
Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Reporting
2.2. Search Strategy
2.3. Selection Criteria
- POPULATION: professional and semi-professional male and female footballers (only 11-a-side footballers were selected in the study, not including Futsal and Gaelic Football). Amateurs were excluded due to lack of a dedicated physiotherapy staff on their football teams and the lower amount of training and playing compared to their professional counterparts.
- INTERVENTIONS: application of conservative preventive protocols, including specific training (using Static-Dynamic Stretching, targeted exercises such as the Nordic hamstring exercise or Russian hamstring curls, core stability exercises, balance training exercises, etc.), physical therapy or pre-established protocols such as the FIFA 11+ programme, which was aimed at reducing the risk of HSI.
- COMPARISONS: articles that provided data that could make possible a general comparison among the different protocols adopted and with an acceptable number of hours of exposition to training and competitions.
- OUTCOMES: studies that had at least 2 months of follow-up, monitoring players between training and competition, and that included the number of hamstring muscle injuries or the number of injuries per 1000 h (HI/1000 h) of exposure, including training and official competitions.
2.4. Exclusion Criteria
2.5. Selection Method
2.6. Quality Assessment
2.7. Risk of Bias
2.8. Statistical Analysis
3. Results
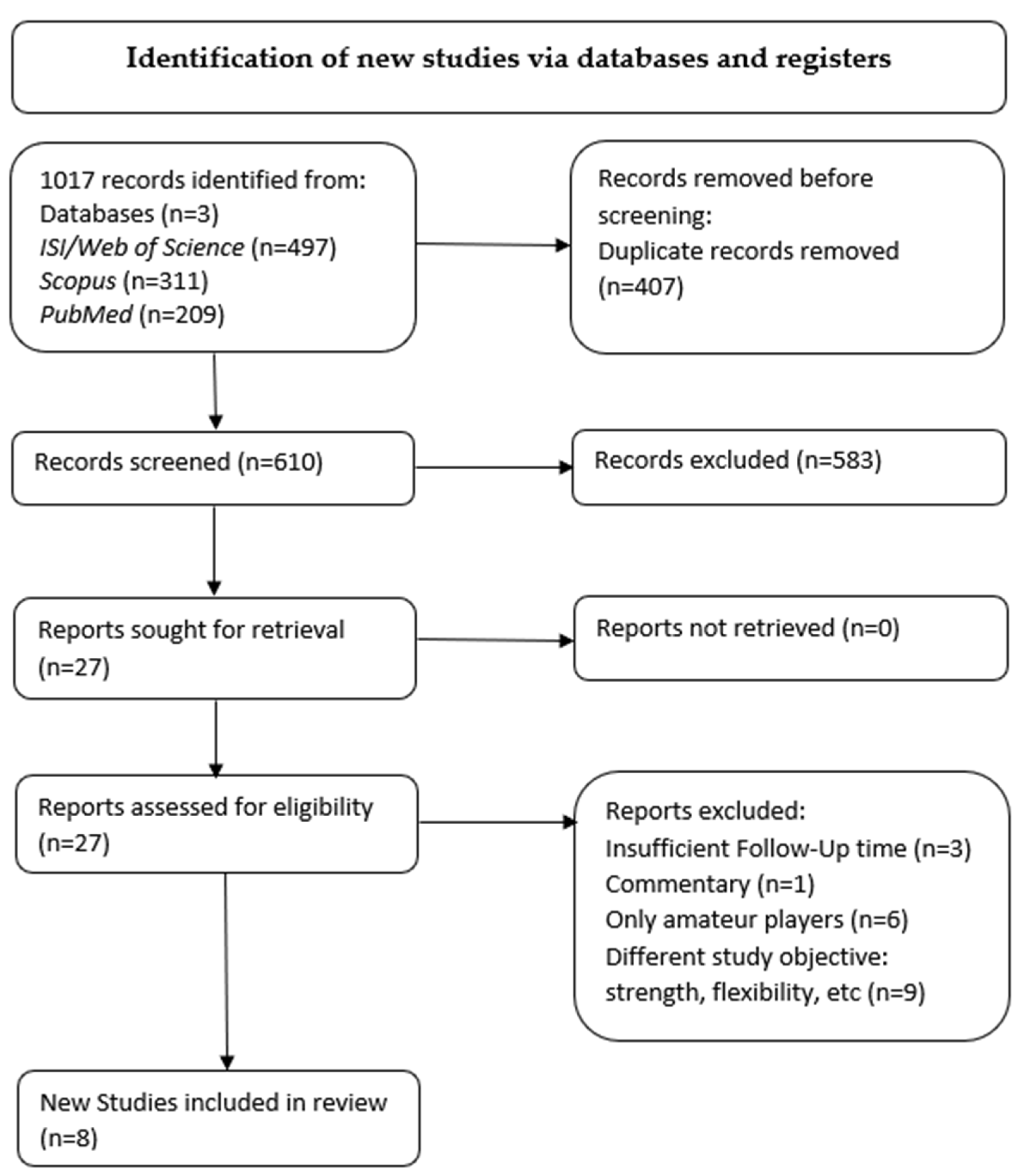
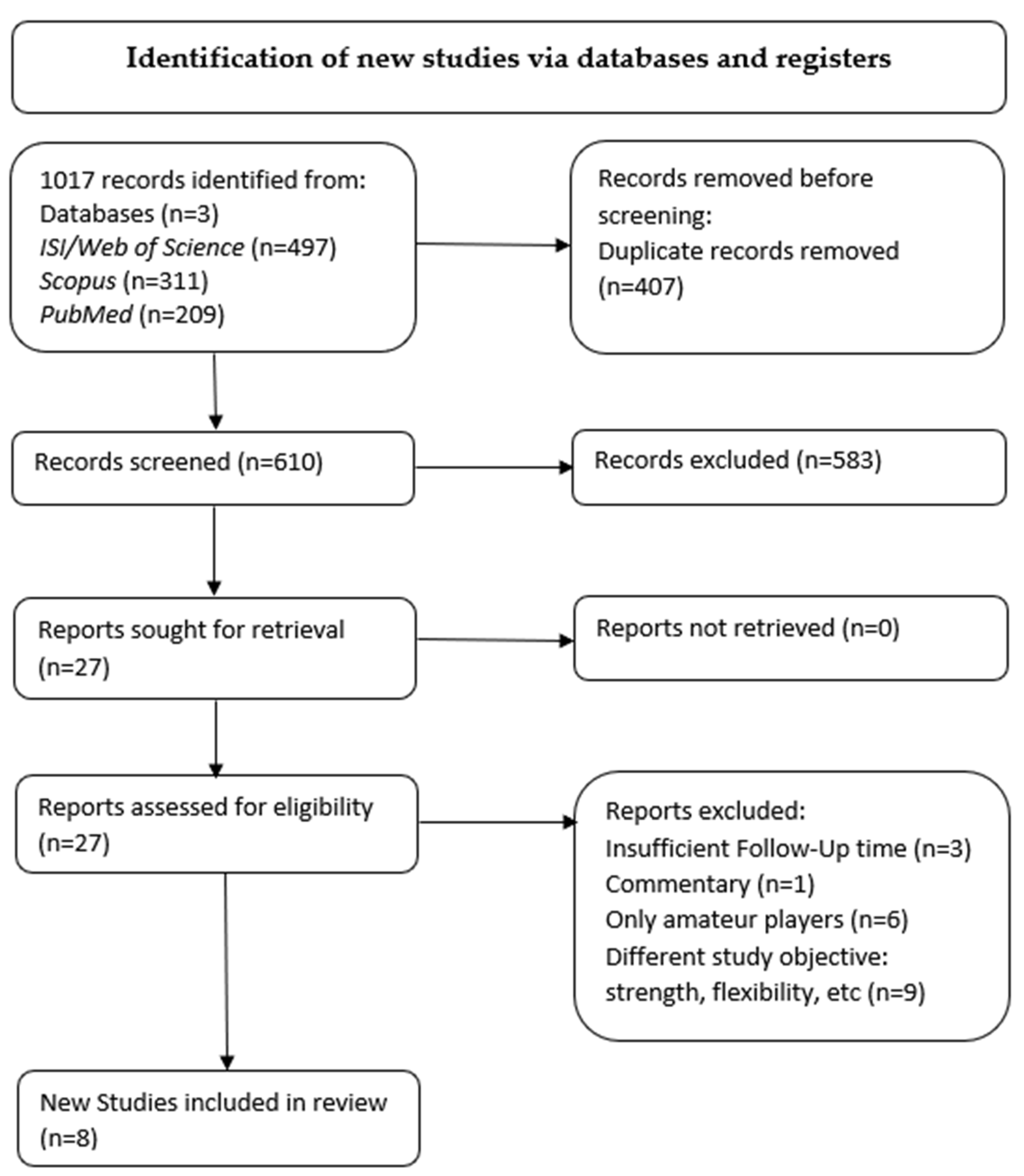
3.1. Literature Search
3.2. Patient Population
3.3. Quality Assessment
3.4. Risk of Bias
3.5. Prevention Protocols
3.6. Outcomes
- Whalan et al. [61]: 1.9569 (IIRCONTROL), 1.5767 (IIRINTERVENTION)
- Elerian et al. [62]: 4.884 (IIRCONTROL), 0.5007 (IIRINTERVENTION 1),
- 2.0008 (IIRINTERVENTION 2)
- Espinosa et al. [65]: U/D (Undetermined)
- Kraemer et al. [59]: 12.4378 (IIRCONTROL), 8.9623 (IIRINTERVENTION 1), 4.99 (IIRINTERVENTION 2), 9.7629 (IIRINTERVENTION 3), 7.4349 (IIRINTERVENTION 4), 5.238 (IIRINTERVENTION 5)
