
A Feeling of Otherness: A Qualitative Research Synthesis Exploring the Lived Experiences of Stigma in Individuals with Inflammatory Bowel Disease



Abstract
:1. Introduction
Aim
2. Materials and Methods
2.1. Search Strategy
2.2. Study Eligibility
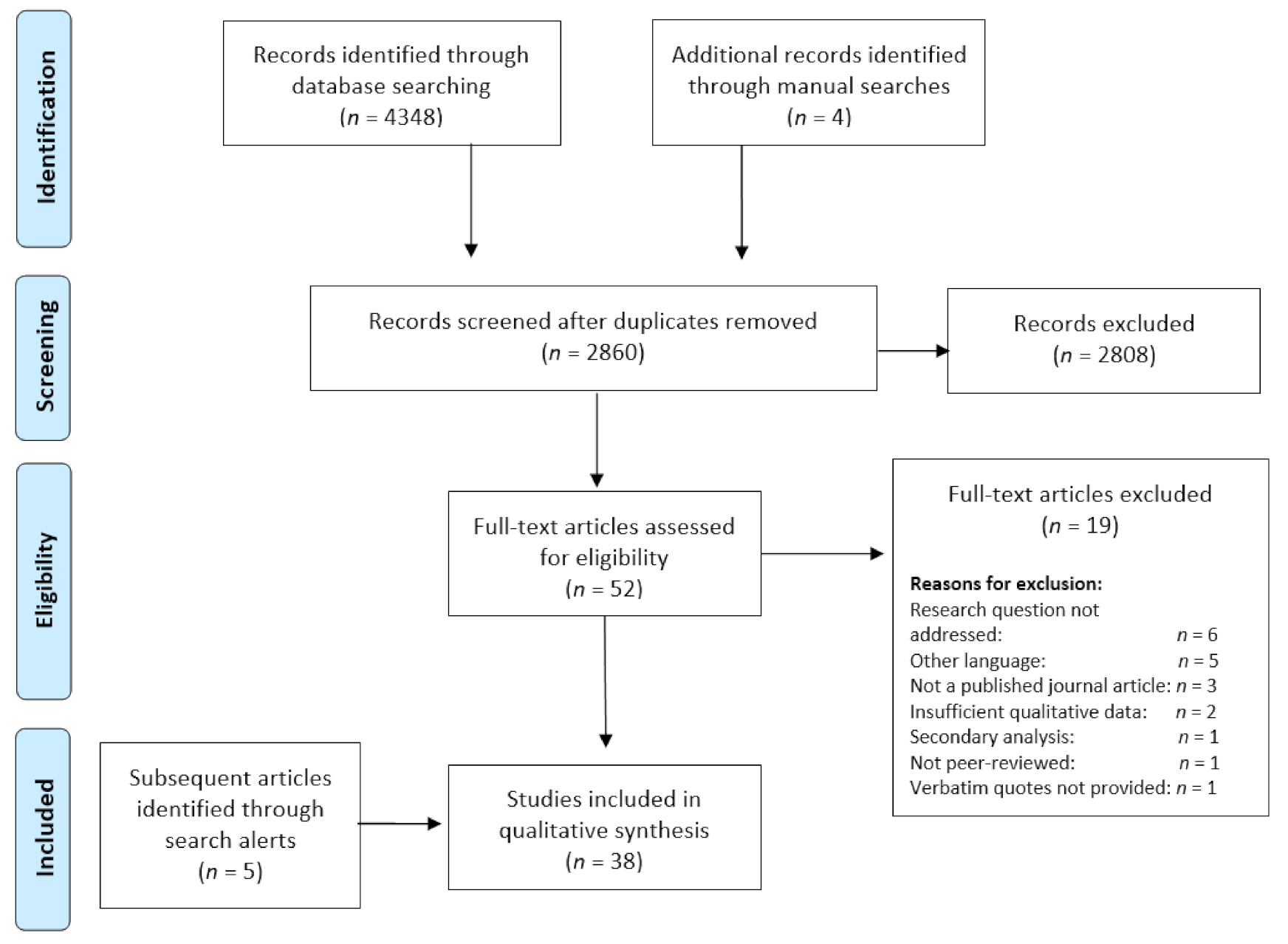
2.3. Literature Screening
2.4. Study Characteristics
2.5. Quality Assessment
2.6. Data Extraction
2.7. Data Analysis, Synthesis, and Interpretation
3. Results
3.1. The IBD Journey
3.1.1. Reduced to a Label
“[The] consultant gave me a [national support group] leaflet and said, ‘You should get in touch because they’re very helpful for people like you.’ I remember walking out of the room thinking, ‘people like me?’ What the hell is he talking about? It took me ages to work out why that rubbed me up the wrong way. He was separating me out from the crowd and putting me in a box that went, ‘people like you over there. You’re not here, you’re over there’.”[23]
“It made me feel like it’s not colitis and Andrea, it’s Andrea with colitis, ya know, I was always putting it like at the front of my mind when I shouldn’t have been, I should have been thinking of myself more.” [47]“I can’t live like this … I don’t want to be a disease; I just want to be me.”[66]
3.1.2. The Spoiled Self
“You just feel like you are different…you’re not a healthy person anymore. I just feel like an unhealthy person, so it just makes me feel like…I’m not good enough in a way.”[56]
“I doubted myself, I doubted my value, I doubted my worth, I doubted my capability.”[71]
“I hate that I can’t handle having a full time job and having my kids. I don’t feel like I’m living up to the standards that I want for wife and mom, that’s one of my biggest struggles.”[64]
“My parents have never made any demands on me. I think this is negative. My mum felt pity about me. She has been coddling me all the time. I became more and more sad.”[52]
3.1.3. Re-Building the Self
“It’s not going to go away, better it stays part of me, but I don’t want it to define me.”[53]
“I don’t want to be considered “unhealthy.” What do I want? Empathy? Support? A visible symptom? I wouldn’t say no to any of them, but what do I really want? I just want me back.”; “I stand there facing the mirror. Not recognizing its reflection. Not wanting to recognize it. It’s not me. This is not me. Who am I kidding? This is what you have become. This is what’s left of you. Is this really me now?”[63]
“I’ve helped a lot of people with Crohn’s and connected with them. I think maybe that’s what I’m here for. To help people dealing with the same thing…”[64]
3.2. A Need to Be Understood
3.2.1. A Shameful Secret
“It comes from me and how I feel about [colitis]; I think it’s disgusting, horrible, and smelly—going to the toilet all the time and seeing all this gunk and blood and mucus. I think it’s disgusting, so I guess if people knew the full extent of what I see every day, they would think the same.”[23]
“When I have to use the bathroom in the house of someone who is not a member of my family, I worry that the people there are thinking ‘look at him, coming to my house to constantly use my WC’, so I look for other alternatives because I don’t want people to think I’m dirty or weird’.”[45]
“I can’t tell you, talking about it is terrible because when I’m ill I don’t go out, I can’t face it. Whenever you go to use public toilets you’re never in a contained area. I can’t cope because of what everybody will think.”[57]
3.2.2. Knowing Is Not Understanding
“a prejudice of sorts that they have against me is when they say… come on, it’s just your stomach… they can’t understand, they go to the toilet like once every other day… ahh… I can’t keep it inside me… I just need to put up with it, so… it’s actually hard [tears start coming].”[70]
“No one in my life understands what I am going through and strangers judge you and think you are contagious or disgusting.’’[50]
“When I first came out of hospital the last time my nan just called it a dicky tummy and I had IBS, so I felt pretty upset about that because that made me feel really like they didn’t understand what I went through, and they should’ve because they’re my family.”[47]
“Once I was admitted to casualty with acute pain and still he [the doctor] told me that nothing was wrong. In the meantime I took tranquillizers and he [the doctor] told me to continue taking them since I was having panic attacks. but I knew that something was wrong... I began to doubt whether my family believed me or not and I would fill up with anger.”[69]
3.2.3. Social Estrangement
“It’s just the way the ethnic community is and with food and obviously food is a big part of the culture… everything is based around food, weddings are based around food, you go into people’s houses, it’s all about bringing as much food as you can and that’s what entertaining is… It is a different culture and just, you know, you will stand out… because you’re not eating.”[54]
“They don’t necessarily have to react badly, but if I think that they’re thinking something then…”[55]
“At work they assigned me to places where I was on my own, so that I could easily go to the bathroom. In that way I would not hinder the work production.”[69]
“People don’t get it, and I don’t expect them to, I guess. But, sometimes it’s easier just to not deal with it, and just stay in our little section, our little corner, on the farm, and be comfortable.”[64]
“Relationships and friendships have suffered a great deal. I’ve found that my circle of friends and family members have very little understanding of IBD. Because of this I feel isolated and mostly keep to myself in my spare time.”[50]
3.2.4. The Freedom of Authenticity
“I’ve wondered if it would help if he [partner] knew a little more. But I don’t know, I don’t want to say all these symptoms, so many of them are gross. [If I communicated more] maybe he would be more empathic.”[64]
“When I could not tell (I had Crohn’s disease), I felt really stressed. I also wanted them (my friends) to understand why I could not travel with them. However, I could not tell the truth.”[67]
