
Association of X-ray Absorptiometry Body Composition Measurements with Basic Anthropometrics and Mortality Hazard



Abstract
1. Introduction
2. Methods
2.1. NHANES
2.2. Indices and Standardization
2.3. Statistical Modeling of Association with Mortality
3. Results
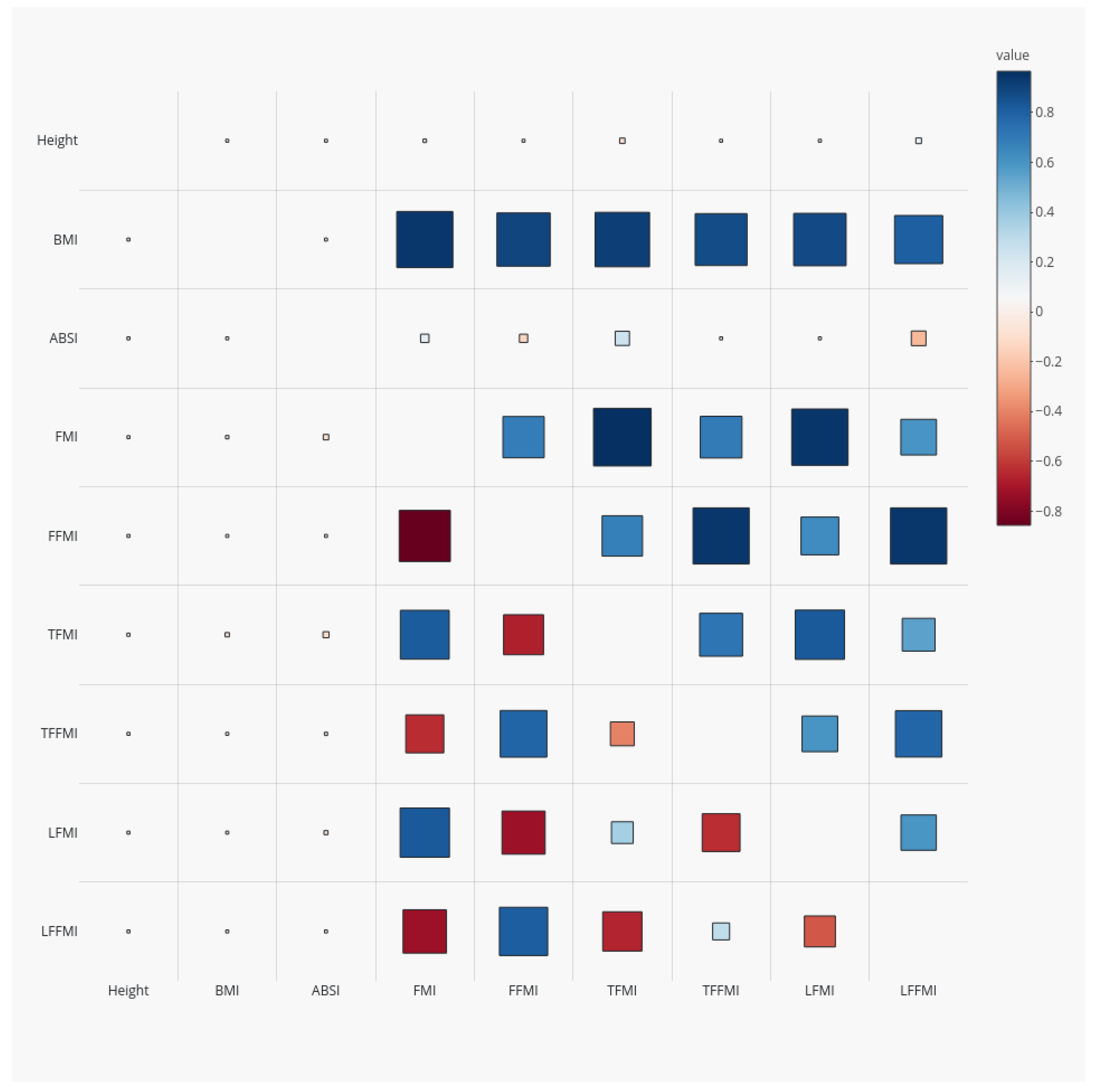
3.1. Sample Characteristics and Correlations
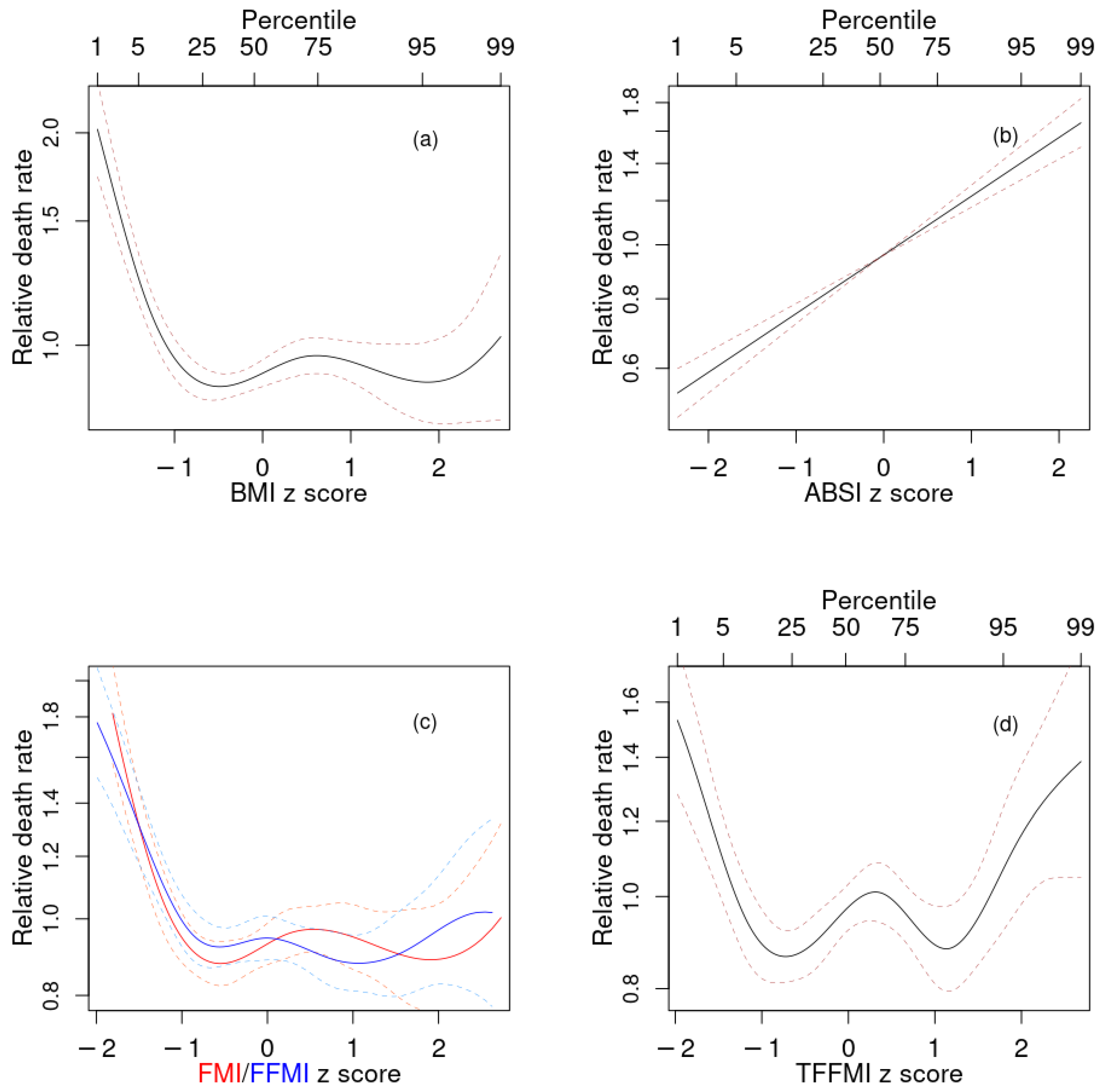
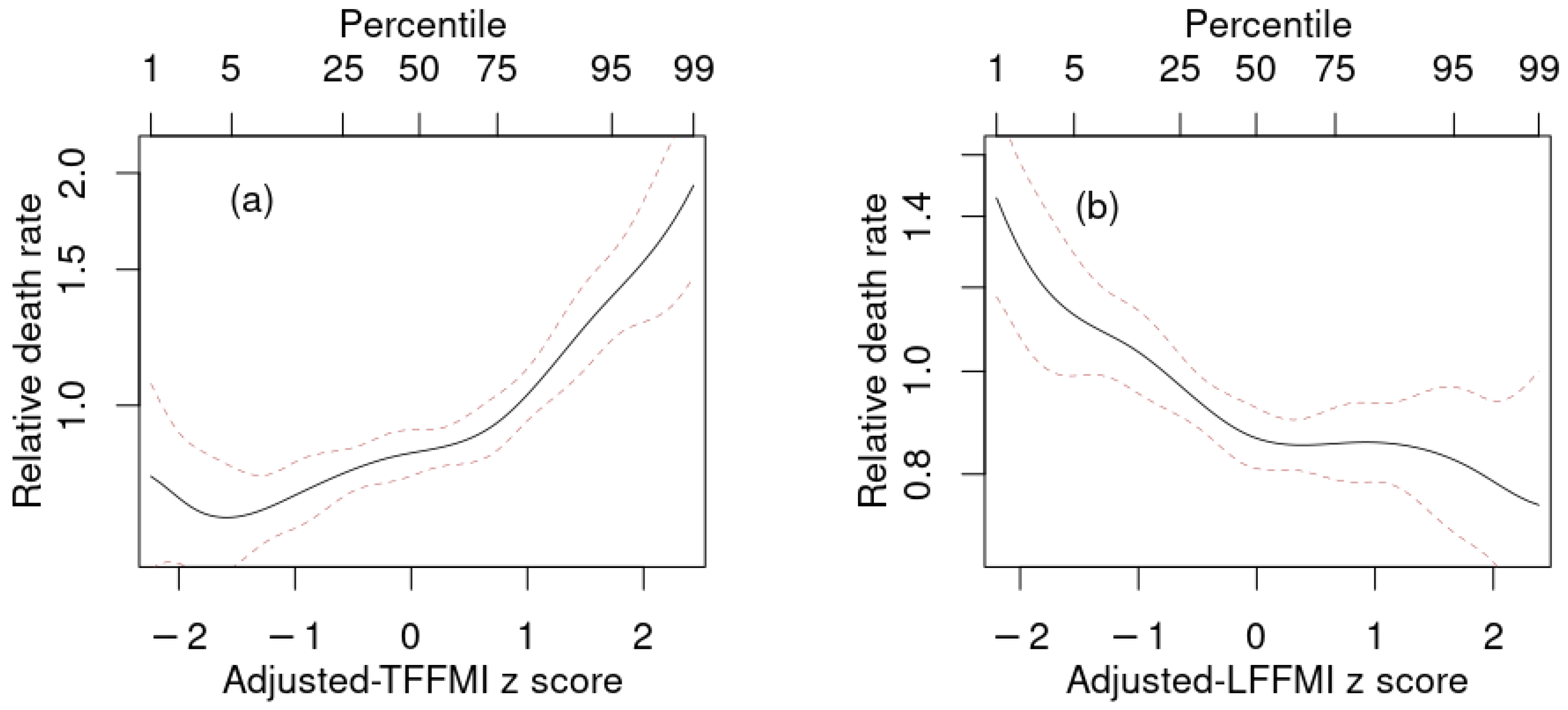
3.2. Associations with Mortality Hazard
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ji, M.; Zhang, S.; An, R. Effectiveness of A Body Shape Index (ABSI) in predicting chronic diseases and mortality: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 737–759. [Google Scholar] [CrossRef]
- Christakoudi, S.; Tsilidis, K.K.; Muller, D.C.; Freisling, H.; Weiderpass, E.; Overvad, K.; Söderberg, S.; Häggström, C.; Pischon, T.; Dahm, C.C.; et al. A Body Shape Index (ABSI) achieves better mortality risk stratification than alternative indices of abdominal obesity: Results from a large European cohort. Sci. Rep. 2020, 10, 14541. [Google Scholar] [CrossRef]
- Snijder, M.; van Dam, R.; Visser, M.; Seidell, J. What aspects of body fat are particularly hazardous and how do we measure them? Int. J. Epidemiol. 2006, 35, 83. [Google Scholar] [CrossRef]
- Ahima, R.S.; Lazar, M.A. The health risk of obesity—better metrics imperative. Science 2013, 341, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Giovannucci, E.L. Body composition and mortality in the general population: A review of epidemiologic studies. Exp. Biol. Med. 2018, 243, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Hulkoti, V.S.; Acharya, S.; Shukla, S.; Partapa, S.K.; Gupte, Y. In search of an ideal obesity assessment tool: Is body mass index reliable enough? J. Evol. Med. Dent. Sci. 2020, 9, 2556–2560. [Google Scholar] [CrossRef]
- Frank, A.P.; de Santos, R.S.; Palmer, B.F.; Clegg, D.J. Determinants of body fat distribution in humans may provide insight about obesity-related health risks. J. Lipid Res. 2019, 60, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.A.; Ng, B.K.; Sommer, M.J.; Heymsfield, S.B. Body composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Ponti, F.; Santoro, A.; Mercatelli, D.; Gasperini, C.; Conte, M.; Martucci, M.; Sangiorgi, L.; Franceschi, C.; Bazzocchi, A. Aging and imaging assessment of body composition: From fat to facts. Front. Endocrinol. 2020, 10, 861. [Google Scholar] [CrossRef] [PubMed]