- Melegati et al. [58]: 2.269 (IIRCONTROL), 1.369 (IIRINTERVENTION)
- Silvers-Granelli et al. [63]: 1.5613 (IIRCONTROL), 0.3619 (IIRINTERVENTION)
- Grooms et al. [60]: 2.0678 (IIRCONTROL), 0.37 (IIRINTERVENTION)
- Petersen et al. [64]: U/D
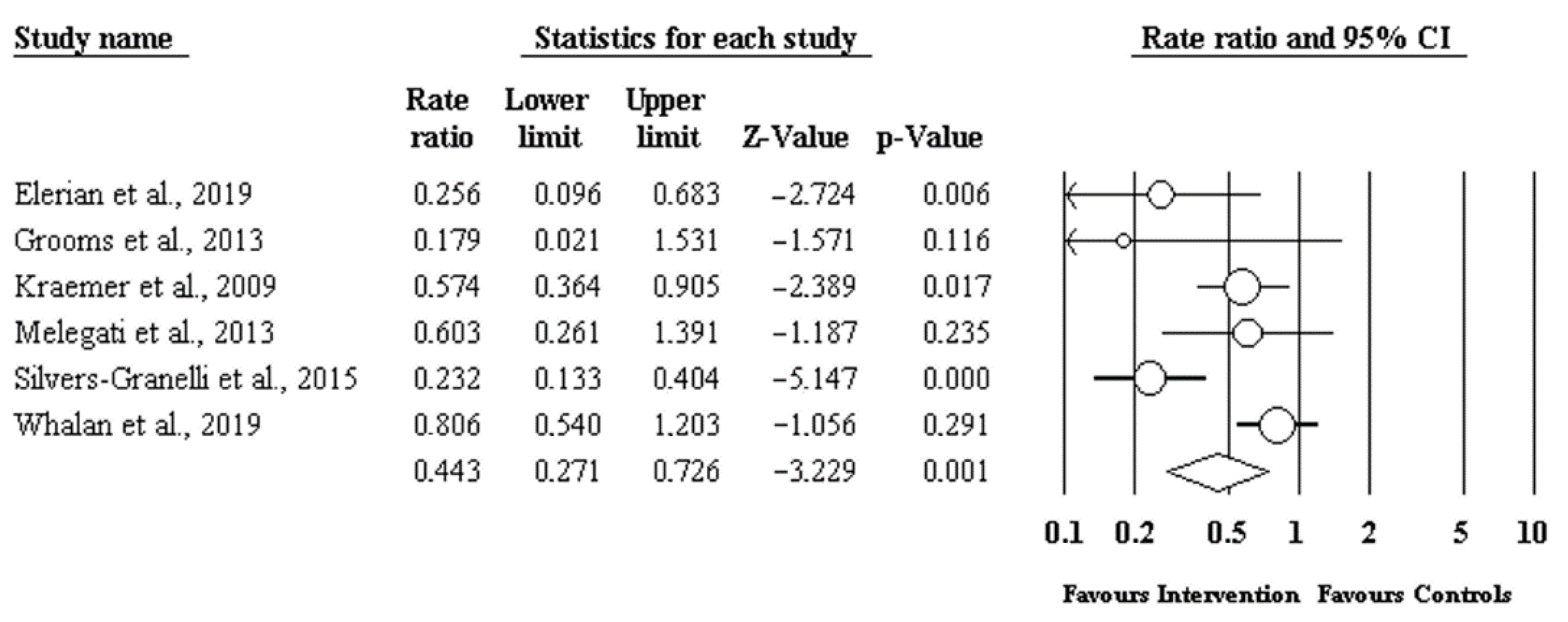
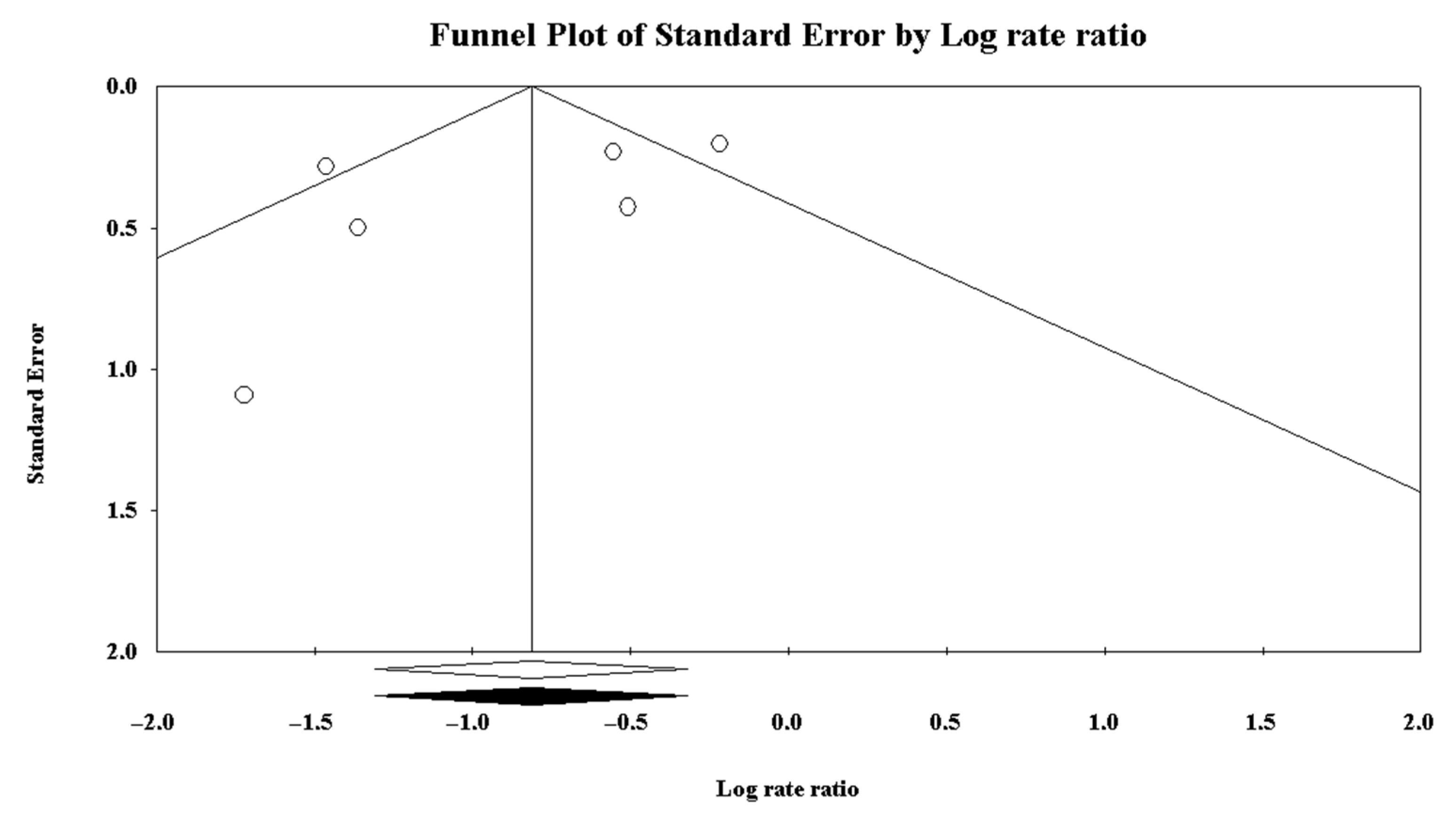
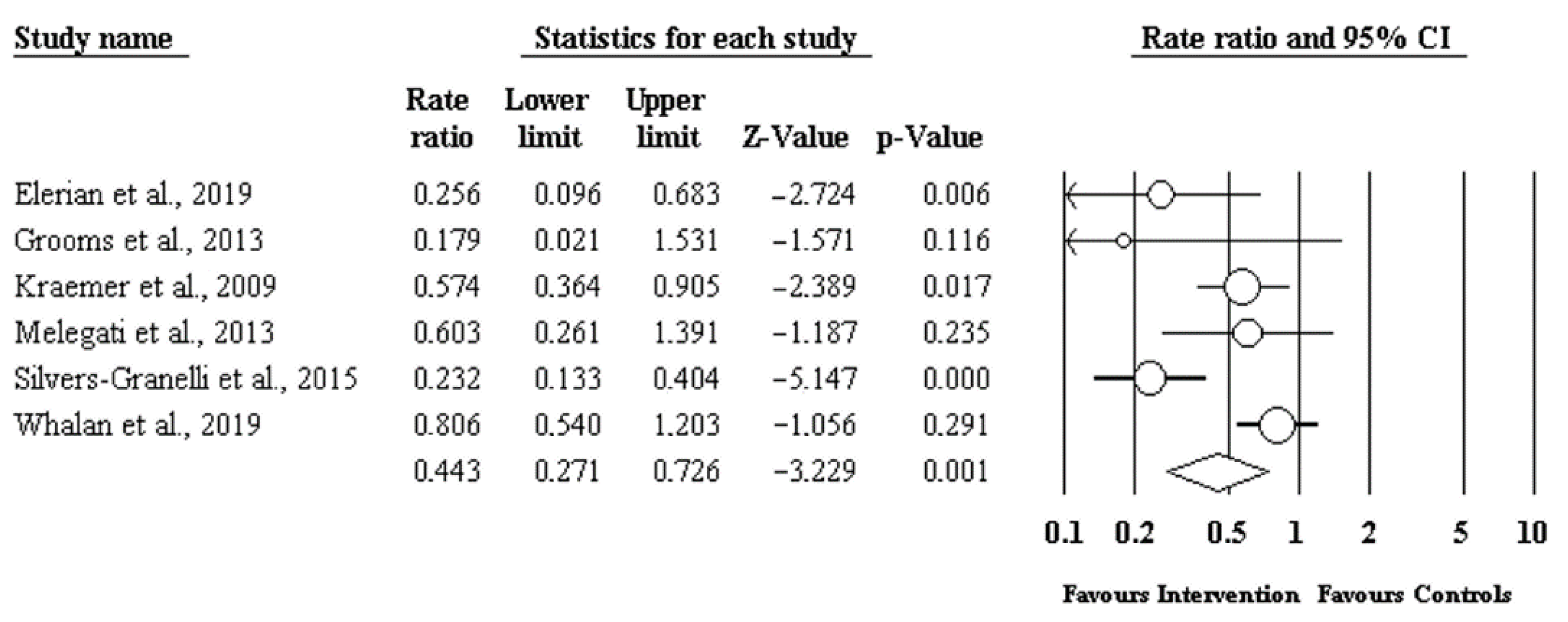
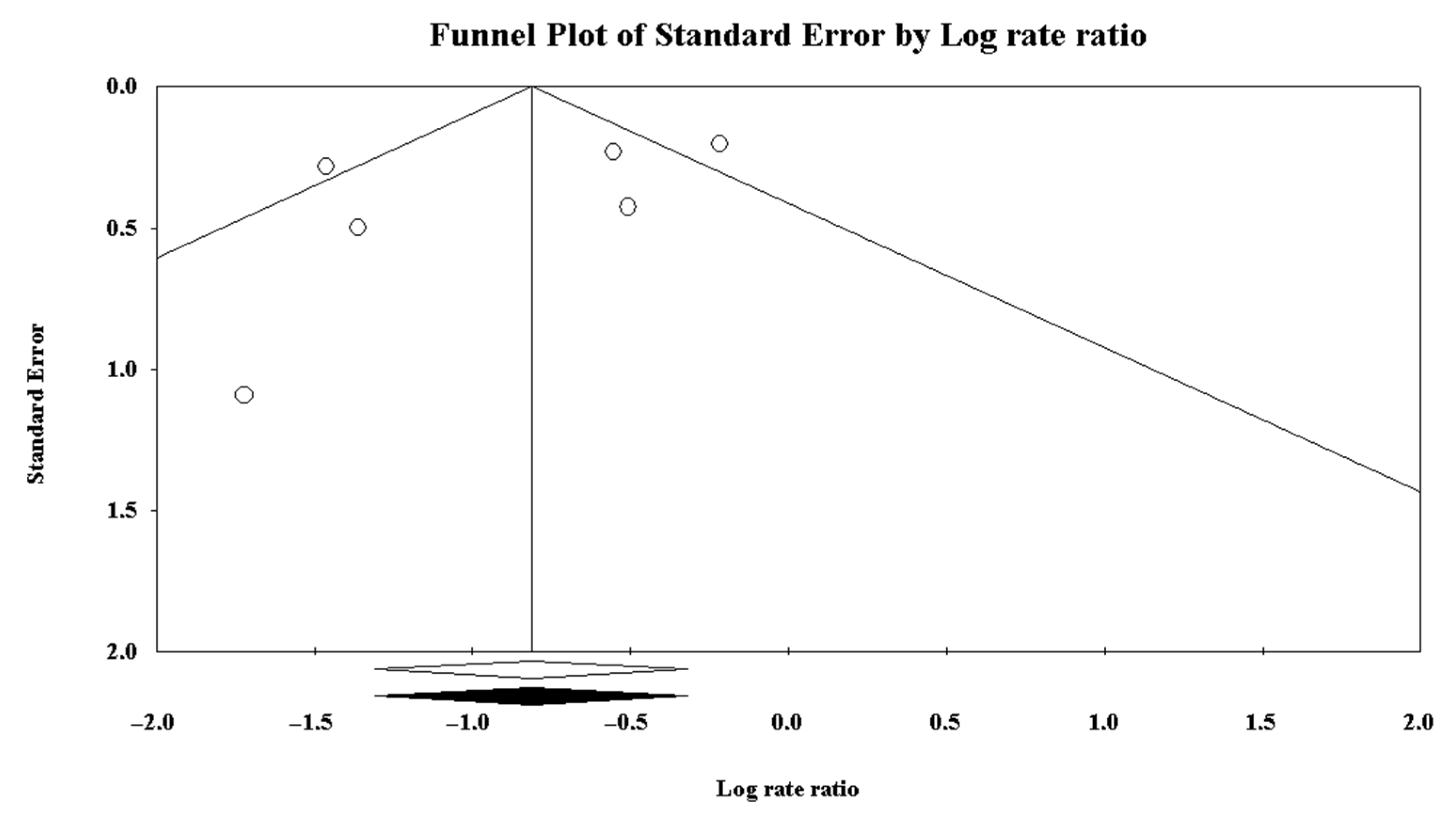
3.7. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longo, U.G.; Loppini, M.; Berton, A.; Marinozzi, A.; Maffulli, N.; Denaro, V. The FIFA 11+ program is effective in preventing injuries in elite male basketball players: A cluster randomized controlled trial. Am. J. Sports Med. 2012, 40, 996–1005. [Google Scholar] [CrossRef]
- Schmikli, S.L.; Backx, F.J.G.; Kemler, H.J.; Van Mechelen, W. National Survey on Sports Injuries in the Netherlands: Target Populations for Sports Injury Prevention Programs. Clin. J. Sport Med. 2009, 19, 101–106. [Google Scholar] [CrossRef]
- Anderson, K.; Strickland, S.M.; Warren, R. Hip and Groin injuries in athletes. Am. J. Sports Med 2001, 40, 521–533. [Google Scholar] [CrossRef]
- Carmichael, J.; Packham, I.; Trikha, S.P.; Wood, D.G. Avulsion of the Proximal Hamstring Origin. J. Bone Jt. Surg. Am. Vol. 2009, 91, 249–256. [Google Scholar] [CrossRef]
- Linklater, J.; Hamilton, B.; Carmichael, J.; Orchard, J.; Wood, D. Hamstring Injuries: Anatomy, Imaging, and Intervention. Semin. Musculoskelet. Radiol. 2010, 14, 131–161. [Google Scholar] [CrossRef]
- Laskovski, J.R.; Kahn, A.J.; Urchek, R.J.; Guanche, C.A. Endoscopic proximal hamstring repair and ischial bur-sectomy using modified portal placement and patient positioning. Arthrosc. Tech. 2018, 7, 1071–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempainen, L.; Sarimo, J.; Mattila, K.; Vaittinen, S.; Orava, S. Proximal hamstring tendinopathy: Results of sur-gical management and histopathologic findings. Am. J. Sports Med. 2009, 37, 727–734. [Google Scholar] [CrossRef]
