
The Effect of Meteorological, Pollution, and Geographic Exposures on Death by Suicide: A Scoping Review

 and
and
Abstract
1. Introduction
2. Materials and Methods
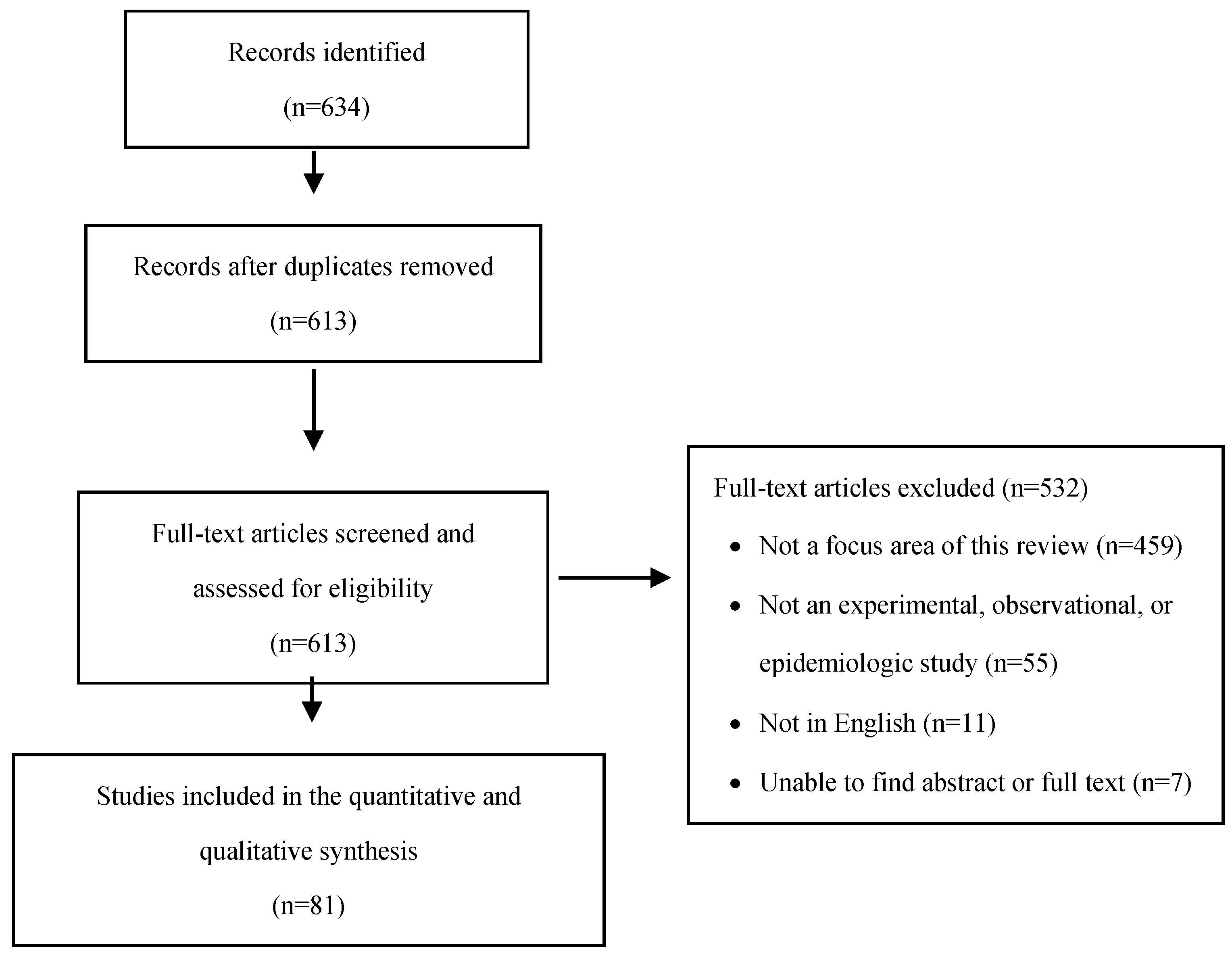
2.1. Study Search and Inclusion
2.2. Analysis
3. Results
3.1. Meteorological Factors
3.2. Pollution Factors
3.3. Geographic Factors
4. Discussion
4.1. Meteorological Factors
4.2. Pollution Factors
4.3. Geographic Factors
4.4. Overview
4.5. Limitations of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Suicide in the World: Global Health Estimates; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- CDC. Preventing Suicide. 2020. Available online: https://www.cdc.gov/violenceprevention/suicide/fastfact.html (accessed on 21 April 2020).