“I think if anything those friends have become closer because I think they feel I’ve shared a lot more with them now because they know so much about it and they know how hard it’s been, they’ve been there in the hospital and wherever else and they’re still with me when I feel terrible so they see it face to face.”[47]
“I met someone at work who also had UC. And it was good to talk to someone who understands exactly my situation. It made me feel less alone with this problem.”[62]
3.3. Overarching Concept: Feeling of Otherness
4. Discussion
4.1. Implications and Recommendations
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fakhoury, M.; Negrulj, R.; Mooranian, A.; Al-Salami, H. Inflammatory bowel disease: Clinical aspects and treatments. J. Inflamm. Res. 2014, 7, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loftus, E.V., Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental influences. Gastroenterology 2004, 126, 1504–1517. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Ha, F.; Khalil, H. Crohn’s disease: A clinical update. Ther. Adv. Gastroenterol. 2015, 8, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Ko, J.K.; Auyeung, K.K. Inflammatory bowel disease: Etiology, pathogenesis and current therapy. Curr. Pharm. Design 2014, 20, 1082–1096. [Google Scholar] [CrossRef]
- Farrell, D.; McCarthy, G.; Savage, E. Self-reported symptom burden inindividuals with inflammatory bowel disease. J. Crohn’s Colitis 2016, 10, 315–322. [Google Scholar] [CrossRef]
- Byron, C.; Cornally, N.; Burton, A.; Savage, E. Challenges of living with and managing inflammatory bowel disease: A meta-synthesis of patients’ experiences. J. Clin. Nurs. 2020, 29, 305–319. [Google Scholar] [CrossRef]
- Kemp, K.; Griffiths, J.; Lovell, K. Understanding the health and social care needs of people living with IBD: A meta-synthesis of the evidence. World J. Gastroenterol. 2012, 18, 6240–6249. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.R.; Ediger, J.P.; Graff, L.A.; Greenfeld, J.M.; Clara, I.; Lix, L.; Rawsthorne, P.; Miller, N.; Rogala, L.; McPhail, C.M.; et al. The Manitoba IBD cohort study: A population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am. J. Gastroenterol. 2008, 103, 1989–1997. [Google Scholar] [CrossRef]
- Van der Have, M.; Van der Aalst, K.S.; Kaptein, A.A.; Leenders, M.; Siersema, P.D.; Oldenburg, B.; Fidder, H.H. Determinants of health-related quality of life in Crohn’s disease: A systematic review and meta-analysis. J. Crohn’s Colitis 2014, 8, 93–106. [Google Scholar] [CrossRef] [Green Version]
- Greene, B.R.; Blanchard, E.B.; Wan, C.K. Long-term monitoring of psychosocial stress and symptomatology in inflammatory bowel disease. Behav. Res. Ther. 1994, 32, 217–226. [Google Scholar] [CrossRef]
- Rampton, D. Does Stress Influence Inflammatory Bowel Disease? The Clinical Data. Dig. Dis. 2009, 27, 76–79. [Google Scholar] [CrossRef]
- Marin-Jiminez, I.; Montoya, M.G.; Panadero, A.; Cañas, M.; Modino, Y.; Romero de Santos, C.; Guardiola, J.; Carmona, L.; Barreiro-de Acosta, M. Management of the Psychological Impact of Inflammatory Bowel Disease: Perspective of Doctors and Patients—The ENMENTE Project. Inflamm. Bowel Dis. 2017, 23, 1492–1498. [Google Scholar] [CrossRef] [Green Version]
- Weiss, M.G.; Ramakrishna, J.; Somma, D. Health-related stigma: Rethinking concepts and interventions. Psychol. Health Med. 2006, 11, 277. [Google Scholar] [CrossRef]
- Major, B.; O’Brien, L. The social psychology of stigma. Annu. Rev. Psychol. 2005, 56, 393–421. [Google Scholar] [CrossRef] [Green Version]
- Link, B.G.; Phelan, J.C. Conceptualizing stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Earnshaw, V.A.; Quinn, D.M. The impact of stigma in health- care on people living with chronic illnesses. J. Health Psychol. 2011, 17, 157–168. [Google Scholar] [CrossRef] [Green Version]
- Scambler, G.; Heijnders, M.; van Brakel, W.H. Under-standing and tackling health-related stigma. Psychol. Health Med. 2006, 11, 269–270. [Google Scholar]
- Polak, E.J.; O’Callaghan, F.; Oaten, M. Perceptions of IBD within patient and community samples: A systematic review. Psychol. Health 2020, 35, 425–448. [Google Scholar] [CrossRef]
- Taft, T.H.; Keefer, L. A systematic review of disease-related stigmatization in patients living with inflammatory bowel disease. Clin. Exp. Gastroenterol. 2016, 9, 49–58. [Google Scholar]
- Jones, E.; Farina, A.; Hastorf, A.; Markus, H.; Miller, D.; Scott, R. Social Stigma: The Psychology of Marked Relationships; Freeman: New York, NY, USA, 1984. [Google Scholar]
- Weinberg, M.; Williams, C. Fecal matters: Habitus. Embodiments and deviance. Soc. Probl. 2005, 52, 315–336. [Google Scholar] [CrossRef]
- Dibley, L.; Norton, C.; Whitehead, E. The experience of stigma in inflammatory bowel disease: An interpretive (hermeneutic) phenomenological study. J. Adv. Nurs. 2018, 74, 838–851. [Google Scholar] [CrossRef] [PubMed]
- Joachim, G.; Acorn, S. Stigma of visible and invisible chronic conditions. J. Adv. Nurs. 2000, 32, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Cococcia, S.; Ghorayeb, J.; Di Sabatino, A.; Selinger, C.P. Stigmatisation and resilience in inflammatory bowel disease. Intern. Emerg. Med. 2020, 15, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Heijnders, M.; Van Der Meij, S. The fight against stigma: An overview of stigma-reduction strategies and interventions. Psychol. Health Med. 2006, 11, 353–363. [Google Scholar] [CrossRef]
- Vanderheyden, L.C.; Verhoef, M.J.; Hilsden, R.J. Qualitative re-search in inflammatory bowel disease: Dispelling the myths of an unknown entity. Dig. Liver Dis. 2006, 38, 60–66. [Google Scholar] [CrossRef]
- Dibley, L.; Williams, E.; Young, P. When family don’t acknowledge: A hermeneutic study of the experience of kinship stigma in community-dwelling people with inflammatory bowel disease. Qual. Health Res. 2019, 30, 1196–1211. [Google Scholar] [CrossRef]