- Degen, R.M. Proximal Hamstring Injuries: Management of Tendinopathy and Avulsion Injuries. Curr. Rev. Musculoskelet. Med. 2019, 12, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Domb, B.G.; Linder, D.; Sharp, K.G.; Sadik, A.; Gerhardt, M.B. Endoscopic Repair of Proximal Hamstring Avulsion. Arthrosc. Tech. 2013, 2, e35–e39. [Google Scholar] [CrossRef] [PubMed]
- Goldman, E.F.; Jones, D. Interventions for preventing hamstring injuries. Cochrane Database Syst. Rev. 2010, CD006782. [Google Scholar] [CrossRef] [PubMed]
- Larruskain, J.; Lekue, J.A.; Diaz, N.; Odriozola, A.; Gil, S.M. A comparison of injuries in elite male and female football players: A five-season prospective study. Scand. J. Med. Sci. Sports 2017, 28, 237–245. [Google Scholar] [CrossRef]
- Carlson, C. The natural history and management of hamstring injuries. Curr. Rev. Musculoskelet. Med. 2008, 1, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Gokeler, A.; Bisschop, M.; Benjaminse, A.; Myer, G.D.; Eppinga, P.; Otten, E. QuadriCeps function following ACL reconstruction and rehabil-itation: Implications for optimisation of current practices. Knee Surg. Sports Traumatol. Arthrosc. 2013, 28, 1163–1174. [Google Scholar]
- Bahr, R.; Thorborg, K.; Ekstrand, J. Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: The Nordic Hamstring survey. Br. J. Sports Med. 2015, 49, 1466–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drezner, J.A. Practical Management: Hamstring Muscle Injuries. Clin. J. Sport Med. 2003, 13, 48–52. [Google Scholar] [CrossRef]
- Sherry, M.A.; Best, T.M. A Comparison of 2 Rehabilitation Programs in the Treatment of Acute Hamstring Strains. J. Orthop. Sports Phys. Ther. 2004, 34, 116–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanni, G.; Frizziero, A.; Oliva, F.; Maffulli, N.; Gli, I.M.; Linee Guida, I.S.; Mu, L.T. Effects of Integrative Core Stability Training on Balance and Walking Speed in Healthy Elderly People. Adv. Phys. Educ. 2020, 1, 4–27. [Google Scholar]
