
Gender Differences in Depression and Sex Hormones among Patients Receiving Long-Term Opioid Treatment for Chronic Noncancer Pain in Taiwan—A Multicenter Cross-Sectional Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Instrument
2.3. Blood Hormone Tests
2.4. Statistical Analysis
3. Results
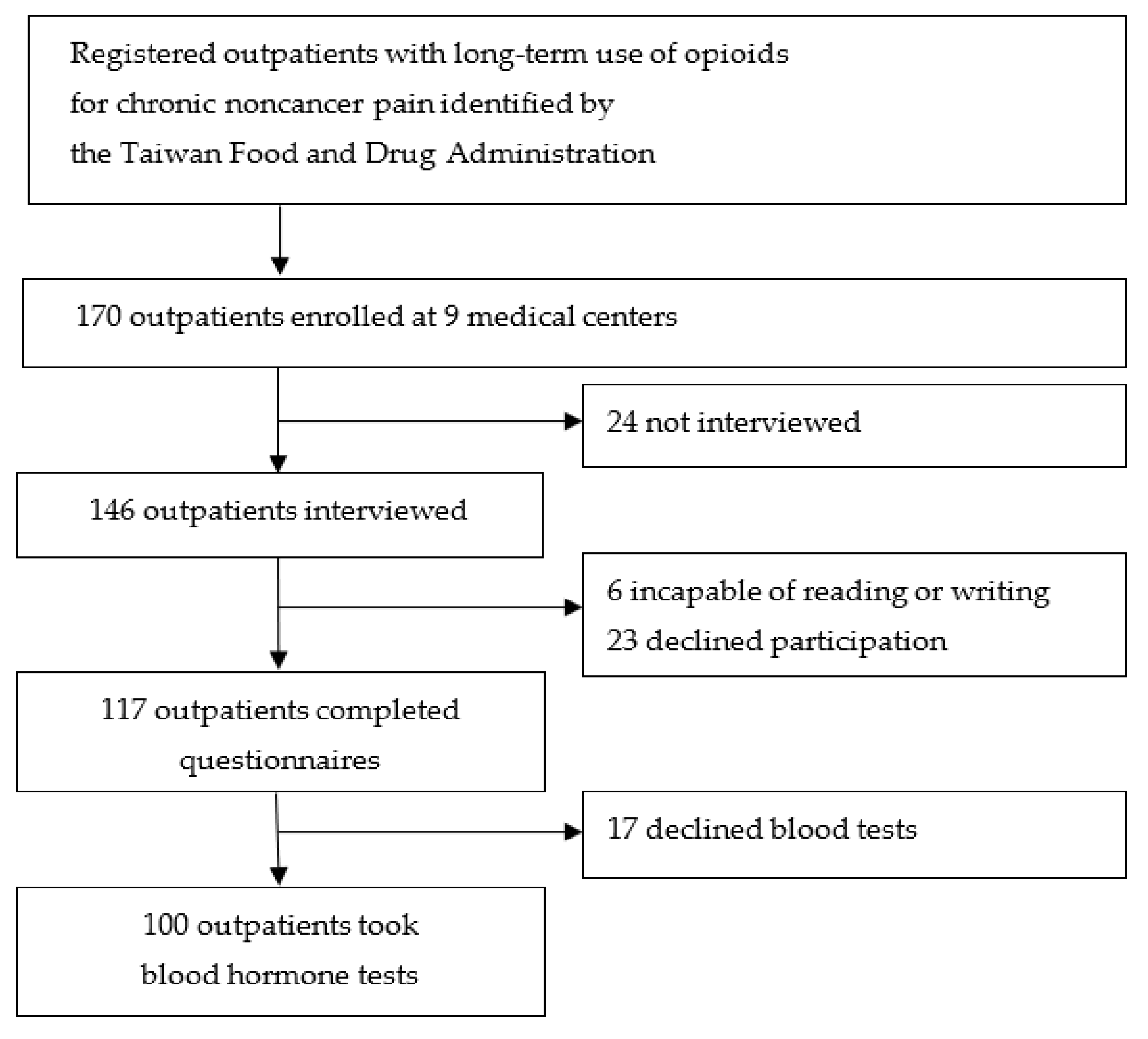
3.1. Participant Recruitment
3.2. General Characteristics of Participants
3.3. Serum Sex Hormone Levels
3.4. Depression, Daily Function and Sexual Interferences
4. Discussion
4.1. Main Findings
4.2. Prolonged Opioid Therapy and High Prescribing Rate in Taiwan
4.3. Chronic Pain, Depression, Suicide, and Opioid-Related Overdose Deaths
4.4. Estrogen and Testosterone Levels
4.5. Sexual Dysfunction
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, N.; Kariisa, M.; Seth, P.; Smith, H.; Davis, N.L. Drug and Opioid-Involved Overdose Deaths—United States, 2017–2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Baillargeon, J.; Raji, M.A.; Urban, R.J.; Lopez, D.S.; Williams, S.B.; Westra, J.R.; Kuo, Y.-F. Opioid-Induced Hypogonadism in the United States. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Antony, T.; Alzaharani, S.Y.; El-Ghaiesh, S.H. Opioid-induced hypogonadism: Pathophysiology, clinical and therapeutics review. Clin. Exp. Pharmacol. Physiol. 2019, 47, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Hajali, V.; Andersen, M.L.; Negah, S.S.; Sheibani, V. Sex differences in sleep and sleep loss-induced cognitive deficits: The influence of gonadal hormones. Horm. Behav. 2019, 108, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Bohnert, A.S.B.; Ilgen, M.A. Understanding Links among Opioid Use, Overdose, and Suicide. N. Engl. J. Med. 2019, 380, 71–79. [Google Scholar] [CrossRef]