- Dibley, L.; Norton, C.; Schaub, J.; Bassett, P. Experiences of gay and lesbian patients with inflammatory bowel disease: A mixed methods study. Gastrointest. Nurs. 2004, 12, 19–30. [Google Scholar] [CrossRef]
- Frohlich, D.O. Support often outweighs stigma for people with inflammatory bowel disease. Gastroenterol. Nurs. 2014, 37, 126–136. [Google Scholar] [CrossRef]
- Saunders, B. Stigma, deviance and morality in young adults’ accounts of inflammatory bowel disease. Sociol. Health Illn. 2014, 36, 1020–1036. [Google Scholar] [CrossRef]
- Major, C.M.; Savin-Baden, M. An Introduction to Qualitative Research Synthesis: Managing the Information Explosion in Social Science Research; Routledge: London, UK, 2010. [Google Scholar]
- Finfgeld-Connett, D. A Guide to Qualitative Meta-Synthesis; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Toye, F.; Seers, K.; Allcock, N.; Briggs, M.; Carr, E.; Barker, K. Meta-ethnography 25 years on: Challenges and insights for synthesising a large number of qualitative studies. BMC Med. Res. Methodol. 2014, 14, 80. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, E.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [Green Version]
- Noblit, G.W.; Hare, R.D. Meta-Ethnography: Synthesizing Qualitative Studies; SAGE: Thousand, Oaks, CA, USA, 1988. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzla, J.; Altman, G. The PRISMA Group. Preferred reporting items for systematic review and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 6 August 2020).
- Norton, B.A.; Thomas, R.; Lomax, K.G.; Dudley-Brown, S. Patient perspectives on the impact of Crohn’s disease: Results from group interviews. Patient Prefer. Adherence 2012, 6, 509–520. [Google Scholar] [CrossRef] [Green Version]
- Barned, C.; Stinzi, A.; Mack, D.; O’Doherty, K.C. To tell or not to tell: A qualitative interview study on disclosure decisions among children with inflammatory bowel disease. Soc. Sci. Med. 2016, 162, 115–123. [Google Scholar] [CrossRef]
- Demirtas, A. The lived experiences of people with inflammatory bowel diseases: A phenomenological hermeneutic study. Int. J. Nurs. Pract. 2021, e12946. [Google Scholar]
- Dudley-Brown, S. Living with ulcerative colitis. Gastroenterol. Nurs. 1996, 19, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Daniel, J.M. Young adults’ perceptions of living with chronic inflammatory bowel disease. Gastroenterol. Nurs. 2012, 25, 83–94. [Google Scholar] [CrossRef]
- Devlen, J.; Beusterien, K.; Yen, L.; Ahmed, A.; Cheifetz, A.S.; Moss, A.C. The burden of inflammatory bowel disease: A patient-reported qualitative analysis and development of a conceptual model. Inflamm. Bowel Dis. 2014, 20, 545–552. [Google Scholar] [CrossRef] [Green Version]
- García-Sanjuán, S.; Lillo-Crespo, M.; Richart-Martínez, M.; Sanjuán Quiles, Á. Understanding life experiences of people affected by Crohn’s disease in Spain. A phenomenological approach. Scand. J. Caring Sci. 2017, 32, 354–362. [Google Scholar] [CrossRef]
- Lynch, T.; Spence, D. A qualitative study of youth living with Crohn disease. Gastroenterol. Nurs. 2008, 31, 224–230. [Google Scholar] [CrossRef]
- Matini, L.; Ogden, J. A qualitative study of patients’ experience of living with inflammatory bowel disease: A preliminary focus on the notion of adaptation. J. Health Psychol. 2016, 21, 2493–2502. [Google Scholar] [CrossRef]
- Mukherjee, S.; Sloper, P.; Turnbull, A. An insight into the experiences of parents with inflammatory bowel disease. J. Adv. Nurs. 2012, 37, 355–363. [Google Scholar] [CrossRef]
- Nicholas, D.B.; Otley, A.; Smith, C.; Avolio, J.; Munk, M.; Griffiths, A.M. Challenges and strategies of children and adolescents with inflammatory bowel disease: A qualitative examination. Health Qual. Life Outcomes 2007, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Purc-Stephenson, R.; Bowlby, D.; Qaqish, S.T. A gift wrapped in barbed wire Positive and negative life changes after being diagnosed with inflammatory bowel disease. Qual. Life Res. 2014, 24, 1197–1205. [Google Scholar] [CrossRef]
- Richard, L.; Noller, G.; Derrett, S.; Sullivan, T.; Noble, F.; McCombie, A.; Schultz, M.; Ho, C.; Stokes, T. Patients’ accounts of living with and managing inflammatory bowel disease in rural Southern New Zealand: A qualitative study. BMJ Open 2020, 10, e041789. [Google Scholar] [CrossRef]
- Brydolf, M.; Segesten, K. Living with ulcerative colitis: Experiences of adolescents and young adults. J. Adv. Nurs. 1996, 23, 39–47. [Google Scholar] [CrossRef]
- Mikocka-Walus, A.; Hanlon, I.; Dober, M.; Emerson, C.; Beswick, L.; Selinger, C.; Taylor, J.; Olive, L.; Evans, S.; Hewitt, C. Lived experience in people with inflammatory bowel disease and comorbid anxiety and depression in the United Kingdom and Australia. J. Health Psychol. 2020. [Google Scholar] [CrossRef]
- Alexakis, C.; Nash, A.; Lloyd, M.; Brooks, F.; Lindsay, J.O.; Poullis, A. Inflammatory bowel disease in young patients: Challenges faced by black and minority ethnic communities in the UK. Health Soc. Care Community 2015, 23, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Carter, B.; Rouncefield-Swales, A.; Bray, L.; Blake, L.; Allen, S.; Probert, C.; Crook, K.; Qualter, P. I Don’t Like to Make a Big Thing out of I": A Qualitative Interview-Based Study Exploring Factors Affecting Whether Young People Tell or Do Not Tell Their Friends about Their IBD. Int. J. Chronic Dis. 2020, 11, 1059025. [Google Scholar] [CrossRef]
- Cho, R.; Wickert, N.M.; Klassen, A.F.; Tsangaris, E.; Marshall, J.K.; Brill, H. Identifying Needs in Young Adults With Inflammatory Bowel Disease. Gastroenterol. Nurs. 2018, 41, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.M.; Collier, J.; James, V.; Hawkey, C.J. Beliefs about personal control and self-management in 30–40 year olds living with inflammatory bowel disease: A qualitative study. Int. J. Nurs. Stud. 2010, 47, 1500–1509. [Google Scholar] [CrossRef] [PubMed]