- Stone, D.; Holland, K.; Bartholow, B.; Crosby, A.; Davis, S.; Wilkins, N. Preventing Suicide: A Technical Package of Policy, Programs, and Practices; CDC: Atlanta, GA, USA, 2017. [Google Scholar]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers 2019, 5, 74. [Google Scholar] [CrossRef]
- Hawton, K.; van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef]
- Mann, J.J.; Currier, D. Stress, genetics and epigenetic effects on the neurobiology of suicidal behavior and depression. Eur. Psychiatry 2010, 25, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Van Heeringen, K.; Mann, J.J. The neurobiology of suicide. Lancet Psychiatry 2014, 1, 63–72. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Aguglia, A.; Escelsior, A.; Serafini, G.; Berardelli, I.; Pompili, M.; Amore, M. When Sick Brain and Hopelessness Meet: Some Aspects of Suicidality in the Neurological Patient. CNS Neurol. Disord. Drug Targets 2020, 19, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Costanza, A.; Baertschi, M.; Weber, K.; Canuto, A. Neurological diseases and suicide: From neurobiology to hopelessness. Rev. Med. Suisse 2015, 11, 402–405. [Google Scholar] [PubMed]
- Benard, V.; Geoffroy, P.; Bellivier, F. Saisons, rythmes circadiens, sommeil et vulnérabilité aux conduites suicidaires. L’Encéphale 2015, 41 (Suppl. 1), S29–S37. [Google Scholar] [CrossRef]
- Galvão, P.V.M.; Silva, H.; da Silva, C.M.F.P. Temporal distribution of suicide mortality: A systematic review. J. Affect. Disord. 2018, 228, 132–142. [Google Scholar] [CrossRef]
- Ajdacic-Gross, V.; Bopp, M.; Ring, M.; Gutzwiller, F.; Rossler, W. Seasonality in suicide—A review and search of new concepts for explaining the heterogeneous phenomena. Soc. Sci. Med. 2010, 71, 657–666. [Google Scholar] [CrossRef]
- Woo, J.-M.; Okusaga, O.; Postolache, T.T. Seasonality of Suicidal Behavior. Int. J. Environ. Res. Public Health 2012, 9, 531–547. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, W.; Gu, X.; Deng, F.; Wang, X.; Lin, H.; Guo, X.; Wu, S. Association between particulate matter air pollution and risk of depression and suicide: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. 2021, 28, 9029–9049. [Google Scholar] [CrossRef] [PubMed]
- Davoudi, M.; Barjasteh-Askari, F.; Amini, H.; Lester, D.; Mahvi, A.H.; Ghavami, V.; Ghalhari, M.R. Association of suicide with short-term exposure to air pollution at different lag times: A systematic review and meta-analysis. Sci. Total Environ. 2021, 771, 144882. [Google Scholar] [CrossRef] [PubMed]
- Kious, B.M.; Kondo, D.; Renshaw, P.F. Living High and Feeling Low: Altitude, Suicide, and Depression. Harv. Rev. Psychiatry 2018, 26, 43–56. [Google Scholar] [CrossRef]
- Yan, Y.Y. Geophysical Variables and Behavior: LXXXXIX. The Influence of Weather on Suicide in Hong Kong. Percept. Mot. Ski. 2000, 91, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Santurtún, M.; Sanchez-Lorenzo, A.; del Real, A.; Zarrabeitia, M.T.; Santurtún, A. Association Between Suicide and Environmental Variables in the North of Spain: A 14-Year Analysis. Cult. Med. Psychiatry 2018, 42, 647–653. [Google Scholar] [CrossRef]
- Schneider, A.; Hampel, R.; Ladwig, K.-H.; Baumert, J.; Lukaschek, K.; Peters, A.; Breitner, S. Impact of meteorological parameters on suicide mortality rates: A case-crossover analysis in Southern Germany (1990–2006). Sci. Total Environ. 2020, 707, 136053. [Google Scholar] [CrossRef]
- Chau, P.H.; Yip, P.S.F.; Lau, H.Y.E.; Ip, Y.T.; Law, F.Y.W.; Ho, R.T.H.; Leung, A.Y.M.; Wong, J.Y.H.; Woo, J. Hot Weather and Suicide Deaths among Older Adults in Hong Kong, 1976–2014: A Retrospective Study. Int. J. Environ. Res. Public Health 2020, 17, 3449. [Google Scholar] [CrossRef]
- Glenn, C.R.; Nock, M.K. Improving the Short-Term Prediction of Suicidal Behavior. Am. J. Prev. Med. 2014, 47 (Suppl. 2), S176–S180. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Ferguson, C.J. An effect size primer: A guide for clinicians and researchers. Prof. Psychol. Res. Pract. 2009, 40, 532–538. [Google Scholar] [CrossRef]
- Haug, M.G. Measures of Association. Available online: https://www.britannica.com/topic/measure-of-association (accessed on 12 May 2021).
