
Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery



Abstract
1. Introduction
2. Method
2.1. The Research Context
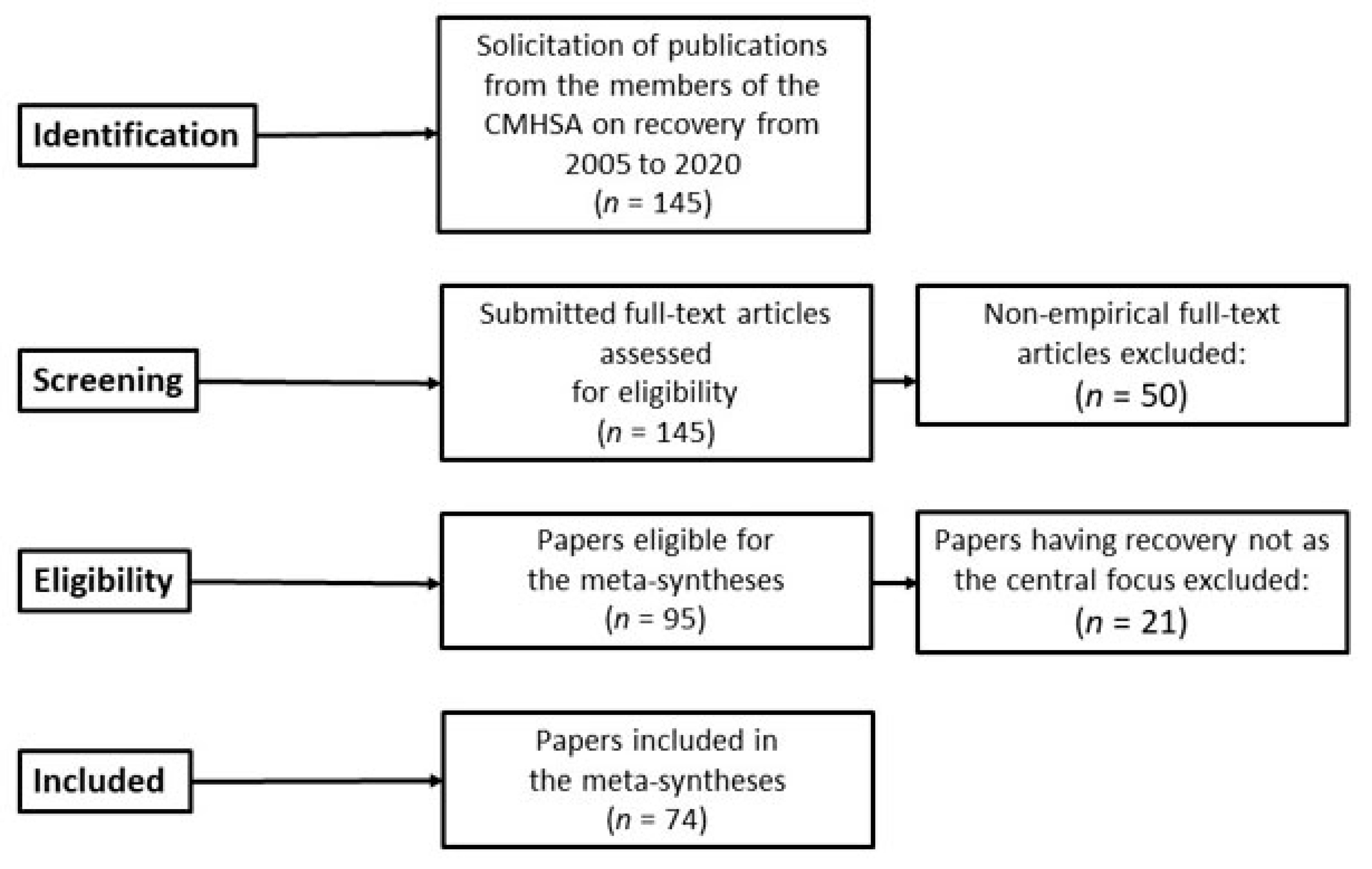
2.2. Qualitative Meta-Syntheses
3. Results
- a
- Being normal
- b
- Respecting and accepting oneself
- c
- Being in control
- d
- Recovery as intentional
- e
- Recovery as material and social
4. Discussion
4.1. Recovery as Dynamics between the Self and Others
4.2. Recovery as Dynamics between the Self and Material Contexts
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pincus, H.A.; Spaeth-Rublee, B.; Sara, G.; Goldner, E.M.; Prince, P.N.; Ramanuj, P.; Gaebel, W.; Zielasek, J.; Großimlinghaus, I.; Wrigley, M.; et al. A review of mental health recovery programs in selected industrialized countries. Int. J. Ment. Health Syst. 2016, 10, 1–9. [Google Scholar] [CrossRef]
- Slade, M.; Amering, M.; Farkas, M.; Hamilton, B.; O’Hagan, M.; Panther, G.; Perkins, R.; Shepherd, G.; Tse, S.; Whitley, R. Uses and abuses of recovery: Implementing recovery-oriented practices in mental health systems. World Psychiatry 2014, 13, 12–20. [Google Scholar] [CrossRef]
- Tuffour, I. The concept of recovery and its practical application. Ment. Health Pract. 2017, 20, 37–41. [Google Scholar] [CrossRef][Green Version]
- Austin, S.F.; Mors, O.; Secher, R.G.; Hjorthøj, C.R.; Albert, N.; Bertelsen, M.; Jensen, H.; Jeppesen, P.; Petersen, L.; Randers, L.; et al. Predictors of recovery in first episode psychosis: The OPUS cohort at 10 year follow-up. Schizophr. Res. 2013, 150, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, R.; Pesola, F.; Leamy, M.; Bird, V.; Le Boutillier, C.; Williams, J.; Slade, M. The relationship between clinical and recovery dimensions of outcome in mental health. Schizophr. Res. 2016, 175, 142–147. [Google Scholar] [CrossRef]
- McCabe, R.; Whittington, R.; Cramond, L.; Perkins, E. Contested understandings of recovery in mental health. J. Ment. Health 2018, 27, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.; Borg, M.; Marin, I.; Topor, A.; Mezzina, R.; Sells, D. Processes of recovery in serious mental illness: Findings from a multi-national study. Am. J. Psychiatr. Rehabil. 2005, 8, 177–201. [Google Scholar] [CrossRef]