- Czuber-Dochan, W.; Dibley, L.B.; Terry, H.; Ream, E.; Norton, C. The experience of fatigue in people with inflammatory bowel disease: An exploratory study. J. Adv. Nurs. 2012, 69, 1987–1999. [Google Scholar] [CrossRef] [PubMed]
- Czuber-Dochan, W.; Morgan, M.; Hughes, L.D.; Lomer, M.C.; Lindsay, J.O.; Whelan, K. Perceptions and psychosocial impact of food, nutrition, eating and drinking in people with inflammatory bowel disease: A qualitative investigation of food-related quality of life. J. Hum. Nutr. Diet. 2020, 33, 115–127. [Google Scholar] [CrossRef]
- Hall, N.J.; Rubin, G.P.; Dougall, A.; Hungin, A.P.S.; Neely, J. The fight for ‘health-related normality’: A qualitative study of the experiences of individuals living with established inflammatory bowel disease (IBD). J. Health Psychol. 2005, 10, 443–455. [Google Scholar] [CrossRef]
- Jordan, C.; Ohlsen, R.; Hayee, B.H.; Chalder, T. A qualitative study exploring the experience of people with IBD and elevated symptoms of anxiety and low mood and the type of psychological help they would like. Psychol. Health 2017, 33, 634–651. [Google Scholar] [CrossRef]
- Larsson, K.; Lööf, L.; Nordin, K. Stress, coping and support needs of patients with ulcerative colitis or Crohn’s disease: A qualitative descriptive study. J. Clin. Nurs. 2016, 26, 648–657. [Google Scholar] [CrossRef]
- Moore, I.S. The beast within: Life with an invisible chronic illness. Qual. Inq. 2013, 19, 201–208. [Google Scholar] [CrossRef]
- Nutting, R.; Grafsky, E.L. Crohn’s disease and the young couple: An interpretative phenomenological analysis. Contemp. Fam. Ther. 2018, 40, 176–187. [Google Scholar] [CrossRef]
- Lesnovska, K.P.; Hjortswang, H.; Ek, A.C.; Frisman, G.H. Patients’ perspective of factors influencing quality of life while living with Crohn disease. Gastroenterol. Nurs. 2010, 33, 37–44. [Google Scholar] [CrossRef]
- Lesnovska, K.P.; Frisman, G.H.; Hjortswang, H.; Börjeson, S. Critical situations in daily life as experienced by patients with inflammatory bowel disease. Gastroenterol. Nurs. 2016, 39, 195. [Google Scholar] [CrossRef] [Green Version]
- Ruan, J.; Wu, L.; Zho, Y. Experiences of Body Image Changes in Chinese Patients Living with Inflammatory Bowel Disease: A Descriptive Qualitative Study. Asian Nurs. Res. 2020, 14, 196–205. [Google Scholar] [CrossRef]
- Ruan, J.; Zhou, Y. Regaining normality: A grounded theory study of the illness experiences of Chinese patients living with Crohn’s disease. Int. J. Nurs. Stud. 2019, 93, 87–96. [Google Scholar] [CrossRef]
- Sammut, J.; Scerri, J.; Xuereb, R.B. The lived experience of adults with ulcerative colitis. J. Clin. Nurs. 2015, 24, 2659–2667. [Google Scholar] [CrossRef]
- Vejzovic, V.; Bramhagen, A.C.; Idvall, E.; Wennick, A. Swedish children’s lived experience of ulcerative colitis. Gastroenterol. Nurs. 2018, 41, 333–340. [Google Scholar]
- Wilburn, J.; Twiss, J.; Kemp, K.; McKenna, S.P. A qualitative study of the impact of Crohn’s disease from a patient’s perspective. Frontline Gastroenterol. 2017, 8, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Goffman, E. Stigma: Notes on the Management of a Spoiled Identity; Prentice Hall: Englewood Cliffs, NJ, USA, 1963. [Google Scholar]
- Taft, T.H.; Keefer, L.; Artz, C.; Bratten, J.; Jones, M.P. Perceptions of illness stigma in patients with inflammatory bowel disease and irritable bowel syndrome. Qual. Life Res. 2011, 20, 1391. [Google Scholar] [CrossRef]
- Taft, T.H.; Keefer, L.; Leonhard, C.; Nealon-Woods, M. Impact of perceived stigma on inflammatory bowel disease patient outcomes. Inflamm. Bowel Dis. 2009, 15, 1224–1232. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J.; Buron, A.; Rojas-Farreras, S.; De Graaf, R.; Haro, J.M.; De Girolamo, G. Perceived stigma among individuals with common mental disorders. J. Affect. Disord. 2009, 118, 180–186. [Google Scholar] [CrossRef]
- Lowther, K.; Selman, L.; Harding, R.; Higginson, I.J. Experience of persistent psychological symptoms and perceived stigma among people with HIV on antiretroviral therapy (ART): A systematic review. Int. J. Nurs. Stud. 2014, 51, 1171–1189. [Google Scholar] [CrossRef]
- Watson, A.C.; Corrigan, P.; Larson, J.E.; Sells, M. Self-stigma in people with mental illness. Schizophr. Bull. 2007, 33, 1312–1318. [Google Scholar] [CrossRef] [Green Version]
- Stanton, A.; Revenson, T.; Tennen, H. Health psychology: Psycho-logical adjustment to chronic illness. Annu. Rev. Psychol. 2007, 58, 565–592. [Google Scholar] [CrossRef] [Green Version]
- Parekh, N.K.; McMaster, K.; Nguyen, D.L.; Shah, S.; Speziale, A.; Miller, J.; Melmed, G. Coping Strategies Used by Adult Patients with Inflammatory Bowel Disease. South. Med. J. 2015, 108, 337–342. [Google Scholar]
- Miller, C.T.; Kaiser, C.R. A theoretical perspective on coping with stigma. J. Soc. Issues 2001, 57, 73–92. [Google Scholar] [CrossRef]
- Quinn, D.M.; Earnshaw, V.A. Understanding concealable stigmatized identities: The role of identity in psychological, physical, and behavioral outcomes. Soc. Issues Policy Rev. 2011, 5, 160–190. [Google Scholar] [CrossRef]
- Guo, L.; Rohde, J.; Farraye, F.A. Stigma and disclosure in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2020, 26, 1010–1016. [Google Scholar] [CrossRef]
- Fourie, S.; Jackson, D.; Aveyard, H. Living with inflammatory bowel disease: A review of qualitative research studies. Int. J. Nurs. Stud. 2018, 87, 149–156. [Google Scholar] [CrossRef]
- Cook, J.E.; Purdie-Vaughns, V.; Meyer, I.H.; Busch, J.T. Intervening within and across levels: A multilevel approach to stigma and public health. Soc. Sci. Med. 2014, 103, 101–109. [Google Scholar] [CrossRef]
- Kohut, S.A.; Stinson, J.; Jelen, A.; Ruskin, D. Feasibility and Acceptability of a Mindfulness-Based Group Intervention for Adolescents with Inflammatory Bowel Disease. J. Clin. Psychol. Med. Settings 2020, 27, 68–78. [Google Scholar] [CrossRef]
- Wynne, B.; McHugh, L.; Gao, W.; Keegan, D.; Byrne, K.; Rowan, C.; Mulcahy, H.E. Acceptance and commitment therapy reduces psychological stress in patients with inflammatory bowel diseases. Gastroenterology 2019, 156, 935–945. [Google Scholar] [CrossRef] [Green Version]