- Inoue, K.; Nishimura, Y.; Fujita, Y.; Ono, Y.; Fukunaga, T. The Relationship between Suicide and Five Climate Issues in a Large-scale and Long Term Study in Japan. West Indian Med. J. 2012, 61, 532–537. [Google Scholar] [CrossRef]
- Tsai, J.-F.; Cho, W. Temperature change dominates the suicidal seasonality in Taiwan: A time-series analysis. J. Affect. Disord. 2012, 136, 412–418. [Google Scholar] [CrossRef]
- Min, J.-Y.; Kim, H.-J.; Min, K.-B. Long-term exposure to air pollution and the risk of suicide death: A population-based cohort study. Sci. Total Environ. 2018, 628–629, 573–579. [Google Scholar] [CrossRef]
- Casas, L.; Cox, B.; Bauwelinck, M.; Nemery, B.; Deboosere, P.; Nawrot, T. Does air pollution trigger suicide? A case-crossover analysis of suicide deaths over the life span. Eur. J. Epidemiol. 2017, 32, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Bakian, A.V.; Huber, R.S.; Coon, H.; Gray, D.; Wilson, P.; McMahon, W.M.; Renshaw, P.F. Acute air pollution exposure and risk of suicide completion. Am. J. Epidemiol. 2015, 181, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Jung, S.H.; Kang, D.R.; Kim, H.C.; Moon, K.T.; Hur, N.W.; Shin, D.C.; Suh, I. Ambient Particulate Matter as a Risk Factor for Suicide. Am. J. Psychiatry 2010, 167, 1100–1107. [Google Scholar] [CrossRef]
- Kim, Y.; Ng, C.F.S.; Chung, Y.; Kim, H.; Honda, Y.; Guo, Y.L.; Lim, Y.H.; Chen, B.Y.; Page, L.A.; Hashizume, M. Air Pollution and Suicide in 10 Cities in Northeast Asia: A Time-Stratified Case-Crossover Analysis. Environ. Health Perspect. 2018, 126, 037002. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Myung, W.; Kim, S.E.; Kim, D.K.; Kim, H. Ambient air pollution and completed suicide in 26 South Korean cities: Effect modification by demographic and socioeconomic factors. Sci. Total Environ. 2018, 639, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.Z.; Li, L.; Song, Y.F.; Zhou, Y.X.; Shen, S.Q.; Ou, C.Q. The impact of ambient air pollution on suicide mortality: A case-crossover study in Guangzhou, China. Environ. Health 2016, 15, 90. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.F.S.; Stickley, A.; Konishi, S.; Watanabe, C. Ambient air pollution and suicide in Tokyo, 2001–2011. J. Affect. Disord. 2016, 201, 194–202. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Huang, Y.-T.; Chiu, H.-F. Does ambient ozone air pollution trigger suicide attempts? A case cross-over analysis in Taipei. J. Toxicol. Environ. Health Part A 2019, 82, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-Y.; Weng, Y.-H.; Chiu, Y.-W. Relationship between ozone air pollution and daily suicide mortality: A time-stratified case-crossover study in Taipei. J. Toxicol. Environ. Health Part A 2019, 82, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Min, J.-Y.; Min, K.-B. Night noise exposure and risk of death by suicide in adults living in metropolitan areas. Depress. Anxiety 2018, 35, 876–883. [Google Scholar] [CrossRef]