- Laskey, M. Dual-energy X-ray absorptiometry and body composition. Nutrition 1996, 12, 45–51. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Formica, C.; Wang, Z.; Heymsfield, S.B. Dual-energy X-ray absorptiometry body composition model: Review of physical concepts. Am. J. Physiol. Endocrinol. Metab. 1996, 271, E941–E951. [Google Scholar] [CrossRef]
- Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual energy X-ray absorptiometry body composition reference values from NHANES. PLoS ONE 2009, 4, e7038. [Google Scholar] [CrossRef]
- Hinton, B.J.; Fan, B.; Ng, B.K.; Shepherd, J.A. Dual energy X-ray absorptiometry body composition reference values of limbs and trunk from NHANES 1999–2004 with additional visualization methods. PLoS ONE 2017, 12, e0174180. [Google Scholar] [CrossRef] [PubMed]
- Zong, G.; Zhang, Z.; Yang, Q.; Wu, H.; Hu, F.B.; Sun, Q. Total and regional adiposity measured by dual-energy X-ray absorptiometry and mortality in NHANES 1999–2006. Obesity 2016, 24, 2414–2421. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Defining cutoffs to diagnose obesity using the relative fat mass (RFM): Association with mortality in NHANES 1999–2014. Int. J. Obes. 2020, 44, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Sedlmeier, A.M.; Baumeister, S.E.; Weber, A.; Fischer, B.; Thorand, B.; Ittermann, T.; Dörr, M.; Felix, S.B.; Völzke, H.; Peters, A.; et al. Relation of body fat mass and fat-free mass to total mortality: Results from 7 prospective cohort studies. Am. J. Clin. Nutr. 2021, 113, 639–646. [Google Scholar] [CrossRef]
- Wilson, J.P.; Kanaya, A.M.; Fan, B.; Shepherd, J.A. Ratio of trunk to leg volume as a new body shape metric for diabetes and mortality. PLoS ONE 2013, 8, e68716. [Google Scholar] [CrossRef]
- Abramowitz, M.K.; Hall, C.B.; Amodu, A.; Sharma, D.; Androga, L.; Hawkins, M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study. PLoS ONE 2018, 13, e0194697. [Google Scholar] [CrossRef]