- Nastri, C.O.; Lara, L.A.; Ferriani, R.A.; Rosa, E.S.A.C.; Figueiredo, J.B.; Martins, W.P. Hormone therapy for sexual function in perimenopausal and postmenopausal women. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Rastrelli, G.; Morgentaler, A.; Sforza, A.; Mannucci, E.; Maggi, M. Meta-analysis of Results of Testosterone Therapy on Sexual Function Based on International Index of Erectile Function Scores. Eur. Urol. 2017, 72, 1000–1011. [Google Scholar] [CrossRef] [PubMed]
- Cepeda, M.S.; Zhu, V.; Vorsanger, G.; Eichenbaum, G. Effect of Opioids on Testosterone Levels: Cross-Sectional Study using NHANES. Pain Med. 2015, 16, 2235–2242. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rubinstein, A.; Carpenter, D.M. Elucidating Risk Factors for Androgen Deficiency Associated with Daily Opioid Use. Am. J. Med. 2014, 127, 1195–1201. [Google Scholar] [CrossRef]
- Wersocki, E.; Bedson, J.; Chen, Y.; LeResche, L.; Dunn, K.M. Comprehensive systematic review of long-term opioids in women with chronic noncancer pain and associated reproductive dysfunction (hypothalamic–pituitary–gonadal axis disruption). Pain 2016, 158, 8–16. [Google Scholar] [CrossRef]
- Aminilari, M.; Manjoo, P.; Craigie, S.; Couban, R.; Wang, L.; Busse, J.W. Hormone Replacement Therapy and Opioid Tapering for Opioid-Induced Hypogonadism Among Patients with Chronic Noncancer Pain: A Systematic Review. Pain Med. 2018, 20, 301–313. [Google Scholar] [CrossRef]
- Hochberg, U.; Ojeda, A.; Brill, S.; Perez, J. An Internet-Based Survey to Assess Clinicians’ Knowledge and Attitudes Towards Opioid-Induced Hypogonadism. Pain Pr. 2018, 19, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Food and Drug Administration. Physician Guidelines on Clinical Use of Narcotics in Chronic Noncancer Pain. (in Chinsese, Amended on 4 December 2018). Available online: https://www.fda.gov.tw/tc/lawContent.aspx?cid=183&id=3086 (accessed on 30 November 2020).