- Figgs, L.W.; Holsinger, H.; Freitas, S.J.; Brion, G.M.; Hornung, R.W.; Rice, C.H.; Tollerud, D. Increased suicide risk among workers following toxic metal exposure at the Paducah gaseous diffusion plant from 1952 to 2003: A cohort study. Int. J. Occup. Environ. Med. 2011, 2, 199–214. [Google Scholar] [PubMed]
- Asirdizer, M.; Kartal, E.; Etli, Y.; Tatlisumak, E.; Gumus, O.; Hekimoglu, Y.; Keskin, S. The effect of altitude and climate on the suicide rates in Turkey. J. Forensic Leg. Med. 2018, 54, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Betz, M.E.; Valley, M.A.; Lowenstein, S.R.; Hedegaard, H.; Thomas, D.; Stallones, L.; Honigman, B. Elevated Suicide Rates at High Altitude: Sociodemographic and Health Issues May Be to Blame. Suicide Life Threat. Behav. 2011, 41, 562–573. [Google Scholar] [CrossRef]
- Brenner, B.; Cheng, D.; Clark, S.; Camargo, C.A., Jr. Positive association between altitude and suicide in 2584 U.S. counties. High Alt. Med. Biol. 2011, 12, 31–35. [Google Scholar] [CrossRef]
- Haws, C.A.; Gray, D.D.; Yurgelun-Todd, D.A.; Moskos, M.; Meyer, L.J.; Renshaw, P.F. The possible effect of altitude on regional variation in suicide rates. Med. Hypotheses 2009, 73, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Tu, W. An Ecological Study on the Spatially Varying Relationship between County-Level Suicide Rates and Altitude in the United States. Int. J. Environ. Res. Public Health 2018, 15, 671. [Google Scholar] [CrossRef]
- Kim, N.; Mickelson, J.B.; Brenner, B.E.; Haws, C.A.; Yurgelun-Todd, D.A.; Renshaw, P.F. Altitude, gun ownership, rural areas, and suicide. Am. J. Psychiatry 2011, 168, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Choi, N.; Lee, Y.J.; An, H.; Kim, N.; Yoon, H.K.; Lee, H.J. High altitude remains associated with elevated suicide rates after adjusting for socioeconomic status: A study from South Korea. Psychiatry Investig. 2014, 11, 492–494. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Oka, M.; Kubota, T.; Tsubaki, H.; Yamauchi, K. Analysis of impact of geographic characteristics on suicide rate and visualization of result with Geographic Information System. Psychiatry Clin. Neurosci. 2014, 69, 375–382. [Google Scholar] [CrossRef]
- Sabic, H.; Kious, B.; Boxer, D.; Fitzgerald, C.; Riley, C.; Scholl, L.; McGlade, E.; Yurgelun-Todd, D.; Renshaw, P.F.; Kondo, D.G. Effect of Altitude on Veteran Suicide Rates. High Alt. Med. Biol. 2019, 20, 171–177. [Google Scholar] [CrossRef]
- Selek, S. Altitude, Immigration and Suicide Rates: A Study from Turkey. Psychiatry Investig. 2013, 10, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, J.L.; Whittemore, A.S.; Evans, A.S.; Thompson, W.D. Cross-Sectional and Other Types of Studies. In Methods in Observational Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1996; pp. 244–267. [Google Scholar]
- Riblet, N.B.; Gottlieb, D.J.; Watts, B.V.; Cornelius, S.L.; Fan, V.S.; Shi, X.; Shiner, B. Hypoxia-related risk factors for death by suicide in a national clinical sample. Psychiatry Res. 2019, 273, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Commentary: Does Air Pollution Confound Studies of Temperature? Epidemiology 2014, 25, 242–245. [Google Scholar] [CrossRef]