- Ekstrand, J.; Hägglund, M.; Kristenson, K.; Magnusson, H.; Waldén, M. Fewer ligament injuries but no preventive effect on muscle in-juries and severe injuries: An 11-year follow-up of the UEFA Champions League Injury Study. Br. J. Sports Med. 2013, 47, 732–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sports Med. 2011, 46, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Árnason, A.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of hamstring strains in elite soccer: An intervention study. Scand. J. Med. Sci. Sports 2007, 18, 40–48. [Google Scholar] [CrossRef]
- Árnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Risk Factors for Injuries in Football. Am. J. Sports Med. 2004, 32, 5–16. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: A cluster-randomised controlled trial. Br. J. Sports Med. 2010, 44, 555–562. [Google Scholar] [CrossRef]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of injuries among male soccer players: A prospective, randomized intervention study targeting players with previous injuries or reduced function. Am. J. Sports Med. 2008, 36, 1052–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football: A cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Askling, C.M.; Tengvar, M.; Saartok, T.; Thorstensson, A. Acute first-time hamstring strains during high-speed running: A longitudinal study including clinical and magnetic resonance imaging findings. Am. J. Sports Med. 2007, 35, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Askling, C.; Saartok, T.; Thorstensson, A. Type of acute hamstring strain affects flexibility, strength, and time to return to pre-injury level. Br. J. Sports Med. 2006, 40, 40–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadebo, B.; White, J.; George, K.P. A survey of flexibility training protocols and hamstring strains in professional football clubs in England. Br. J. Sports Med. 2004, 38, 388–394. [Google Scholar] [CrossRef]