- Taiwan Food and Drug Administration. 2019 International Conference on Narcotics: Safe Use and Management. Available online: https://www.fda.gov.tw/ENG/newsContent.aspx?id=25571 (accessed on 30 November 2020).
- Lin, T.-C.; Hsu, C.-H.; Lu, C.-C.; Tsai, Y.-C.; Ho, S.-T. Chronic opioid therapy in patients with chronic noncancer pain in Taiwan. J. Anesthesia 2010, 24, 882–887. [Google Scholar] [CrossRef]
- Lin, T.-C.; Ger, L.-P.; Pergolizzi, J.V.; Raffa, R.B.; Wang, J.-O.; Ho, S.-T. Long-term use of opioids in 210 officially registered patients with chronic noncancer pain in Taiwan: A cross-sectional study. J. Formos. Med Assoc. 2017, 116, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-C.; Ho, S.-T.; Ger, L.-P.; Liou, H.-H.; Hwang, S.-L. Gender difference in long-term use of opioids among Taiwan officially registered patients with chronic noncancer pain. Medicine 2018, 97, e10805. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-C.; Wu, W.-J.; Lee, Y.-C.; Wang, C.-J.; Ke, H.-L.; Li, W.-M.; Hsiao, H.-L.; Yeh, H.-C.; Li, C.-C.; Chou, Y.-H.; et al. The Prevalence of and Risk Factors for Androgen Deficiency in Aging Taiwanese Men. J. Sex. Med. 2009, 6, 936–946. [Google Scholar] [CrossRef]
- Pan, H.-H.; Ho, S.-T.; Lu, C.-C.; Wang, J.-O.; Lin, T.-C.; Wang, K.-Y. Trends in the Consumption of Opioid Analgesics in Taiwan From 2002 to 2007: A Population-Based Study. J. Pain Symptom Manag. 2013, 45, 272–278. [Google Scholar] [CrossRef]
- Ger, L.-P.; Ho, S.-T.; Sun, W.-Z.; Wang, M.-S.; Cleeland, C.S. Validation of the Brief Pain Inventory in a Taiwanese Population. J. Pain Symptom Manag. 1999, 18, 316–322. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Kahan, M.; Mailis-Gagnon, A.; Wilson, L.; Srivastava, A. Canadian guideline for safe and effective use of opioids for chronic noncancer pain: Clinical summary for family physicians. Part 1: General population. Can. Fam. Physician 2011, 57, 1257–1266. [Google Scholar]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef]
- Opioid Dose Equivalence. Faculty of Pain Medicine, ANZCA—March 2019. Available online: https://www.anzca.edu.au/getattachment/6892fb13-47fc-446b-a7a2-11cdfe1c9902/PM01-(Appendix-2)-Opioid-Dose-Equivalence-Calculation-of-Oral-Morphine-Equivalent-Daily-Dose-(oMEDD).aspx (accessed on 30 November 2020).
- Stanczyk, F.Z.; Clarke, N.J. Measurement of Estradiol—Challenges Ahead. J. Clin. Endocrinol. Metab. 2014, 99, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Wu, P.H.; Chang, C.H.; Tsai, T.J.; Hsu, L.L.; Lee, M.J. Hormone levels and menopausal status in middle aged women: A cross-sectional study (in Chinese). Chin. J. Public Health 1999, 18, 209–221. [Google Scholar] [CrossRef]
- Guy, G.P.; Zhang, K. Opioid Prescribing by Specialty and Volume in the U.S. Am. J. Prev. Med. 2018, 55, e153–e155. [Google Scholar] [CrossRef]
- Lin, T.-C.; Ger, L.-P.; Pergolizzi, J.V.; Raffa, R.B.; Wang, J.-O.; Ho, S.-T. Knowledge, Attitude and Practice Survey of Prescribing Opioids for Chronic Noncancer Pain in Taiwan—Comparison of Pain and Non-Pain Physicians. Pain Med. 2016, 20, 2397–2410. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Lin, S.-L.; Sung, C.-S.; Ger, L.-P.; Liou, H.-H.; Lin, T.-C.; Ho, S.-T. Knowledge, attitude, and barriers regarding prescribing long-term opioids among Taiwan physicians treating officially registered patients with chronic noncancer pain. J. Chin. Med. Assoc. 2020, 84, 227–232. [Google Scholar] [CrossRef]
- Taiwan Food and Drug Administration. Controlled Drugs Act. Amended Date 14 June 2017. Available online: https://www.fda.gov.tw/ENG/lawContent.aspx?cid=5061&id=603 (accessed on 30 November 2020).