- Davidson, L.; O’Connell, M.J.; Tondora, J.; Staheali, M.; Evans, A.C. Recovery in serious mental illness: Paradigm shift or shibboleth. In Recovery from Severe Mental Illnesses: Research Evidence and Implications for Practice; Davidson, L., Harding, C., Spaniol, L., Eds.; Center for Psychiatric Rehabilitation, Sargent College of Health and Rehabilitation Sciences, Boston University: Boston, MA, USA, 2005; Volume 1, pp. 5–25. [Google Scholar]
- Leamy, M.; Bird, V.; Le Boutillier, C.; Williams, J.; Slade, M. Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. Br. J. Psychiatry 2011, 199, 445–452. [Google Scholar] [CrossRef]
- van Weeghel, J.; van Zelst, C.; Boertien, D.; Hasson-Ohayon, I. Conceptualizations, assessments, and implications of personal recovery in mental illness: A scoping review of systematic reviews and meta-analyses. Psychiatr. Rehabil. J. 2019, 42, 169. [Google Scholar] [CrossRef]
- Davidson, L. The recovery movement: Implications for mental health care and enabling people to participate fully in life. Health Aff. 2016, 35, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.; Tondora, J.; Ridgway, P. Life is not an ‘outcome’: Reflections on recovery as an outcome and as a process. J. Psychiatr. Rehabil. 2012, 13, 1–8. [Google Scholar] [CrossRef]
- Hummelvoll, J.K.; Karlsson, B.; Borg, M. Recovery and person-centredness in mental health services: Roots of the concepts and implications for practice. Int. Pract. Dev. J. 2015, 5, 7. [Google Scholar] [CrossRef]
- Jørgensen, K.; Praestegaard, J.; Holen, M. The conditions of possibilities for recovery: A critical discourse analysis in a Danish psychiatric context. J. Clin. Nurs. 2020, 29, 3012–3024. [Google Scholar] [CrossRef]
- Karlsson, B.; Borg, M. Recovery: Traditioner, Fornyelser og Praksiser [Recovery: Traditions, Innovations and Practices]; Gyldendal Akademisk: Oslo, Norway, 2017. [Google Scholar]
- Hunt, M.G.; Resnick, S.G. Two birds, one stone: Unintended consequences and a potential solution for problems with recovery in mental health. Psychiatr. Serv. 2015, 66, 1235–1237. [Google Scholar] [CrossRef]
- Norwegian Directorate of Health. «Sammen om Mestring» Veileder i Lokalt Psykisk Helsearbeid [Mastering Together—Guidelines for Local Mental Health Work]; Norwegian Directorate of Health: Oslo, Norway, 2014.