- Aguglia, A.; Giacomini, G.; Montagna, E.; Amerio, A.; Escelsior, A.; Capello, M.; Cutroneo, L.; Ferretti, G.; Scafidi, D.; Costanza, A.; et al. Meteorological Variables and Suicidal Behavior: Air Pollution and Apparent Temperature Are Associated with High-Lethality Suicide Attempts and Male Gender. Front. Psychiatry 2021, 12, 653390. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Terms | Number of Studies | |
|---|---|---|
| Medline | ||
| Meteorology and Suicide | “Sunlight”[Mesh] OR “Ultraviolet Rays”[Mesh] OR “Temperature”[Mesh] OR “Hot Temperature”[Mesh] OR “Cold Temperature”[Mesh] OR “Humidity”[Mesh] OR “Meteorology”[Mesh] OR Sunlight[ti] OR Meterorol*[ti] OR Temperature[ti] or UV[ti] OR Humidity[ti] OR Weather[ti] | 202 |
| Pollution and Suicide | “Non-Point Source Pollution”[Mesh] OR “Water Pollution, Radioactive”[Mesh] OR “Water Pollution, Chemical”[Mesh] OR “Water Pollution”[Mesh] OR “Environmental Pollution”[Mesh] OR “Air Pollution, Radioactive”[Mesh] OR “Air Pollution”[Mesh] OR “Traffic-Related Pollution”[Mesh] OR “Noise”[Mesh] OR “Water Pollutants, Chemical”[Mesh] OR “Environmental Pollutants”[Mesh] OR “Vehicle Emissions”[Mesh] OR “Air Pollutants, Radioactive”[Mesh] OR Pollution[ti] OR Pollutants[ti] OR Smog[ti] | 339 |
| Geography and Suicide | “Altitude”[Mesh] OR Altitude[ti] or Elevation[ti] | 52 |
| Embase | ||
| Meteorology and Suicide | Sunlight, Ultraviolet Rays, Temperature, Humidity, Meteorology, or Weather | 61 |
| Pollution and Suicide | Pollution, Pollutants, or Smog | 26 |
| Geography and Suicide | Altitude or Elevation | 25 |
| PsychInfo | ||
| Meteorology and Suicide | Sunlight, Ultraviolet, Temperature, Humidity, Meteorology, or Weather | 24 |
| Pollution and Suicide | Pollution, Pollutants, or Smog | 5 |
| Geography and Suicide | Altitude or Elevation | 4 |
| Significant Association * | No Association | ||
|---|---|---|---|
| Total Studies | Total N Studies | N (%) | N (%) |
| Meteorological factors | |||
| Primary Exposure | |||
| Sunlight intensity | 5 | 3 (60.0%) | 2 (40.0%) |
| Sunlight duration | 23 | 15 (65.2%) | 8 (34.8%) |
| Temperature | 38 | 30 (78.9%) | 6 (15.8%) |
| Humidity | 11 | 4 (36.4%) | 7 (63.6%) |
| Air pressure | 7 | 3 (42.9%) | 4 (57.1%) |
| Rainfall | 16 | 3 (18.8%) | 13 (81.3%) |
| Primary Analysis | |||
| Population level | 34 | 30 (88.2%) | 4 (11.8%) |
| Individual level | 12 | 10 (83.3%) | 2 (16.7%) |
| Pollution factors | |||
| Primary Exposure | |||
| Air Pollution | |||
| PM2.5 | 7 | 4 (57.1%) | 3 (42.9%) |
| PM10 | 11 | 7 (63.6%) | 4 (36.4%) |
| O3 | 8 | 5 (62.5%) | 3 (37.5%) |
| NO2 | 10 | 6 (60.0%) | 4 (40.0%) |
| SO2 | 9 | 5 (55.6%) | 4 (44.4%) |
| Pesticides | 7 | 5 (71.4%) | 2 (28.6%) |
| Toxic Metals | 1 | 1 (100.0%) | 0 (0.0%) |
| Noise | 2 | 2 (100.0%) | 0 (0.0%) |
| Observation Level | |||
| Population | 6 | 4 (66.7%) | 2 (33.3%) |
| Individual | 17 | 15 (88.2%) | 2 (11.8%) |
| Geographic factors a | |||
| Primary Exposure | |||