- Gerson, M.J.; Gerson, C.D. A collaborative family-systemic approach to treating chronic illness: Irritable bowel syndrome as exemplar. Contemp. Fam. Ther. 2005, 27, 37–49. [Google Scholar] [CrossRef]
- McCombie, A.; Gearry, R.; Mulder, R. Preferences of inflammatory bowel disease patients for computerised versus face-to-face psychological interventions. J. Crohn’s Colitis 2014, 8, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulson, N.S. How do online patient support communities affect the experience of inflammatory bowel disease? An online survey. JRSM Short Rep. 2013, 4, e2042533313478004. [Google Scholar] [CrossRef] [PubMed]
- Angelberger, S.; Vogelsang, H.; Novacek., G.; Miehsler, W.; Dejaco, C.; Gamgl, A.; Reinisch, W. Public awareness of Crohn’s disease and ulcerative colitis: A national survey. J. Crohn’s Colitis 2009, 3, 157–161. [Google Scholar] [CrossRef]
- Michaels, P.; Corrigan, P.W.; Buchholz, B.; Brown, J.; Arthur, T.; Netter, C.; Macdonald-Wilson, K.L. Changing Stigma through a Consumer-Based Stigma Reduction Program. Community Ment. Health J. 2014, 50, 395–401. [Google Scholar] [CrossRef]
- Pinfold, V.; Toulmin, H.; Thornicroft, G.; Huxley, P.; Farmer, P.; Graham, T. Reducing psychiatric stigma and discrimination: Evaluation of educational interventions in UK secondary schools. Br. J. Psychiatry 2018, 182, 342–346. [Google Scholar] [CrossRef]
- Salazar, G.; Barker, J.C.; Heyman, M.B. Medical students’ conceptualizations of quality of life associated with children who have Inflammatory Bowel Disease. J. Pediatric Gastroenterol. Nutr. 2013, 57, 493. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.T.; Siegel, C.A.; Kane, S.V.; Binion, D.G.; Panaccione, R.; Dubinsky, M.C.; Loftus, E.V.; Hopper, J. Impact of Ulcerative Colitis from Patients’ and Physicians’ Perspectives: Results from the UC: NORMAL survey. Inflamm. Bowel Dis. 2009, 15, 581–588. [Google Scholar] [CrossRef]
- Greenwood, K.; Carroll, C.; Crowter, L.; Jamieson, K.; Ferraresi, L.; Jones, A.M.; Brown, R. Early intervention for stigma towards mental illness? Promoting positive attitudes towards severe mental illness in primary school children. J. Public Ment. Health. 2016, 5, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Müller, K.E.; Lakatos, P.L.; Papp, M.; Veres, G. Incidence and Paris classification of pediatric Inflammatory Bowel Disease. Gastroenterol. Res. Pract. 2014, 2014, 904307. [Google Scholar] [CrossRef]
- Dubinsky, M. Special issues in paediatric inflammatory bowel disease. World J. Gastroenterol. 2008, 21, 413–420. [Google Scholar]
- Blakemore, S.J.; Mills, K.L. Is adolescence a sensitive period for sociocultural processing? Annu. Rev. Psychol. 2014, 65, 187–207. [Google Scholar] [CrossRef]
- Gamwell, K.L.; Baudino, M.N.; Bakula, D.M.; Sharkey, C.M.; Roberts, C.M.; Grunow, J.E.; Noel, J.; Jacobs, N.J.; Gillaspy, S.R.; Mullins, L.L.; et al. Perceived illness stigma, thwarted belongingness, and depressive symptoms in youth with inflammatory bowel disease (IBD). Inflamm. Bowel Dis. 2018, 24, 960–965. [Google Scholar] [CrossRef]

{kind=link}
| IBD | Experience | Qualitative |
|---|---|---|
| “Inflammatory Bowel Disease” “Colitis, Ulcerative” “Crohn Disease” colitis[Title/Abstract] crohn*[Title/Abstract] | Experience*[Text Word] Perspective*[Text Word] “living with”[Title/Abstract] life[Title/Abstract] influence[Title/Abstract] impact[Title/Abstract] effect[Title/Abstract] | Interview*[All Fields] qualitative[All Fields] themes[All Fields] |
| Author and Date | Location of Research | Population and Number | Aim of Study | Data Collection | Data Analysis * | Results/Findings |
|---|---|---|---|---|---|---|
| Alexakis et al. (2015) [54] | UK | Young people with IBD from BME groups (16–24 yrs) n = 20 | To identify and characterise the experiences (positive and negative) and difficulties faced by young IBD patients from BME communities. | Semi-structured interviews. | Thematic analysis. | Four themes: Culture and religion Parents, families, and the wider community Education Healthcare services and support |
| Barned et al. (2016) [40] | Canada | Children and adolescents with IBD (10–17 yrs) n = 25 | To determine how children and adolescents with IBD go about deciding if and when to tell others about their illness. | Semi-structured interviews. | Thematic analysis. | Three themes: To disclose or conceal: making the decision When to tell: factors influencing disclosure decisions
Challenges of IBD disclosure: the reactions of others |
| Brydolf and Segesten (1996) [52] | Sweden | Adolescents and young adults with UC (11–31 yrs) n = 28 | To gain a deeper understanding of the adolescents’ experiences of how it felt to live with UC. | Interviews. | Constant comparative method for grounded theory. | Eight categories: Alienation Reduced living space Support Lack of support Confidence in self Disbelief in self Role identification as a child/patient Role identification as an adult |
| Carter et al. (2020) [55] | UK | Young people with IBD (14–25 yrs) n = 31 | Exploring stigma and disclosure in young people with IBD. | Interviews, friendship maps, and photographs. | Interpretive description. | Three themes: To tell or not to tell Controlling the flow: the who, when, what, and how of telling Reactions and responses to telling: anticipated and actual |
| Cho et al. (2018) [56] | Canada | Young adults with IBD (18–30 yrs) n = 21 | To identify the health-related quality of life needs of young adults with IBD. | Interviews. | Constant comparative method. | Four broad categories of needs: Psychosocial needs Informational needs Self-advocacy needs Daily living needs |
| Cooper et al. (2010) [57] | UK | Adults with IBD (30–40 yrs) n = 24 | To explore beliefs about personal control and self-management of IBD. | Semi-structured interviews. | Systematic framework analysis. | One main theme: Reconciliation of the self in IBD Three sub-themes: Living with uncertainties and contradictions I’ve got it or it’s got me Evaluating images of me and health |