- Norwegian Ministry of Health and Social Affairs. Opptrappingsplanen for Psykisk Helse [The National Action Program for Mental Health]; Norwegian Ministry of Social and Health Affairs: Oslo, Norway, 1999.
- Brekke, E.; Lien, L.; Biong, S. Experiences of professional helping relations by persons with co-occurring mental health and substance use disorders. Int. J. Ment. Health Addict. 2018, 16, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Horsfall, D.; Paton, J.; Carrington, A. Experiencing recovery: Findings from a qualitative study into mental illness, self and place. J. Ment. Health 2018, 27, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Topor, A.; Ljungqvist, I.; Strandberg, E.L. Living in poverty with severe mental illness coping with double trouble. Nord. Soc. Work Res. 2016, 6, 201–210. [Google Scholar] [CrossRef]
- Klevan, T.; Jonassen, R.; Sælør, K.T.; Borg, M. Using dyadic interviews to explore recovery as collaborative practices: Challenging the epistemic norm of the single person perspective. Int. J. Qual. Methods 2020, 19, 1–9. [Google Scholar] [CrossRef]
- Price-Robertson, R.; Obradovic, A.; Morgan, B. Relational recovery: Beyond individualism in the recovery approach. Adv. Ment. Health 2017, 15, 108–120. [Google Scholar] [CrossRef]
- Sandelowski, M.; Docherty, S.; Emden, C. Qualitative metasynthesis: Issues and techniques. Res. Nurs. Health 1997, 20, 365–371. [Google Scholar] [CrossRef]
- Noblit, G.W.; Hare, R.D. Meta-Ethnography: Synthesizing Qualitative Studies; Sage: Newcastle upon Tyne, UK, 1988. [Google Scholar]
- Noblit, G.W. How Qualitative (or Interpretive or Critical) Is Qualitative Synthesis and What We Can Do about This; A Public Lecture by Professor George W. Noblit; University of North Carolina: Chapel Hill, NC, USA, 2016. [Google Scholar]
- CASP (Critical Appraisal Skills Program). CASP Qualitative Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 15 March 2021).