| Altitude | 12 | 9 (75.0%) | 1 (8.3%) |
| Observation Level | |||
| Population | 9 | 7 (77.8%) | 1 (11.1%) |
| Individual | 3 | 2 (66.7%) | 0 (0.0%) |
| Significant Association * | No Association | |||||
|---|---|---|---|---|---|---|
| Sample Size | Sample Size | |||||
| Meteorological Factors | N Studies (%) b | Min–Max Number of Suicides | Median (IQR) Number of Suicides | N Studies (%) b | Min–Max Number of Suicides | Median (IQR) Number of Suicides |
| Primary Exposure | ||||||
| Sunlight intensity | 3 (100.0%) | 3717–43,393 | 6600.0 (39,676.0) | 1 (50.0%) | 3984–3984 | 3984.0 (0.0) |
| Sunlight duration | 12 (80.0%) | 197–128,322 | 17,378.0 (74,332.5) | 6 (75.0%) | 536–55,362 | 6301.0 (6611.0) |
| Temperature | 23 (71.9%) | 197–1,320,148 | 22,564.0 (84,909.0) | 3 (50.0%) | 3984–7944 | 5706.0 (3960.0) |
| Humidity | 2 (50.0%) | 6600–18,083 | 12,341.5 (11,483.0) | 5 (71.4%) | 197–45,293 | 10,595.0 (21,879.0) |
| Air pressure | 1 (33.3%) | 18,083–18,083 | 18,083.0 (0.0) | 2 (50.0%) | 685–6600 | 3642.5 (5915.0) |
| Rainfall | 2 (66.7%) | 6600–55,362 | 30,981.0 (48,762.0) | 9 (69.2%) | 197–128,322 | 18,083.0 (37,687.0) |
| Primary Analysis | ||||||
| Population level | 21 (70.0%) | 685–1,320,148 | 39,347.0 (86,596.0) | 1 (25.0%) | 3984–3984 | 3984.0 (0.0) |
| Individual level | 9 (90.0%) | 197–69,462 | 10,595.0 (9569.0) | 2 (100.0%) | 536–7944 | 4240.0 (7408.0) |
| Pollution Factors | ||||||
| Primary Exposure | ||||||
| Air Pollution | ||||||
| PM2.5 | 4 (100.0%) | 1546–134,811 | 17,140.0 (79,431.5) | 2 (66.7%) | 528–1942 | 1235.0 (1414.0) |
| PM10 | 6 (85.7%) | 564–134,811 | 12,437.0 (71,895.0) | 3 (75.0%) | 528–1942 | 1546.0 (1414.0) |
| O3 | 4 (80.0%) | 1008–73,445 | 11,267.0 (45,484.5) | 2 (66.7%) | 528–1942 | 1235.0 (1414.0) |
| NO2 | 5 (83.3%) | 564–73,445 | 1550.0 (28,393.0) | 3 (75.0%) | 528–134,811 | 1942.0 (134,283.0) |
| SO2 | 5 (100.0%) | 564–134,811 | 29,939.0 (71,895.0) | 2 (50.0%) | 1546–1942 | 1744.0 (396.0) |
| Pesticides | 5 (100.0%) | 109–117,469 | 4991.0 (10,250.0) | 2 (100.0%) | 90–110 | 100.0 (20.0) |
| Toxic Metals | 1 (100.0%) | 40–40 | 40.0 (0.0) | n/a | n/a | n/a |
| Noise | 2 (100.0%) | 315–528 | 421.5 (213) | n/a | n/a | n/a |
| Observation Level | ||||||
| Population | 3 (75.0%) | 528–117,469 | 1008.0 (116,941.0) | 1 (50.0%) | 1942–1942 | 1942 (0.0) |
| Individual | 15 (100.0%) | 40–134,811 | 2001.0 (19,969.0) | 2 (100.0%) | 90–110 | 100.0 (20.0) |
| Geographic Factors a | ||||||
| Primary Exposure | ||||||
| Altitude | 3 (33.3%) | 22,403–596,704 | 35,725.0 (574,301.0) | 0 (0.0%) | n/a | n/a |
| Observation Level | ||||||
| Population | 1 (14.3%) | 596,704–596,704 | 596,704 (0.0) | 0 (0.0%) | n/a | n/a |
| Individual | 2 (100.0%) | 22,403–35,725 | 29,064.0 (13,322.0) | n/a | n/a | n/a |
| Total N Significant Studies * | Very Small Effect | Small Effect | Moderate Effect | |
|---|---|---|---|---|
| Meteorological factors | ||||
| Sunlight intensity | 3 | 2 (66.7%) | 0 (0.0%) | 1 (33.3%) |
| Sunlight duration | 15 | 6 (40.0%) | 6 (40.0%) | 3 (20.0%) |