| Czuber-Dochan et al. (2012) [58] | UK | Adults with IBD (27–80 yrs) n = 46 | To explore fatigue, its impact on daily life and the strategies used to ameliorate the symptom, as described by people with IBD. | Focus group interviews. | Inductive thematic framework. | Five themes: The experience of fatigue Causes of fatigue Managing fatigue Consequences of fatigue Seeking support |
| Czuber-Dochan et al. (2020) [59] | UK | Adults with IBD (17–63 yrs) n = 28 | To address unmet needs regarding psychosocial aspects of food, eating, and drinking in IBD. | Semi-structured interviews. | Colaizzi’s framework. | Five themes: Personal experience of relationship between IBD and food Managing diet to control IBD and its symptoms Impact of food-related issues on everyday life Acceptance and normalisation of food and its impact in IBD Sources of information and support |
| Daniel (2002) [43] | Canada | Young adults with IBD (18–24 yrs) n = 5 | To expand awareness and enhance empirical understanding of the young adult IBD patient’s perspective of living with IBD. | Semi-structured interviews. | Descriptive phenomenological method. | Themes in the study compared with King’s concepts in the Personal System, Interpersonal System and Social System |
| Demirtas (2021) [41] | Turkey | Adults with IBD (25–58 yrs) n = 25 | To determine the life experiences of patients with IBD. | Semi-structured interviews. | Phenomenological method. | Three main themes: A flare phase of the disease A remission period Coping behaviours |
| Devlen et al. (2014) [44] | USA | Adult with IBD (20–59 yrs) n = 27 | To describe the impacts of IBD from a patient perspective. | Focus groups and individual interviews. | Grounded theory. | A conceptual model of impacts including: Immediate impacts Lifestyle impacts Impacts of daily activities Impacts on social and leisure activities Treatment impacts Psychological impacts Impacts on relationships |
| Dibley et al. (2014) [29] | UK | Gay and lesbian people (GLP) with IBD (27–54 yrs) n = 22 | To explore the parallels between coming out about sexual identity and IBD in order to compare GLP IBD-related concerns with those in the non-gay IBD community and to identify the social and psychological aspects of IBD in GLP. | Semi-structured interviews. | Pragmatic thematic analysis. | Four central themes: GL sexual activity Receiving health care IBD and GL life Identity and coming out |
| Dibley et al. (2018) [23] | UK | Adults with IBD (23–78 yrs) n = 40 | To explore the lived experience of stigma in IBD. | Unstructured interviews. | Interpretive hermeneutic phenomenological analysis. | Three constitutive patterns: Being in and out of control Relationships and social support Mastery and mediation |
| Dibley et al. (2019) [28] | UK | Adults with IBD (21 – 64 yrs) n = 18 | An exploration of the experience and meaning of kinship stigma in people with IBD. | Unstructured interviews. | Interpretive hermeneutic phenomenological analysis. | Three relational themes: Being Visible/Becoming Invisible Being the Disease/Having the Disease Amplification, Suffering, and Loss Constitutive Pattern: Lacking Acknowledgment/Being Acknowledged |
| Dudley-Brown (1996) [42] | Hong Kong | Adults with UC (30–58 yrs) n = 3 | To describe real life experiences of patients with UC. | Semi-structured interviews. | Phenomenological analysis. | Five themes: Uncertainty surrounding the length of time between exacerbations of symptoms Fear and humiliation accompanying stool incontinence The desperate need to find successful treatment and return to normal life The profound effect of family life, social life, and work The feeling of being controlled by the disease |
| Frohlich (2014) [30] | USA | Adults with IBD (20–56 yrs) n = 14 | To understand how people with IBD experience stigma because of their disease. | Semi-structured interviews. | Identification of common themes. | Six potentially stigmatising illness sites: Initial diagnosis Romantic relationships Work and school Surgery Medicine Overt stigma |
| García-Sanjuán, et al. (2017) [45] | Spain | Adults with CD (25–83 yrs) n = 19 | To understand the lived experience of CD. | Interviews. | Colaizzi’s framework. | Five themes: Self-protection against the unknown cause self-training Learning to live with CD Perceived losses associated to CD Relationship with others |
| Hall et al. (2005) [60] | UK | Adults with IBD (28–79 yrs) n = 31 | To gain a better understanding of the perspectives and experiences of individuals with IBD and a poor quality of life. | Individual semi-structured interviews and focus groups. | Grounded theory. | Emergent core concept: ‘Health-related normality’ |
| Jordan et al. (2017) [61] | UK | Adults with IBD (22–68 yrs) n = 25 | To explore the experience of people with IBD and elevated symptoms of anxiety and low mood and the type of psychological help they would like. | Semi-structured interviews. | Template analysis. | Two themes related to anxiety: under performance; preventing an accident Two themes related to low mood: lack of understanding; stigma One main theme for type of psychological help desired: Expertise and understanding |
| Larsson et al. (2016) [62] | Sweden | Adults with IBD (29–63 yrs) n = 15 | To investigate the specific disease-related stress in individuals with IBD, how they cope with this stress and what help is requested from the healthcare. | Interviews. | Content analysis. | Three central areas: Stress: disease-related stress and relations to others Coping: behavioural strategies, social strategies and emotional strategies Need for help or support: instrumental support and emotional support. |
| Lynch and Spence (2008) [46] | New Zealand | Adolescents and young adults with CD (16–21 yrs) n = 4 | To explore how youth experience living with recently diagnosed CD. | Semi-structured interviews. | Thematic analysis. | Three themes: Stress as integral to living with CD The paradoxical relationship between fear and hope What helps and what hinders |