- Sells, D.; Andrés-Hyman, R.; Lawless, M.S.; Borg, M.; Topor, A.; Mezzina, R.; Marin, I.; Davidson, L. Contexts and narratives of recovery. Am. J. Psychiatr. Rehabil. 2005, 8, 203–221. [Google Scholar] [CrossRef]
- Borg, M.; Sells, D.; Topor, A.; Mezzina, R.; Marin, I.; Davidson, L. What makes a house a home: The role of material resources in recovery from severe mental illness. Am. J. Psychiatr. Rehabil. 2005, 8, 243–256. [Google Scholar] [CrossRef]
- Sells, D.; Borg, M.; Davidson, L.; Marin, I.; Mezzina, R.; Topor, A. Arenas of recovery for persons with severe mental illness. Am. J. Psychiatr. Rehabil. 2006, 9, 3–16. [Google Scholar] [CrossRef]
- Topor, A.; Borg, M.; Mezzina, R.; Sells, D.; Marin, I.; Davidson, L. Others: The role of family, friends, and professionals in the recovery process. Am. J. Psychiatr. Rehabil. 2006, 9, 17–37. [Google Scholar] [CrossRef]
- Mezzina, R.; Borg, M.; Marin, I.; Sells, D.; Topor, A.; Davidson, L. From participation to citizenship: How to regain a role, a status, and a life in the process of recovery. Am. J. Psychiatr. Rehabil. 2006, 9, 39–61. [Google Scholar] [CrossRef]
- Biong, S.; Ravndal, E. Young men’s experiences of living with substance abuse and suicidal behaviour: Between death as an escape from pain and the hope of a life. Int. J. Qual. Stud. Health Well-Being 2007, 2, 246–259. [Google Scholar] [CrossRef]
- Borg, M.; Davidson, L. Recovery as lived in everyday experience. J. Ment. Health 2008, 17, 129–141. [Google Scholar] [CrossRef]
- Borg, M.; Kristiansen, K. Working on the edge. Everyday life research from Norway on the meaning of work for people recovering in psychosis. Disabil. Soc. 2008, 23, 511–523. [Google Scholar] [CrossRef]
- Topor, A.; Borg, M.; Di Girolamo, S.; Davidson, L. Not just an individual journey: Social aspects of recovery. J. Soc. Psychiatry 2009, 57, 90–99. [Google Scholar] [CrossRef]
- Herrestad, H.; Biong, S. Relational hopes: A study of the lived experience of hope in some patients hospitalized for intentional self harm. Int. J. Qual. Stud. Health Well-Being 2010, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Veseth, M.; Binder, P.E.; Borg, M.; Davidson, L. Toward caring for oneself in a life of intense ups and downs: A reflexive-collaborative exploration of recovery in bipolar disorder. Qual. Health Res. 2012, 22, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Borg, M.; Veseth, M.; Binder, P.E.; Topor, A. The role of work in recovery from bipolar disorders. Qual. Soc. Work 2013, 12, 323–339. [Google Scholar] [CrossRef]
- Veseth, M.; Binder, P.E.; Borg, M.; Davidson, L. How I found out I had a bipolar disorder: A reflexive-collaborative exploration of participants’ experiences of identifying that one is struggling with a severe mental health problem. Qual. Stud. 2013, 4, 21–38. [Google Scholar] [CrossRef]
- Sælør, K.T.; Ness, O.; Semb, R. Taking the plunge: Service users’ experiences of hope within the mental health and substance use services. Scand. Psychol. 2015, 2. [Google Scholar] [CrossRef]
- Biong, S. Å bli en del av fellesskapet—En analyse av recovery som personlige og sosiale prosesser ved ROP-lidelser [Becoming part of the community: An analysis of recovery as personal and social processes in dual diagnosis]. In Et Bedre liv. Historier, Erfaringer og Forskning om Bedring ved Rusproblemer og Psykiske Helseproblemer [A Better Life. Stories, Experiences and Research on Recovery from Substance Abuse and Mental Health Problems]; Landheim, A., Wiig, F.L., Brendbekken, M., Brodahl, M., Biong, S., Eds.; Gyldendal Akademiske: Oslo, Norway, 2016; pp. 134–145. [Google Scholar]