- Johnson, J.N. Competitive swimming illness and injury: Common conditions limiting participation. Curr. Sports Med. Rep. 2003, 2, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Mellion, M.B. Common cycling injuries. Management and prevention. Sports Med. 1991, 11, 52–70. [Google Scholar] [CrossRef]
- Levine, W.N.; Bergfeld, J.A.; Tessendorf, W. Intramuscular corticosteroid injection for hamstring injuries: A 13-year experience in the national football league. Am. J. Sports Med. 2000, 28, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J.; Seward, H. Epidemiology of injuries in the Australian Football League, season 1997. Br. J. Sports Med. 2002, 36, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Waldén, M.; Atroshi, I.; Magnusson, H.; Wagner, P.; Hägglund, M. Prevention of acute knee injuries in adolescent female football players: Cluster randomised controlled trial. BMJ 2012, 344, e3042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, C.S.; Redler, L.H.; Ciccotti, M.G.; Maffulli, N.; Longo, U.G.; Bradley, J. Evaluation and Management of Hamstring Injuries. Am. J. Sports Med. 2013, 41, 2933–2947. [Google Scholar] [CrossRef]
- Jonhagen, S.; Nemeth, G.; Eriksson, E. Hamstring injuries in sprinters. The role of concentric and eccentric ham-string muscle strength and flexibility. Am. J. Sports Med. 1994, 22, 6. [Google Scholar] [CrossRef]
- Schache, A. Eccentric hamstring muscle training can prevent hamstring injuries in soccer players. J. Physiother. 2012, 58, 58. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, Y.; Saito, T.; Sakuraba, K.; Sakuma, K.; Suzuki, E. Strength Deficits Identified with Concentric Action of the Hip Extensors and Eccentric Action of the Hamstrings Predispose to Hamstring Injury in Elite Sprinters. J. Orthop. Sports Phys. Ther. 2008, 38, 457–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, C.; Hawkins, R.D.; Maltby, S.; Hulse, M.; Thomas, A.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football--analysis of hamstring injuries. Br. J. Sports Med. 2004, 38, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sports 2003, 13, 244–250. [Google Scholar] [CrossRef]