- Van Aller, C.; Lara, J.; Stephan, B.C.; Donini, L.M.; Heymsfield, S.; Katzmarzyk, P.T.; Wells, J.C.; Prado, C.M.; Siervo, M. Sarcopenic obesity and overall mortality: Results from the application of novel models of body composition phenotypes to the National Health and Nutrition Examination Survey 1999–2004. Clin. Nutr. 2019, 38, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Xie, X.; Dou, Q.; Liu, C.; Zhang, W.; Yang, Y.; Deng, R.; Cheng, A.S.K. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: A updated meta-analysis. BMC Geriatr. 2019, 19, 183. [Google Scholar] [CrossRef] [PubMed]
- Biolo, G.; Di Girolamo, F.G.; Breglia, A.; Chiuc, M.; Baglio, V.; Vinci, P.; Toigo, G.; Lucchin, L.; Jurdana, M.; Mazzucco, S.; et al. Inverse relationship between “a body shape index” (ABSI) and fat-free mass in women and men: Insights into mechanisms of sarcopenic obesity. Clin. Nutr. 2015, 34, 323–327. [Google Scholar] [CrossRef]
- Dhana, K.; Koolhas, C.; Schoufour, J.; Rivadeneira, F.; Hofman, A.; Kavousi, M.; Franco, O.H. Association of anthropometric measures with fat and fat-free mass in the elderly: The Rotterdam study. Maturitas 2016, 88, 96–100. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. An Anthropometric Risk Index based on combining height, weight, waist, and hip measurements. J. Obes. 2016, 2016, 8094275. [Google Scholar] [CrossRef]
- Chung, W.; Park, J.H.; Chung, H.S.; Yu, J.M.; Kim, D.S.; Moon, S. Utility of the Z-score of log-transformed A Body Shape Index (LBSIZ) in the assessment for sarcopenic obesity and cardiovascular disease risk in the United States. Sci. Rep. 2019, 9, 9292. [Google Scholar] [CrossRef]
- NHANES. National Health and Nutrition Examination Survey Technical Documentation for the 1999–2004 Dual Energy X-ray Absorptiometry (DXA) Multiple Imputation Data Files; Technical Report; National Center for Health Statistics: 2008. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/dxa/dxa_techdoc.pdf (accessed on 8 June 2021).
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. J. Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- VanItallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef]