- Semb, R.; Borg, M.; Ness, O. Tilpasning eller tilbaketrekning? Tilhørighetsstrategier blant unge voksne med rus- og psykisk helseproblemer [Adjustment or withdrawal? Strategies of belonging among young adults with substance abuse and mental health problems]. Tidsskr. Velferdsforskning 2016, 19, 206–222. [Google Scholar] [CrossRef]
- Storch, J.; Ness, O. Relationel identitet: Hvordan professionelle og borgere skaber hinanden som komplementære identiteter [Relational identity: How professionals and citizens create each other as complementary identities]. Kognit. Og Pædagogik 2016, 26, 42–51. [Google Scholar]
- Veseth, M.; Binder, P.E.; Borg, M.; Davidson, L. Recovery in bipolar disorders: Experienced therapists’ view of their patients’ struggles and efforts when facing a severe mental illness. J. Psychother. Integr. 2016, 26, 437–449. [Google Scholar] [CrossRef]
- Brekke, E.; Lien, L.; Davidson, L.; Biong, S. First-person experiences of recovery in co-occurring mental health and substance use conditions. Adv. Dual Diagn. 2017, 10, 13–24. [Google Scholar] [CrossRef]
- Karlsson, B.; Borg, M.; Ogundipe, E.; Sjåfjell, T.; Bjørlykhaug, K.I. Aspekter ved samarbeidsrelasjoner mellom erfaringsmedarbeidere og brukere i psykisk helse- og rustjenester: En kvalitativ studie [Aspects of collaborative relationships between staff with lived experience and service users in mental health and substance abuse services: A qualitative study]. Nord. Tidsskr. Helseforskning 2017, 13. [Google Scholar] [CrossRef][Green Version]
- Sælør, K.T.; Biong, S. “Å få lyset til å fortsette å brenne”: En fenomenologisk studie av håp hos pårørende i psykisk helsevern [“Keeping the candle burning”: A phenomenological study of family members’ hope in mental health care]. Scand. Psychol. 2017, 4. [Google Scholar] [CrossRef]
- Sælør, K.; Klevan, T.; Sundet, R. «Du må gi for å få…». Historier om hvordan håp kan vokse gjennom dialog og samhandling [“You have to give in order to get…”. Stories about how hope can grow through dialogue and interaction]. In Perspektiver på psykisk helse- og rusarbeid [Perspectives on Mental Health and Substance Abuse Work]; Karlsson, B., Borg, M., Eds.; Fagbokforlaget: Oslo, Norway, 2018; pp. 45–55. [Google Scholar]
- Pettersen, H.; Landheim, A.; Skeie, I.; Biong, S.; Brodahl, M.; Oute, J.; Davidson, L. How social relationships influence substance use disorder recovery: A collaborative narrative study. Subst. Abus. Res. Treat. 2019, 13, 1–8. [Google Scholar] [CrossRef]
- Semb, R.; Tjora, A.; Borg, M. Communal invalidation of young adults with co-occurring substance abuse and mental health issues. Disabil. Soc. 2019, 34, 926–944. [Google Scholar] [CrossRef]
- Brekke, E.; Ness, O.; Lien, L. Relational recovery in co-occurring conditions: Qualitative study of first-person experiences. Adv. Dual Diagn. 2020, 13, 89–100. [Google Scholar] [CrossRef]
- Ogundipe, E.; Sælør, K.T.; Dybdahl, K.; Davidson, L.; Biong, S. “Come together”: A thematic analysis of experiences with belonging. Adv. Dual Diagn. 2020, 13, 123–134. [Google Scholar] [CrossRef]
- Trangsrud, L.J.; Borg, M.; Bratland-Sanda, S.; Klevan, T. Embodying experiences with nature in everyday life recovery for persons with eating disorders. Int. J. Environ. Res. Public Health 2020, 17, 2784. [Google Scholar] [CrossRef] [PubMed]
- McConnell, D. Narrative self-constitution and vulnerability to co-authoring. Theor. Med. Bioeth. 2016, 37, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M. Time, human being and mental health care: An introduction to Gilles Deleuze. Nurs. Philos. 2005, 6, 161–173. [Google Scholar] [CrossRef]