| Temperature | 30 | 20 (66.7%) | 8 (26.7%) | 4 (13.3%) |
| Humidity | 4 | 1 (25.0%) | 2 (50.0%) | 1 (25.0%) |
| Air pressure | 3 | 0 (0.0%) | 3 (100.0%) | 0 (0.0%) |
| Rainfall | 3 | 2 (66.7%) | 1 (33.3%) | 0 (0.0%) |
| Pollution factors | ||||
| Air Pollution | ||||
| PM2.5 | 4 | 4 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| PM10 | 7 | 6 (85.7%) | 0 (0.0%) | 1 (14.3%) |
| O3 c | 5 | 4 (80.0%) | 0 (0.0%) | 0 (0.0%) |
| NO2 | 6 | 6 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| SO2 | 5 | 5 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| Pesticides | 5 | 4 (80.0%) | 1 (20.0%) | 0 (0.0%) |
| Toxic Metals | 1 | 0 (0.0%) | 1 (100.0%) | 0 (0.0%) |
| Noise | 2 | 2 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| Geographic factors a,c | ||||
| Altitude | 9 | 2 (22.2%) | 2 (22.2%) | 4 (44.4%) |
| Adjustment for Confounding | Effect Modification | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total N Studies | Measure of Time d | Measure of Season e | Environment Covariates | Individual-Level Factors | Community-Level Factors | Age | Gender | Suicide Method | |
| Meteorological factors | |||||||||
| Significant association * | 40 | 14 (35.0%) | 26 (65.0%) | 8 (20.0%) | 3 (7.5%) | 3 (7.5%) | 6 (15.0%) | 13 (32.5%) | 3 (7.5%) |
| No association | 6 | 2 (33.3%) | 2 (33.3%) | 1 (16.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (16.7%) | 1 (16.7%) |
| Pollution factors | |||||||||
| Significant association * | 19 | 10 (52.6%) | 8 (42.1%) | 10 (52.6%) | 7 (36.8%) | 0 (0.0%) | 9 (47.4%) | 11 (57.9%) | 3 (15.8%) |
| No association | 4 | 3 (75.0%) | 1 (25.0%) | 1 (25.0%) | 2 (50.0%) | 0 (0.0%) | 2 (50.0%) | 2 (50.0%) | 0 (0.0%) |
| Geographic factors a | |||||||||
| Significant association * | 9 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 7 (77.8%) | 2 (22.2%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| No association | 1 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornelius, S.L.; Berry, T.; Goodrich, A.J.; Shiner, B.; Riblet, N.B. The Effect of Meteorological, Pollution, and Geographic Exposures on Death by Suicide: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7809. https://doi.org/10.3390/ijerph18157809
Cornelius SL, Berry T, Goodrich AJ, Shiner B, Riblet NB. The Effect of Meteorological, Pollution, and Geographic Exposures on Death by Suicide: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(15):7809. https://doi.org/10.3390/ijerph18157809
Chicago/Turabian StyleCornelius, Sarah L., Tara Berry, Amanda J. Goodrich, Brian Shiner, and Natalie B. Riblet. 2021. "The Effect of Meteorological, Pollution, and Geographic Exposures on Death by Suicide: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 15: 7809. https://doi.org/10.3390/ijerph18157809
APA StyleCornelius, S. L., Berry, T., Goodrich, A. J., Shiner, B., & Riblet, N. B. (2021). The Effect of Meteorological, Pollution, and Geographic Exposures on Death by Suicide: A Scoping Review. International Journal of Environmental Research and Public Health, 18(15), 7809. https://doi.org/10.3390/ijerph18157809