN, TB, TH | 137 | 24 | NR | NR | NR | |
| Canale 1978 | Retrospective | TN | 71 | 57 | NR | 25 | 11 | |
| Lorentzen 1977 E | Retrospective | TN | 123 | 20 | 33 | 14 | 2 | |
| Peterson 1977 | Retrospective | TN | 46 | 29 | 14 | 7 | 8 | |
| Sneppen 1977 | Retrospective | TN | 51 | 9 | 9 | |||
| Gilquist 1974 | Retrospective | TN, TB | 28 | 13 | 9 | 13 | ||
| Pantazopoulos 1974 | Retrospective | TN | 20 | 11 | 5 | 10 | 1 | |
| Hawkins 1970 | Retrospective | TN | 55 | 34 | 24 | 22 | ||
| Herwig 1967 | Retrospective | TN, TB, TH | 22 | 13 | 9 | 4 |
| Author | Study Year | Study Design | Level of Evidence | CMS A | CMS B | CMS Total |
|---|---|---|---|---|---|---|
| Liu | 2019 | Retrospective | 4 | 21 | 12 | 33 |
| Liu | 2017 | Retrospective | 4 | 29 | 12 | 41 |
| Xue | 2014 | Retrospective | 4 | 34 | 13 | 47 |
| Chen | 2014 | Retrospective | 3 | 24 | 12 | 36 |
| Ohl | 2011 | Retrospective | 4 | 36 | 11 | 47 |
| Tang | 2010 | Retrospective | 4 | 10 | 9 | 19 |
| Pogliacomi | 2009 | Retrospective | 4 | 17 | 10 | 27 |
| Vallier | 2004 | Retrospective | 4 | 30 | 8 | 38 |
| Lindvall | 2004 | Retrospective | 4 | 24 | 12 | 36 |
| Schulze | 2002 | Retrospective | 4 | 30 | 12 | 42 |
| Besch | 2002 | Retrospective | 3 | 24 | 10 | 34 |
| Elgafy | 2000 | Retrospective | 4 | 25 | 10 | 35 |
| Kankare | 1998 | Retrospective | 4 | 28 | 10 | 38 |
| Schwarz | 1997 | Retrospective | 4 | 26 | 10 | 36 |
| Frawley | 1995 | Retrospective | 4 | 24 | 10 | 34 |
| Freund | 1988 | Retrospective | 4 | 20 | 10 | 30 |
| Szyszkowitz | 1985 | Retrospective | 4 | 27 | 10 | 37 |
| Santavirta | 1984 | Retrospective | 4 | 9 | 10 | 19 |
| Penny | 1980 | Retrospective | 4 | 14 | 10 | 24 |
| Lemaire | 1980 | Retrospective | 4 | 22 | 10 | 32 |
| Zifko | 1979 | Retrospective | 4 | 25 | 10 | 35 |
| Canale | 1978 | Retrospective | 4 | 25 | 10 | 35 |
| Lorentzen | 1977 | Retrospective | 4 | 22 | 10 | 32 |
| Peterson | 1977 | Retrospective | 4 | 27 | 10 | 37 |
| Sneppen | 1977 | Retrospective | 4 | 22 | 10 | 32 |
| Gilquist | 1974 | Retrospective | 4 | 29 | 10 | 39 |
| Pantazopoulos | 1974 | Retrospective | 4 | 24 | 10 | 34 |
| Hawkins | 1970 | Retrospective | 4 | 22 | 10 | 32 |
| Herwig | 1967 | Retrospective | 4 | 24 | 10 | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saravi, B.; Lang, G.; Ruff, R.; Schmal, H.; Südkamp, N.; Ülkümen, S.; Zwingmann, J. Conservative and Surgical Treatment of Talar Fractures: A Systematic Review and Meta-Analysis on Clinical Outcomes and Complications. Int. J. Environ. Res. Public Health 2021, 18, 8274. https://doi.org/10.3390/ijerph18168274
Saravi B, Lang G, Ruff R, Schmal H, Südkamp N, Ülkümen S, Zwingmann J. Conservative and Surgical Treatment of Talar Fractures: A Systematic Review and Meta-Analysis on Clinical Outcomes and Complications. International Journal of Environmental Research and Public Health. 2021; 18(16):8274. https://doi.org/10.3390/ijerph18168274
Chicago/Turabian StyleSaravi, Babak, Gernot Lang, Robert Ruff, Hagen Schmal, Norbert Südkamp, Sara Ülkümen, and Jörn Zwingmann. 2021. "Conservative and Surgical Treatment of Talar Fractures: A Systematic Review and Meta-Analysis on Clinical Outcomes and Complications" International Journal of Environmental Research and Public Health 18, no. 16: 8274. https://doi.org/10.3390/ijerph18168274
APA StyleSaravi, B., Lang, G., Ruff, R., Schmal, H., Südkamp, N., Ülkümen, S., & Zwingmann, J. (2021). Conservative and Surgical Treatment of Talar Fractures: A Systematic Review and Meta-Analysis on Clinical Outcomes and Complications. International Journal of Environmental Research and Public Health, 18(16), 8274. https://doi.org/10.3390/ijerph18168274