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2019, 45, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, J.F.; Salas, J.; Schneider, D.; Bucholz, K.K.; Sullivan, M.D.; Copeland, L.; Ahmedani, B.K.; Burroughs, T.; Lustman, P.J. Characteristics of new depression diagnoses in patients with and without prior chronic opioid use. J. Affect. Disord. 2017, 210, 125–129. [Google Scholar] [CrossRef]
- Oliva, E.M.; Bowe, T.; Manhapra, A.; Kertesz, S.; Hah, J.M.; Henderson, P.; Robinson, A.; Paik, M.; Sandbrink, F.; Gordon, A.J.; et al. Associations between stopping prescriptions for opioids, length of opioid treatment, and overdose or suicide deaths in US veterans: Observational evaluation. BMJ 2020, 368, m283. [Google Scholar] [CrossRef] [PubMed]
- Decaroli, M.C.; Rochira, V. Aging and sex hormones in males. Virulence 2016, 8, 545–570. [Google Scholar] [CrossRef]
- De Vries, F.; Bruin, M.; Lobatto, D.J.; Dekkers, O.M.; Schoones, J.W.; Van Furth, W.R.; Pereira, A.M.; Karavitaki, N.; Biermasz, N.R.; Najafabadi, A.H.Z. Opioids and Their Endocrine Effects: A Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2019, 105, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.R.; Baber, R.; Panay, N.; Bitzer, J.; Perez, S.C.; Islam, R.M.; Kaunitz, A.M.; Kingsberg, S.A.; Lambrinoudaki, I.; Liu, J.; et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J. Clin. Endocrinol. Metab. 2019, 104, 4660–4666. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Women (n = 38) | Men (n = 62) | p-Value | Odds Ratio | |||
|---|---|---|---|---|---|---|
| Mean ± SD (Range) | Median | Mean ± SD (Range) | Median | |||
| Age, year | 55.4 ± 13.6 (25–94) | 57 | 50.3 ± 9.2 (37–78) | 48 | 0.026 a | 0.96 |
| Height, cm | 156.8 ± 8.9 (130–168) | 158.5 | 168.5 ± 7.5 (150–185) | 168.5 | <0.001 a | 1.23 |
| Weight, kg | 57.9 ± 15.4 (30–97) | 56 | 67.2 ± 15.0 (41–102) | 64 | 0.004 a | 1.04 |
| Body mass index | 23.4 ± 5.2 (15.6–34.4) | 23.4 | 23.7 ± 5.0 (14.5–38.9) | 23.7 | 0.797 a | |