- Schutz, Y.; Kyle, U.; Pichard, C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18–98 y. Int. J. Obes. 2002, 26, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.R. Partial likelihood. Biometrika 1975, 62, 269–276. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. Anthropometrics, metabolic syndrome, and mortality hazard. J. Obes. 2018, 2018, 9241904. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. Dynamic association of mortality hazard with body shape. PLoS ONE 2014, 9, e88793. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. Association of body shape index (ABSI) with hand grip strength. Int. J. Environ. Res. Public Health 2020, 17, 6797. [Google Scholar] [CrossRef] [PubMed]
- Burnham, K.P.; Anderson, D.R. Multimodel inference: Understanding AIC and BIC in model selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Royston, P. Explained variation for survival models. Stata J. 2006, 6, 83–96. [Google Scholar] [CrossRef]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Heagerty, P.J.; Lumley, T.; Pepe, M.S. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics 2000, 56, 337–344. [Google Scholar] [CrossRef]
- Pantoja-Galicia, N.; Okereke, O.I.; Blacker, D.; Betensky, R.A. Concordance measures and time-dependent ROC methods. Biostat. Epidemiol. 2021, 1–18. [Google Scholar] [CrossRef]
- Hurvich, C.M.; Simonoff, J.S.; Tsai, C.L. Smoothing parameter selection in nonparametric regression using an improved Akaike information criterion. J. R. Stat. Soc. 1998, 60B, 271–293. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Therneau, T.M. A Package for Survival Analysis in R; R Package Version 3.2-7; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Krakauer, J.C.; Franklin, B.; Kleerekoper, M.; Karlsson, M.; Levine, J.A. Body composition profiles derived from dual-energy X-ray absorptiometry total body scan and mortality. Prev. Cardiol. 2004, 7, 109–115. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. Untangling waist circumference and hip circumference from body mass index with a body shape index, hip index, and anthropometric risk indicator. Metab. Syndr. Relat. Disord. 2018, 16, 160–165. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. The new anthropometrics and abdominal obesity: A body shape index, hip index, and anthropometric risk index. In Nutrition in the Prevention and Treatment of Abdominal Obesity, 2nd ed.; Watson, R.R., Ed.; Academic Press: Cambridge, MA, USA, 2019; Chapter 2; pp. 19–27. [Google Scholar] [CrossRef]