- Timander, A.-C.; Möller, A.; Davidson, L. The negative effects of oppression in the recovery process. Scand. J. Disabil. Res. 2017, 19, 34–44. [Google Scholar] [CrossRef][Green Version]
- Duff, C. Atmospheres of recovery: Assemblages of health. Environ. Plan. A 2016, 48, 58–74. [Google Scholar] [CrossRef]
- Roberts, M. Gilles Deleuze: Psychiatry, subjectivity, and the passive synthesis of time. Nurs. Philos. 2006, 7, 191–204. [Google Scholar] [CrossRef]
- Skatvedt, A. Bedringens Sosiologi: Om Potensialet i Hverdagslig Samhandling [The Sociology of Recovery: The Potential of Everyday Interaction], 1st ed.; Fagbokforlaget: Bergen, Norway, 2020. [Google Scholar]
- Thomas, C. Female Forms: Experiencing and Understanding Disability; Open University Press: Buckingham, UK, 1999. [Google Scholar]
- Glover, H. Guest editorial: Recovery based service delivery: Are we ready to transform the words into a paradigm shift? Aust. E-J. Adv. Ment. Health 2005, 4, 179–182. [Google Scholar] [CrossRef]
- Honneth, A. Kamp om Anerkjennelse: Om de Sosiale Konfliktenes Moralske Grammatikk [The Struggle for Recognition: The Moral Grammar of Social Conflicts]; Pax: Oslo, Norway, 2008. [Google Scholar]
- Bateson, G. Ecology of Mind: The Sacred. A Sacred Unity. Further Steps to an Ecology of Mind; Bessie/HarperCollins: New York, NY, USA, 1991. [Google Scholar]
- Doroud, N.; Fossey, E.; Fortune, T. Place for being, doing, becoming and belonging: A meta-synthesis exploring the role of place in mental health recovery. Health Place 2018, 52, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Nesse, L.; Gonzalez, M.T.; Aamodt, G.; Raanaas, R.K. Recovery, quality of life and issues in supported housing among residents with co-occurring problems: A cross-sectional study. Adv. Dual Diagn. 2020, 13, 73–87. [Google Scholar] [CrossRef]
- United Nations Human Rights Council. Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health; United Nations: Geneva, Switzerland, 2017. [Google Scholar]
- Norwegian Ministries. Housing for Welfare: National Strategy for Social Housing (2014–2020); Norwegian Ministries: Oslo, Norway, 2014.
- Tsai, J.; Bond, G.R.; Salyers, M.P.; Godfrey, J.I.; Davis, K.E. Housing preferences and choice among adults with mental illness and substance use disorder: A qualitative study. Community Ment. Health J. 2010, 46, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Padgett, D.K.; Gulcur, L.; Tsemberis, S. Housing first services for people who are homeless with co-occurring serious mental illness and substance abuse. Res. Soc. Work Pract. 2006, 16, 74–83. [Google Scholar] [CrossRef]
- Nes, R.B.; Clench-Aas, J. Psykisk Helse i Norge: Tilstandsrapport med Internasjonale Sammenligninger [Mental Health in Norway: Status Report with International Comparisons]; Norwegian Institute of Public Health: Oslo, Norway, 2011.
- O’Donnell, O.; Van Doorslaer, E.; Van Ourti, T. Health and inequality. In Handbook of Income Distribution; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Sælør, K.; Bjørlykhaug, K.; Bank, R.; Johnson, T. Møter i mørket: Økonomiske helseproblemer, subsidier og det sosiale liv [Meetings in the dark: Economic health problems, subsidies and social life]. Tidsskr. Velferdsforskning 2019. [Google Scholar] [CrossRef]
- Barstad, A. Økonomi, Helse og Livskvalitet. En Analyse av Levekårsundersøkelsen EU-SILC 2017. [Economy, Health and Quality of Life]; Statistisk Sentralbyrå: Oslo, Norway, 2020.