- Croisier, J.-L. Factors Associated with Recurrent Hamstring Injuries. Sports Med. 2004, 34, 681–695. [Google Scholar] [CrossRef]
- Freckleton, G.; Pizzari, T. Risk factors for hamstring muscle strain injury in sport: A systematic review and me-ta-analysis. Br. J. Sports Med. 2013, 47, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef] [Green Version]
- Junge, A.; Lamprecht, M.; Stamm, H.; Hasler, H.; Bizzini, M.; Tschopp, M.; Reuter, H.; Wyss, H.; Chilvers, C.; Dvorak, J. Countrywide Campaign to Prevent Soccer Injuries in Swiss Amateur Players. Am. J. Sports Med. 2010, 39, 57–63. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive seasons. Br. J. Sports Med. 2006, 40, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewett, T.E.; Stroupe, A.L.; Nance, T.A.; Noyes, F.R. Plyometric training in female athletes: Decreased impact forces and increased hamstring torques. Am. J. Sports Med. 1996, 24, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Mjolsnes, R.; Árnason, A.; Osthagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.-E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, J.; Holmich, P. Evidence based prevention of hamstring injuries in sport. Br. J. Sports Med. 2005, 39, 319–323. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding Interobserver Agreement: The Kappa Statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Kennelly, J. Methodological approach to assessing the evidence. In Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes; Handler, A., Kennelly, J., Peacock, N., Eds.; Springer: Boston, MS, USA, 2011; pp. 7–19. [Google Scholar]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomized and non-randomized studies of health care interventions. J. Epidemiol. Commun. Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://search.pedro.org.au/ (accessed on 12 March 2021).