- Achamrah, N.; Colange, G.; Delay, J.; Rimbert, A.; Folope, V.; Petit, A.; Grigioni, S.; Déchelotte, P.; Coëffier, M. Comparison of body composition assessment by DXA and BIA according to the body mass index: A retrospective study on 3655 measures. PLoS ONE 2018, 13, e0200465. [Google Scholar] [CrossRef]
- Zhou, W.; Eckler, S.; Barszczyk, A.; Waese-Perlman, A.; Wang, Y.; Gu, X.; Feng, Z.P.; Peng, Y.; Lee, K. Waist circumference prediction for epidemiological research using gradient boosted trees. BMC Med. Res. Methodol. 2021, 21, 47. [Google Scholar] [CrossRef]
- Porter, S.A.; Massaro, J.M.; Hoffmann, U.; Vasan, R.S.; O’Donnel, C.J.; Fox, C.S. Abdominal Subcutaneous Adipose Tissue: A Protective Fat Depot? Diabetes Care 2009, 32, 1068–1075. [Google Scholar] [CrossRef]
- Dulloo, A.G.; Jacquet, J.; Solinas, G.; Montani, J.P.; Schutz, Y. Body composition phenotypes in pathways to obesity and the metabolic syndrome. Int. J. Obes. 2010, 34, S4–S17. [Google Scholar] [CrossRef] [PubMed]
- Goossens, G.H. The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function. Obes. Facts 2017, 10, 207–215. [Google Scholar] [CrossRef]
- Justin, M.; Zaman, S.; Sanders, J.; Crook, A.M.; Feder, G.; Shipley, M.; Timmis, A.; Hemingway, H. Cardiothoracic ratio within the “normal” range independently predicts mortality in patients undergoing coronary angiography. Heart 2007, 93, 491–494. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ryu, H.; Kim, H.; Park, H.C.; Kim, H.; Cho, E.J.; Lee, K.B.; Chung, W.; Oh, K.H.; Cho, J.Y.; Hwang, Y.H.; et al. Total kidney and liver volume is a major risk factor for malnutrition in ambulatory patients with autosomal dominant polycystic kidney disease. BMC Nephrol. 2017, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Ghobrial, I.M.; Fonseca, R.; Gertz, M.A.; Plevak, M.F.; Larson, D.R.; Therneau, T.M.; Wolf, R.C.; Hoffmann, R.J.; Lust, J.A.; Witzig, T.E.; et al. Prognostic model for disease-specific and overall mortality in newly diagnosed symptomatic patients with Waldenstrom macroglobulinaemia. Br. J. Haematol. 2006, 133, 158–164. [Google Scholar] [CrossRef]