- Henwood, B.; Whitley, R. Creating a recovery-oriented society: Research and action. Aust. N. Z. J. Psychiatry 2013, 47, 609–610. [Google Scholar] [CrossRef] [PubMed]
- Dell, N.A.; Long, C.; Mancini, M.A. Models of mental health recovery: An overview of systematic reviews and qualitative meta-syntheses. Psychiatr. Rehabil. J. 2021. [Google Scholar] [CrossRef]
- Ramon, S. The place of social recovery in mental health and related services. Int. J. Environ. Res. Public Health 2018, 15, 1052. [Google Scholar] [CrossRef]
- Kim, H.S. The Nature of Theoretical Thinking in Nursing; Springer: New York, NY, USA, 2010. [Google Scholar]


{kind=link}
| Publications | Research Question(s) | Methods | Research Participants | Themes and Meanings |
|---|---|---|---|---|
| Davidson, L. et al. [7] | Explore processes of recovery in psychosis | Narrative and phenomenological approach with individual interviews | Twelve adults with experiences of recovery in psychosis |
|
| Sells, D. et al. [28] | To describe service system contexts in which the informants lived and received services and support | Phenomenological narrative interviews | Twelve persons in recovery | Roles of home, significant others, and coping strategies being interwoven in the context of individuals’ lives and personal recovery journeys |
| Borg, M. et al. [29] | How do people in recovery from psychosis develop and accept their role in society and where does that take place? | Qualitative interviews | Twelve adult service users in recovery from psychosis |
|
| Sells, D. et al. [30] | To identify community settings that appear to foster recovery, as well as the mechanisms through which this takes place | Qualitative individual interviews | Persons in recovery from psychosis | Involvement across various community settings can establish more beneficial and lasting understandings of the self
|
| Topor, A. et al. [31] |
| Qualitative interviews | Twelve persons in recovery |
|
| Mezzina, R. et al. [32]. | How do people in recovery from psychosis develop and accept their roles in society and where does that take place? | Qualitative interviews | Persons in recovery from psychosis | Social barriers to recovery:
|
| Biong, S. et al. [33] | How is meaning constructed in narratives of suicidal behavior? | Phenomenological hermeneutic approach with narrative interviews | Four adult males receiving substance abuse services | The meaning of living with suicidal behavior as a movement between different positions of wanting death as an escape from pain and hope for a better life:
|
| Borg, M. et al. [34] | To explore recovery within the context of the person’s everyday life | In-depth individual interviews | Thirteen adults in recovery |
|
| Borg, M. et al. [35] | To identify and discuss the role that work plays on the road to recovery for people with severe mental illness, particularly those diagnosed with psychosis | Phenomenological approach with in-depth individual interviews | Thirteen adult users with mental health problems |
|
| Topor, A. et al. [36] | To broaden the individual perspective on recovery by describing additional aspects of the journey that involve the contribution of others and various social factors and elements that can facilitate or impede inclusion in community life | Qualitative individual interviews |
| |
| Herrestad, H. et al. [37] | How meaning is constructed in narratives of hope by persons that have recently engaged in suicidal behavior | Hermeneutic–phenomenological approach using semi-structured in-depth interviews | Twelve adult patients admitted for overdose of medication |
|
| Veseth, M. et al. [38] | What do individuals with bipolar disorder do to promote their own recovery and what challenges do they meet? | Hermeneutic–phenomenological approach with individual in-depth interviews | Thirteen persons with bipolar disorder |
|
| Borg, M. et al. [39] | To understand the role of work in recovery from bipolar disorder, and to understand how people with such disorders deal with work-related challenges | Hermeneutic phenomenology and reflexive methodology | Thirteen adults with experience of bipolar disorder who are receiving or have received treatment |
|
| Veseth, M. et al. [40] | Explore first person perspectives on identifying a bipolar disorder: how do individuals experience the process of discovering that they have a bipolar disorder? What does it mean for the person to find out that their symptoms and distress are in line with descriptions commonly seen as a severe mental illness? | Hermeneutic–phenomenological approach with individual in-depth interviews | Thirteen individuals with recovery experiences | Three phases of recovery: (a) “uncertainty and confusion” through (b) “grasping the novel and unusual experiential states” to (c) “giving meaning to the lived experiences of intense ups and downs” |