- Monajati, A.; Larumbe-Zabala, E.; Goss-Sampson, M.; Naclerio, F. The Effectiveness of Injury Prevention Pro-grams to Modify Risk Factors for Non-Contact Anterior Cruciate Ligament and Hamstring Injuries in Uninjured Team Sports Athletes: A Systematic Review. PLoS ONE 2016, 11, e0155272. [Google Scholar] [CrossRef]
- Farley, J.B.; Stein, J.; Keogh, J.W.L.; Woods, C.T.; Milne, N. The Relationship Between Physical Fitness Qualities and Sport-Specific Technical Skills in Female, Team-Based Ball Players: A Systematic Review. Sports Med. Open 2020, 6, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Melegati, G.; Tornese, D.; Gevi, M.; Trabattoni, A.; Pozzi, G.; Schonhuber, H.; Volpi, P. Reducing muscle injuries and reinjuries in one italian professional male soccer team. Muscle Ligaments Tendons J. 2019, 3, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, R.; Knobloch, K. A soccer-specific balance training program for hamstring muscle and patellar and Achilles tendon injuries: An intervention study in premier league female soccer. Am. J. Sports Med. 2009, 37, 1384–1393. [Google Scholar] [CrossRef] [PubMed]
- Grooms, D.R.; Palmer, T.; Onate, J.A.; Myer, G.D.; Grindstaff, T. Soccer-Specific Warm-Up and Lower Extremity Injury Rates in Collegiate Male Soccer Players. J. Athl. Train. 2013, 48, 782–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whalan, M.; Lovell, R.; Steele, J.R.; Sampson, J.A. Rescheduling Part 2 of the 11+ reduces injury burden and increases compliance in semi-professional football. Scand. J. Med. Sci. Sports 2019, 29, 1941–1951. [Google Scholar] [CrossRef]
- Elerian, A.E.; El-Sayyad, M.M.; Dorgham, H.A.A. Effect of Pre-training and Post-training Nordic Exercise on Hamstring Injury Prevention, Recurrence, and Severity in Soccer Players. Ann. Rehabil. Med. 2019, 43, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Silvers-Granelli, H.; Mandelbaum, B.R.; Adeniji, O.; Insler, S.; Bizzini, M.; Pohlig, R.; Junge, A.; Snyder-Mackler, L.; Dvorak, J. Efficacy of the FIFA 11+ Injury Prevention Program in the Collegiate Male Soccer Player. Am. J. Sports Med. 2015, 43, 2628–2637. [Google Scholar] [CrossRef] [Green Version]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmichn, P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: A cluster-randomized controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, G.D.A.; Pöyhönen, T.; Aramendi, J.F.; Samaniego, J.C.; Knorr, J.I.E.; Kyröläinen, H. Effects of an eccentric training programme on hamstring strain injuries in women football players. Biomed. Hum. Kinet. 2015, 7, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Gilchrist, J.; Mandelbaum, B.R.; Melancon, H.; Ryan, G.W.; Silvers, H.J.; Griffin, L.Y.; Watanabe, D.S.; Dick, R.W.; Dvorak, J. A Randomized Controlled Trial to Prevent Noncontact Anterior Cruciate Ligament Injury in Female Collegiate Soccer Players. Am. J. Sports Med. 2008, 36, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Safran, M.R.; Garrett, W.E.; Seaber, A.V.; Glisson, R.R.; Ribbeck, B.M. The role of warm up in muscular injury prevention. Am. J. Sports Med. 1988, 16, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Sarimo, J.; Lempainen, L.; Mattila, K.; Orava, S. Complete proximal hamstring avulsions: A series of 41 patients with operative treatment. Am. J. Sports Med. 2008, 36, 1110–1115. [Google Scholar] [CrossRef]
- Parkkari, J.; Kujala, U.M.; Kannus, P. Is it possible to prevent sports injuries? Review of controlled clinical trials and recommendations for future work. Sports Med. 2001, 31, 985–995. [Google Scholar] [CrossRef]
- Matsuda, D.K. Editorial Commentary: Proximal Hamstring Syndrome: Another Pain in the Buttock. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 122–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Author (Pubbliction Date) | Whalan et al. (2019) | Elerian et al. (2019) | Espinosa et al. (2015) | Kraemer et al. (2009) | Melegati et al. (2013) | Silvers-Granelli et al. (2015) | Grooms et al. (2013) | Petersen et al. (2011) | Total | |
|---|---|---|---|---|---|---|---|---|---|---|
| Type of study | Randomized Clinical Trial | Randomized Clinical Trial | Randomized Clinical Trial | Cohort Study | Case Series | Randomized Clinical Trial | Cohort Study | Randomized Clinical Trial | ||
| Level of Evidence | I | I | I | III | IV | I | III | I | ||
| n(M/F) | ||||||||||
| IG | 408 (M) | IG 1: 17 (M) | IG 2: 17 (M) | 22 (F) | 120 (F) | 36 (M) | 675 (M) | 34 (M) | 461 (M) | 1648 (M)/142 (F) |
| CG | 398 (M) | 35 (M) | 21 (F) | 24 (F) | 36 (M) | 850 (M) | 30 (M) | 481 (M) | 1830 (M)/45 (F) | |
| AGE * (years) | ||||||||||
| IG | 23.8 | 24.2 ± 3.2 | 24.5 ± 4.4 | 20 ± 3 | 21.0 ± 4 | U/D | 20.68 ± 1.46 | 20.0 ± 2.4 | 23.5 ± 4 | |
| CG | 24.8 | (same team) | 20 ± 3 | 21.0 ± 4 | U/D | 20.40 ± 1.66 | 20.3 ± 1.6 | 23 ± 4 | ||
| BMI (kg/m2) | ||||||||||