- Zaina, S.; Pettersson, L.; Thomsen, A.B.; Chai, C.M.; Qi, Z.; Thyberg, J.; Nilsson, J. Shortened life span, bradycardia, and hypotension in mice with targeted expression of an Igf2 transgene in smooth muscle cells. Endocrinology 2003, 144, 2695–2703. [Google Scholar] [CrossRef][Green Version]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Wells, J.C.K. The capacity–load model of non-communicable disease risk: Understanding the effects of child malnutrition, ethnicity and the social determinants of health. Eur. J. Clin. Nutr. 2018, 72, 688–697. [Google Scholar] [CrossRef]
- Christakoudi, S.; Evangelou, E.; Riboli, E.; Tsilidis, K.K. GWAS of allometric body-shape indices in UK Biobank identifies loci suggesting associations with morphogenesis, organogenesis, adrenal cell renewal and cancer. Sci. Rep. 2021, 11, 10688. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Farmer, R.E.; Mathur, R.; Schmidt, A.F.; Bhaskaran, K.; Fatemifar, G.; Eastwood, S.V.; Finan, C.; Denaxas, S.; Smeeth, L.; Chaturvedi, N. Associations between measures of sarcopenic obesity and risk of cardiovascular disease and mortality: A cohort study and Mendelian randomization analysis using the UK Biobank. J. Am. Heart Assoc. 2019, 8, e011638. [Google Scholar] [CrossRef]
- Zeng, Q.; Wang, L.; Dong, S.; Zha, X.; Ran, L.; Li, Y.; Chen, S.; Gao, J.; Li, S.; Lu, Y.; et al. CT-derived abdominal adiposity: Distributions and better predictive ability than BMI in a nationwide study of 59,429 adults in China. Metabolism 2021, 115, 154456. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Kim, Y.J.; Yu, J.M.; Kang, J.G.; Chung, H.S. Z-score of the log-transformed A Body Shape Index predicts low muscle mass in population with abdominal obesity: The U.S. and Korea National Health and Nutrition Examination Survey. PLoS ONE 2020, 15, e0242557. [Google Scholar] [CrossRef]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the Health, Aging and Body Composition Study cohort. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Valid DEXA Scans | All Adults | |
|---|---|---|
| Number | 14,064 | 19,959 |
| Deaths | 2140 | 3478 |
| % female | 48 | 52 |
| Ethnicity | Mexican: 25% | 24% |
| Other Hispanic: 4% | 4% | |
| White: 47% | 47% | |
| Black: 20% | 21% | |
| Other: 4% | 4% | |
| Age (y) | 43 ± 19 | 46 ± 20 |
| Height (cm) | 168 ± 10 | 167 ± 10 |
| Weight (kg) | 76 ± 17 | 79 ± 20 |
| BMI () | 27.1 ± 5.1 | 28.1 ± 6.3 |
| WC (cm) | 94 ± 14 | 96 ± 16 |
| ABSI () | 8.04 ± 0.52 | 8.10 ± 0.54 |
| FMI () | 9.2 ± 3.8 [8.6 ± 2.0] | |