| Sælør, K. T. et al. [41] |
| Cooperative action research approach with individual semi-structured interviews | Nine persons with MHSA problems |
|
| Biong, S. [42] | Wha are the personal narratives of recovery of persons with substance abuse problems? | Phenomenological narratives—written narratives | Fourteen persons with MHSA | Recovery as a long process and involving changes in significant aspects of the persons’ lives for the better:
|
| Semb, R. et al. [43] | To explore how young adults with co-occurring MHSA problems experience a sense of belonging in their local environment, and facilitators and barriers related to belonging | Hermeneutic–phenomenological approach with in-depth interviews | Seven young adult users |
|
| Storch, J. et al. [44] | Explore and describe recovery as experienced by young adults who live with co-occurring MHSA | Qualitative, individual interviews | Seven young adult service users of municipal community MHSA services |
|
| Veseth, M. et al. [45] | Explore therapists’ views of the processes of recovery in bipolar disorders | A reflexive, collaborative approach with semi-structured individual interviews | Twelve professional providers |
|
| Brekke, E. et al. [46] | Explore and describe recovery as experienced by persons living with co-occurring MHSA | Phenomenological individual interviews | Eight persons with recovery experiences | Four dimensions of recovery:
|
| Karlsson, B. et al. [47] | To explore and describeservice users’ experiences with peer support relationships, support and collaboration | Hermeneutic–phenomenological approach with focus group interviews | Twenty-six service users with MHSA problems |
|
| Sælør, K. T. et al. [48] | How do relatives of people with mental illness describe their experiences of hope? | Phenomenological, descriptive approach with focus group interviews | Fifteen relatives of people with mental illness |
|
| Sælør, K. et al. [49] | Stories of hope and recovery in MHSA | Written narratives | Two men with experience of MHSA |
|
| Pettersen, H. et al. [50] | To examine the role of social relationships in reaching and maintaining stable recovery after many years of substance use disorders | Individual interviews, narrative analysis | Eighteen adult service users with at least five years of stable recovery |
|
| Semb, R. et al. [51] | What do young adults with co-occurring MHSA find challenging in relation to belonging in their local communities? | In-depth individual interviews | Seven young adult users of municipal MHSA services |
|
| Brekke, E. et al. [52] | To explore and describe first-person experiences of relational recovery in persons with MHSA conditions | In-depth individual interviews | Eight adult service users with MHSA problems at various stages of recovery | Social relationships viewed as both supportive and hindering recovery:
|
| Ogundipe, E. et al. [53] |
| Collaborative and reflexive individual interviewing and focus group interview | Residents of a supported housing facility and the staff | The experience of belonging in relation to the contribution of the community and contextual factors in supported housing, such as:
|
| Trangsrud, L. J. et al. [54] | To explore embodying experiences of nature related to recovery in everyday life for persons with eating disorders | Hermeneutic–phenomenological approach with individual interviews | Eight persons with experience of eating disorders |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klevan, T.; Bank, R.-M.; Borg, M.; Karlsson, B.; Krane, V.; Ogundipe, E.; Semb, R.; Sommer, M.; Sundet, R.; Sælør, K.T.; et al. Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery. Int. J. Environ. Res. Public Health 2021, 18, 7761. https://doi.org/10.3390/ijerph18157761
Klevan T, Bank R-M, Borg M, Karlsson B, Krane V, Ogundipe E, Semb R, Sommer M, Sundet R, Sælør KT, et al. Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery. International Journal of Environmental Research and Public Health. 2021; 18(15):7761. https://doi.org/10.3390/ijerph18157761
Chicago/Turabian StyleKlevan, Trude, Rose-Marie Bank, Marit Borg, Bengt Karlsson, Vibeke Krane, Esther Ogundipe, Randi Semb, Mona Sommer, Rolf Sundet, Knut Tore Sælør, and et al. 2021. "Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery" International Journal of Environmental Research and Public Health 18, no. 15: 7761. https://doi.org/10.3390/ijerph18157761
APA StyleKlevan, T., Bank, R.-M., Borg, M., Karlsson, B., Krane, V., Ogundipe, E., Semb, R., Sommer, M., Sundet, R., Sælør, K. T., Tønnessen, S. H., & Kim, H. S. (2021). Part I: Dynamics of Recovery: A Meta-Synthesis Exploring the Nature of Mental Health and Substance Abuse Recovery. International Journal of Environmental Research and Public Health, 18(15), 7761. https://doi.org/10.3390/ijerph18157761