| Pain duration, month | 140.5 ± 108.4 (12–485) | 120 | 172.0 ± 96.0 (24–480) | 171 | 0.134 a | |
| Opioid therapy, month | 104.3 ± 95.7 (6–384) | 81 | 126.5 ± 83.0 (6–335) | 120 | 0.223 a | |
| MME, oral, mg/day | 194.2 ± 172.1 (15–604) | 134 | 227.6 ± 230.0 (3–1350) | 165 | 0.440 a | |
| MME per kg, mg/day/kg | 3.5 ± 3.2 (0.4–12) | 2.5 | 3.6 ± 3.8 (0.0–24.6) | 2.5 | 0.945 a | |
| MME ≥ 200 mg/day, n = 40 | 14 (36.8%) | 26 (41.9%) | 0.614 b | |||
| MME ≥ 90 mg/day, n = 68 | 23 (60.5%) | 45 (72.6%) | 0.210 b | |||
| Concomitant use of adjuvants, n (%) | ||||||
| Gabapentin or pregabalin | 15 (39.5%) | 24 (38.7%) | 0.939 b | |||
| Tricyclic antidepressants | 5 (13.2%) | 12 (19.4%) | 0.423 b | |||
| Serotonin reuptake inhibitor antidepressants | 5 (13.2%) | 7 (11.3%) | 0.762 c | |||
| Benzodiazepine | 9 (23.7%) | 20 (32.3%) | 0.359 b | |||
| Top 3 diagnoses of pain source, n (%) | ||||||
| Failed back surgery syndrome, n = 20 | 8 (21.1%) | 12 (19.4%) | 0.837 b | |||
| Chronic pancreatitis, n = 15 | 1 (2.6%) | 14 (22.6%) | 0.007 b | 10.79 | ||
| Spinal cord injury, n = 14 | 5 (13.2%) | 9 (14.5%) | 0.849 b | |||
| Blood hormone tests ever received, n = 23 | 8 (21.1%) | 15 (24.2%) | 0.717 b |
| Women (n = 38) | Men (n = 62) | p-Value | |||
|---|---|---|---|---|---|
| Mean ± SD (Range) | Median | Mean ± SD (Range) | Median | ||
| Follicle-stimulating hormone level, mIU/mL | |||||
| With menstruation, n = 9 | 8.2 ± 3.6 (3.9–15.6) | 7.4 | - | - | - |
| *Clinical menopause, n = 29 | 46.4 ± 28.5 (0.7–117.3) | 45.2 | - | - | - |
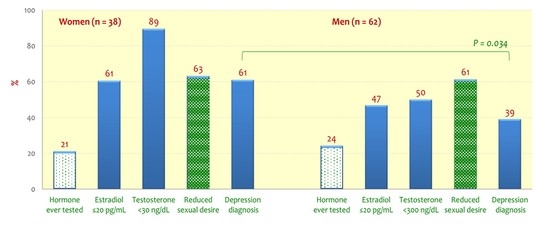
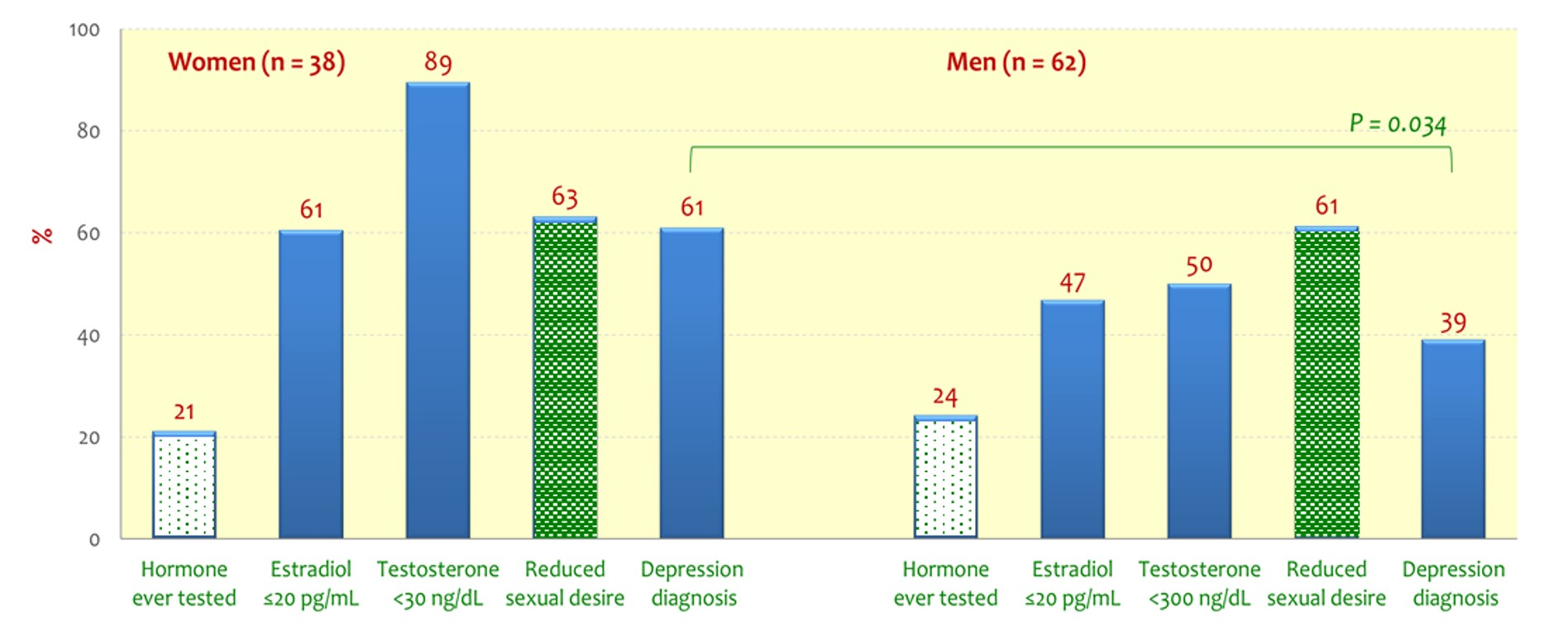
| Serum estradiol level, pg/ml | 41.8 ± 76.5 (5–424) | 20 | 25.7 ± 11.6 (10–52) | 21 | - |
| >20 pg/mL, n | 15 (39.5%) | 33 (53.2%) | - | ||
| Age < 50, W/M = 8/18 | 122.4 ± 137.5 (27–424) | 46.9 | 35.0 ± 11.5 (21–52) | 34.5 | - |
| Age ≥ 50, W/M = 7/15 | 42.9 ± 46.1 (24–147) | 24.7 | 30.9 ± 10.0 (21–52) | 27.9 | - |
| ≤20 pg/mL, n | 23 (60.5%) | 29 (46.8%) | 0.182 a | ||