| FFMI () | 18.1 ± 2.8 [17.9 ± 1.8] | |
| TFMI () | 4.5 ± 2.1 [4.1 ± 0.9] | |
| TFFMI () | 8.8 ± 1.3 [8.8 ± 0.9] | |
| LFMI () | 4.3 ± 1.9 [4.1 ± 1.3] | |
| LFFMI () | 8.0 ± 1.5 [7.8 ± 1.0] |
| Index | Height | BMI | ABSI | |
|---|---|---|---|---|
| FMI | −0.362 | 1.830 | 1.246 | 0.930 |
| FFMI | 0.140 | 0.611 | −0.364 | 0.912 |
| TFMI | −0.867 | 2.183 | 2.354 | 0.918 |
| TFFMI | 0.013 | 0.600 | −0.011 | 0.863 |
| LFMI | 0.202 | 1.666 | 0.423 | 0.882 |
| LFFMI | 0.491 | 0.672 | −0.764 | 0.879 |
| Predictor | C | ||
|---|---|---|---|
| Baseline | 0 | 0.031 | 0.567 |
| BMI | 79.3 | 0.056 | 0.581 |
| ABSI | 115.1 | 0.064 | 0.602 |
| FMI | 72.0 | 0.055 | 0.582 |
| FFMI | 46.8 | 0.047 | 0.585 |
| TFMI | 47.6 | 0.047 | 0.579 |
| TFFMI | 31.1 | 0.043 | 0.583 |
| LFMI | 80.3 | 0.057 | 0.586 |
| LFFMI | 99.7 | 0.061 | 0.598 |
| Predictor | C | ||
|---|---|---|---|
| BMI + ABSI | 195.2 | 0.088 | 0.615 |
| +FMI | 200.6 | 0.096 | 0.618 |
| +FFMI | 207.5 | 0.097 | 0.620 |
| +TFMI | 202.0 | 0.094 | 0.618 |
| +TFFMI | 255.6 | 0.110 | 0.627 |
| +LFMI | 200.9 | 0.097 | 0.620 |
| +LFFMI | 222.4 | 0.100 | 0.619 |
| +TFFMI + LFFMI | 317.6 | 0.130 | 0.635 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krakauer, N.Y.; Krakauer, J.C. Association of X-ray Absorptiometry Body Composition Measurements with Basic Anthropometrics and Mortality Hazard. Int. J. Environ. Res. Public Health 2021, 18, 7927. https://doi.org/10.3390/ijerph18157927
Krakauer NY, Krakauer JC. Association of X-ray Absorptiometry Body Composition Measurements with Basic Anthropometrics and Mortality Hazard. International Journal of Environmental Research and Public Health. 2021; 18(15):7927. https://doi.org/10.3390/ijerph18157927
Chicago/Turabian StyleKrakauer, Nir Y., and Jesse C. Krakauer. 2021. "Association of X-ray Absorptiometry Body Composition Measurements with Basic Anthropometrics and Mortality Hazard" International Journal of Environmental Research and Public Health 18, no. 15: 7927. https://doi.org/10.3390/ijerph18157927
APA StyleKrakauer, N. Y., & Krakauer, J. C. (2021). Association of X-ray Absorptiometry Body Composition Measurements with Basic Anthropometrics and Mortality Hazard. International Journal of Environmental Research and Public Health, 18(15), 7927. https://doi.org/10.3390/ijerph18157927