| Matini and Ogden (2016) [47] | UK | Adults with IBD (18–39 yrs) n = 22 | To explore the notion of adaptation in patients with IBD. | Semi-structured interviews. | Thematic analysis. | Three core themes: Making sense of the illness Impact Feelings Overarching theme: Uncertainty |
| Mikocka-Walus et al. (2020) [53] | UK (n = 13) and Australia (n = 11) | Adults with IBD (20–70 yrs) n = 24 | To explore the lived experience and healthcare needs of patients with IBD and mild-to-moderate comorbid anxiety and/or depression. | Semi-structured interviews and focus groups. | Thematic analysis (UK) and template analysis (Australia) | Three UK themes: Bidirectional relationship between IBD and mental health, Need for healthcare integration Lack of awareness about the disease Three Australia themes: The ‘vicious cycle’ of IBD and psychosocial health The need for biopsychosocial healthcare integration and The stigma of a hidden disease |
| Moore (2013) [63] | UK | Adult with UC (20 yrs) n = 1 | To document the author’s lived experience while in the midst of an acute flare-up of UC. | Journal logs. | Autoethnography. | Reflection upon the influence of illness on an athletic body within a sporting subculture. |
| Mukherjee et al. (2002) [48] | UK | Parents with IBD (26–54 yrs) n = 24 | To identify parents’ views on how IBD affects people in their parenting role; effects parents with IBD have noticed in their children; ways of dealing with any difficulties in parenting; support needed by parents with IBD. | Individual interviews and focus groups. | Framework approach. | Five main themes: Effects on parents Effects on children Ways of dealing with difficulties Support received from services Messages for service providers |
| Nicholas et al. (2007) [49] | Canada | Children and adolescents with IBD (7–19 yrs) n = 80 | To understand the lived experience and elements of quality of life as depicted by children and adolescents with IBD. | Semi-structured interview. | Content analysis. | Five themes: Concerns relating to IBD symptoms and treatments Vulnerability and lack of control Perceiving the self negatively as different than peers Benefits of social support Personal resources in coping |
| Norton et al. (2012) [39] | USA | Adults with CD (18–75 yrs) n = 48 | To understand the impact of CD on various aspects of daily life from the perspective of patients living with CD. | Video diaries and focus groups. | Descriptive summaries. | Impact of CD on various aspects of life: General impact of CD Relationship with provider Psychological impact of CD Social impact of CD Impact of CD on activities Impact of CD on professional life |
| Nutting and Grafsky (2017) [64] | USA | Five adult heterosexual couples with CD (28–40 yrs) n = 10 | To understand how a partner’s diagnosis of CD is perceived to affect couple relationship functioning and satisfaction, as well as young adult life-cycle transitions. | Interviews (each partner interviewed individually). | Interpretive phenomenological analysis. | Four areas of experiences: Diagnosis Biopsychosocial wellbeing Relationship functioning and satisfaction Life-cycle transitions |
| Lesnovska et al. (2010) [65] | Sweden | Adults with CD (29–83 yrs) n = 11 | To identify and describe the meaning of quality of life in patients with CD. | Interviews. | Grounded theory. | Five dominant themes: Self-image Confirmatory relations Powerlessness Attitude toward life Sense of well-being |
| Lesnovska et al. (2016) [66] | Sweden | Adults with IBD (29–83 yrs) n = 30 | To describe how patients living with IBD experience critical incidents in daily life in relation to their disease and symptoms. | Interviews. | Critical incident technique (inductive). | Five categories: Losing bowel control Having a body that smells Being unable to meet own and others’ expectations Not being believed or seen Experiencing frustration due to side effects and ineffective treatment. One main area describing the overall result: The bowels rule life |
| Purc-Stephenson et al. (2014) [50] | Canada | Adults with IBD (18–62 yrs) n = 378 | To explore the positive and negative changes patients with IBD have experienced since diagnosis. | Online survey. | Grounded theory. | Five themes related to positive changes: Interpersonal Relations, Personal Growth, Valuing Life, New Life Paths, and Spiritual Growth. Three themes related to negative changes: Freedom Restrictions, Psychological Side Effects, and Social Isolation |
| Richard et al. (2020) [51] | New Zealand | Adults with IBD (30–79 yrs) n = 18 | To explore how adults living with IBD in rural New Zealand manage their condition and engage with healthcare providers. | Semi-structured interviews. | Thematic analysis. | Five constructs: Journey to confirming and accepting diagnosis Importance of the relationship with the healthcare team Support from others Learning how to manage IBD Care at a distance |
| Ruan et al. (2020) [67] | China | Adults with IBD (21–58 yrs) n = 16 | To explore the experiences of body image changes in patients with IBD in China and to describe how those changes influence patients’ perception of body and self. | Semi-structured interviews. | Content analysis. | Six themes: Being a constrained person Being a flawed person Being a disliked person Being an alienated person Being a reconciled person Being a blessed person |
| Ruan and Zhou (2019) [68] | China | Adults with CD (19–68 yrs) n = 31 | To explore the illness experiences of patients with CD in China and construct an interpretive understanding of these experiences from the perspective of the patients. | Interviews. | Grounded theory. | Four categories: Comparing Struggling Reflecting Realising One core category: Regaining normality |
| Sammut et al. (2015) [69] | Malta | Adults with UC (29–60 yrs) n = 10 | To explore the experiences of adults living with UC. | Semi-structured interviews. | Interpretative phenomenological analysis. | Three super-ordinate themes: Living with physical discomfort Emotional turmoil in living the experience Social interactions |