| With menstruation, n = 1 in 9 | 1 (11.1%) | - | - | - | |
| Clinical menopause, n = 22 in 29 | 22 (75.9%) | - | - | - | |
| Serum testosterone level, ng/dL | 15.2 ± 9.5 (3–40) | 13 | 347.6 ± 273.8 (50–1416) | 297 | |
| Age 20–39, W/M = 4/6 | 14.4 ± 3.6 (10–18) | 15 | 334.3 ± 99.1 (179–474) | 339 | |
| Age 40–64, W/M = 29/51 | 15.2 ± 10.0 (3–40) | 10 | 360.5 ± 296.5 (50–1416) | 289 | 0.527 b |
| Age 65–79, W/M = 3/5 | 12.3 ± 8.9 (3–21) | 13 | 232.9 ± 114.6 (86–383) | 214 | |
| Age ≥ 80, W/M = 2/0 | 10, 31 | - | - | - | |
| Women < 30 ng/dL, n | 34 (89.5%) | - | |||
| Men < 300 ng/dL, n | 31 (50.0%) | - |
| Women (n = 38) | Men (n = 62) | p-Value | Odds Ratio | |||
|---|---|---|---|---|---|---|
| Mean ± SD (Range) | Median | Mean ± SD (Range) | Median | |||
| Pain intensity reduction after taking opioids, % | 43.2 ± 19.6 (0–90) | 45 | 49.5 ± 18.4 (10–100) | 50 | 0.105 a | |
| Daily function interference, in average | ||||||
| Before taking opioids, 0–10 | 7.9 ± 2.1 (3.6–10) | 8.4 | 8.0 ± 2.0 (0.9–10) | 8.4 | 0.696 a | |
| After taking opioids, 0–10 | 5.0 ± 2.5 (0–9.6) | 4.8 | 4.7 ± 2.6 (0–10) | 4.7 | 0.610 a | |
| Interference reduction after taking opioids, % | 35.9 ± 26.2 (−18.0–100) | 33.5 | 41.6 ± 29.5 (–33.8–100) | 39.5 | 0.327 a | |
| Sexual desire, n = 100 | ||||||
| Increased or unchanged, n = 38 | 14 (36.8%) | 24 (38.7%) | ||||
| Decreased, n = 62 | 24 (63.2%) | 38 (61.3%) | 0.852 b | |||
| Sexual function in those sexually active, n = 50 | 18 (47.4%) | 32 (51.6%) | 0.680 b | |||
| Increased or unchanged, n = 16 | 6 (33.3%) | 10 (31.2%) | ||||
| Decreased, n = 34 | 12 (66.7%) | 22 (68.8%) | 0.880 b | |||
| Depression diagnosis by now, n = 47 | 23 (60.5%) | 24 (38.7%) | 0.034 b | 0.41 | ||
| Depression diagnosis before chronic pain, n = 30 | 18 (47.4%) | 12 (19.4%) | 0.003 b | 0.27 | ||
| Beck Depression Inventory score, 0–63# | 26.7 ± 15.7 (0–55) | 28.5 | 17.4 ± 12.9 (0–63) | 16 | 0.003 c | 0.96 |
| With decreased sexual desire, W/M = 24/38 | 30.3 ± 16.7 (1–55) | 31.5 | 18.1 ± 14.2 (0–63) | 15.5 | 0.003 c | 0.95 |