| IG | U/D | 22.4 ± 0.4 | 22.5 ± 0.2 | 23.3 ± 1.8 | 26.9 ± 1.2 | U/D | U/D | U/D | U/D | |
| CG | U/D | (same team) | 23.3 ± 1.8 | 26.9 ± 1.2 | U/D | U/D | U/D | U/D | ||
| Melegati et al. | Kraemer et al. | Grooms et al. | Whalan et al. | Elerian et al. | Silvers-Granelli et al. | Petersen et al. | Espinosa et al. | |
|---|---|---|---|---|---|---|---|---|
| 1. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 3. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 4. | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 |
| 5. | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 |
| 6. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 7. | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 |
| 8. | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 9. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10. | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 11. | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| 12. | U/D | U/D | 1 | 1 | 1 | U/D | 1 | 1 |
| 13. | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 |
| 14. | U/D | U/D | U/D | U/D | 1 | 1 | 1 | 1 |
| 15. | U/D | U/D | 1 | 0 | 1 | 1 | 1 | 1 |
| 16. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 17. | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| 18. | 0 | 0 | 0 | U/D | U/D | U/D | 1 | 1 |
| 19. | 0 | 1 | 1 | 1 | U/D | U/D | 1 | 1 |
| 20. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 21. | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 |
| 22. | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 |
| 23. | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 24. | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 25. | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 26. | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 |
| 27. | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 |
| 28. | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 |
| 29. | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 |
| 30. | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 |
| 31. | U/D | U/D | U/D | 1 | 0 | U/D | 1 | 1 |
| 32. | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 33. | U/D | U/D | 1 | 1 | 1 | 1 | 1 | 1 |
| 34. | U/D | U/D | 0 | 0 | 1 | U/D | U/D | 1 |
| TOTAL | 13/34 | 18/34 | 21/34 | 25/34 | 26/34 | 26/34 | 28/34 | 30/34 |
| Quality of the study | Poor | Fair | Good | Good | Good | Good | Good | Good |
| % | 38.2 | 52.9 | 61.8 | 73.5 | 76.5 | 76.5 | 82.4 | 88.2 |
| Author | Groups (=n) | Type of Protocol | EXP. (in h) | HSI (n) | Follow-Up (Weeks) | HI/1.000 h |
|---|---|---|---|---|---|---|
| Whalan et al. | IG (=408) | FIFA 11+ modified | 28,541.4 | 45 | 28–34 | 1.58/1000 h |
| CG (=398) | FIFA 11+ | 26,062.1 | 51 | 28–34 | 1.97/1000 h | |
| Elerian et al. | IG (=17) | Nordic Hamstring Exercise (NHE) Protocol pre and post training | 1997.1 | 1 | 12 | 0.5/1000 h |
| IG 2 (=17) | NHE Protocol pre training | 1999.2 | 4 | 12 | 2/1000 h | |
| CG (=35) | No prevention programme | 4095 | 20 | 12 | 4.89/1000 h | |
| Espinosa et al. | IG (=22) | Eccentring Training for 21 weeks, NHE and eccentric band exercise (EBE) | N/D | 1 | 28 | U/D |
| CG (=21) | Programme with leg swings (FLS), side leg swings (SLS) e multiple jumping (MJ) | N/D | 5 | 28 | U/D | |
| Kraemer et al. | IG (=120) | Balance Training Calculated in minutes after training sessions | TOT: 10,079 | TOT: 72 | TOT: 90–100 | 7.14/1000 h |
| CG (=24) | No prevention programme | 2003/2004: 2010 | 25 | 18–20 | 12.44/1000 h | |
| Melegati et al. | IG (=36) | Core Stability Exercises | 8041 | 11 | 42 | 1.37/1000 h |
| CG (=36) | No prevention programme | 4848 | 11 | 30 | 2.27/1000 h | |
| Silvers-Granelli et al. | IG (=675) | FIFA 11+ | 44,212 | 16 | 20–22 | 0.45/1000 h |
| CG (=850) | No prevention programme | 35,226 | 55 | 20–22 | 1.24/1000 h | |
| Grooms et al. | IG (=34) | FIFA 11+ | 2703 | 1 | 32–36 | 0.37/1000 h |
| CG (=30) | No prevention programme | 2418 | 5 | 32–36 | 2.07/1000 h | |
| Petersen et al. | IG (=461) | NHE Protocol | U/D | 15 | 80 | U/D |
| CG (=481) | No prevention programme | U/D | 52 | 80 | U/D | |
| Total | IG (=1790) | 95,093.4 | 165 | |||
| CG (=1875) | 75,128.4 | 224 | ||||
| Total of Patients | (=3665) | 170,221.8 | 389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272. https://doi.org/10.3390/ijerph18168272
Biz C, Nicoletti P, Baldin G, Bragazzi NL, Crimì A, Ruggieri P. Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8272. https://doi.org/10.3390/ijerph18168272
Chicago/Turabian StyleBiz, Carlo, Pietro Nicoletti, Giovanni Baldin, Nicola Luigi Bragazzi, Alberto Crimì, and Pietro Ruggieri. 2021. "Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8272. https://doi.org/10.3390/ijerph18168272
APA StyleBiz, C., Nicoletti, P., Baldin, G., Bragazzi, N. L., Crimì, A., & Ruggieri, P. (2021). Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(16), 8272. https://doi.org/10.3390/ijerph18168272