| Saunders (2014) [31] | UK | Adults with IBD (18–29 yrs) n = 16 | To explore how stigma is discursively constructed by young adults, with a focus on the moral underpinnings of the participants’ talk. | Semi-structured interviews. | Rhetorical discourse analysis. | Representations showed both felt stigma and enacted stigma; principally related to the perceived taboo surrounding the symptoms of their condition, which often led to the non-disclosure or concealment of the condition |
| Vejzovic et al. (2018) [70] | Sweden | Adolescents with UC (13–18 yrs) n = 7 | To illuminate the meaning of children’s lived experience of UC. | Interviews. | Phenomenological hermeneutical method. | One main theme: Daily struggle to adapt and be perceived as normal Four subthemes: Being healthy despite the symptoms Being healthy despite being afraid Being healthy despite a sense of being different Being healthy despite needing support |
| Wilburn et al. (2017) [71] | UK | Adults with CD (25–68 yrs) n = 30 | To understand how the lives of people with CD are affected. | Interviews. | Theoretical thematic analysis. | Thirteen main need themes: Nutrition, hygiene, continence, freedom from infection, security, self-esteem, role, attractiveness, relationships, intimacy, clear-mindedness, pleasure, and autonomy |
| Category | Theme | Overarching Concept |
|---|---|---|
| The IBD journey | Reduced to a label The spoiled self Re-building the self | Feeling of Otherness |
| A need to be understood | A shameful secret Knowing is not understanding Social estrangement The freedom of authenticity |
| The IBD Journey | A Need to Be Understood | ||||||
|---|---|---|---|---|---|---|---|
| Author and Date | Reduced to a Label | The Spoiled Self | Re-Building the Self | A Shameful Secret | Knowing Is Not Understanding | Social Estrangement | The Freedom of Authenticity |
| Alexakis et al. (2015) [54] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Barned et al. (2016) [40] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Brydolf and Segesten (1996) [52] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Carter et al. (2020) [55] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Cho et al. (2018) [56] | ✓ | ✓ | ✓ | ✓ | |||
| Cooper et al. (2010) [57] | ✓ | ✓ | ✓ | ✓ | |||
| Czuber-Dochan et al. (2012) [58] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Czuber-Dochan et al. (2020) [59] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Daniel (2002) [43] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Demitras (2021) [41] | ✓ | ✓ | ✓ | ✓ | |||
| Devlen et al. (2014) [44] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Dibley et al. (2014) [29] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Dibley et al. (2018) [23] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Dibley et al. (2020) [28] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Dudley-Brown (1996) [42] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Frohlich (2014) [30] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| García-Sanjuán et al. (2017) [45] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Hall et al. (2005) [60] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Jordan et al. (2017) [61] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Larsson et al. (2016) [62] | ✓ | ✓ | ✓ | ✓ | |||
| Lynch and Spence (2008) [46] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Matini and Ogden (2016) [47] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Mikocka-Walus et al. (2020) [53] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Moore (2013) [63] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Mukherjee et al. (2002) [48] | ✓ | ✓ | ✓ | ✓ | |||
| Nicholas et al. (2007) [49] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Norton et al. (2012) [39] | ✓ | ✓ | ✓ | ✓ | |||
| Nutting and Grafsky (2017) [64] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Lesnovska et al. (2010) [65] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Lesnovska et al. (2016) [66] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Purc-Stephenson et al. (2014) [50] | ✓ | ✓ | ✓ | ✓ | |||
| Richard et al. (2020) [51] | ✓ | ✓ | ✓ | ||||
| Ruan et al. (2020) [67] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Ruan and Zhou (2019) [68] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sammut et al. (2015) [69] | ✓ | ✓ | ✓ | ||||
| Saunders (2014) [31] | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Vejzovic et al. (2018) [70] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Wilburn et al. (2017) [71] | ✓ | ✓ | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muse, K.; Johnson, E.; David, A.L. A Feeling of Otherness: A Qualitative Research Synthesis Exploring the Lived Experiences of Stigma in Individuals with Inflammatory Bowel Disease. Int. J. Environ. Res. Public Health 2021, 18, 8038. https://doi.org/10.3390/ijerph18158038
Muse K, Johnson E, David AL. A Feeling of Otherness: A Qualitative Research Synthesis Exploring the Lived Experiences of Stigma in Individuals with Inflammatory Bowel Disease. International Journal of Environmental Research and Public Health. 2021; 18(15):8038. https://doi.org/10.3390/ijerph18158038
Chicago/Turabian StyleMuse, Kate, Emma Johnson, and Annabel L. David. 2021. "A Feeling of Otherness: A Qualitative Research Synthesis Exploring the Lived Experiences of Stigma in Individuals with Inflammatory Bowel Disease" International Journal of Environmental Research and Public Health 18, no. 15: 8038. https://doi.org/10.3390/ijerph18158038
APA StyleMuse, K., Johnson, E., & David, A. L. (2021). A Feeling of Otherness: A Qualitative Research Synthesis Exploring the Lived Experiences of Stigma in Individuals with Inflammatory Bowel Disease. International Journal of Environmental Research and Public Health, 18(15), 8038. https://doi.org/10.3390/ijerph18158038