| With decreased sexual function, W/M = 12/22 | 26.3 ± 14.2 (6–46) | 27.5 | 15.2 ± 7.8 (1–37) | 14.5 | 0.028 c | 0.91 |
| Suicidal ideation, n (%) | ||||||
| Always / Frequently | 5 (13.2%) | 6 (9.7%) | 0.469 d | |||
| Sometimes | 12 (31.6%) | 13 (21.0%) | ||||
| Seldom | 5 (13.2%) | 14 (22.6%) | ||||
| Never | 16 (42.1%) | 29 (46.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, S.-T.; Lin, T.-C.; Yeh, C.-C.; Cheng, K.-I.; Sun, W.-Z.; Sung, C.-S.; Wen, Y.-R.; Hsieh, Y.-J.; Wang, P.-K.; Liu, Y.-C.; et al. Gender Differences in Depression and Sex Hormones among Patients Receiving Long-Term Opioid Treatment for Chronic Noncancer Pain in Taiwan—A Multicenter Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7837. https://doi.org/10.3390/ijerph18157837
Ho S-T, Lin T-C, Yeh C-C, Cheng K-I, Sun W-Z, Sung C-S, Wen Y-R, Hsieh Y-J, Wang P-K, Liu Y-C, et al. Gender Differences in Depression and Sex Hormones among Patients Receiving Long-Term Opioid Treatment for Chronic Noncancer Pain in Taiwan—A Multicenter Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7837. https://doi.org/10.3390/ijerph18157837
Chicago/Turabian StyleHo, Shung-Tai, Tso-Chou Lin, Chun-Chang Yeh, Kuang-I Cheng, Wei-Zen Sun, Chun-Sung Sung, Yeong-Ray Wen, Yi-Jer Hsieh, Po-Kai Wang, Yen-Chin Liu, and et al. 2021. "Gender Differences in Depression and Sex Hormones among Patients Receiving Long-Term Opioid Treatment for Chronic Noncancer Pain in Taiwan—A Multicenter Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 15: 7837. https://doi.org/10.3390/ijerph18157837
APA StyleHo, S.-T., Lin, T.-C., Yeh, C.-C., Cheng, K.-I., Sun, W.-Z., Sung, C.-S., Wen, Y.-R., Hsieh, Y.-J., Wang, P.-K., Liu, Y.-C., & Tsai, Y.-C. (2021). Gender Differences in Depression and Sex Hormones among Patients Receiving Long-Term Opioid Treatment for Chronic Noncancer Pain in Taiwan—A Multicenter Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(15), 7837. https://doi.org/10.3390/ijerph18157837